
Abstract
Background:
Knee osteoarthritis is common. The evidence regarding the effectiveness of braces and orthoses for patients with knee osteoarthritis is inconclusive according to English-language literature. English-language reviews to date have not included Japanese-language studies.
Objectives:
This study aimed to collect and synthesise Japanese-language randomised controlled trials investigating the effectiveness of braces and orthoses for patients with knee osteoarthritis.
Study design:
Systematic review.
Methods:
Eight databases were systematically searched from inception to 29 July 2015. Only Japanese-language randomised controlled trials were included. Risk of bias was assessed using Physiotherapy Evidence Database scale. A meta-analysis was not appropriate due to the heterogeneity in the included studies.
Results:
Seven randomised controlled trials with low to high risks of bias were included. Six of seven included studies were conducted by the same author group. Limited evidence supported the positive effects of short-lever elastic knee braces to improve pain and functional disability in specific outcomes. No evidence was found to support the use of foot orthoses, such as laterally wedged insoles, medial arch support and metatarsal arch pad.
Conclusion:
Our systematic review found no conclusive evidence about the effectiveness of any braces and orthoses for patients with medial knee osteoarthritis. Future Japanese-language studies should address methodological flaws exposed in this review and strengthen the international evidence base.
Clinical relevance
This is the first systematic review of Japanese-language randomised controlled trials investigating orthoses for patients with knee osteoarthritis. Clinicians can consider the use of short-lever elastic knee braces to improve specifically pain on squat or walking. Evidence found in this review does not support the use of foot orthoses.
Background
Knee osteoarthritis (OA) is an increasingly common condition in the world. 1 The growing prevalence is attributed to ageing societies and rising obesity throughout the world.2,3 The prevalence of radiographic knee OA (Kellgren and Lawrence 4 grades 2–4) among the general population aged 45 years or older in the United States was 28.0%, according to a large-scale study in 2007. 5 The available prevalence of radiographic knee OA in Europe, Australia and Canada is also high, ranging from 13.4% to 67.0%.6–10 Knee OA typically causes pain, swelling and decreased range of motion, which leads to functional disability and decreased quality of life among patients. 11 Due to the increasing prevalence, this disabling condition is anticipated to impose substantial individual suffering and global economic burden to our societies in the future. 12
Although the pathophysiology of knee OA is not entirely clear, it is generally characterised as a degenerative joint disease which commonly involves the damage to the articular cartilage and subchondral bone, 13 osteophyte formation, ligament laxity, atrophy of periarticular muscles 14 and synovial inflammation. 15 The medial compartment has been reported to be involved nearly 10 times more often than the lateral compartment. 14 Patients with medial knee OA often have varus alignment, while patients with the involvement of the lateral compartment tend to assume valgus alignment. 16 These malalignments increase the lever arm length between the ground reaction force and the centre of the joint thereby increasing the adduction/abduction moment resulting in increased contact pressure to the medial or lateral compartment.17,18 In fact, malalignments have been reported to increase the risk of progression of this disease. 19
Conservative management is usually recommended at first for knee OA. Conservative management includes various strategies, such as patient education, 20 weight management, 21 aerobic exercise, 22 strengthening exercise, 22 manual therapy, 23 ultrasound, 24 braces and orthoses, 25 walking aids, 26 anti-inflammatory medication, 27 hyaluronic acid injection 28 and corticosteroid injection. 29 Braces and orthoses are commonly used to improve pain and functional disability of patients with knee OA.30,31 Although its mechanism has not been proven yet, mechanical unloading to the affected compartment and neurophysiological pain modulation by proprioceptive inputs have been hypothesised.30–32
In Japan, knee OA is epidemic due to the infamously ageing society, where the proportion of population aged over 65 years was estimated to be 26.5% in 2015. 33 According to a large cross-sectional study recruiting Japanese adults at various ages in 2012, 34 the prevalence of radiological knee OA (Kellgren and Lawrence grades 2–4) was 51.5% (57.9% in women and 38.8% in men). In another study focusing on subjects aged 60 years or older in 2009, 35 the figures were even higher (70.2% in women; 47.0% in men).
Historically, scientific studies written in non-English languages have been largely overlooked from international academics due to the dominant use of English. 36 However, this linguistic constraint can confound English-language secondary research, undermining the totality of evidence base. 37 Considering the high prevalence of this condition in the super-ageing society in Japan, we suspected that there might be some evidence on this topic in Japanese-language literature which had not been introduced into English-language literature. The uncharacteristic inclusion of English-language studies by Japanese authors Toda and colleagues38–42 in the recent English-language reviews investigating the effectiveness of braces and orthoses for patients with knee OA25,43–46 also heightened our expectation.
The aim of this systematic review was to collect, assess and synthesise Japanese-language randomised controlled trials (RCTs) about the effects of braces and orthoses on pain and functional disability of patients with knee OA.
Methods
Study protocol
This systematic review was written in line with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) statement. 47 The protocol of this review was registered in the international prospective register of systematic reviews PROSPERO network (registration number CRD42015024689) before commencing a systematic search.
Eligibility criteria
The clinical question for the review was developed through a participants, intervention, comparator, outcome measures and study design (PICOS) format. 48 Specific definitions of the components of the clinical question are provided in Table 1. Studies were included if they reported on patients with knee OA, diagnosed with radiological investigation (Kellgren and Lawrence 4 grades 1–4) and clinical symptoms. Limitation was not set on age or gender. Interventions of interest included any types of braces or orthoses for knee, foot or ankle. No restriction was placed on comparator interventions. We considered primary outcome measures such as pain and functional disability with any duration of follow-up. Studies examining only kinetic or kinematic parameters were excluded. This systematic review included only RCTs to minimise bias. Only Japanese-language articles published in peer-reviewed journals were included.
PICOS format and search terms.
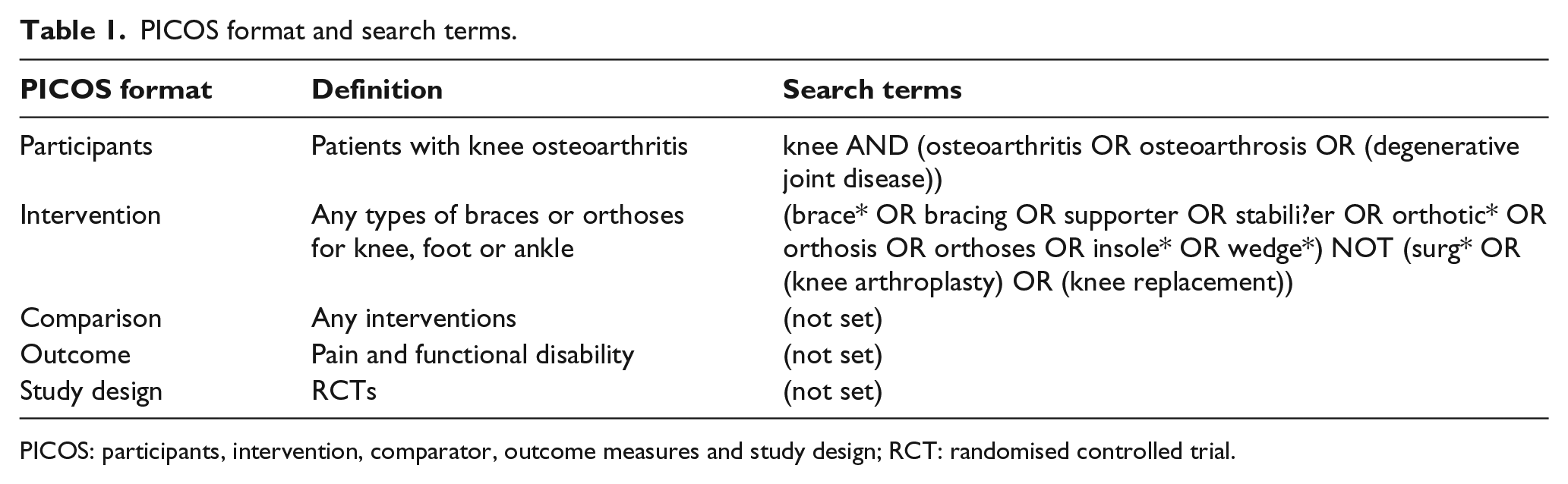
PICOS: participants, intervention, comparator, outcome measures and study design; RCT: randomised controlled trial.
Information sources and search strategy
A systematic search was performed using three Japanese-language databases, including CiNii, Ichushi and Medical*Online. An additional search through five English-language databases with Japanese indexes (CINAHL, Embase, MEDLINE, Scopus and Web of Science) was performed to find relevant Japanese-language studies with English-language abstracts. All databases were searched from the earliest available dates to 29 July 2015. The three Japanese-language databases were chosen due to their comprehensiveness. Five English-language databases were selected due to their capacity to limit articles to Japanese language. Search terms were established based on the PICOS format (Table 1). In Japanese-language databases, Japanese equivalents of these words were used. The systematic search was performed collaboratively by two authors (T.N. and K.M.).
After the initial systematic search, duplicates were removed and titles and abstracts of the remaining articles were screened subsequently. In the last process, full texts of potentially relevant articles were assessed for eligibility. Reference lists of included studies were also hand searched.
Risk of bias assessment
Risk of bias assessment was performed using Physiotherapy Evidence Database (PEDro) scale. 49 The PEDro scale consists of 11 specific criteria. Items 2–9 refer to the internal validity of an article, and items 10 and 11 refer to the statistical analysis, ensuring sufficient data to enable appropriate interpretation of the results. 49 Item 1 is related to the external validity and therefore not included in the total PEDro score. This critical appraisal tool has been proven to be reliable and valid by previous studies.50,51 The risk of bias in each study was classified as ‘high’ (4/10 or less), ‘moderate’ (5 or 6/10) or ‘low’ (7/10 or more) according to total PEDro scores.
Two independent Japanese-speaking physiotherapists (T.N. and K.M.) critically appraised all included studies. After completing individual assessments, the scores were compared, and inter-tester reliability of the PEDro scores was determined as Cohen’s kappa statistics. 52 Kappa statistics were classified as almost perfect agreement (0.81–1.00), substantial agreement (0.61–0.80), moderate agreement (0.41–0.60), fair agreement (0.21–0.40), slight agreement (0.00–0.20) or poor agreement (<0.00). 53 When consensus could not be reached between the two assessors, opinions from an English-speaking author (S.M.) were sought to resolve disagreements.
Data extraction and synthesis
Data were extracted on sample characteristics (sample size, age, gender, body mass index (BMI), ethnicity, radiological severity, pain duration, laterality and co-morbidity count), types of interventions, outcome measures, results (pre- and post-intervention data, follow-up data, statistical significance and effect size) and ethical considerations for participants. The results with any duration of follow-ups were extracted. We anticipated that a meta-analysis might be undertaken, should there be homogeneity among included studies and sufficient data available. The corresponding authors of included articles were expected to be contacted for necessary data to complete further analysis.
Results
Study selection
The literature search process using eight electronic databases is illustrated in Figure 1. The initial search identified 437 records. After removing 89 duplicates, titles and abstracts of 348 articles were screened. In the screening, 337 articles were excluded primarily because they were not RCTs. This yielded 11 potentially relevant articles. In a full-text assessment, three studies were excluded because they used pseudo-randomisation.54–56 Another one study, where interventions were chosen by patients, was also excluded at this stage. 57 The hand search in reference lists of included studies did not discover any other relevant articles. Accordingly, seven Japanese-language RCTs were included in this review.
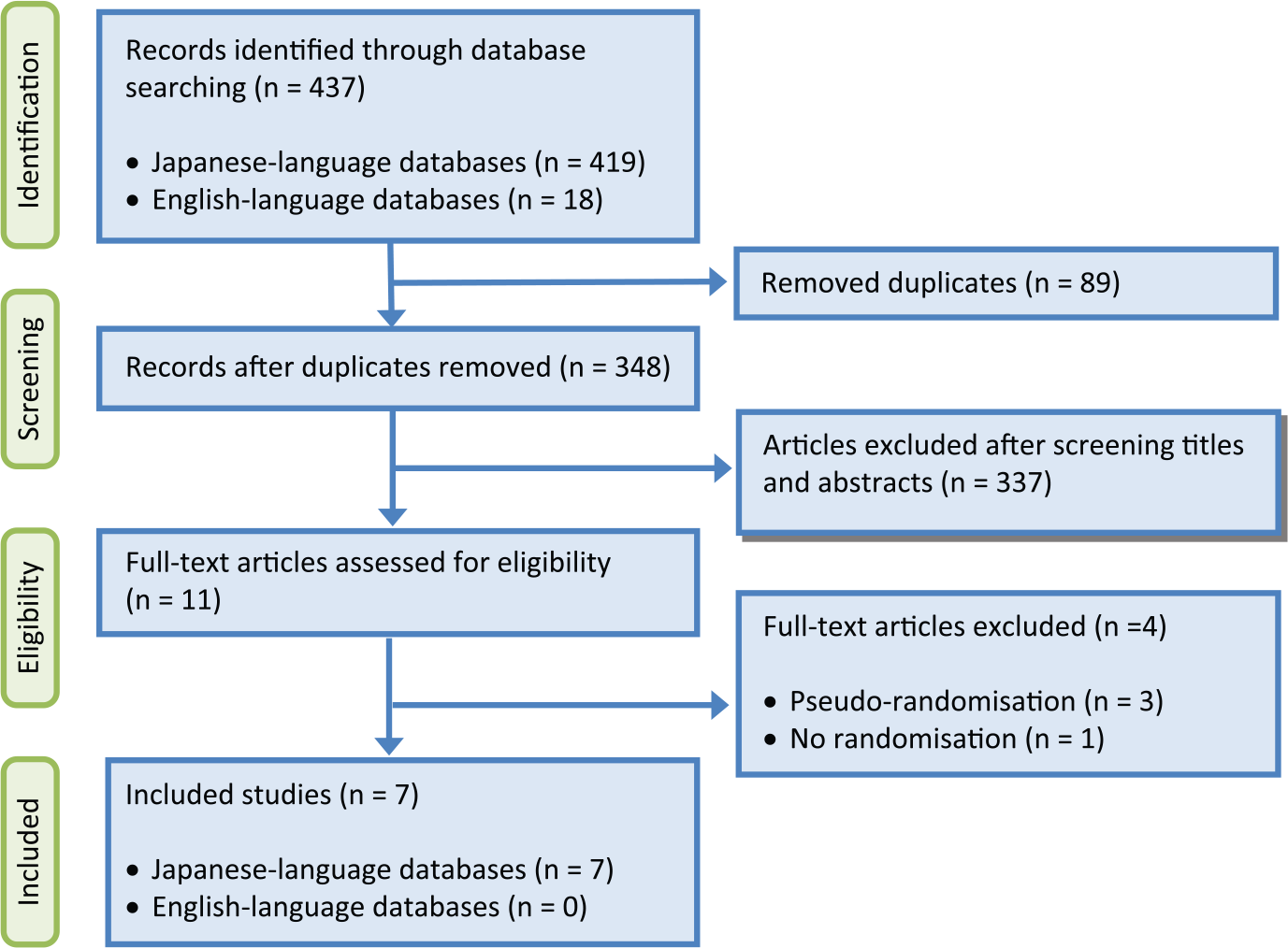
Flowchart of study selection.
Study characteristics
A summary of the most important characteristics of seven included studies is presented in Table 2. The same author group was involved in six of seven studies and all the six trials were conducted in the authors’ private orthopaedic clinic.58,60–64 Five different articles written in English by this author group had been included in one English-language systematic review. 25 The corresponding author was contacted by e-mail and it was confirmed that their studies recruited only patients who had never received treatments using braces or orthoses, and therefore there was no duplicate patient across their studies irrespective of languages. None of the included studies was approved by external ethics committees.
Summary of included studies.
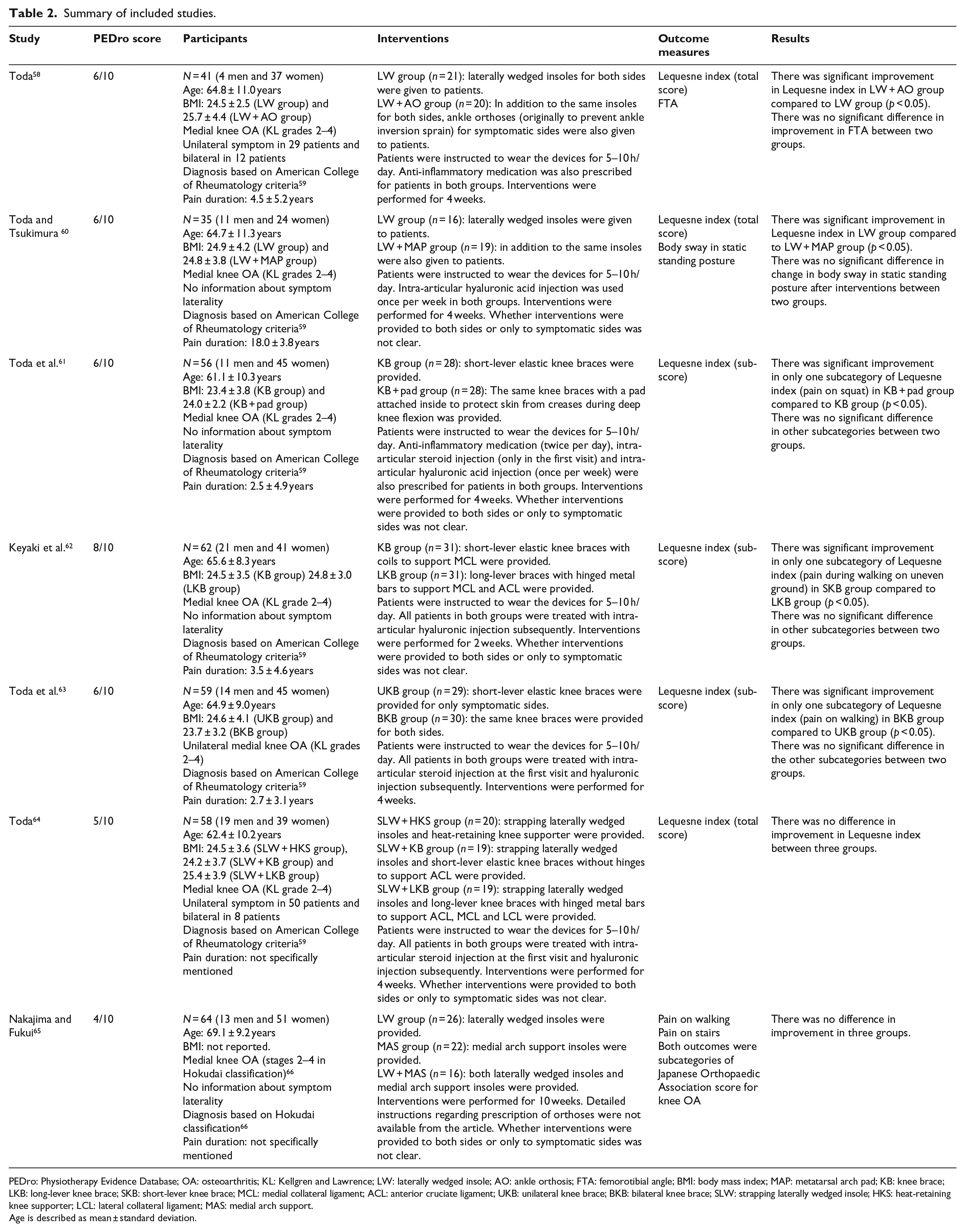
PEDro: Physiotherapy Evidence Database; OA: osteoarthritis; KL: Kellgren and Lawrence; LW: laterally wedged insole; AO: ankle orthosis; FTA: femorotibial angle; BMI: body mass index; MAP: metatarsal arch pad; KB: knee brace; LKB: long-lever knee brace; SKB: short-lever knee brace; MCL: medial collateral ligament; ACL: anterior cruciate ligament; UKB: unilateral knee brace; BKB: bilateral knee brace; SLW: strapping laterally wedged insole; HKS: heat-retaining knee supporter; LCL: lateral collateral ligament; MAS: medial arch support.
Age is described as mean ± standard deviation.
Study designs
All seven studies were RCTs with parallel designs.
Participants
Overall, 375 patients (93 men and 282 women) participated in the seven studies. Sample sizes ranged from 35 to 64 per study. None of the studies performed sample size calculations. The mean ages of patients were relatively consistent, ranging from 61.1 to 69.1 years. Information regarding participants’ ethnicity was not available. All included studies recruited patients with medial knee OA. In six studies by the same author group,58,60–64 diagnosis was made based on American College of Rheumatology, 59 and patients with Kellgren and Lawrence 4 grades 2–4 were eligible. Only one study used Hokudai classification for diagnosis, and patients with stages 2–4 were included. 65 The majority of participants in the included studies were categorised into grade 2 or 3 in these classification systems in terms of the radiological severity. The mean BMI ranged from 23.4 to 25.7, except for one trial which did not clarify BMI. 65 The mean pain durations ranged from 2.5 to 18.0 years in six studies,58,60–64 whereas two studies did not specifically mentioned pain duration.64,65 One study recruited only patients with unilateral OA, 63 while two studies examined both patients with unilateral and bilateral OA.58,64 The other four studies did not clarify the laterality of symptoms.60–62,65
Interventions
Three studies explored the effects of various types of knee braces.61–63 Although detailed mechanical properties of knee braces were not available in two studies,61,63 none of the three studies used conventional valgus knee braces according to the visual images in the articles. Four studies investigated different types of foot orthoses, including laterally wedged insoles, medial arch supports and metatarsal arch supports.58,60,64,65 The maximum thickness of laterally wedged insoles ranged from 7 to 8 mm,58,60,64,65 and one study did not mention wedge thickness. 64 Only one study used a combination of knee braces and foot orthoses. 64 In the six studies by the same author group, patients were instructed to wear devices for 5–10 h/day,58,60–64 while the other study did not specify the dosage of interventions. 65 In five studies, whether interventions were provided to both sides or only to symptomatic sides was not clear.60–62,64,65 Included studies commonly used co-interventions, such as intra-articular hyaluronic injection,60–64 intra-articular steroid injection61,63,64 and anti-inflammatory medication. 58 One study did not specifically report co-interventions. 65 Intervention periods were 4 weeks in five studies,58,60,61,63,64 2 weeks in one study 62 and 10 weeks in the other study. 65
Outcome measures
The six studies by the same author group consistently used the Lequesne index. The Lequesne et al. 67 index was originally developed and validated in French as an assessment tool to assess pain, stiffness and functional disability of patients with knee or hip OA. This questionnaire has been translated into several languages.68–70 To the best of the authors’ knowledge, however, there is no formally translated and validated Japanese version of the Lequesne index. This outcome measure was analysed as a total score in three studies58,60,64 or as a separate scores in subcategories in the other three studies.61–63 One study by another author group used two subcategories of the Japanese Orthopaedic Association (JOA) score for knee OA, including pain on walking and stairs. 65 The JOA score for knee OA in Japanese has been reported to be a reliable and valid assessment tool. 71 All studies assessed outcome measures immediately before and after interventions and did not perform any long-term follow-up assessments.
Risk of bias assessment
The results of the critical appraisal using PEDro scale are presented in Table 3. Included studies had a median score 6 of 10, ranging from 4 to 8. Five studies had moderate risk of bias, while one study had high risk of bias and only one study had low risk. Common methodological flaws included no blinding of participants (100%), therapists (100%) and assessors (85.7%), and no intention-to-treat analysis (85.7%). The two reviewers (T.N. and K.M.) showed an almost perfect level of inter-rater reliability in determining PEDro scores of included articles (overall kappa score of 0.96).
A comparison of between-group effect sizes.
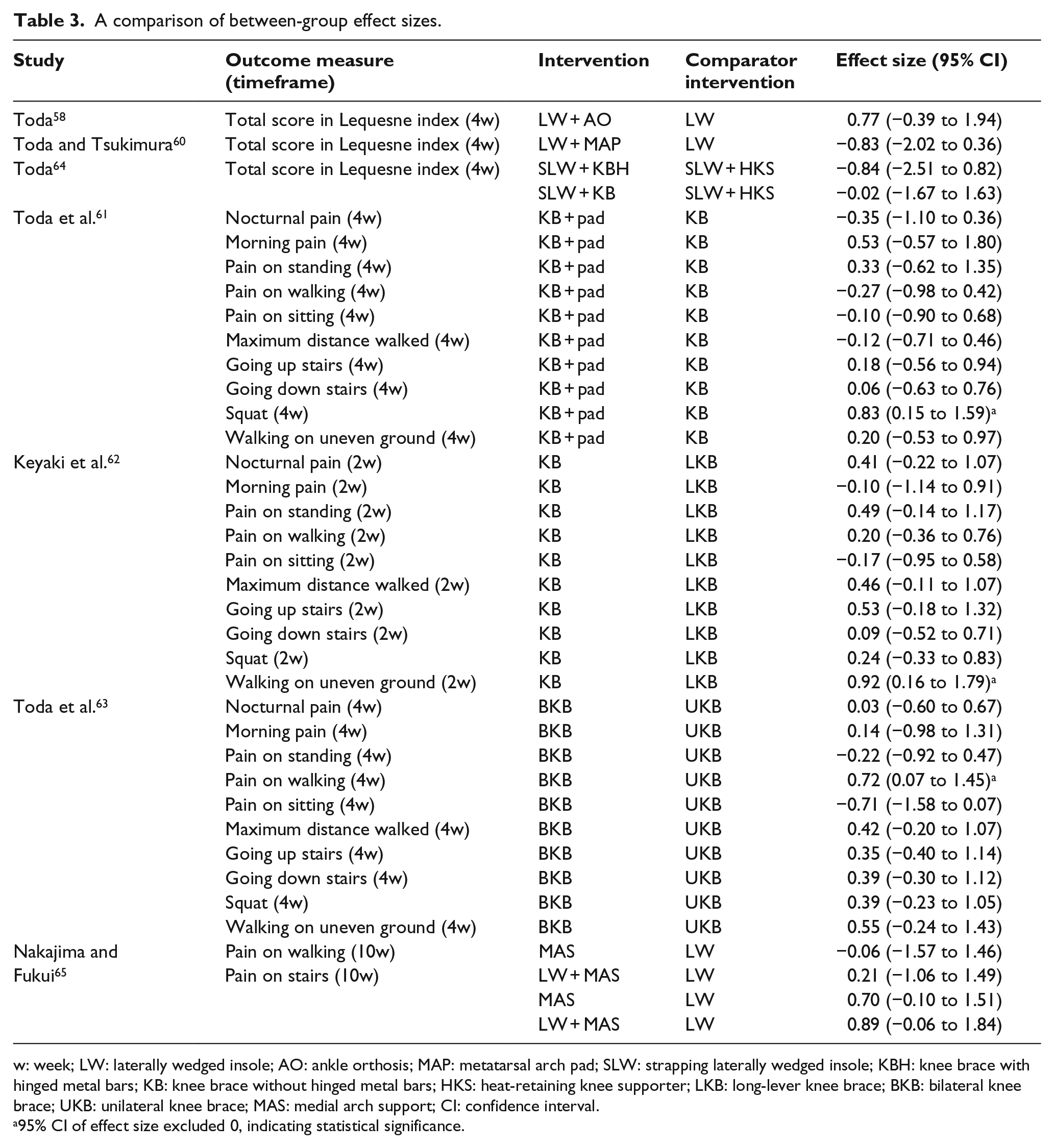
w: week; LW: laterally wedged insole; AO: ankle orthosis; MAP: metatarsal arch pad; SLW: strapping laterally wedged insole; KBH: knee brace with hinged metal bars; KB: knee brace without hinged metal bars; HKS: heat-retaining knee supporter; LKB: long-lever knee brace; BKB: bilateral knee brace; UKB: unilateral knee brace; MAS: medial arch support; CI: confidence interval.
95% CI of effect size excluded 0, indicating statistical significance.
Data extraction and synthesis
Due to the heterogeneous interventions and comparator interventions across the included studies, it was thought to be inappropriate to undertake a meta-analysis. A qualitative synthesis was undertaken instead. None of the included studies reported effect sizes. Cohen’s d and 95% confidence interval (CI) were calculated for between-group effect sizes based on available data (Table 3).72,73 Cohen’s d was calculated by dividing mean change difference between intervention and comparator groups by pooled standard deviation. 74
Effectiveness of knee braces
Three studies by the same author group investigated the effectiveness of different types of knee braces.61–63 One study by Toda et al. 61 reported significantly greater effects of knee braces with pads to improve pain on squat compared to knee braces without pads. Knee braces used in this study were short-lever, elastic, equipped with coils but not hinges. The location of coils was not clearly mentioned in the article. The reported findings corresponded with our further analysis (Cohen’s d = 0.83, 95% CI = 0.15–1.59). The authors hypothesised that the pads inside the knee braces might have protected skin from creases of braces during squat, resulting in reduction in pain. It should be noted that there was no significant difference between the two interventions in the other nine outcomes in the Lequesne index.
One study by Keyaki et al. 62 found that elastic short-lever knee braces were significantly more effective to improve pain on walking on uneven ground compared to long-lever braces (Cohen’s d = 0.92, 95% CI = 0.16–1.79). According to the study, short-lever knee braces were equipped with coils to support the medial collateral ligament (MCL), while long-lever braces were equipped with metal hinges and bars on both medial and lateral sides to support MCL and anterior cruciate ligament (ACL). The location of coils in the short-lever brace was not specified in the article. This study reported no significant difference between the two interventions in the other nine outcomes in Lequesne index.
Another study by the same author group reported a significantly greater effect on pain on walking when knee braces were applied to both knees compared to when the same type of braces were applied to only symptomatic sides (Cohen’s d = 0.72, 95% CI = 0.07–1.45). Knee braces used in this study were elastic and not equipped with hinges. Detailed mechanical properties of the knee braces were not available in the article. No significant difference was reported between the two interventions in the other nine outcomes in the Lequesne index.
Effectiveness of foot orthoses
Three studies examined the effectiveness of various types of foot orthoses.58,60,65 One study by Toda 58 found that the combined use of laterally wedged insoles (8-mm maximum thickness) and figure-eight ankle orthoses was more effective than laterally wedged insoles alone to improve the total score of Lequesne index. However, our analysis using effect size revealed no statistical significance (Cohen’s d = 0.77, 95% CI = −0.39 to 1.94).
Another study by the same author group reported significantly better effect of laterally wedged insoles (8-mm maximum thickness) compared to the combined use of the same insoles and metatarsal arch pads to improve Lequesne index. According to our further analysis, however, its effect size was not statistically significant (Cohen’s d = 0.83, 95% CI = −0.36 to 2.02).
The last study by Nakajima and Fukui 65 compared the effectiveness of laterally wedged orthoses (7-mm maximum thickness), medial arch support and a combination of both. They found no difference among three interventions, which corresponded to our analysis using effect sizes (see Table 3).
Effectiveness of combined interventions
One study investigated the effectiveness of combinations of foot orthoses and knee braces: laterally wedged insoles with subtalar strapping and a heat-retaining knee supporter, the same insoles and short-lever knee braces without hinges and the same insoles and long-lever knee braces with hinged metal bars. The thickness of the laterally wedged insoles was not stated. The article described that short-lever knee braces were elastic and designed to support the ACL, while long-lever knee braces were equipped with hinged metal bars on both medial and lateral sides to support MCL, lateral collateral ligament (LCL) and ACL. This study reported no significant difference between three groups, which corresponded to our additional analysis of effect sizes (see Table 3).
Discussion
Summary of main results
The purpose of this review was to collect and synthesise all available Japanese-language RCTs investigating the effectiveness of braces and orthoses for patients with knee OA. The systematic search identified seven eligible RCTs with low to high risk of bias. Meta-analysis was thought to be inappropriate due to the absence of common interventions and comparator terms. The reported positive effects of knee braces were limited to specific symptoms and might not be related to clinically relevant overall effects on pain and functional disability. Although two studies reported significant findings on the effects of foot orthoses on the Lequesne index, our further analysis revealed that effect sizes were not statistically significant.
Source of bias and limitations of studies
All seven included studies failed to blind patients and clinicians.58,60–65 Given that blinding patients to interventions is important particularly when the outcome measures are subjective, this methodological flaw might have affected the findings of these studies which consistently used subjective questionnaires, including the Lequesne index and JOA. Six of seven studies had or potentially had drop-outs and they did not perform intention-to-treat analysis. The lack of intention-to-treat analysis might have biased the estimates of treatment effects in these studies. 75
Reporting styles were generally poor and information regarding results was insufficient across all the included studies. No information was available with regard to laterality of OA in four studies.60–62,65 Although co-morbidity count and ethnicity have been reported to be strong prognostic factors for symptomatic progression of knee OA, 76 none of the included studies clarified these factors. The mechanical properties of knee braces (e.g. supporting LCL, MCL and/or ACL) investigated in two studies were not reported in detail in two studies.61,63 It was not clearly stated whether interventions were provided to both sides or only to symptomatic sides in five studies.60–62,64,65 Potential heterogeneity in participants and inconsistencies in intervention methodologies within these studies might have confounded the results.
Sample sizes were consistently small (35–64 per study) and none of the studies performed sample size calculation. Potentially insufficient sample sizes might have compromised statistical precision, leading to wide 95% CI and statistical insignificance. 77 Although effect sizes were large in some comparisons, statistical significance was identified only in two comparisons out of 38 (see Table 3). 78 Finally, the use of invalidated Japanese version of the Lequesne index evaluated in six studies might have introduced another bias.58,60–64
Limitations of this review
This review was potentially limited by its search strategy, as we aimed to include only published literature. This strategy may be subject to publication bias because trials with positive findings tend to be published more often and more quickly compared with trials with negative findings. 79 We found that six of seven included studies were investigated by the same author group.58,60–64 Thus, the findings in our review might be affected by potential selection bias in these studies. Since all included studies evaluated only short-term outcomes, long-term effects of braces and orthoses were unclear. This review also suffered from the lack of homogeneity in the included studies, preventing the quantitative synthesis of effect sizes with enhanced statistical precision. Although language bias was an inevitable consequence of this systematic review, we hope that the findings in this study will be integrated into broader framework in further research and complement the international evidence base.
Comparison with other reviews
Although one recent English-language systematic review concluded that valgus knee braces might be more effective to decrease external knee adduction moment during walking compared to no intervention, clinical benefits were uncertain. 80 Another recent review reported low-quality evidence that patients with medial knee OA might benefit more from knee braces than from no treatment and moderate-quality evidence that laterally wedged insoles are as effective as neutral insoles. 25 This review also found the lack of evidence to support superior effects of laterally wedged insoles compared to no treatment. In another systematic review, a significant difference in effect sizes of laterally wedged insoles was found between the two types of control interventions (either neutral insoles or no treatment) with smaller effect sizes seen in studies where control interventions were neutral insoles. 46 Based on this finding, we speculate that various comparator interventions used in the included studies in our review might have led to statistically insignificant effect sizes for foot orthoses (see Table 3).
Implications for future research
Due to the paucity of high-quality RCTs, evidence regarding positive effects of braces and orthoses for patients with knee OA is inconclusive. Future Japanese-language RCTs should reflect on and improve the methodological flaws exposed in this review to contribute to a stronger evidence base. Particularly, future studies should recruit sufficient numbers of patients based on sample size calculations to ensure higher statistical precision and improve reporting styles, disclosing sufficient information to enable further analysis in secondary studies. Future studies should seek ethics approval from relevant human ethics committees.
Implications for clinical practice
Our analysis of effect sizes revealed statistically significant differences favouring knee braces with pads for improvement in pain on squat (Cohen’s d = 0.83, 95% CI = 0.15–1.59), short-lever elastic braces for improvement in pain on walking on uneven grounds (Cohen’s d = 0.92, 95% CI = 0.16–1.79) and the use of short-lever elastic knee braces for both sides to improve pain on walking (Cohen’s d = 0.72, 95% CI = 0.07–1.45) (see Table 3). These were the only three comparisons where statistical significance was identified. Therefore, the use of these knee braces can be discussed between clinicians and patients with the consideration of patient preferences and costs, when pain on squat or pain during walking on uneven or flat surface is the main symptom of patients. Given that evidence showed that braces and orthoses might not be effective to improve pain and functional disability in general, these interventions might not be justifiable when patients also suffer from multiple complaints listed in the Lequesne index, such as nocturnal pain or difficulties of using stairs.
Conclusion
Our systematic review found no conclusive evidence about the effectiveness of any braces and orthoses for patients with medial knee OA. The use of short-lever elastic knee braces without hinges for symptomatic side or both sides might have potential clinical utility in specific cases. Future Japanese-language studies should address methodological flaws exposed in this review and strengthen the international evidence base.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.