
Abstract
Background and aim:
Upper extremity myoelectric prostheses are expensive. The Robohand demonstrated that three-dimensional printing reduces the cost of a prosthetic extremity. The goal of this project was to develop a novel, inexpensive three-dimensional printed prosthesis to address limitations of the Robohand.
Technique:
The prosthesis was designed for patients with transradial limb amputation. It is shoulder-controlled and externally powered with an anthropomorphic terminal device. The user can open and close all five fingers, and move the thumb independently. The estimated cost is US$300.
Discussion:
After testing on a patient with a traumatic transradial amputation, several advantages were noted. The independent thumb movement facilitated object grasp, the device weighed less than most externally powered prostheses, and the size was easily scalable. Limitations of the new prosthetic include low grip strength and decreased durability compared to passive prosthetics.
Clinical relevance
Most children with a transradial congenital or traumatic amputation do not use a prosthetic. A three-dimensional printed shoulder-controlled robotic prosthesis provides a cost effective, easily sized and highly functional option which has been previously unavailable.
Keywords
Background and aim
In 2005, approximately 541,000 Americans were living with upper limb differences. 1 Upper limb differences can be congenital or the result of an amputation. In the United States, it is estimated that about 15 out of 100,000 newborns are affected with congenital upper limb anomalies, and 6000–10,000 people undergo upper limb amputations each year.1,2
Upper extremity prostheses are expensive. The average cost of body-powered prosthesis ranges from US$4000–US$8000 while externally powered prostheses are more expensive, often US$25,000–US$50,000. 3 The high cost of upper extremity prostheses is an especially large economic barrier for families because as a child grows, socket and liner modifications and new prosthetics are regularly required.
The application of three-dimensional (3D) printing technology to prosthetic arm development is a promising avenue for cost reduction. In 2011, Richard Van As and Ivan Owen developed a prosthesis with 3D-printed parts, the ‘Robohand’. This prosthesis utilises wrist motion, the tenodesis affect, to open and close mechanical fingers. The project is open source, allowing anyone with access to a 3D printer to print the parts independently. Alternatively, patients can pay US$2000 to buy a fully assembled device from Robohand. 4
The Robohand has two significant limitations. First, only patients with a functioning wrist can use the device. And second, the prosthetic is limited to opening and closing all five fingers simultaneously. The goal of this project was to design an inexpensive, 3D-printed prosthetic arm to address the Robohand’s limitations. Our externally powered design provides independent thumb movement in addition to opening and closing the fingers, and can be used by patients with transradial-level limb differences. A prototype of this design was built and tested on a patient.
Technique
Design overview
The overall design is a shoulder-controlled, externally powered, 3D-printed prosthetic arm with a voluntary-open, anthropomorphic terminal device (Figure 1(a)). An inertial measurement unit (IMU) assesses shoulder movements, and a microcontroller activates motors in the hand if the correct movements are sensed. The user can open and close the entire hand by moving the shoulder up and down, respectively, or open/close only the thumb with a pattern of forward and backward shoulder movements. The hand is held closed by elastic cables that run through the lower parts of the fingers. When the motors activate, cables running through the upper parts of the fingers are put under tension, and the hand opens. The estimated weight of the prosthesis is 240 g with a cost of US$300.
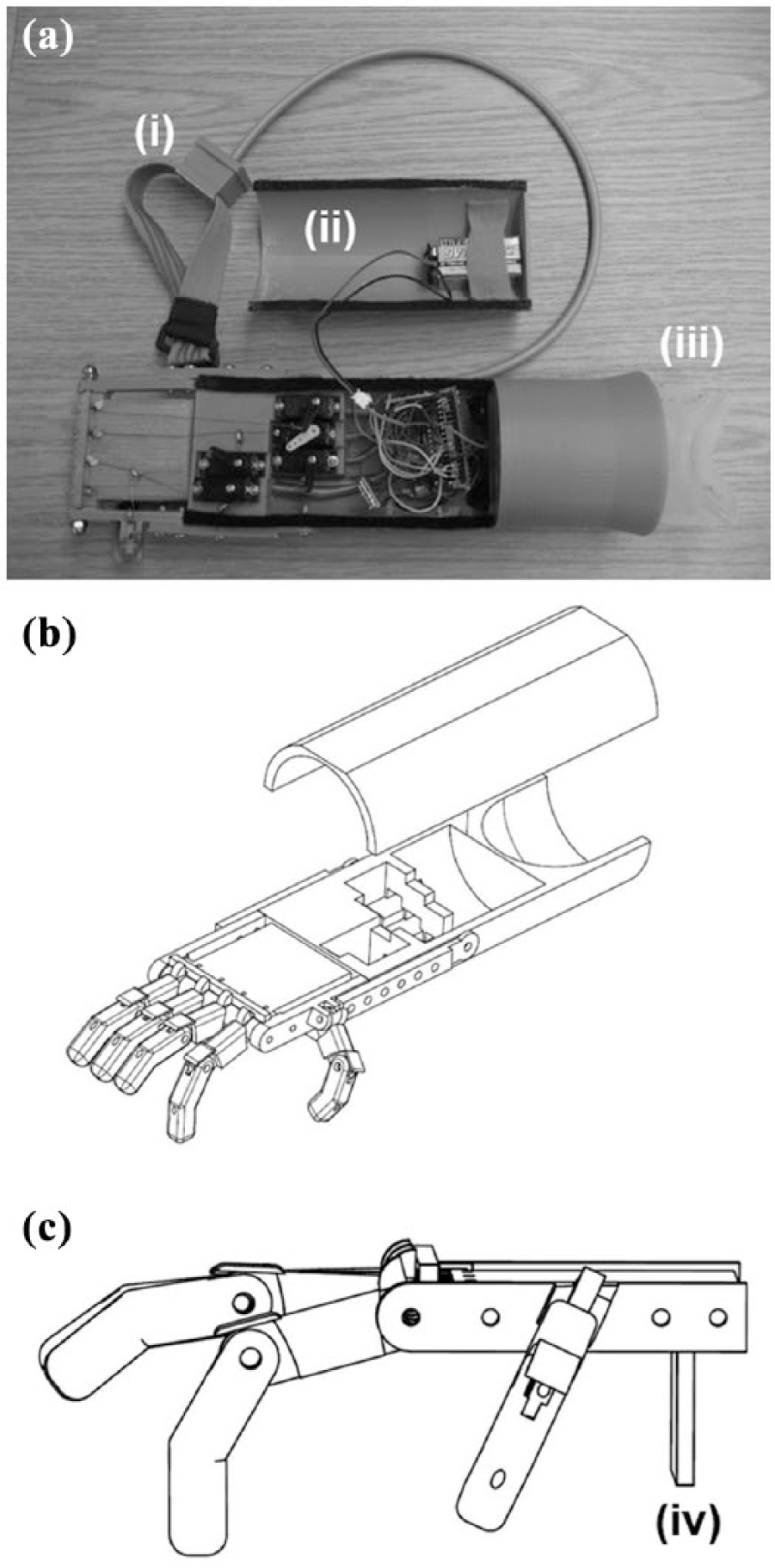
(a) Complete prosthesis. Cable connects shoulder motion sensor (i) to the electronics compartment. Top of electronics compartment (ii) shown detached. Clear plastic (iii) is the custom socket interface, (b) Computer-rendering of arm, with top detached and (c) Computer-rending of hand, with backstop (iv).
Mechanical design
The individual parts were designed in Autodesk Inventor (Autodesk, Inc., San Rafael, CA, USA) and printed with acrylonitrile butadiene styrene (ABS) plastic on a MakerGear M2 desktop 3D printer (MakerGear LLC; Beachwood, OH, USA). A computer-aided design (CAD) assembly drawing of the arm is shown in Figure 1(b) and (c).
Hand
The hand has five fingers, each with 2 degrees of freedom. In addition to the fingers, the hand has a palm-block. This acts as the palm of the hand and has a backstop to help grasp objects. Based on measurements of the affected and unaffected limbs, the final designs can be scaled appropriately for each user before printing. This ensures that the hand size matches the sound limb. The cabling is 1 mm elastic cord and 0.15 mm bead weaving thread that is designed to resist stretch over time.
Electronics compartment
The electronics compartment consists of a top and bottom component. The bottom of the electronics compartment holds the motors, microcontroller, voltage regulator and wiring components. The top has an area for the battery and covers the bottom component. The two parts are held together by Velcro®. This allows the top to be easily detached when the battery needs to be removed and charged.
Socket
The socket is made of ABS plastic and attaches the prosthesis to the residual limb and directly connects to the electronics compartment. The socket is custom-made and 3D-printed for each user to fit over a custom ethylene based thermoplastic gel liner made by a certified prosthetist. The gel liner and socket are attached to the residual limb through friction alone.
Overview of electronics
The IMU (IMU v2.3; JB Robotics, Irvine, CA, USA) constantly transmits motion data to the microcontroller board (Arduino Micro; Arduino; Torino, Italy) located in the electronics compartment. A 9 V lithium ion battery (Hi-Tech; GN Batteries, Walnut, CA, USA) directly powers the microcontroller. The battery also connects to a 5 V switching voltage regulator (UBEC; Adafruit Industries, New York City, NY, USA), which steps the voltage down to the motors. The battery capacity is 720 mAh. The estimate battery life varies from 0.5 h (hand always closed) to 5 h (hand always open) depending on how the prosthesis is used. We expect the hand to be in an open, resting position most of the time and therefore battery life should be closer to 5 h. The battery costs approximately US$14. All grounds are connected, and a simple sliding switch turns all components on and off.
IMU
The IMU (slave) transmits data by 4-wire serial peripheral interface (SPI) to the Arduino (master). It is powered at 3.3 V by the Arduino’s on-board 3.3 V voltage regulator (LP2985) and consumes a constant current of 75 mA. It internally updates at 250 Hz and directly outputs roll, pitch, yaw angles, their time derivatives and acceleration in the x, y and z directions. Arduino code to receive IMU data by SPI was provided by JB Robotics. The IMU is oriented such that when the shoulder is moved up and down relative to the body, the roll angle changes, and when the shoulder moves forward and backward in the transverse plane of the body, the yaw angle changes.
Microcontroller
The Arduino Micro (running off the ATmega32u4 microcontroller) was chosen as the microcontroller board because it can be easily programmed by those with minimal programming experience and includes all required features. This allows others to expand on our open-source design. The Arduino Micro operates at 5 V, which is supplied by an on-board voltage regulator (NCP1117) that steps down the voltage from the battery, and draws 42 mA. The digital output pins of the Arduino Micro controls each of the 5 motors independently by pulse-width modulation (PWM).
Motors
Each of the five fingers is driven by one micro-servo motor (MG90; Tower Pro, New Taipei City, Taiwan), which has a stall torque of 2.2 kg cm at 4.8 V. The motors are inexpensive (approximately US$7), lightweight (14 g) and small (23 × 12 × 29 mm3). Collectively, the motors draw 28 mA when stationary and unloaded (closed position). When the hand is opening, the components collectively draw a peak of roughly 1.7 A. When the hand is open and stationary, the components collectively draw approximately 1 A.
Code
The Arduino Micro was programmed in the Arduino integrated development environment. Arduino code includes a setup function that runs once and a main loop which repeats indefinitely after the setup function is completed. During each run, it reads the data from the IMU and checks for one of four conditions to be met. There is a minimum of 9 ms between each run giving a maximum sampling rate of 111 Hz. The flow of code is shown in Figure 1(a).
The shoulder up and down detection conditions are based solely on the time derivative, or velocity, of the roll angle. Adding a second signature shoulder motion to control thumb movement presents a challenge. Moving the shoulder forward changes the yaw angle, but so does rotating the entire body. Therefore, the yaw velocity alone cannot be used. We decided to control the thumb by moving the shoulder forward/backward twice in succession. To evaluate this motion, the history of yaw velocity needs to be known. A history vector keeps track of the last 1 s of yaw velocities reported by the IMU. This allows maximum and minimum values to be compared to determine forward/backward conditions, as shown in Figure 2 and Table 1.
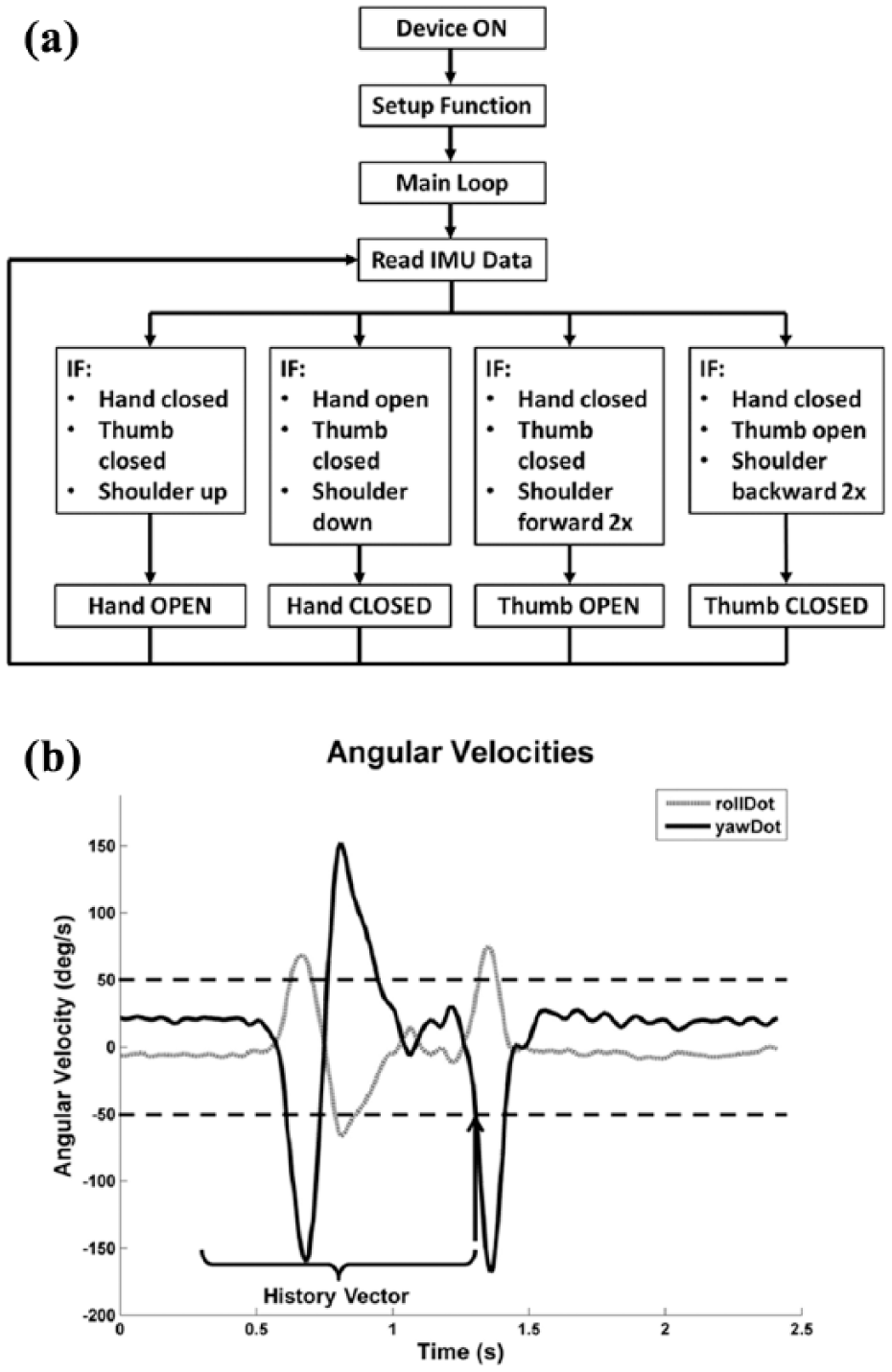
(a) Block diagram for code and (b) rollDot and yawDot recorded from shoulder moving forward twice. Dashed horizontal lines indicate thresholds for this motion. The arrow denotes where all forward 2x motion conditions would be met.
Shoulder movement conditions.
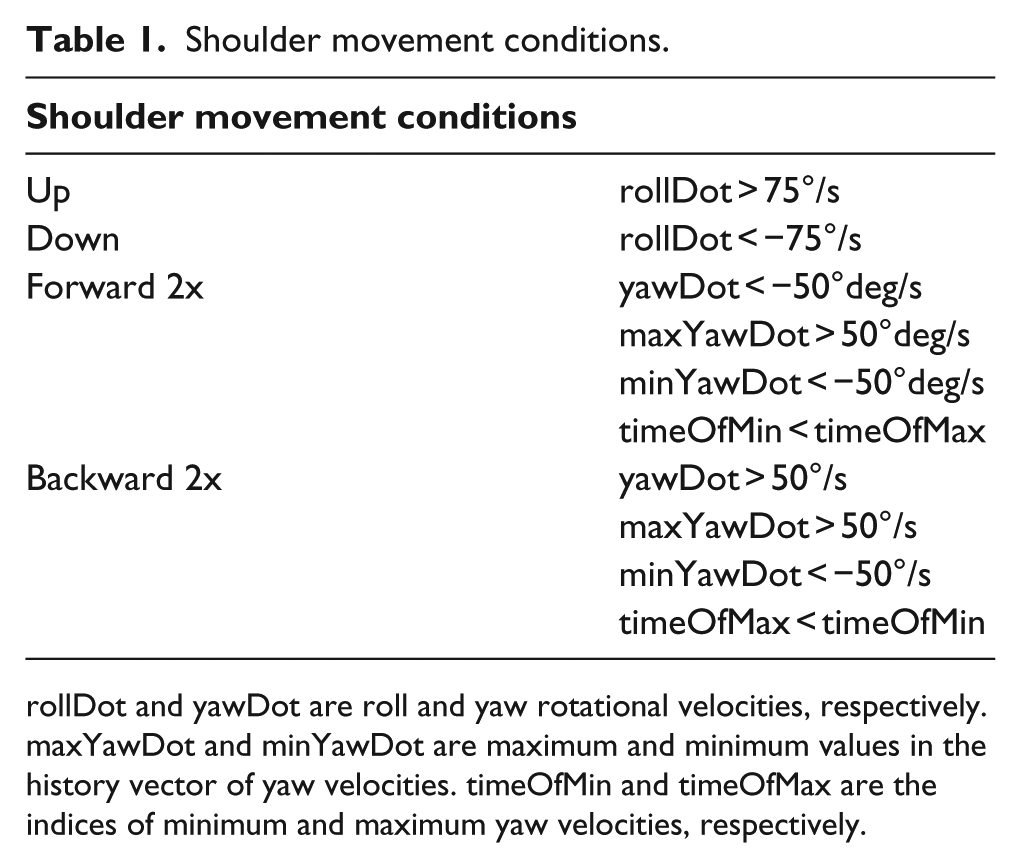
rollDot and yawDot are roll and yaw rotational velocities, respectively. maxYawDot and minYawDot are maximum and minimum values in the history vector of yaw velocities. timeOfMin and timeOfMax are the indices of minimum and maximum yaw velocities, respectively.
The thresholds are set to allow easy activation, but not trigger false positives. Users can easily adjust the threshold levels to suit their preferences. The activating motion is distinct enough from everyday motion that the user has full control of the arm across all normal range of motion.
Discussion
There are a variety of transradial-level upper extremity prostheses but a limited number are appropriate for children. 5 Most children are fitted with either a passive prostheses or a body powered voluntary closing terminal hook device given the durability and low cost of these options. More complex devices or myoelectric devices are rarely used in the skeletally immature due to both cost and weight.
Throughout the prototyping process we worked with a 13-year-old female patient with a transradial traumatic amputation. The patient cited that biggest advantages of the new prosthetic were the individual thumb movement, the ability to grasp objects with all five fingers and the low weight compared to other externally powered prostheses. The patient’s family also noted the design’s financial feasibility. Because the device is inexpensive and the size of the hand and socket can be scaled, users can easily print new devices as they grow older.
The design has a few limitations. These include short battery life, noise from the motors, low grip strength of the terminal device and low durability of mechanical components. With these limitations identified, improvements on the prototype can be developed.
Footnotes
Acknowledgements
We would like to thank Patricia Widder for the use of laboratory facilities and 3-D printers. We would also like to thank the patient and her family for their cooperation and support, and Valerie Calhoun and Maggie Ware-Smith (Shriners Hospitals for Children) for their consultation. Finally, we thank Humberto Gonzalez, PhD, for his technical guidance.
Key points
Developed a shoulder-controlled, externally powered, 3D-printed prosthetic arm. Significantly reduced cost compared to non 3D-printed devices. Expands Robohand patient population to those with transradial limb amputations. Prototype tested by 13-year-old female patient.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.