
Abstract
Background:
To overcome the challenges of rehabilitation of bilateral transfemoral amputees, we developed a novel “hip prosthesis in the sitting posture.”
Case Description and Methods:
A 64-year-old male bilateral transfemoral amputee was transferred for rehabilitation 4 months following a burn injury. His wounds remained unhealed for 20 months; thus, he was unable to participate in standing training with the standard prosthetic sockets. Hip prosthesis in the sitting posture has very little friction between the sockets and residual limbs, which facilitated our patient to begin standing and walking exercises.
Findings and Outcomes:
The patient’s refractory wounds healed 1 month after initiating exercises using hip prosthesis in the sitting posture, and he could begin rehabilitation with the standard prostheses.
Discussion and Conclusion:
Hip prosthesis in the sitting posture enabled a bilateral transfemoral amputee with unhealed residual limbs to stand, walk, and begin balance training. Hip prosthesis in the sitting posture is an effective temporary prosthesis to prevent disuse until wounds are healed and to continue rehabilitation with standard prostheses.
Clinical relevance
Hip prosthesis in the sitting posture is useful for bilateral transfemoral amputees with unhealed residual limbs after burn injuries to prevent disuse and maintain motivation for walking.
Keywords
Background
Rehabilitation of bilateral transfemoral amputees is challenging, and resumption of walking ability is difficult in these cases.1–8 The prognosis is particularly poor with respect not only to function but also to the quality of life of patients with bilateral lower amputations because of the risk of peripheral arterial disease. 7 Moreover, amputation after a burn injury is of clinical concern because the fragile skin of the residual limbs is prone to bruising due to friction between the residual limbs and sockets. Therefore, it is difficult to adapt a residual limb to a prosthetic socket following amputation due to a burn injury.9–12 The poor prognosis of function and daily activities is not only due to the severity of underlying diseases but also to disuse after amputation. Therefore, we developed a novel “hip prosthesis in sitting posture (HPSP)” for the rehabilitation of a bilateral femoral amputee after a burn injury, for whom it was impossible to engage in standing and walking training without prostheses. The sockets of current standard types of prostheses are unsuitable for unhealed residual limbs. The purpose of HPSP was to enable a bilateral transfemoral amputee to perform standing, walking, upper arm, trunk, and balance training even with unhealed residual limbs to prevent disuse after amputation.
Case description and methods
The study protocol was approved by the Human Ethics Review Committee of Ibaraki Prefectural University of Health Sciences (H28-63, Ami, Japan), and the patient provided informed consent for the publication of this report. A 64-year-old man was transferred to our hospital for rehabilitation with the hope of gaining the ability to walk with bilateral leg prostheses. Four months before admission, he suffered third-degree burns to 40% of the body, which included the buttock, right abdomen, part of the back, and bilateral calves. He was transported to an emergency hospital and underwent relaxation incisions. Furthermore, he underwent split-thickness skin grafting from the back to the bilateral thighs at 3 days after the burn injury and bilateral femoral amputation at 1 month after the burn injury. A second split-thickness skin graft from the back to the bilateral thighs was performed at 2.5 months after the burn injury.
On admission, his bilateral femoral residual limbs were immature, column-shaped, and edematous. The length from the ischial tuberosity to the end of the residual limbs was 25 cm (right) and 28 cm (left). His residual limbs were unhealed, and most of the back skin was scarred. His active range of motion of the left shoulder was restricted by 40° (passive range was 160°), 160° of right active range of motion, and bilateral hip flexion range of motion was 90°, and extension was 0°. Manual muscle test (MMT) results were 2 of 5 for the upper left extremity, 4 of 5 for the upper right extremity, and 4 of 5 for both lower extremities. The patient had a 10-year history of noninsulin-dependent diabetes mellitus. Diabetic control was fair with a dipeptidyl peptidase-4 inhibitor. Fasting blood sugar level was 120 mg/dL and HbA1c (National Glycohemoglobin Standardization Program (NGSP)) was 6.0%.
At 1 month after admission (4 months after the burn injury, 3 months after bilateral transfemoral amputation), he was restricted to a wheelchair to prevent his wounds from worsening. He was rehabilitated bedside and underwent muscle and range of motion exercises using a stretcher as a transportation device.
At 3 months after admission (7 months after the burn injury, 6 months after amputation), he started to use a wheelchair for 30 min a day. Transfers between the wheelchair and bed were difficult because of muscle weakness in his left hand. Cervical laminoplasty was performed for myelopathy after his wound improved enough to hold a prone position with a mild hip flexion during the operation. Postoperatively, muscle strength of the bilateral upper extremities improved to 4 of 5, and he was almost able to transfer himself from a bed to a wheelchair. Moreover, he applied for public care insurance for house renovations to eliminate the difference in floor levels, and an elevator was installed to help him enter his house.
At 7 months after admission (11 months after the burn injury, 10 months after amputation), he gained the ability to live at home with a wheelchair and was, therefore, discharged from the hospital, although there were some 1- to 2-cm unhealed wounds.
Findings and outcomes
At 9 months after discharge (20 months after the burn injury, 19 months after amputation), his wounds were not completely healed. Nevertheless, he still hoped to be able to walk with the prostheses, and he was re-admitted. However, using the standard prostheses would have made his still unhealed wounds worse because of friction between the residual limbs and prosthetic sockets. Therefore, we considered that a novel socket, used in the sitting position, would be effective for someone with unhealed bilateral lower thigh residual limbs, and thus, we developed HPSP (Figure 1(a)). The socket was cast with the patient in a sitting position and included a pelvis portion and bilateral thigh parts as a unit with attached hip joints, knee joints, support pillars, and foot parts (Figure 1(b)). The bench alignment of this prosthesis was as follows: both prosthetic hip joints were placed under the center of the hip joints of the patient so that the gravity line of the pillars passed from the hip joints to the center between the toe break and heel. We attached a suspension belt to support the pelvis and two types of ready-made knee joints and ready-made prosthetic feet. We used one type of ready-made knee joints (modular lightweight single axis knee joint with a lock, 3R40; Otto Bock HealthCare Deutschland GmbH, Ottobock, Germany) for hip joints, which were placed in an inverted position for the user to be able to sit while wearing the prostheses. Moreover, we used other ready-made knee joints (multilink safety knee; SwanS; Imasen Engineering Corporation, Kakamigahara, Japan) and ready-made energy-storing prosthetic feet (1C40; Otto Bock HealthCare Deutschland GmbH). However, those ready-made parts of prostheses can be substituted for similar parts.
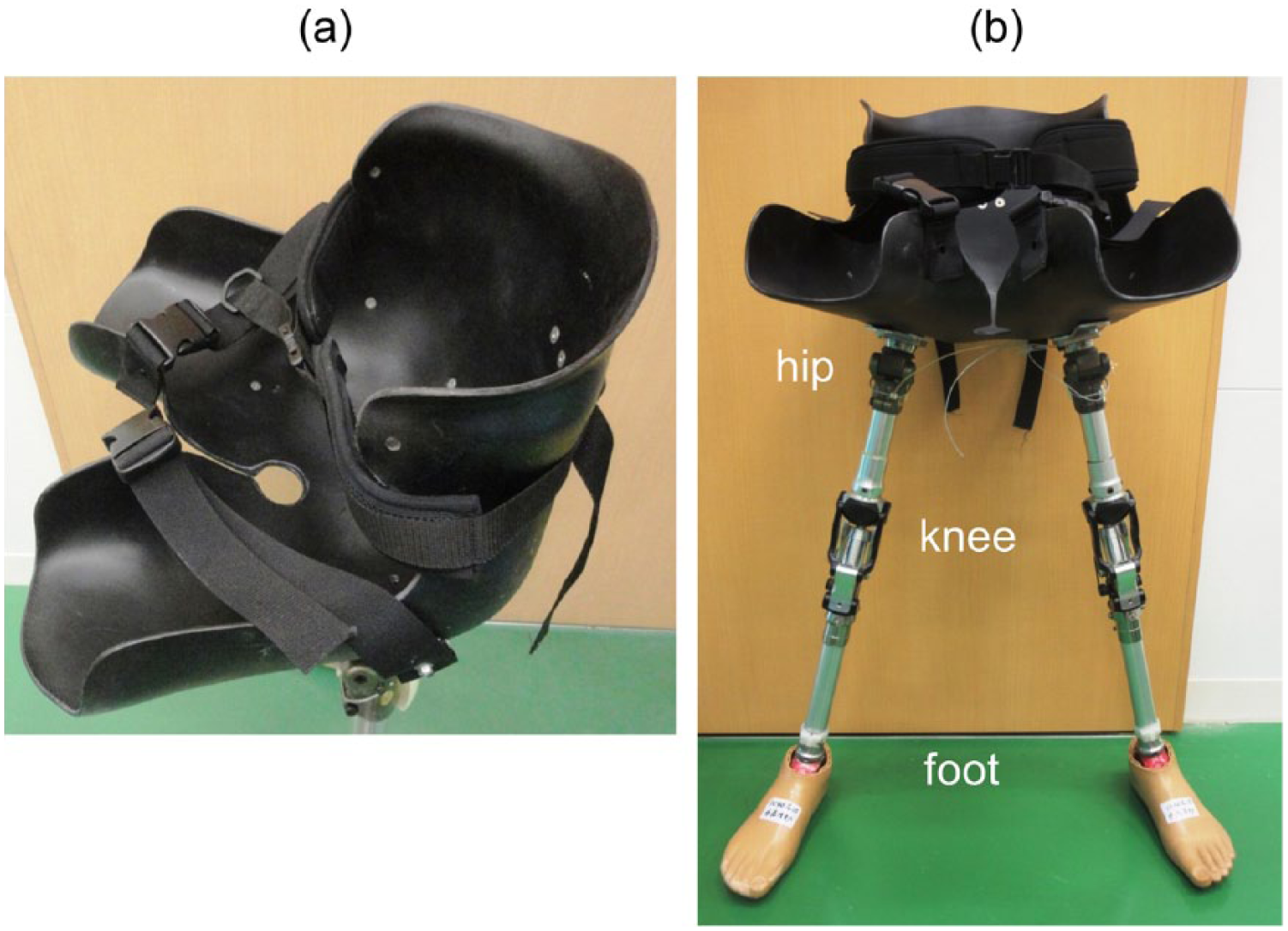
(a) The socket of the “hip prosthesis in sitting posture” (HPSP) comprises a pelvis part and bilateral thigh parts as a unit and (b) ready-made hip joints, knee joint, support pillars, and foot parts under the socket.
The patient began rehabilitation for standing with this prosthesis using parallel bars (Figure 2), at first with total assistance from a physiotherapist. Later, he was able to walk using a parallel bar or a walker. At the early stage of using HPSP, his trunk was bent forward and required total assistance from a physiotherapist. However, the trunk position improved with a little assistance, and the muscle strength of his upper extremities also improved. MMT of the bilateral upper extremities improved from 4 of 5 before HPSP exercise to 5 of 5 one month after beginning HPSP exercise, and the effort of the upper extremities during walking with HPSP reduced. In addition, during HPSP walking, his bilateral hips were flexed, although HPSP did not restrict the range of hip extension. After 1 month, he began to use HPSP, and his wounds finally healed 22 months after the burn injury.

Standing with HPSP.
The patient began to use plug-fit sockets with short stubby pillars (Figure 3(a)) and suspension belts. However, the upper femoral wounds became irritated by friction with the socket; therefore, the plug-fit socket was discontinued, and HPSP was used for 1 month until his wounds healed, which completely healed by 2 months. The sockets were changed from the plug-fit to a silicone liner type. We initially presumed that silicone liners might worsen his wounds; however, once healed, the residual limbs remained in good condition.
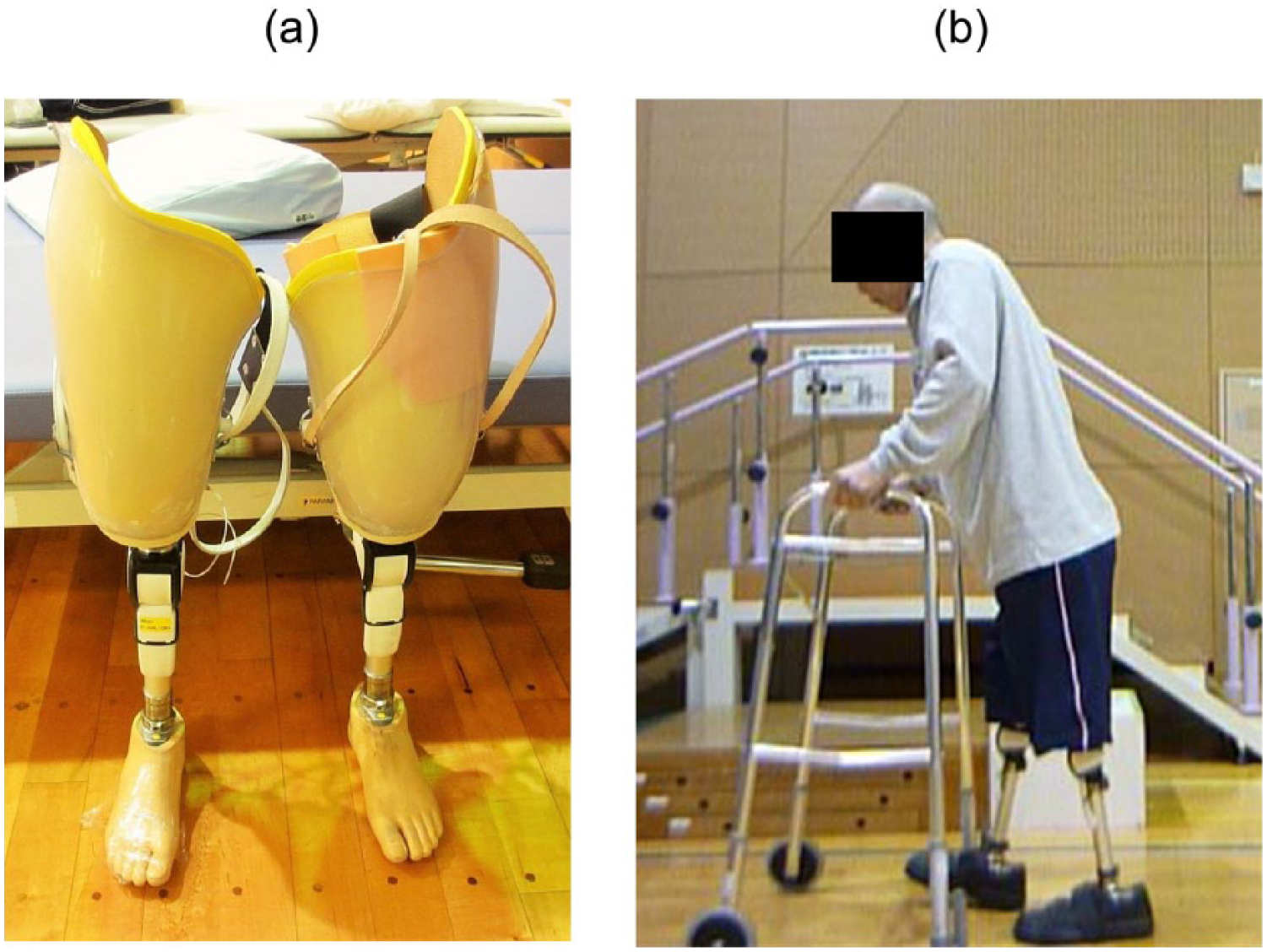
(a) Prostheses of stubby type and (b) walking with a walker and bilateral femoral prostheses on his own.
The patient was able to walk with standard prostheses and a walker (Figure 3(b)) at the end of the second hospitalization at 26 months after the burn injury. At that time, his diabetic control had improved using the same prescription: fasting blood sugar level of 104 mg/dL and HbA1c (NGSP) of 5.8%. At 36 months after the burn injury, although he also used a wheelchair, the patient was able to walk around his home with his standard prostheses and a walker.
Discussion and conclusion
Our patient had two main problems: bilateral femoral amputation and refractory wounds after a burn with controlled diabetic mellitus. Although rehabilitation would be difficult for him for both reasons, he was able to be rehabilitated with the use of HPSP and finally regained household ambulation. HPSP is not a socket closely attached to residual limbs; therefore, it can be used for immature or unhealed wounds. Because HPSP produces less friction between the unhealed residual limb and socket, the wound healed in a relatively short time. Standing with HPSP not only requires muscle strength of the upper limbs and trunk but also requires postural balance function, although balance training is difficult for bilateral amputees.
This patient required 22 months for healing of his wounds. This long healing time might have been because of diabetes. Bilateral above-knee amputees because of dysvascular disease have poor prognosis of function and quality of life.1–8,13 We presume that not only physical condition and cardiopulmonary dysfunction from arteriosclerosis but also disuse after amputation, such as due to muscle atrophy, cardiorespiratory depression, and balance dysfunction, are related to this poor prognosis. Using HPSP may reduce disuse syndrome, increase motivation of amputees for rehabilitation, enable future prosthetic rehabilitation, and increase the quality of life of bilateral amputees. Our patient hoped to be able to walk with the prostheses at 20 months after the burn injury. Brown 2 concluded that motivation was an important factor.
Prosthetic rehabilitation is challenging for bilateral transfemoral amputees, and regaining walking ability is reportedly difficult.1 –8,13 It is much more difficult for amputees with dysvascular diseases than those with trauma to regain walking ability (success rates 0% and 54.5%–84.9%, respectively). Bilateral lower limb amputation in patients with dysvascular disease has a particularly poor prognosis of not only function but also the quality of life. Inderbitzi et al. 7 reported mortality rates in patients with peripheral arterial disease following bilateral amputation of 38% after 2 years and 69% after 5 years. Our patient was elderly and had diabetes mellitus and refractory wounds to the residual limbs. Therefore, it is difficult to compare our case to bilateral amputees with dysvascular diseases. Furthermore, prosthetic rehabilitation is challenging for amputees after a burn injury because it is difficult to adapt the fragile skin of the residual limbs to a prosthetic socket.9–12 Furthermore, there is a risk of carcinoma formation in amputation of residual limbs. 11 Staley and Richard 14 reported that burn treatment for the elderly must consider the physiological and physical conditions of the patient; 14 thus, it is important that elderly patients with burn injuries improve balance.
Regaining the ability to walk is a severe problem for bilateral transfemoral amputees because of many clinical concerns, such as wound problems, muscle atrophy, balance dysfunction, and energy consumption. 8 However, with the use of HPSP, bilateral amputees can perform sufficient exercise to improve muscle strength to regain the ability to walk, perform balance training without leading to further complications in unhealed wounds, and be motivated to walk with a prosthesis. HPSP is an effective temporary prosthesis for continued rehabilitation to regain the ability to walk with standard prostheses.
In conclusion, we treated a bilateral transfemoral amputee after a burn injury using a novel HPSP. He used this prosthesis for walking training, except during a period when his unhealed wounds worsened, and he was finally able to regain household ambulation. HPSP can be an effective tool for the rehabilitation of bilateral lower leg amputees whose wounds are difficult to heal after a burn injury.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.