
Abstract
Background:
Osteogenesis imperfecta is an inherited disorder of the connective tissue characterized primarily by fractures with no or small causal antecedents and extremely variable clinical presentation. The disorder requires a global and, therefore, multidisciplinary therapeutic approach that should aim, among other aspects, at the prevention and treatment of deformities resulting from osteogenesis imperfecta. Due to limitations related to bony deformities, it can be difficult to place these infants in a variety of positions that would help remediate skull deformities, so a cranial orthosis becomes the therapy of choice. The aim of this study was to demonstrate the results obtained during treatment with a cranial remolding orthosis (helmet) in babies with osteogenesis imperfecta.
Case Description and Methods:
For the first time in the scientific literature, this study describes the use of a cranial orthosis for the treatment of infants with osteogenesis imperfecta. Both children had severe asymmetrical brachycephaly documented by laser digital scanning and were submitted to treatment with a cranial remolding orthosis.
Outcomes and Conclusion:
The study showed that there was a significant improvement in cranial proportion and symmetry, with a reduction in the cephalic index at reevaluation. It is concluded that the orthotic therapy is an effective therapeutic modality to improve the proportion and minimize the asymmetry in children with osteogenesis imperfecta.
Clinical relevance
The clinical relevance of such a description is that children with osteogenesis imperfecta may have numerous deformities and minimizing them can be an important factor. This report showed a beneficial result as the orthotic therapy modality improved the proportions and minimized the asymmetry. This treatment offers too high levels of satisfaction to parents and brings these children closer to normal indices.
Background
Osteogenesis imperfecta (OI) is an inherited disorder of the connective tissue, primarily characterized by fractures with no or small causal antecedents. Collagen fiber alterations are the basis of its physiopathology. Its frequency varies from 6 to 7:100,000 individuals in Brazil, and it is estimated that there are 12,000 individuals with this diagnosis according to De Lima and Horovitz. 1
Traditionally, the classification of this disorder has been subdivided into types I to IV by Sillence et al., 2 and more recently other types were added to this original classification as the disease has a very heterogeneous clinical presentation.2–4 Affected individuals are subject to spontaneous fractures or fractures occurring secondary to minimal trauma.3–6
Due to this variability, it is recommended that the approach to this disease be multidisciplinary. The non-surgical management of these children is mainly aimed at the prevention and treatment of fractures, contractures, and deformities; improving motor development, functional capacity, and mobility. 3
Due to frequent presentation of concomitant developmental delay, infants with OI remain in the supine position for long periods, which can lead to deformational brachycephaly. This deformity is commonly associated with OI and can further complicate the infant’s ability to roll and move.
Brachycephaly is a skull deformity characterized by occipital flattening that can occur symmetrically or asymmetrically. 7 In brachycephaly, the ratio between the head width and length (known as cephalic ratio, CR) is quite high.8–10
The factors that lead to the development of brachycephaly include sleeping in the supine position, remaining in the same position for a long period of time in the first months of life, and developmental delays, which cause babies to move less and thus may lead to cranial flattening. All these factors are associated in the baby with OI, favoring the development of positional brachycephaly in these children. 11 Parents of children with OI often seek out traditional therapies (physical therapy, hydrotherapy) to help improve their child’s motor development, but those treatments do not improve the deformity exhibited by the extremely wide and abnormal skull shape. Since repositioning and handling strategies are difficult with these babies due to their elevated fracture risk, cranial remolding orthoses are the treatment of choice.
The cranial orthosis therapy is safe and effective and does not interfere with the head circumference growth. 12 The aim of this study is to demonstrate the results obtained during treatment with a cranial remolding orthosis (helmet) in two babies with OI.
Case Descriptions, Methods, Findings and Outcomes
This is a retrospective study that analyzed the medical records of two patients with OI undergoing treatment with a cranial orthosis due to significant deformational brachycephaly. This study was approved by the Research Ethics Committee of Fundação José Luiz Egydio Setúbal/Hospital Infantil Sabará, and free and informed consent was obtained from the parents of the children undergoing treatment.
Case 1
GMCA is a 6-month-old female patient, born prematurely (34 weeks) resulting in a neonatal intensive care unit (NICU) stay for 1 week after birth. She had type III-IV OI with a history of intrauterine fractures and at 6 months of age was evaluated for her cranial asymmetry in a specialized clinic.
The patient was assessed by clinical examination, photographic record with a Nikon™ camera, and three-dimensional (3D) laser scanning using the STARscanner Acquisition System™ equipment (Orthomerica Inc., Orlando, FL). Physical examination showed significant flattening of the entire occipital region with no clinical evidence of craniosynostosis. The child was then diagnosed with severe asymmetrical brachycephaly. The scanning process used anatomical landmarks to determine a reference plane, from which the indices were calculated and measurements were obtained.
The data were analyzed by CCU software (Cranial Comparison Utility™) and sent electronically to Orthomerica Inc., where a mold was carved on a 3-axis carver that precisely matched child’s head shape and a correction of the cranial shape is precisely determined on the mold allowing the construction of the customized helmet (Starband® with ½″ pelite liner foam) already with the space for the corrected growth. The orthosis was fit 14 days after the initial assessment and the parents were instructed in the proper application and follow-up procedures. From the beginning to the end of treatment, nine follow-up visits were carried out. At each visit, adjustments were made to the inner liner of the orthosis to direct growth into the flattened quadrants.
We analyzed the clinical scan data acquired at the beginning and end of treatment and conducted a parental satisfaction assessment. The following variables were analyzed:
CR: Percentage obtained by dividing cranial width by length at level 3 (plane 3 cm above the anatomical reference plane).
Diagonal difference (cranial vault asymmetry (CVA)): The difference in mm between the oblique diagonals at 30°.
Cranial Vault Asymmetry Index (CVAI): The diagonal difference divided by the largest diagonal and expressed in percentage.13,14
Overall Symmetry Index (OSI): The mean value of the anterior and posterior symmetry ratio. A value equal to 1 represents perfect symmetry.7,13
Figure 1 illustrates the photographic records and comparative pictures of the initial and final scans. It is possible to visualize the flatness of the entire occipital region at the beginning of treatment, somewhat more pronounced to the right, as well as the clinical appearance improvement of this occipital flattening at the end of the treatment. This is also demonstrated by the 3D image, seen here on the right lateral position, obtained by laser digital scanning.
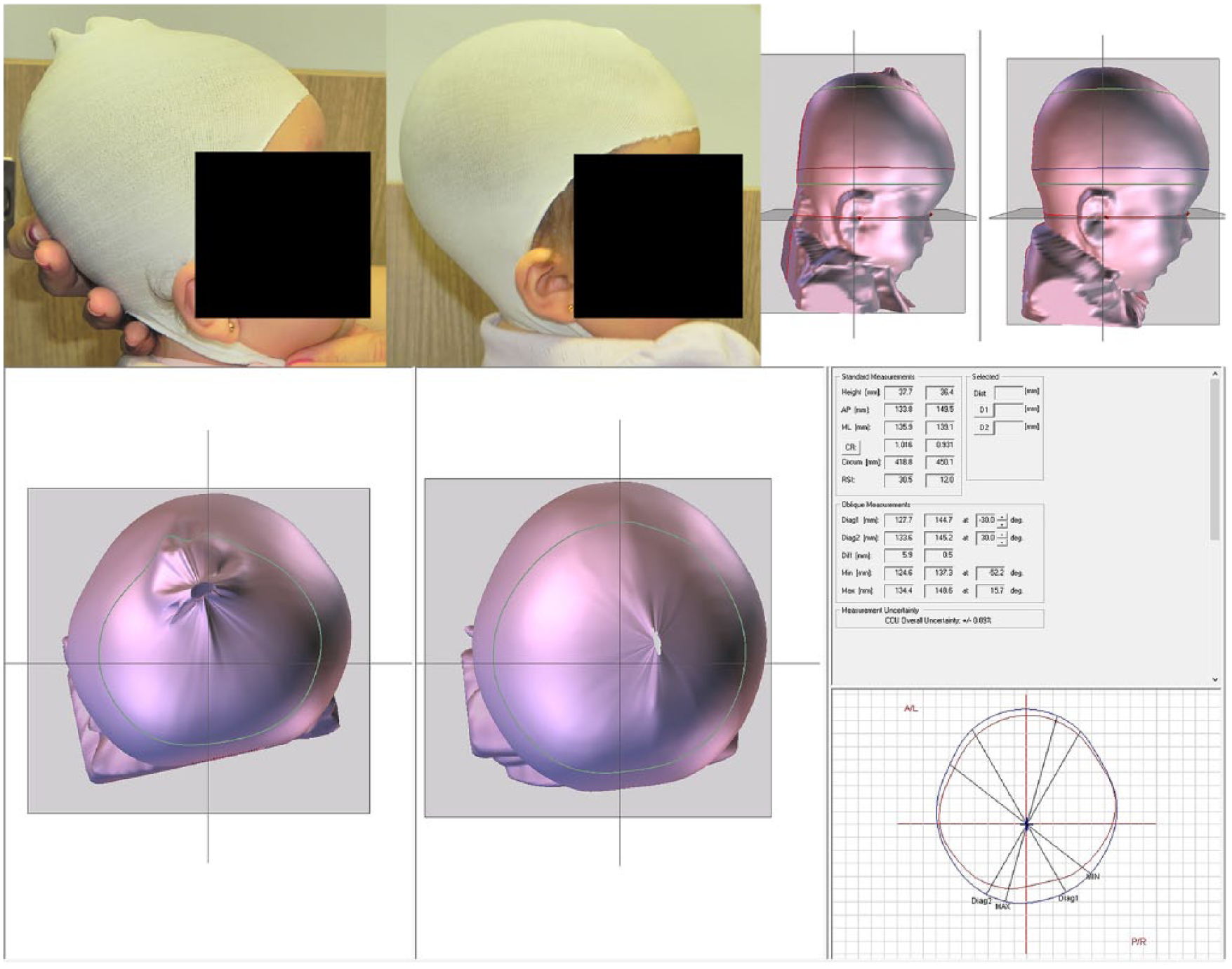
Images obtained before and after treatment with cranial orthosis in various views, showing posterior volume gain and simultaneous lateral-lateral growth inhibition with the use of the orthosis. One can also observe the increase in the degree of symmetry of one side in relation to the other, showing a more symmetrical skull.
After 4 months of orthotic treatment, the baby was reassessed. The rescanning image shows that there was an increment of head circumference from 418.8 to 450.1 mm. Growth was directed into the posterior quadrants during the treatment period, and posterior symmetry also improved, reducing the diagonal differences (CVA) from 5.9 to 0.5 mm. The skull proportion improved from 1.016 to 93.1, demonstrating a significant cosmetic improvement. The baby’s CVAI also showed improvement, from 4.5 to 0.3, and overall symmetry (OSI) increased from 0.915 to 0.973. At the end of treatment, all indexes moved toward more homogeneous and normal values.
Considering such gains, the parents were asked about their subjective impression of the asymmetry analysis before and after treatment. They were satisfied with the treatment and, if before the treatment they perceived their baby’s asymmetry as “severe,” after it they evaluated the baby’s skull shape as “no problem.”
It is important to report that during 4-month treatment, the mother followed the recommendations that the child should use the orthosis for 23 hours a day. Intermittent use was reported for a short time during the last 2 weeks of treatment because the baby had a tibial fracture and fever, requiring that the orthosis be removed during that period.
Case 2
MCFN, a 4-month-old male patient, was born at term. He had type III OI and suffered an occiput fracture during labor. He was assessed for cranial asymmetry in a specialized clinic. The parents’ complaint was the child’s significant flattening in the posterior region of the head.
The patient was evaluated through clinical examination, photographic record using a Nikon camera, and 3D laser scanning using Scanner Acquisition System equipment too.
The physical examination showed significant flattening of the entire posterior occipital region, also without any clinical evidence of craniosynostosis. The baby was diagnosed with severe symmetrical brachycephaly.
The scanning process used the same anatomical reference points described in the previous case and thus the data obtained and the manufacturing of the orthosis followed the same process (Starband with ½″ pelite liner foam). The orthosis treatment started 15 days after the clinical evaluation and initial scanning (period also related to the manufacturing and importation time). The initial adjustments were performed and the same recommendations were provided to the parents regarding orthosis use and hygiene. The child was seen at 2- to 3-week intervals at nine follow-up visits, and the orthosis was adjusted to direct growth into the posterior quadrants.
The same data as seen in the previous case were analyzed, obtained at the beginning and the end of treatment including the photographic record, parental satisfaction assessment, and scanning values.
Figure 2 shows the comparative images of the first and last 3D scans.
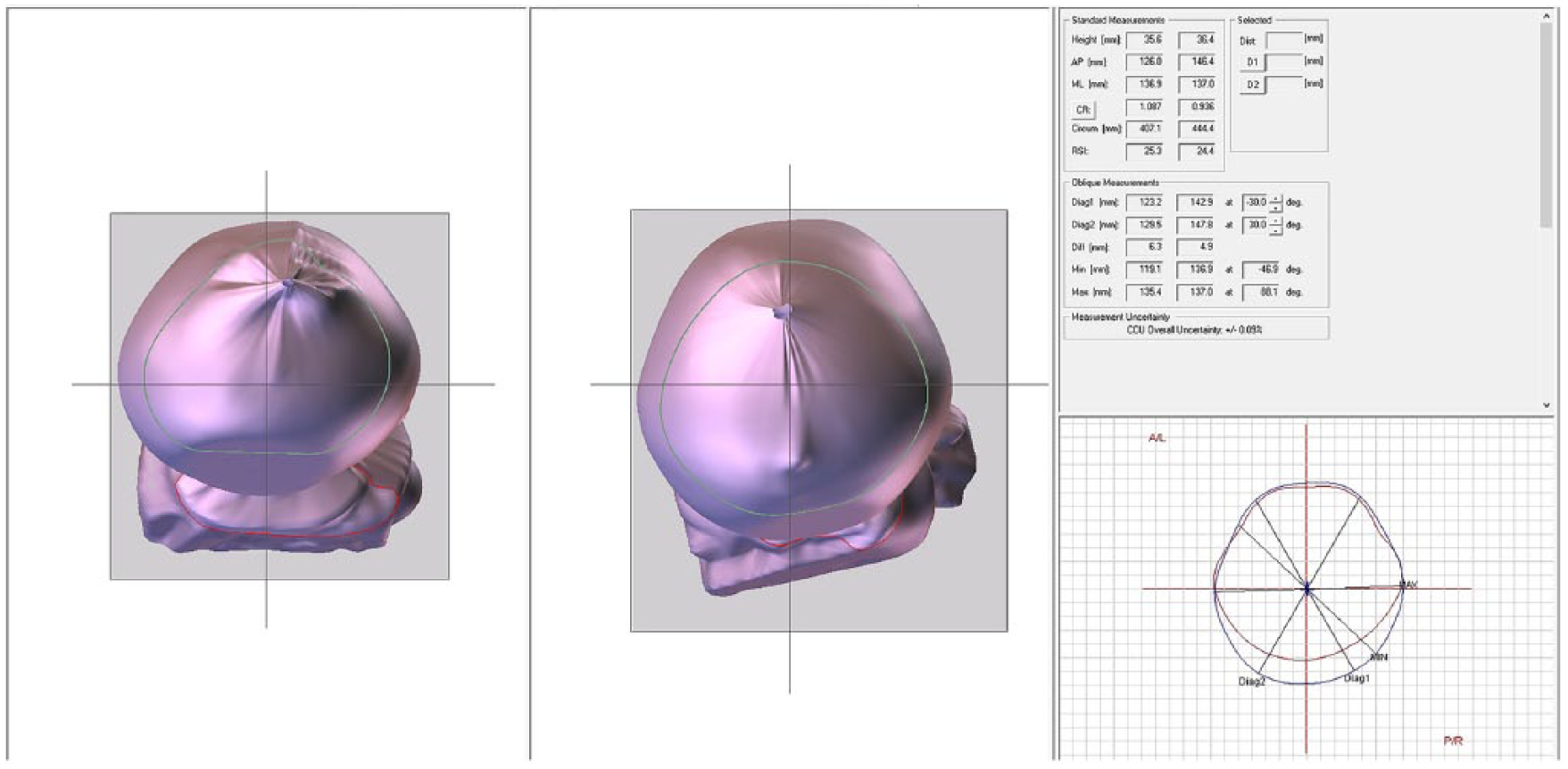
Image obtained before and after treatment with cranial orthosis.
After 6 months of orthotic treatment, the baby was reassessed, with visible results shown in Figure 2. The 3D scan shows normal cranial circumference growth from 407.11 to 444.4 mm. The child’s improvement in skull proportion is evident from the decrease in the CR from 1.087 to 0.936, CVA from 6.3 to 4.9, and CVAI from 4.8 to 3.3. Since the baby had bronchiolitis and some episodes of fever throughout the treatment requiring that the orthosis be removed, the treatment time was extended to 6 months to ensure the best possible outcome.
The parents were completely satisfied with the treatment. Prior to the treatment, the assessment indicated that they felt their child’s head shape was “severe.” Following treatment, they assessed the head shape as “no problem.”
Table 1 shows a summary of the achieved results.
Before and after treatment data.
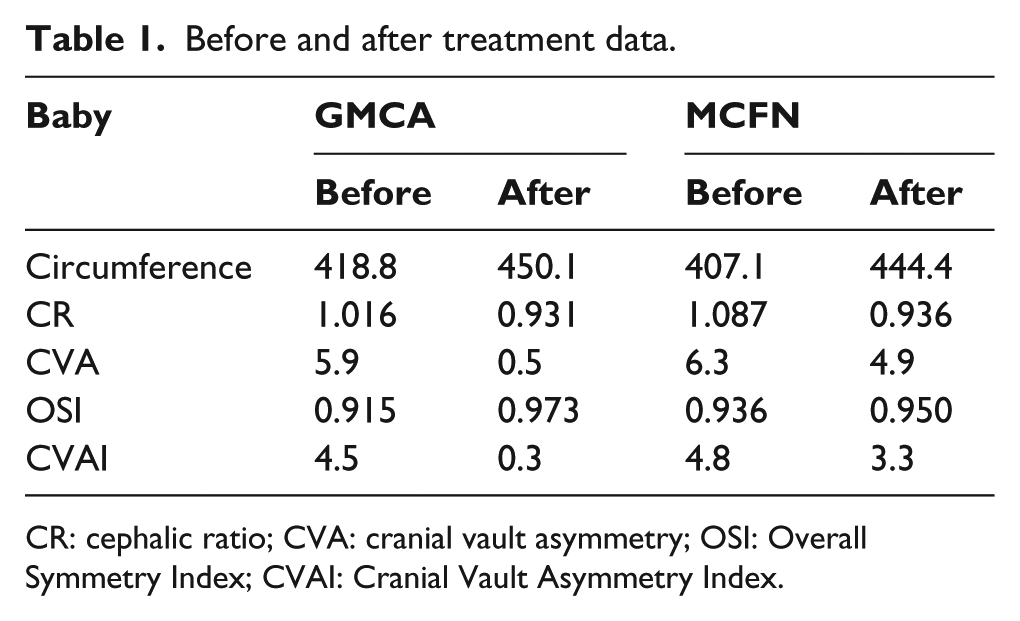
CR: cephalic ratio; CVA: cranial vault asymmetry; OSI: Overall Symmetry Index; CVAI: Cranial Vault Asymmetry Index.
Discussion and conclusion
This study sought to objectively (through laser digital scanning) and subjectively (through photos and parents’ evaluation) quantify the results of cranial remolding orthosis treatment for babies with OI. Although this is a report of only two cases, it is the first study in the international literature that demonstrates treatment outcomes for this patient population. The data obtained using the 3D laser scanning tool proved to be useful in accurately demonstrating skull shape changes throughout the treatment period, as has been reported previously in babies without OI. 13
Babies who sleep and spend much of their days in the supine position can develop a wider and shorter skull than those in whom positions are alternated. 15 Although positional brachycephaly is not a progressive disease, it can have a negative impact on the child’s physical appearance. Severe cases can cause serious emotional and psychological problems and affect patients’ self-image perception at several stages of their lives. Especially for children with OI, improvement in the skull proportions can minimize possible deficiencies that may remain with the baby throughout life, so it is important to consider such therapy.
In an effort to prevent sudden infant death and deformational head shape problems, pediatric societies have instructed parents to keep babies in the supine position to sleep and to encourage prone positioning when the baby is awake. 16 However, when one thinks about children with OI, this recommendation is almost unattainable as the baby will spend most of the first months in the supine position. Developmental delays coupled with the need for the extreme attention and care needed to manage and prevent fractures result in the child being in the supine position for several hours per day, extended over many months. During this time, a cranial remolding orthosis can help correct skull deformities and prevent the development of more severe deformation.
As shown by the results achieved, there was significant improvement in cranial symmetry documented mainly by the decrease in the CR.
The increase in volume of the entire posterior region of the skull area, where growth was desired to achieve a better head proportion in these babies, was observed in both babies and is shown in Figures 2 and 3. Furthermore, there was improvement in all symmetry indexes, especially in the first child, in whom the asymmetry was more significant and improvements were more marked.
Successful treatment with a cranial remolding orthosis is dependent on cranial growth, which is very rapid in the first year but particularly in the first 6 months of life. It is for this reason that most specialists recommend that the optimal time to start orthotic therapy is between 5 and 6 months of age. 17 Cranial treatment takes advantage of this dynamic growth period to direct skull growth into the flattened quadrants.
All indexes showed improvement, and these results were achieved due to the constant contraposition that the orthosis caused to the prominent parietal regions, where growth was not desired, while providing, at the same time, free space for the flattened regions to reach the desired growth. Therefore, the orthosis directed and shaped the natural growth of the baby’s skull. The improvements in the second infant with respect to symmetry were below those observed in the first. The frequent interruptions to treatment provide a plausible (and likely) reason for this disparity.
Other studies have shown significant cranial symmetry gain with the orthotic therapy. Mulliken et al. 14 concluded that therapy with the helmet resulted in a statistically significant reduction in cranial symmetry index when compared to active repositioning. Graham et al. 18 also compared repositioning to the orthotic therapy and found 61% reduction in CVA, while the repositioning resulted in 52%. The biggest challenge, however, in infants with OI would be the great difficulty in performing the repositioning and the “tummy time” strategy due to bone fragility as previously emphasized. It is important to note that for these children, the band did not impair movement or activities in any way and may also have served as protection for the baby’s fragile skull.
A limitation of our study lies in the fact that only two cases are being reported, but no study in the international medical literature has documented the results of this therapy in babies with severe brachycephaly associated with OI. It is important, therefore, to present the results that have been achieved in clinical practice, as there are no data yet concerning this type of treatment for this population. It is within this context that the reporting of these cases becomes important. We hope that our study will serve to stimulate the scientific study and research on these children, which is presently so scarce. While our study shows that cranial remolding orthoses are effective in reducing skull deformities in babies with OI, clinical trials and studies with larger sample sizes should be a priority.
The treatment of this disease requires the joint efforts of parents, pediatricians, specialists, and therapists, especially when asymmetry is present. They must assess the baby’s skull shape early in life, in an attempt to minimize the consequences of inadequate treatment.
As reported, the parents were satisfied with the orthotic treatment results. In addition to the acquisition of anthropometric data that allow the documentation of the measurements obtained with treatment, some authors have also discussed the importance of measuring the parents’ perception of the performed treatment. Most studies do not depict the association of anthropometric data with parental perception data and/or different tools that were used for such assessment.19,20 Clinically, the personal relationship of parents with the treatment may affect treatment compliance and continuity. Thus, the study of the parents’ reaction, even if performed subjectively, provides parameters about care that must be provided to families. This study demonstrated that the parents observed the correction to the point of describing the head size of their babies as “no problem.” This finding should not be neglected, and clinicians should aim to understand the needs of these families, which goes beyond the simple pursuit of morphological regularity. The treatment of one’s child can be a deep and remarkable emotional experience, especially when the baby has several deformities. Thus, the parents’ perception should always be the object of investigation. 21
We conclude that the orthotic therapy is an effective therapeutic modality to improve the proportions and minimize the asymmetry in children with OI. This treatment offers high levels of satisfaction to parents and brings these children closer to normal indices. The unquestionable improvement in skull appearance is documented through 3D digital laser scanning, an important tool that allows an objective, 3D cranial asymmetry assessment. We reinforce the need for studies that will statistically document the results seen with this treatment, comparing it to other therapeutic modalities.
Footnotes
Author contribution
Carolina Gomes Matarazzo conceptualized and designed the study, drafted the initial manuscript, and approved the final manuscript as submitted.
Gerd Schreen: critically reviewed and revised the manuscript, and approved the final manuscript as submitted.
Camilla Domingues do Lago-Rizardi contributed to the translation and study images design and approved the final manuscript as submitted.
Maria Stella Peccin critically reviewed the manuscript, and approved the final manuscript as submitted.
Fernando Campos Gomes Pinto critically reviewed the manuscript, and approved the final manuscript as submitted.
All authors approved the final manuscript as submitted.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Research Ethics Committee of Fundação José Luiz Egydio Setúbal/Hospital Infantil Sabará, and free and informed consent was obtained from the parents of the children undergoing treatment.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.