
Abstract
Background:
To improve gait function in children with cerebral palsy, ankle-foot orthoses are often prescribed. However, until now, little attention has been devoted to the effect of ankle-foot orthoses on the postural control during walking in children with cerebral palsy.
Objectives:
The aim was to compare the differences in thorax, spine, and pelvis movements in children with cerebral palsy during walking barefoot and walking with ankle-foot orthoses.
Study design:
Clinical study with an intra subject design.
Methods:
A total of 15 children (12 boys and 3 girls; mean age, 8 ± 2 years) with bilateral spastic cerebral palsy (12 with Gross Motor Function Classification System I and 3 with Gross Motor Function Classification System II) performed a full-body three-dimensional gait analysis. Differences in the range of motion of the thorax, spine, and pelvis during walking barefoot and walking with bilateral ankle-foot orthoses were analyzed (SPSS v20, paired-samples t-test).
Results:
Children with cerebral palsy showed a significantly larger range of motion of the thorax (flexion/extension, lateral bending, and rotation) and the spine (lateral bending) during walking with ankle-foot orthoses compared to walking barefoot. No significant differences were found in the range of motion of the pelvis between these two conditions.
Conclusion:
It can be concluded that wearing ankle-foot orthoses influences the postural control during walking in children with bilateral spastic cerebral palsy. Due to the increased range of motions, the movement pattern of the trunk diverges from the typically developing children.
Clinical relevance
Wearing ankle-foot orthoses not only gives more stability at the pelvis and ankle joint but also influences trunk motion. In order of the level of core stability of the child, compensations can be either seen in the lower back or the upper trunk. Clinicians should be aware of these compensations and should evaluate postural control in a more detailed evaluation.
Background
Cerebral palsy (CP) is a complex of symptoms that originates from a non-progressive disorder of the immature brain including various types and expressions of persistent motor function alterations. 1 Based on the main motor disorder, three main subtypes of CP are defined: spastic, dyskinetic, and ataxic CP. These subtypes are characterized by abnormal posture and movements. 2
In spastic CP, which is the most common diagnosed subtype, children may develop quite normally during the early stages of supported locomotion but fail to progress into plantigrade gait. They retain the digitigrade pattern during the last stages of their locomotor development, characterized by excessive muscle co-contraction, deficient equilibrium, and poor kinematic chain coordination. This partly results in an immature postural control of the center of mass (CoM) during walking with up keeping a negative vertical CoM acceleration at foot contact. 3 Children with bilateral spastic CP present typical gait abnormalities related to deficient trunk postural control and insufficient lower limb coordination. 4 Previous research showed a difference in trunk kinematics during walking between children with CP and typically developed children.5,6
In comparison with typically developed children, children with CP show a delayed development in the capacity to generate direction-specific adjustments in tasks with a mild postural challenge. 7 Further on, they have dysfunctions in the fine-tuning of the postural adjustment, that is, an invariable recruitment order, an excessive degree of antagonistic co-activation during external perturbations, and a reduced capacity to modulate postural adjustments. 7 Children with CP have a decreased dynamic head and trunk stability during gait compared to typically developing children. Children with a more impaired form of CP also showed a decreased lateral thorax bending stability while walking. 8 Walking with ankle-foot orthoses (AFOs) influenced these trunk excursions and can interfere with postural control. These increased trunk excursions can be problematic in children who already have problems with postural control. Therefore, we wanted to investigate more in detail where the problems at postural control arise. Children with CP usually start to walk later than their peers without CP, walk at a slower speed, and with a higher energy cost. Orthosis is widely used in the management of children with CP even though there is no robust evidence for its effect. 9 To align the foot and ankle in children with CP, an AFO is most frequently used. This distal control is believed to exert a positive effect on more proximal joints as well. 10 AFOs are designed to improve balance and stability, to improve walking ability, and/or to affect the body structure (i.e. to prevent or treat muscle contractures). 9 Also improvements in the stability and in the gait pattern of children with CP, measured during gait analysis and with the index of symmetry, were reported when using AFOs. 11 Furthermore, AFOs have been found to increase step length and velocity and decrease cadence and energy cost.4,9
Despite the fact that many studies investigated the effect of AFOs on the gait pattern in children with CP, 12 little attention has been given to the effect of AFOs on postural control during gait in children with bilateral spastic CP. 4
Therefore, the aim of this study was to evaluate the differences in range of motion (ROM) of the thorax, the spine, and the pelvis during walking barefoot and walking with AFOs in children with bilateral spastic CP.
Methods
Participants
Children with CP were measured during a gait analysis between January 2014 and December 2015 at the center of motion analysis of the rehabilitation hospital Inkendaal in Vlezenbeek (Belgium). The children had to meet the following inclusion criteria: boys and girls diagnosed with bilateral spastic CP, with an age between 5 and 12 years and a Gross Motor Function Classification System (GMFCS) classification I or II (to be sure that the patients could walk without any assistive device). The exclusion criteria were other neurological disorders or congenital disease, a lower-extremity fracture or surgery during the last year, botulinum toxin injection during the last 3 months, and GMFCS classification III, IV, and V (not able to walk without assistive device).
The effect size was set at 0.68 (based on the results of a study by Degelean et al. 4 ) with a power of (1 − β) 0.80 and a type I error (α) of 0.05. Sample size was calculated by making use of “G*Power 3.1.9.2 for Windows XP.” A total of 15 participants were required to be able to perform the study. Because all the measurements were completed during one visit per participant, there was no need to add 10%–15% of participants in case of drop-outs.
Data collection
In preparation of the gait analysis, the participants were subject to a physical examination by a physiotherapist. The information acquired was sex, age, GMFCS, ankle, knee and hip mobility, intensity of spasticity (modified Ashworth Scale), and muscle strength (Manual Muscle Testing).
All children involved wore the same bilateral orthosis: posterior leaf spring AFOs. These AFOs provide support to the ankle-foot complex in the coronal and sagittal planes and restrict dorsal and plantar flexion at the ankle joint. They are made for functional use and aim to optimize gait and improve foot control in patients with spastic or flaccid paralysis and/or postural abnormalities of the lower leg. Typically, these are made of plastic. Specific information about the bilateral AFOs was collected: type, number of hours per day that he or she is wearing the orthoses, and how long he or she is already wearing the orthosis. Subsequently, the markers were placed according to the full-body plug-in-gait model. When the subjects wore the AFOs, where required, the markers were placed on the AFOs.
During the three-dimensional (3D) motion capture, the participants walked at a self-determined walking speed along a 10-m walkway, looking straight forward. Cones were placed at the start and end of the walkway to inform subjects when to stop and turn. Five trials of barefoot walking were followed by five trials of walking with the children’s own bilateral AFOs. All motion was tracked by the VICON motion analysis system. In all, 16 infrared cameras (MXT40S, 100 Hz, Vicon motion system Ltd, UK) detected the markers (reflective markers 14 mm hard) and 4 Bonita 720C cameras (100 Hz) registered the subject during walking.
Data analysis
Marker labeling and trajectory reconstruction were performed using Nexus 1.8.5 (Oxford Metrics, UK) and filtered with the Woltring procedure. 3D motion analysis was done by means of Vicon 512 (VICON Motion Systems, Inc., Los Angeles, CA).
From the absolute angles of the thorax and the pelvis relative to the global laboratory frame, the following variables were calculated: (1) the ROM in the sagittal plane of the thorax (flexion and extension), (2) the ROM in the frontal plane of the thorax (lateral bending), (3) the ROM in the transversal plane of the thorax (rotations), (4) the ROM in the sagittal plane of the pelvis (flexion and extension), (5) the ROM in the frontal plane of the pelvis (lateral bending), (6) the ROM in the transversal plane of the pelvis (rotation), (7) the ROM in the sagittal plane of the spine (flexion and extension), (8) the ROM in the frontal plane of the spine (lateral bending), and (9) the ROM in the transversal plane of the spine (rotation).
Statistical analysis
Statistics was performed using SPSS v20 (IBM Corporation, Armonk, NY, USA). All data were tested for normal distribution using Kolmogorov–Smirnov test. For the normally distributed ROM parameters, a paired-samples t-test was used to evaluate differences in the kinematics of the thorax, spine, and pelvis in children with CP during walking barefoot and walking with AFOs. A Wilcoxon test was done on the data which were not normally distributed. To cope with the family wise error, the p-values of the pairwise comparisons were adapted following the Benjamini–Hochberg procedure. The level of significance (α) was set at 10% (p < 0.10).
Ethical aspects
The study was approved by the local ethical committee (2016-WMD-002) and informed consent was obtained from each subject and legal guardian.
Results
Participants
A total of 15 children with bilateral spastic CP (12 boys and 3 girls; 12 with GMFCS level I and 3 with GMFCS level II; mean age, 8 ± 2 years; mean height, 127.4 ± 14.4 cm; and mean body weight, 25.68 ± 8.75 kg) were included in the study. All subject characteristics are reported in Table 1.
Characteristics of the participants.
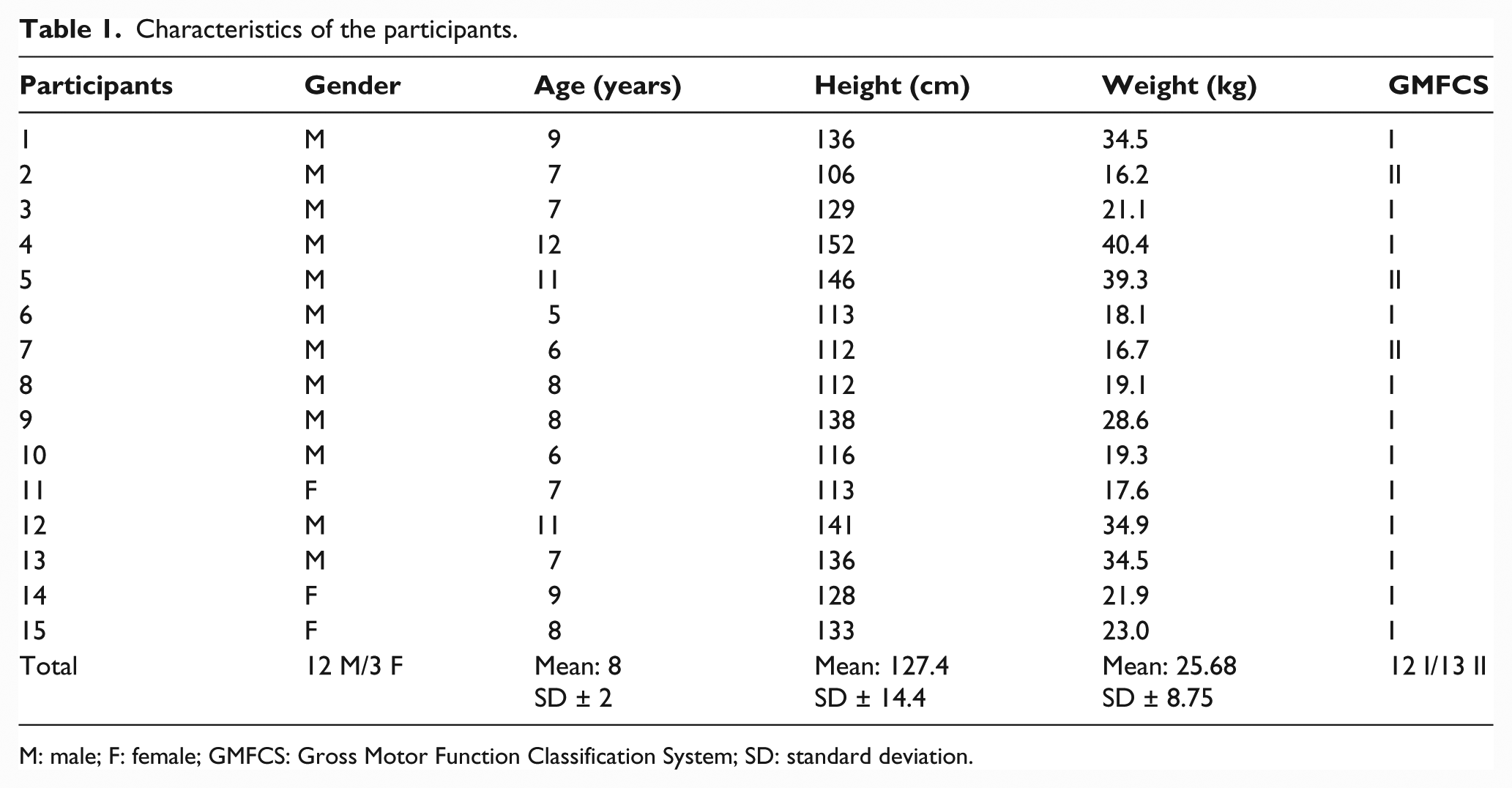
M: male; F: female; GMFCS: Gross Motor Function Classification System; SD: standard deviation.
Movement amplitudes
Table 2 gives an overview of the differences in kinematics of the thorax, the spine, and the pelvis during walking with AFOs and walking barefoot.
Comparison of the kinematics of the thorax, spine, and pelvis during walking with AFOs and walking barefoot.
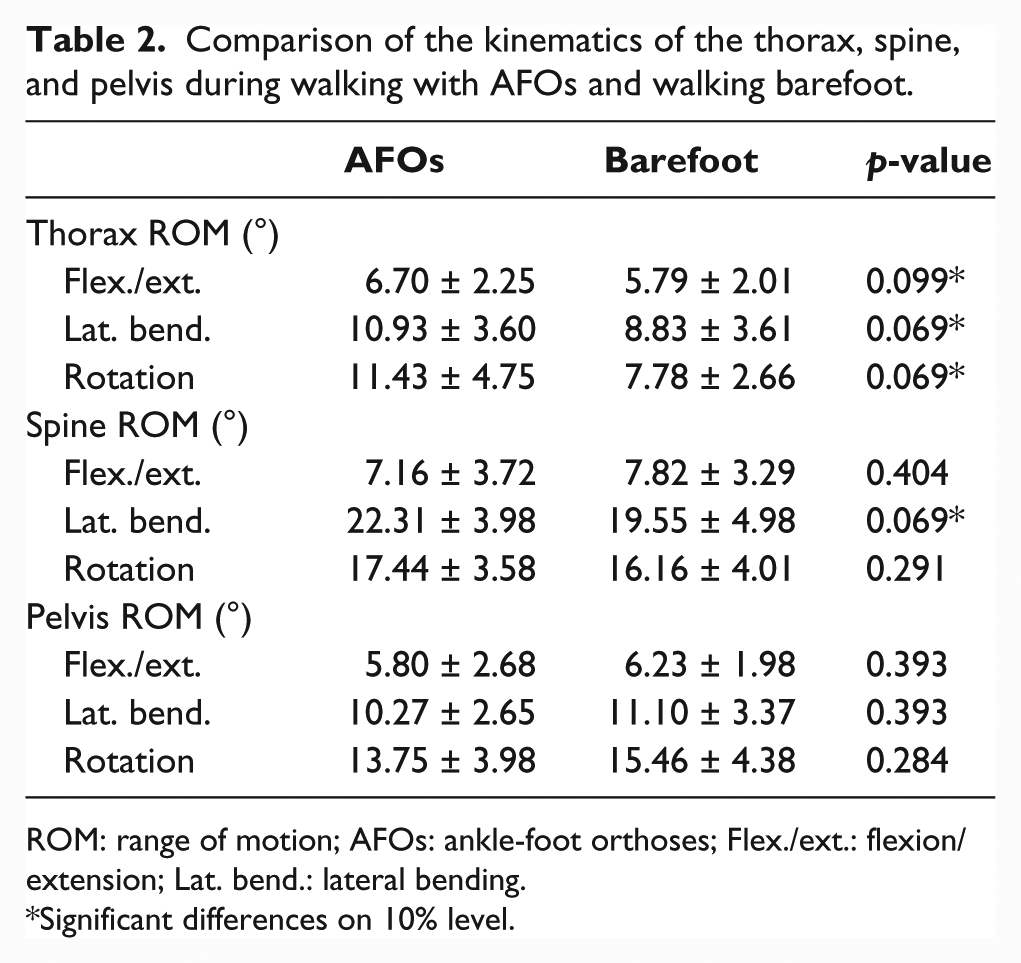
ROM: range of motion; AFOs: ankle-foot orthoses; Flex./ext.: flexion/extension; Lat. bend.: lateral bending.
Significant differences on 10% level.
ROM of the thorax during walking with AFOs compared to walking barefoot
Children with CP showed a significant greater ROM of the thorax during walking with AFOs compared to barefoot walking. The greater ROM is presented in sagittal (flexion/extension), frontal (lateral bending), and transversal planes (rotation). Comparing the mean values shown in Table 2, walking with AFOs led to a greater ROM in flexion/extension (6.7° vs 5.79°; p = 0.099), in lateral bending (10.93° vs 8.83°; p = 0.069), and in rotation (11.43° vs 7.78°; p = 0.069) of the thorax compared to walking barefoot.
ROM of the spine during walking with AFOs compared to walking barefoot
A significant greater ROM of the spine was found in lateral bending (22.31° vs 19.55°; p = 0.069) during walking with AFOs compared to walking barefoot in children with CP. The flexion/extension movements of the spine were decreased (7.16° vs 7.82°; p = 0.404) and the rotation of the spine was increased (17.44 vs 16.16; p = 0.194) during walking with AFOs compared to walking barefoot in children with CP, but those differences were not significant.
ROM of the pelvis during walking with AFOs compared to walking barefoot
The pelvis flexion/extension (5.80° vs 6.23°; p = 0.349), lateral bending (10.27° vs 11.10°; p = 0.322), and rotation (13.75° vs 15.46°; p = 0.158) were decreased during walking with AFOs compared to walking barefoot, but no significant differences were found.
Discussion
AFOs are often prescribed for children with bilateral spastic CP, to improve gait by increasing walking velocity, stride, and step length and decreasing cadence and energy cost.13–15 Despite this, little is known about the differences in kinematics of the thorax, spine, and pelvis in children with CP walking with AFOs compared to walking barefoot. In this study, a significant larger ROM of the thorax in the sagittal, frontal, and transversal planes and a significant larger ROM of the spine in the frontal plane were found during walking with AFOs compared to walking barefoot. Nevertheless, the ROM of the spine and the pelvis in the sagittal plane was decreased, but not significantly, during walking with AFOs.
Degelean et al. 4 investigated the effect of AFOs on trunk sway and lower limb intersegmental coordination in children with bilateral CP and concluded that wearing AFOs results in increased trunk motion, and Molenaers et al. 16 found significantly increased trunk ROM in children with CP during walking with AFOs compared to walking barefoot. In general, the results of our study were similar with the few studies found in the literature.4,12,16 However, our results are not directly comparable as for example with the mixed patients with unilateral and bilateral CP in the study of Molenaers et al. 16 In our study, only children with spastic bilateral CP were included. Ridgewell et al. 12 identified 41 full papers which examined the effect of AFO use on a diverse range of outcome measures in children or adolescents (aged 6–18 years) who had a primary diagnosis of CP. Unfortunately, no conclusions could be defined due to the variety in the level and quality of detail reported. They recommended to focus on participant groups which exhibit some degree of homogeneity with regard to gait pattern or to subdivide groups to investigate the possibility that heterogeneity affects the results. 12 To ensure homogeneity of the groups, we took this recommendation into account in this study.
All the patients included in this study were diagnosed with bilateral spastic CP, and 80% of the patients had GMFCS I, which is the mildest type of gait deviation, and 20% had GMFCS II. This way the participants showed some degree of homogeneity in gait pattern. Gait abnormalities seen in other types of CP, ataxic and dyskinetic subtypes, cannot influence the results. Furthermore, since this study contains 15 subjects, the sample size calculation is satisfactory.
Children with bilateral CP already have an increased ROM of the thorax, pelvis, and spine in all planes compared to typically developed children.6,17,18 This can be a result of a combination between the compensation of lower limb impairments and the presence of trunk control deficit. 19
In a systematic literature study, Swinnen et al. 6 concluded that the ability to control trunk movements varies between bilateral spastic CP children with different degrees of motor involvement. Children with GMFCS II showed increased ROM at more levels (thorax, pelvis, and spine) than children with GMFCS I (thorax). 6 Other studies had the same conclusion.8,17,18
An increased movement amplitude of the trunk can be considered as an indicator of a diminished dynamic stability or as a compensatory strategy for the reduction of ankle power generation at push off.5,6 The biomechanical constraints associated with the AFOs are another possible cause of an increased movement amplitude of the trunk. 4 This last one is an acceptable explanation for the larger movements of the thorax and spine found in this study during walking with AFOs. This study shows us that the trunk cannot be seen as one segment and that it is important to distinguish the upper (trunk) from the lower (spine) part. Underlying trunk control deficit in children with CP is related to altered trunk movements during gait. 8 The observed thorax movements during gait should not solely be considered as compensatory movements for lower limb impairments, but most likely are the resultant of both compensatory movements for lower limb deficits and an underlying trunk control deficit. More knowledge of the underlying coordination mechanism between trunk and lower limbs can help us to set up therapeutic interventions aiming to improve trunk control in these children.
There are some limitations to this study. First, a comparison was made between walking with AFOs and walking barefoot. Data for walking with shoes only are missing. Second, children walked at their preferred walking speed. Gait parameters like starting position, walking speed, step, and stride length were not taken into account. The influence of these parameters could therefore not be established on the data found in this study. Furthermore, all patients were accustomed to walk with AFOs in daily life. Therefore, it is possible that they have learned and adapted a gait pattern by wearing AFOs, which they continue to use when they walk barefoot. 20 This should be investigated during future research. Moreover, during further research, the integration of electromyographic (EMG) analysis to measure the activity of the postural muscles can be of added value. Measurements of the timing and activity of these muscles are important to understand the root causes of movements.
Conclusion
It can be concluded that in children with bilateral spastic CP, compared to walking barefoot, walking with AFOs led to significant greater movement amplitudes of the thorax in the three directions and of the spine for lateral bending. No significant differences in movement amplitudes were found for the pelvis between these two conditions. An increased movement amplitude of the trunk can be considered as an indicator of a diminished dynamic stability or as a compensatory strategy for the reduction of ankle power generation at push off. This could be caused by the biomechanical constraints associated with the AFOs. Further investigations are required with the integration of EMG analysis to understand the root causes of the altered trunk movements.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.