
Abstract
Nail bed injuries were commonly found concomitantly with fingertip injuries. Reconstruction of fingertip including the nail bed should be attempted at acute stage. Aim of the surgery was to restore as much finger length and achieve normal nail growth. In chemical burns, the initial presentation might not reflect the exact extent of injury. Appropriate acute management must be initiated while waiting for demarcation. We report a case of young stewardess who presented with fingertip chemical burn injury. Surgical debridement was done on third day post-injury. A cross-finger flap to cover skin defect and split-thickness nail bed grafting from the remnant of injured finger were done. Excellent functional and cosmetic outcome was achieved in 6 months. Surgical treatment in a chemical burn was similar to traumatic injury. Nail bed graft was the best option for nail bed reconstruction. In cases of soft tissue loss, advancement or pedicle flaps are beneficial.
Background
Nail bed injuries were usually found concomitantly present with fingertip injuries. 1,2 Convenient management was always refashioning or amputation. Little importance was given for reconstruction surgery for fingertip considering time consumption, cost and technical demands. However, the morbidity could be devastating cosmetically and functionally. Without nail, it is cumbersome to pick up small objects 3,4 as nail provides counter-pressure for pulp. 4
Fingertip injuries were commonly associated with industrial mishaps including crush injuries or burns. 5 In children, the injuries were frequently due to door crush. 5 –7 Chemical burn injuries at fingertips were rarely reported in literatures. The commonest chemical used in industries was hydrofluoric acid, the strongest inorganic acid which is also corrosive. 8 –10 In different concentrations, they were used in electropolishing metal, removing rust from fabrics and cleaning bricks, stone, iron and steel. 8,9 The hydrofluoric acid burn has a unique feature where the patients would suffer from severe excruciating pain and the tissue destruction could be deep 11 involving bone. 8,9 This was due to the free fluoride ions which are capable of penetrating quickly and destroying the tissues. 8 It disrupts the calcium-related processes at cell membrane level causing nerve stimulations that exaggerate pain. 8,11
In acute injury, it was recommended to cleanse the skin and apply topical calcium or magnesium salts or inject calcium gluconate locally. 8,12 The calcium gluconate or magnesium sulphate forms chelation with fluoride ions. 8,10 Hence, it reduces the pain and improves the burn lesion. 11 Even though acute management was prompt, necrosis of tissues still could occur. Fingertip necrosis is best treated surgically. There was no case reported which had been surgically treated for chemical burn at fingertip. There was case reviews reported on fingertip and nail bed reconstructions in traumatic injuries.
The ideal aim in management of fingertip traumatic injury was to restore the length of finger, obtain painless and sensate tip with normal nail growth. 5 Replantations of fingertips were not always possible; it depends on the severity of the injury and the availability of experts. In these cases, soft tissue coverage with flaps and nail bed reconstruction would offer good outcome.
With advancement of medical care, more reconstruction surgeries were attempted at initial presentation. Surgeons preferred thorough debridement and early coverage of fingertips. Options for soft tissue coverage were advancement flaps or pedicle flaps, 3,5,7,13 digital island flap, groin flap or even free flap from toes. 6 Early repair or reconstruction of nail beds in acute injuries had better outcome compared to chronic nail deformities. 1,4
Nail bed is a highly specialized tissue where replacement with other tissues results in inconsistent outcome. 4,5,7,14 For example, split-thickness skin grafts and dermal grafts caused non-adherence of nail plate. 14 This was cosmetically unpleasant and functionally unhygienic. 2,15 Best option for replacement was nail bed graft including both split-thickness nail bed graft (STNBG) and full-thickness nail bed graft (FTNBG). STNBG could be harvested from toes or the residual nail bed of the injured finger stump. FTNBG was better harvested from the amputated fingertip (if the patient brought the part) or toes as it has 100% donor site morbidity. 16
Case report
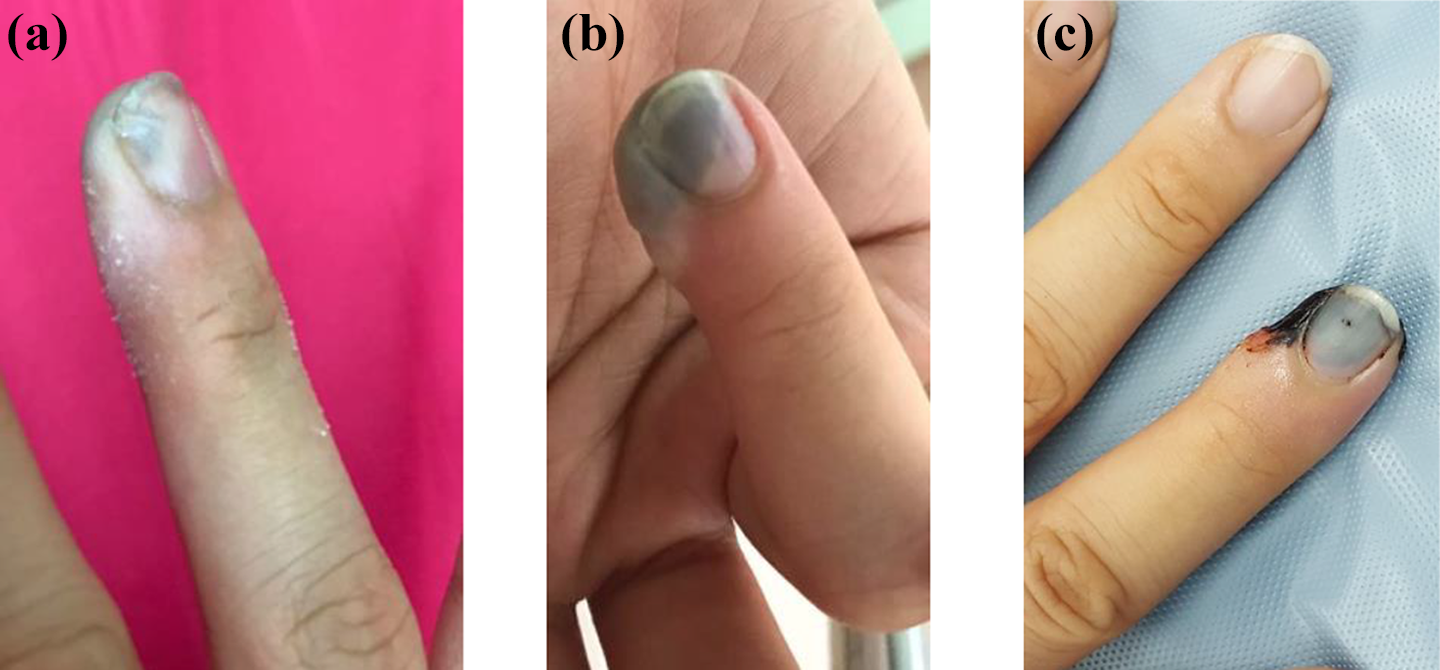
A 25-year-old stewardess presented with chemical burn injury of her right ring finger. She is right hand dominant. She was helping her father to carry a small bucket of acid which was used in cleaning gold. A drop of the chemical penetrated her wool glove and burnt her fingertip. She immediately immersed her right hand into cold water. She claimed that the fingertip was very painful with stinging sensation (Figures 1(a) and 2(a)). On day 2 post-injury, there was blister formation over the pulp of the right ring finger with a severe constant burning pain (Figures 1(b) and 2(b)). The pain had been gradually worsening. Thus, she presented to our Emergency Unit.

Appearance of right ring finger pulp on day 1 (a), day 2 (b) and day 3 (c) of chemical burn injury.
Dorsal appearance of right ring finger tip on day 1(a), day 2 (b) and day 3 (c).
Upon inspection, there was blister at the whole pulp including the radial half of distal phalanx with discoloration at radial half of nail bed. She claimed that the injury worsened with time and worried it will progress further. We intermittently soaked her fingertip in cold water. The blister was removed. Necrotic skin noticed under the blister (Figures 1(c) and 2(c)).
Wound debrided and nail plate removed. Radial half of the pulp and nail bed was necrosed. Distal phalanx was exposed after thorough debridement. Cross-finger flap with the middle finger was performed to cover the pulp defect. Nail bed defect was covered with STNBG obtained from the same 50% remnant healthy nail bed. Graft was harvested as thin and uniform as possible; free hand with a scalpel (size 11) under magnification. Nail plate was re-applied and bandaged. Wound was inspected weekly and dressing changed (Figure 3). Separation of finger was done on the third week. The uptake of nail bed graft was 100%.
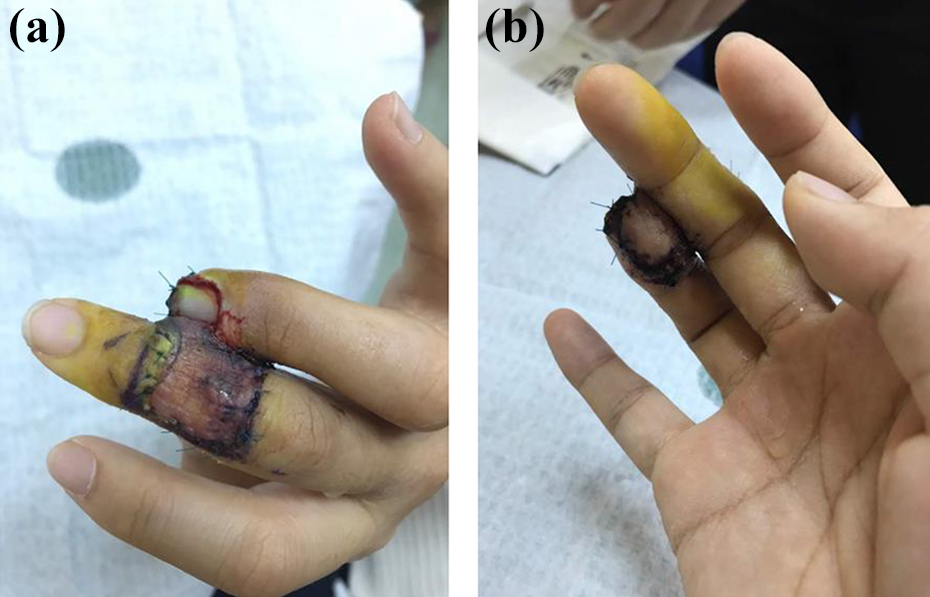
(a and b) Cross-finger flap from middle finger and STNBG from the remnant nail bed of the injured ring finger at 2 weeks after surgery. Nail bed was covered with the same nail plate after trimming the distal end.
Within 3 months, wound healed well (Figure 4(a) and (b)) and she returned to work. Range of motions of fingers was full. Sensation at flap site was intact with two-point discrimination of 6 mm. Tip-to-tip pinch grip was good. Nail appearance was normal with full adherence (Figure 4(c)). Morbidity of donor sites neither skin nor nail bed was absent. There was neither cold intolerance nor hypersensitivity of fingertip.
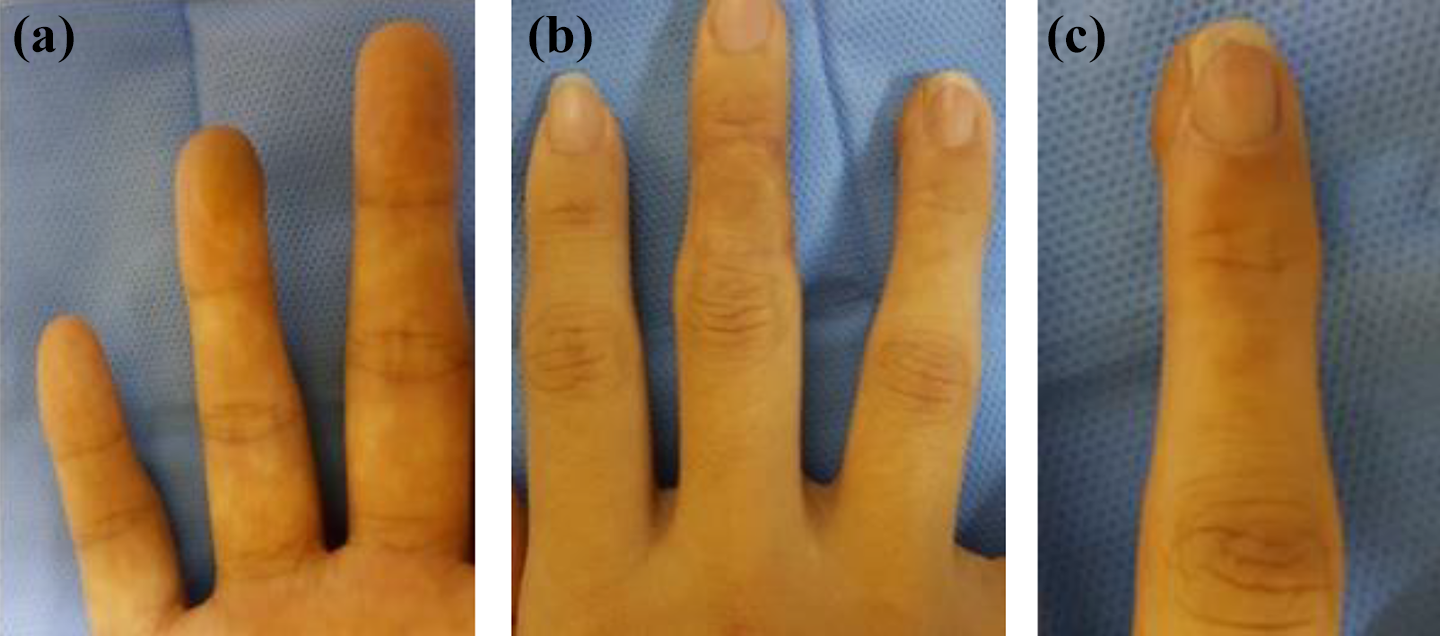
Appearance of donor and recipient of cross-finger flap (a and b) and normal nail appearance with complete adherence of nail (c).
Case review
Literature search was done for acute nail bed injuries. We found seven literatures reported on acute management with various nail bed grafts (Table 1). All reported series of cases; Shepard had the largest series of 48 patients. 14 One patient from Saito et al.’s 13 study and 10 patients from Clayburgh et al.’s 1 study were excluded as they had secondary reconstructions for chronic nail deformities. All patients were treated surgically within 4 days of trauma. Two studies, Hsieh et al. 4 and Clayburgh et al., 1 reported on isolated nail bed injuries, whereas the other studies included patients with concomitant pulp or soft tissue injuries.
Summary of the total acute fingertip injuries reported and their definitive reconstructive surgeries.
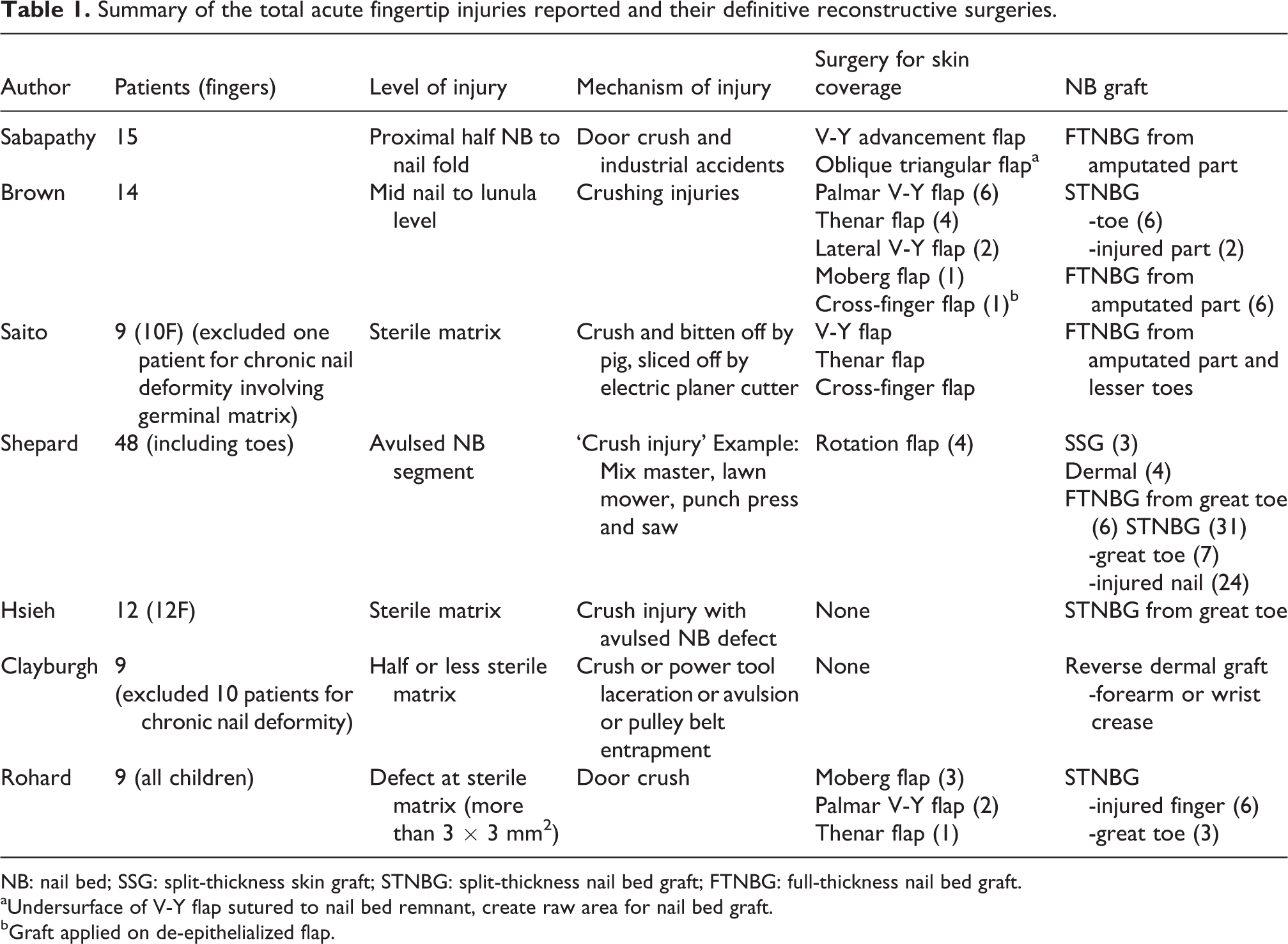
NB: nail bed; SSG: split-thickness skin graft; STNBG: split-thickness nail bed graft; FTNBG: full-thickness nail bed graft.
aUndersurface of V-Y flap sutured to nail bed remnant, create raw area for nail bed graft.
bGraft applied on de-epithelialized flap.
Most of the patients were adults and experienced crushed injury of their fingers. Rohard et al. reported on nine children, aged up to 16 years and most of them had door crush injuries. 7 All the authors reported on sterile matrix injuries where some of them graded the levels. 5,13 All of them agreed that injury to germinal matrix has poor outcome even after nail bed grafting.
Preferred soft tissue coverages by four authors were either advancement flaps like V-Y flap in fingers and Moberg flap in thumbs or pedicle flaps like thenar flap and cross-finger flap. Shepard performed four rotation flaps in their series. 14 All flaps were successful with good cosmetic outcome. Brown et al. reported a case of partial loss of flap which healed well eventually. 3 For nail bed defects, all authors recommended STNBG as the best option for best functional and cosmetic outcome with least morbidity. Donors for STNBG could be from the healthy remnant of injured nail bed or great toe. In cases where the patients bring along the amputated fingers which were not suitable for replantation, best option was FTNBG from the amputated part. All authors had excellent outcome with nail bed grafting at sterile matrix (Table 2). Sabapathy et al. and Rohard et al. reported hook nail deformities in cases of inadequate length of distal phalanges. 5,7
Outcome and complication of reconstructive surgeries performed for acute NB injuries with or without concomitant pulp loss.

SSG: split-thickness skin graft; STNBG: split-thickness nail bed graft; FTNBG: full-thickness nail bed graft
aPatient satisfaction + author’s assessment.
bAuthor’s assessment of surgical outcome.
cPatient satisfaction.
Discussion
Fingertip injuries commonly involved soft tissue and nail bed. In severe crush injuries, both structures need to be considered for reconstruction. The aim of management was to obtain painless sensate fingertip, normal nail growth and maintain length of finger. 5,6
In our patient, the mechanism of injury was chemical burn. We suspected hydrofluoric acid burn in view of the severe pain and deep tissue destruction. Furthermore, it is frequently being used in industries of metal cleaning. For acute management, some literatures recommended topical calcium salts, 8,11 local injection 8,11,12 or intravenous calcium gluconate. 10 Vance et al. reported that intra-arterial calcium infusion had excellent pain relief and marked improvement of the injury. 11 In fingers, this method was beneficial as we could avoid removal of nail and painful local injection of calcium. 11 We did not administer calcium gluconate in our patient as we were unaware of the exact acid substance. Constant immersion in water was done as we believed it would aid in dilution of the acid and might minimize the progression of injury.
High index of suspicion for a deeper soft tissue necrosis was anticipated. We noticed that there was vast difference in the appearance of the lesion between day 1 and day 2. Thus, we waited another day for demarcation and decided to debride and reconstruct on day 3. Intra-operatively, we identified skin and pulp necrosis at radial half of right ring finger with 50% nail bed involvement.
There was neither surgical treatment nor reconstruction of fingertips for chemical burns were reported in literatures. We chose cross-finger flap from middle finger as the lesion was at palmar-radial aspect (lateral oblique). STNBG was obtained from the remnant of injured nail bed as the size was adequate to cover the defect.
Many informative surgical techniques were described by all authors. Shepard emphasized the importance of microscopic assessment of the injured nail bed. 14 In partial thickness loss, grafting was not necessary as the nail could heal and grow normally. 4,14 Placement of nail bed grafts on de-epithelialized flap has excellent graft take. 3 Sabapathy et al. created a raw area for nail bed graft placement by suturing the under surface of flap to nail bed remnant. 5 Rohard et al. described nail bed reconstruction in paediatric group. 7 They emphasized that the nail plate is pliable that it can be bent to elevate for STNBG harvest. Complete removal of nail plate is unnecessary. The possibility of obtaining thick nail bed graft is low as the nail beds are generally thicker in children.
The assessment of surgical outcome was too subjective. Some authors only assessed the outcome appearance of finger and nail without considering the patient’s opinion. 4,13,14 Clayburgh et al. and Rohard et al. introduced scoring systems which included the surgeon’s assessment and patient’s satisfaction level. 1,7 Even these objective assessments did not include the function of the fingers like motion and pinch strength. All of them assessed the cosmetic aspect of the nail, for example, irregularity, adherence and splitting.
Conclusion
Initial presentation of chemical burns does not show the true extent of its injury. High index of suspicion for severe tissue necrosis must be anticipated. Thorough debridement and reconstruction of pulp including the nail bed is the mainstay of treatment. Delayed surgery to observe for demarcation is an option, provided an appropriate early treatment is carried out.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.