
Abstract
Background and Aim:
Three-dimensional printer is widely used in industry, biology, and medical fields. We report a finger prosthesis produced by a three-dimensional scanner and printer for a 67-year-old man with a right thumb amputation above the metacarpophalangeal joint.
Technique:
His right amputated and left intact hands were scanned with a three-dimensional scanner, and the left-hand image was rotated to the right side to design the right thumb prosthesis. The designed prosthesis was printed with a three-dimensional printer using the fused filament fabrication output system.
Discussion:
The Jebsen–Taylor hand function test and Box and Block Test scores improved after application of the prosthesis. Most Quebec User Evaluation of Satisfaction with Assistive Technology results were “very satisfied,” and most Orthotics and Prosthetics Users’ Survey results were “very easy.” Preparing the prosthesis made by three-dimensional scanner and three-dimensional printer was faster and cheaper than preparing a conventional prosthesis.
Clinical relevance
Using three-dimensional scanning and printing technique, we can easily produce specifically shaped finger prostheses for specific movements in amputated patients with low cost.
Background and aim
Three-dimensional (3D) printers have been widely used in industry, biology, food, and medical fields and their use is growing explosively. 3D printers can produce easily modifiable objects without any fixed molding, which makes the objects unique.
3D printers have been used in the medical applications for the human body in the field of plastic surgery, 1 orthopedic implants, 2 dental devices, 3 and orthoses and prostheses.4,5
Silicone finger prosthesis has been used for aesthetics, 6 and acrylic finger prosthesis is used for hand function. 7 Practically, finger prosthesis with a specific shape optimized to perform a specific movement is attractive to patients with finger amputation because it can be easily and inexpensively produced by 3D scanners and printers.
We report a case of a patient with an amputated thumb, who wore specifically shaped finger prostheses that were optimal to perform specific movements and were produced by a 3D scanner and printer and allowed improved functioning.
Technique
A 67-year-old man visited our outpatient department due to a right thumb amputation above the metacarpophalangeal joint in August 2015 (Figure 1). The amputation had happened during work in 1970. He also had gait difficulties with ataxia and mild right-hand weakness due to a left anterior inferior cerebral infarction in 1999. Motor grade of the right upper hand by manual muscle test was good, and a sensory test was normal. He performed most gross motor activities using his right hand because he was right-handed, but he had a difficulty with fine motor activities using his right hand because of the right thumb amputation and mild weakness. He had lived without a prosthesis since the right thumb amputation 45 years ago because no ready-made prostheses met his needs in terms of function and cost. He had to grasp small objects with his left hand or with assistance from others.
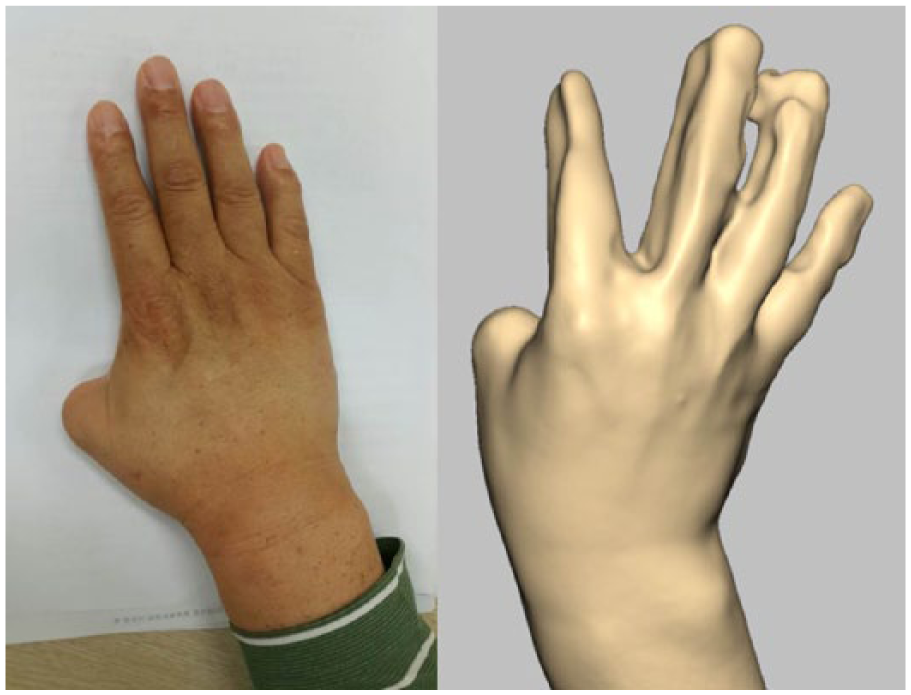
A right thumb was amputated above the metacarpophalangeal joint and this was scanned with a 3D scanner (Artec™ Eva, Artec Group, Luxembourg) at 16 frames/s.
Designing and printing the prosthesis
The patient stated that the most uncomfortable daily activities were writing a letter and picking up a small object. Based on these responses, individualized prostheses were designed to ease the tripod grasp for writing and grasping a small object. His right hand was scanned with a 3D scanner (Artec™ Eva, Artec Group, Luxembourg) at 16 frames/s (Figure 1). The left hand was also scanned in the tripod grasp postures using the same scanner. These scanned data of the left hand were rotated from the left to right side to design the right thumb prosthesis. The right finger prosthesis was designed by overlapping the right amputated hand with the flipped left intact hand (Figure 2), subtracting the overlapped part, and adding the contacted part (Figure 3). All design procedures were performed using the Touch Haptic Stylus (3D Systems Corp., Rock Hill, SC, USA) and Geomagic Freeform (3D Systems Corp.) software.
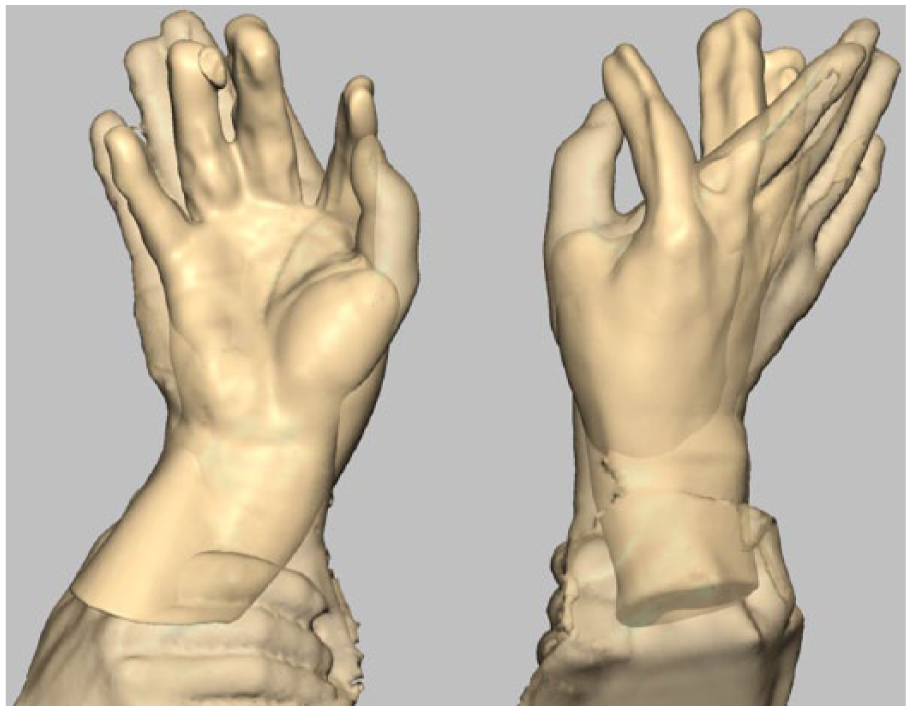
The scanned data of the left intact hand were rotated from the left to right side and overlapped with the right amputated hand to design the prosthesis.
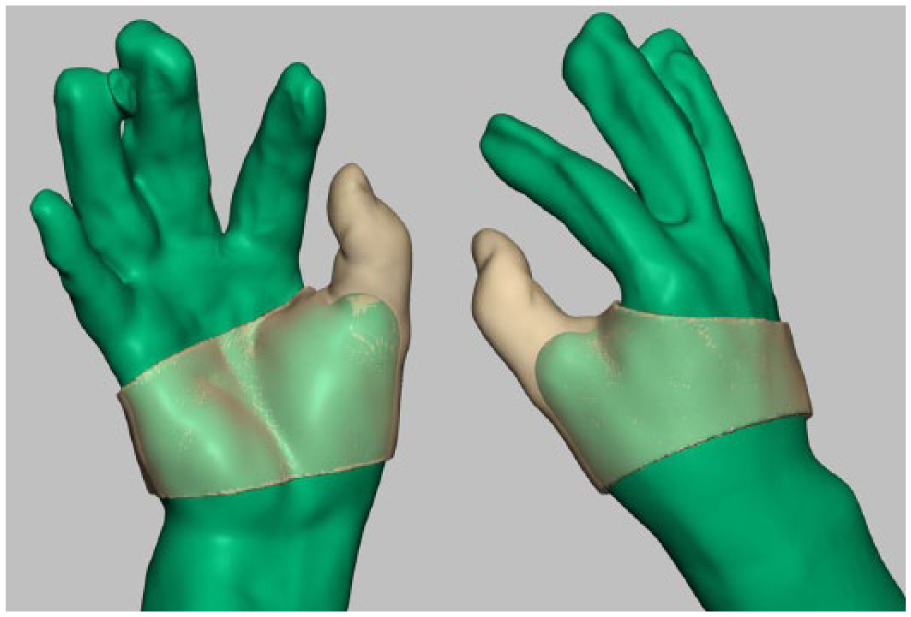
A right-hand prosthesis was designed by subtracting the overlapped part and adding the contacted part.
The designed prosthesis was printed with FB9600 (TPC Mechatronics Inc., Incheon, Korea) using the fused filament fabrication output system, which involved stacking up melted flexible thermoplastic elastomer filaments (Shenzhen Esun Industrial Co., Ltd, Shenzhen, China) layer by layer. These filaments were non-toxic and highly flexible (flexural modulus of 8.1 MPa). After printing out, the finger prosthesis for tripod grasp was given to the patient. To prevent slippage and increase the grip force, the surface of the thumb prosthesis was designed to have a non-slip pattern (Figure 4). The suspension was designed as a band for close attachment to the hand. The patient did not receive occupational therapy to train writing because he adapted easily to using the finger prosthesis.
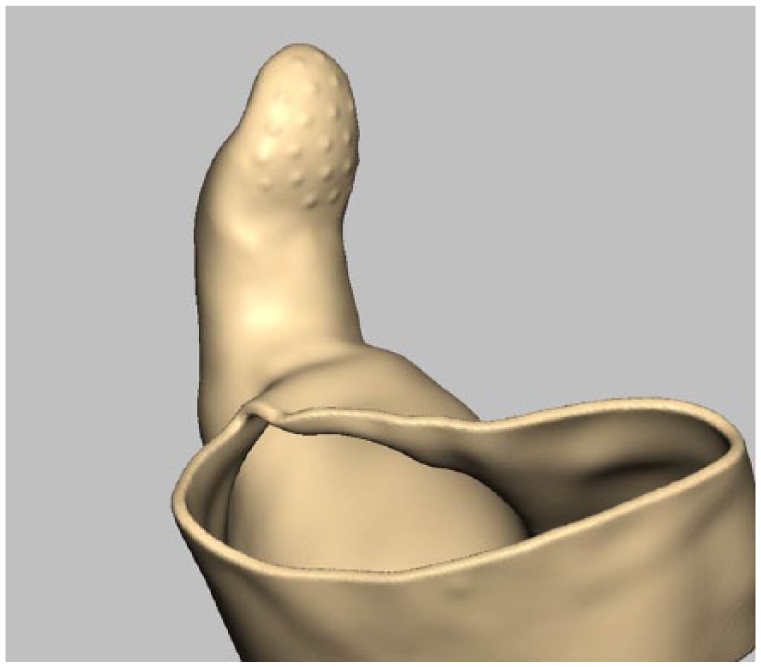
The surface of the thumb prosthesis was designed to have a non-slip pattern to prevent slippage and increase the grip force.
Evaluation of prosthesis
The Jebsen–Taylor hand function test (JTT) and the Box and Block Test (BBT) were performed to evaluate right-hand function in the occupational therapy department. The JTT consists of seven items to evaluate the gross and fine hand motor functions and measures the elapsed time for specific tasks. 8 The BBT is used to measure agility of the upper extremities and to evaluate a worker’s occupational capacity by measuring how many blocks can be moved in 1 min. 9
The patient performed daily activities using the prosthesis for 1 month and revisited our outpatient clinic on 5 October. He underwent JTT and BBT and was tested using the Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST) to determine satisfaction with the prosthesis. The QUEST consists of six items in the area of assistive devices and four items in the area of service parts and scores range from 12 to 60. 10 The service part was omitted because it was not appropriate for the purpose of this study.
The Orthotics and Prosthetics Users’ Survey (OPUS) was used to evaluate performance of daily activities and satisfaction with the tripod-type prosthesis. Upper extremity functional status is evaluated using 19 items on the OPUS (0–57 points), and a score of 27 points represents a moderate level of upper extremity function. 11
Written informed consent was obtained from the patient, and this research was approved by the Institutional Review Board of our hospital (IRB No. 2014-12-013).
The elapsed time and cost for designing and making the prosthesis were about 48 h and US$50.
The BBT score of the patient was 17 before using the prosthesis and 21 after application of the prosthesis. The prosthesis allowed easier grasping of the box and a faster tip pinch (Figure 5).
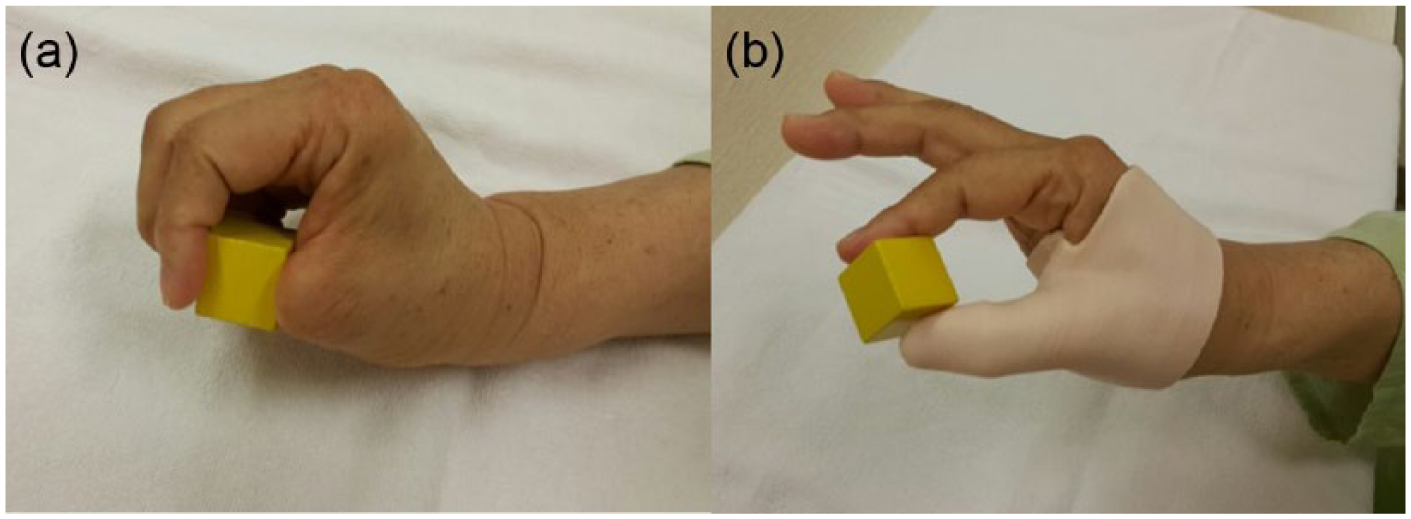
A patient grasps a small box (a) without a prosthesis and (b) with a prosthesis. The prosthesis allowed easier grasping of the box and a faster tip pinch, which increased the BBT score.
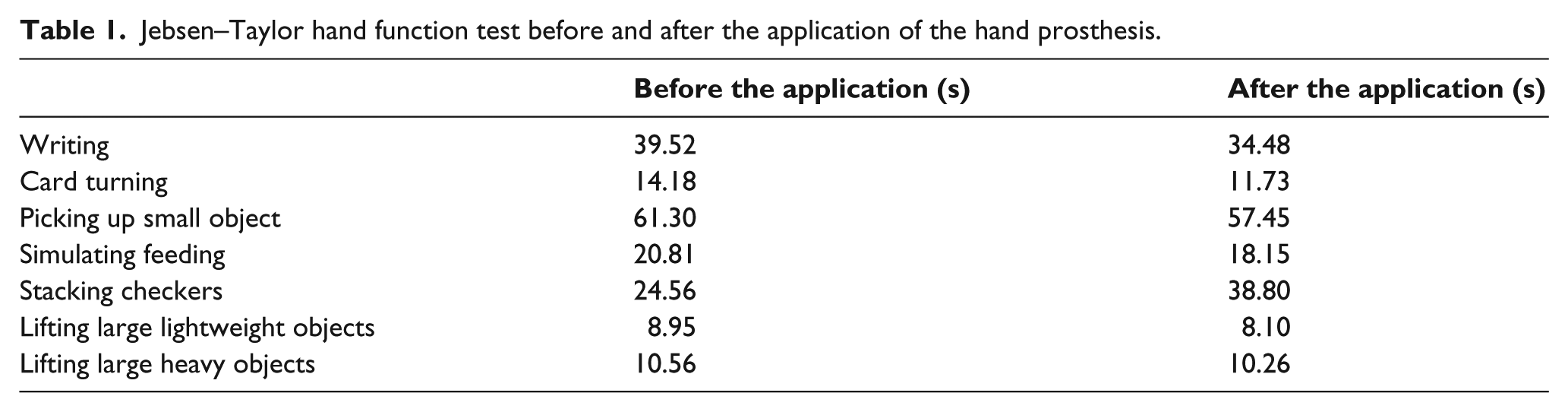
The JTT results showed that elapsed time decreased for all the items except stacking checkers (Table 1). Elapsed time and accuracy of writing improved because the tripod grasp with the finger prosthesis made holding a pencil easier and more delicate writing was possible. Times for card turning and picking up small objects shortened due to opposition and pinching movements of the thumb with the finger prosthesis. Simulated feeding improved because the prosthesis fixed a spoon between the thumb and the second finger. The QUEST satisfaction result was 36 of a total 40 points and most items on the QUEST were “very satisfied” or “quite satisfied.”
Jebsen–Taylor hand function test before and after the application of the hand prosthesis.
Most items except washing the face and tying a shoe on the OPUS test were marked “easy” or “very easy.” The OPUS results revealed “not available (NA)” for washing the face and “difficult” for tying a shoe and using scissors.
The patient wore this finger prosthesis all the time with no complications because he felt the prosthesis was light, close-fitting, easy to don and remove, and gave him no skin troubles.
Discussion
From this study, we applied specifically shaped finger prosthesis made with a 3D scanner and printer designed to perform specific movements for a patient who had his thumb amputated and achieved better functional improvement and satisfaction from the patient.
We easily made the finger prosthesis with the same position taken during a specific action by mirroring the position of the contralateral hand while simulating the action. This simple technique can make the patients produce their prosthesis easily by themselves at any time through a stored design file. In addition, the 3D design process can easily alter diverse changes in finger positions and make a variety of prosthetic hand shapes. This lowers the price and enables patients to make their own prosthesis with diverse finger positions regardless of skill.
In the OPUS test, 16 of 19 items were “easy” or “very easy.” Brush/comb hair, open door with knob, carry laundry basket, and put on and take off prosthesis were “very easy” and put on socks and fold bath towel were “easy.” This means that the tripod-type prosthesis made grasping easier.
All the items on the JTT, except stacking checkers, improved after applying the prosthesis. The patient used his second and third fingers in a lateral pinching motion to stack checkers without the prosthesis. However, he pinched the tips of the prosthetic thumb and second finger to stack checkers. He could not extend his prosthetic thumb voluntarily, so he had difficulty stacking the checkers. Thus, the angle of the prosthetic thumb must be adjusted to ease stacking the checkers.
Considering that this technique has the advantage of adjusting the optimal position of finger joints for specific tasks, it will be useful in cases of amputation above the proximal interphalangeal joint.
It took about 48 h to scan the hand and design and print the prosthesis at a cost of about US$50. This was faster and cheaper than preparing a conventional prosthesis. Acrylic prosthesis by the thermoplastic technique can be made quickly but does not provide optimal angles for specific functions, such as writing or grasping. To produce acrylic prosthesis with optimal angles, specific molds and casts must be made, which require more time and expense. Another advantage of using the 3D printer is that the stored 3D image files can be easily modified, which cannot be achieved with the thermoplastic technique.
In conclusion, we produced specifically shaped finger prostheses for specific movements using a 3D scanner and printer for a patient with an amputated thumb who achieved better function and satisfaction. We hope that 3D scanners and printers will be widely used to prepare finger prostheses with little time and very low cost.
Key points
We easily made the finger prosthesis with the same position taken during a specific action by mirroring the position of the contralateral hand while simulating the action.
This simple technique can make the patients produce their prosthesis easily by themselves at any time through a stored design file and easily alter diverse changes in finger positions.
This technique lowers the price of prosthesis and enables patients to make their own prosthesis with diverse finger positions regardless of skill.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HI14C3229) and ICT R&D program of MSIP/IIPT (Grant No. B0101-16-1081).