
Abstract
Background:
Knee osteoarthritis has commonly been associated with a symptom of pain resulting in an inter-limb weight-bearing asymmetry during functional tasks. Patellar tendon strap is one of the non-pharmacologic interventions to alleviate knee pain.
Objectives:
To investigate the immediate effect of a patellar tendon strap on weight-bearing asymmetry during squatting in people with unilateral knee osteoarthritis.
Study design:
Cross-sectional study.
Methods:
Ten patients with unilateral knee osteoarthritis and 10 healthy subjects were included in the study. Weight-bearing asymmetry of patients was assessed using a weight-bearing squat test during squatting at 30° and 60° both with and without patellar tendon strap. Pain intensity was assessed during squatting in unstrapped and strapped conditions with Visual Analog Scale.
Results:
The decrease in weight-bearing asymmetry values immediately after wearing patellar tendon strap during 30° (p = 0.006) and 60° (p = 0.011) of squatting tests was significantly higher in knee osteoarthritis patients than in healthy subjects. Reported pain intensity was similar in unstrapped and strapped conditions (p = 0.066).
Conclusion:
The results of this study showed improved inter-limb weight-bearing symmetry during squatting. Further research with larger sample sizes investigating the effect of patellar tendon strap on weight-bearing asymmetry during functional activities in people with knee osteoarthritis is warranted.
Clinical relevance
Patellar tendon straps (easily fit and cheap unlike knee braces) had more improvements in inter-limb weight-bearing symmetry during squatting in people with knee osteoarthritis compared to healthy subjects. This study is a new insight for future studies to investigate clinical benefits of wearing patellar tendon straps in this population.
Background
Knee osteoarthritis (OA) is one of the most common musculoskeletal disorders in middle-aged and elderly persons, and the patellofemoral joint is involved in 65% of the cases.1–4 It has commonly been associated with a symptom of pain which is usually aggravated by movement or weight bearing on joint and relieved by rest. 5 Daily activities which include weight bearing on knee joints such as stair climbing and descent, bending to floor, and squatting cause increase in pain in knee OA.6,7
Several pharmacologic and non-pharmacologic interventions are used to relieve knee pain and improve physical performance in functional activities for people with knee OA.8,9 The patellar tendon strap (PTS), a band worn just below the knee, is one of the common methods of treatment for several knee pain problems (mostly in patellar tendinopathy, patellar subluxation, and patellar femoral syndrome). 10 It was first introduced by Levine in 1978 to treat knee pain 11 and used in variety of terms including knee band, jumper’s knee strap, infrapatellar strap, and PTS; the words strap, band, and brace are used interchangeably. 12 The mechanism of this strap in alleviating pain is to reduce loading of the patellar tendon at its insertion by altering the angle and direction of stress at the site of injury, unloading the affected site, and decreasing the pain by distributing forces on it. 13 One of the cadaveric studies demonstrated that PTS reduced patellofemoral contact pressure by an average of 10%. 14 Furthermore, neurophysiological assessments have proven that these straps improve knee extensor function and decrease reaction time of the quadriceps. 15
In spite of the common use of this device in relief of knee pain and aforementioned mechanisms,12–14,16 the effects of wearing PTS on a variety of daily functional activities have not been commonly investigated. Especially, preserving weight-bearing symmetry during functional task such as squatting is an important target in the treatment of unilateral knee problems to avoid secondary injuries of both involved and healthy sides since squatting is one of the most demanding movements of the knee joint. 7
The commonly observed compensation strategy to reduce pain in functional tasks including squatting was an inter-limb weight-bearing asymmetry (WBA). 17 WBA is thought to primarily arise from the pain of the affected side to reduce loading of the limb. 18 Asymmetrical weight bearing due to pain during squatting potentially increases the risk of further injuries, especially on the unaffected side, and falls. 19
Considering the neuromuscular benefits, being support for reduction in patellofemoral contact pressure, and treatment mechanism of PTS on pain relief, we hypothesized that PTS intervention would be a useful method to achieve squatting movement with more symmetrical inter-limb weight-bearing distribution. Therefore, the objective of this study was to investigate the immediate effect of a PTS on WBA during squatting in people with unilateral knee OA.
Methods
Subjects
A total of 46 patients who were diagnosed with unilateral tibiofemoral OA coexisting with patellofemoral knee OA at the Dokuz Eylül University Hospital and 15 healthy subjects were invited to participate in the study. Inclusion criteria used in selection of the patients included the documented radiological alterations in the knee joint of grade 2 or more according to the Kellgren–Lawrence criteria and the presence of weight-bearing knee pain (walking or standing) of ⩾4 on a 10-cm Visual Analog Scale (VAS) on their affected knee. In addition, none of the patients had varus deformity on their affected knee.
Patients were excluded from the study if they had any of the following: inability to understand the study protocol, history of any known neurological or orthopedic disorders, and history of surgery in both knees. The healthy volunteers were recruited from partners of the knee OA patients and hospital staff. Figure 1 shows the flow of subjects through the study.
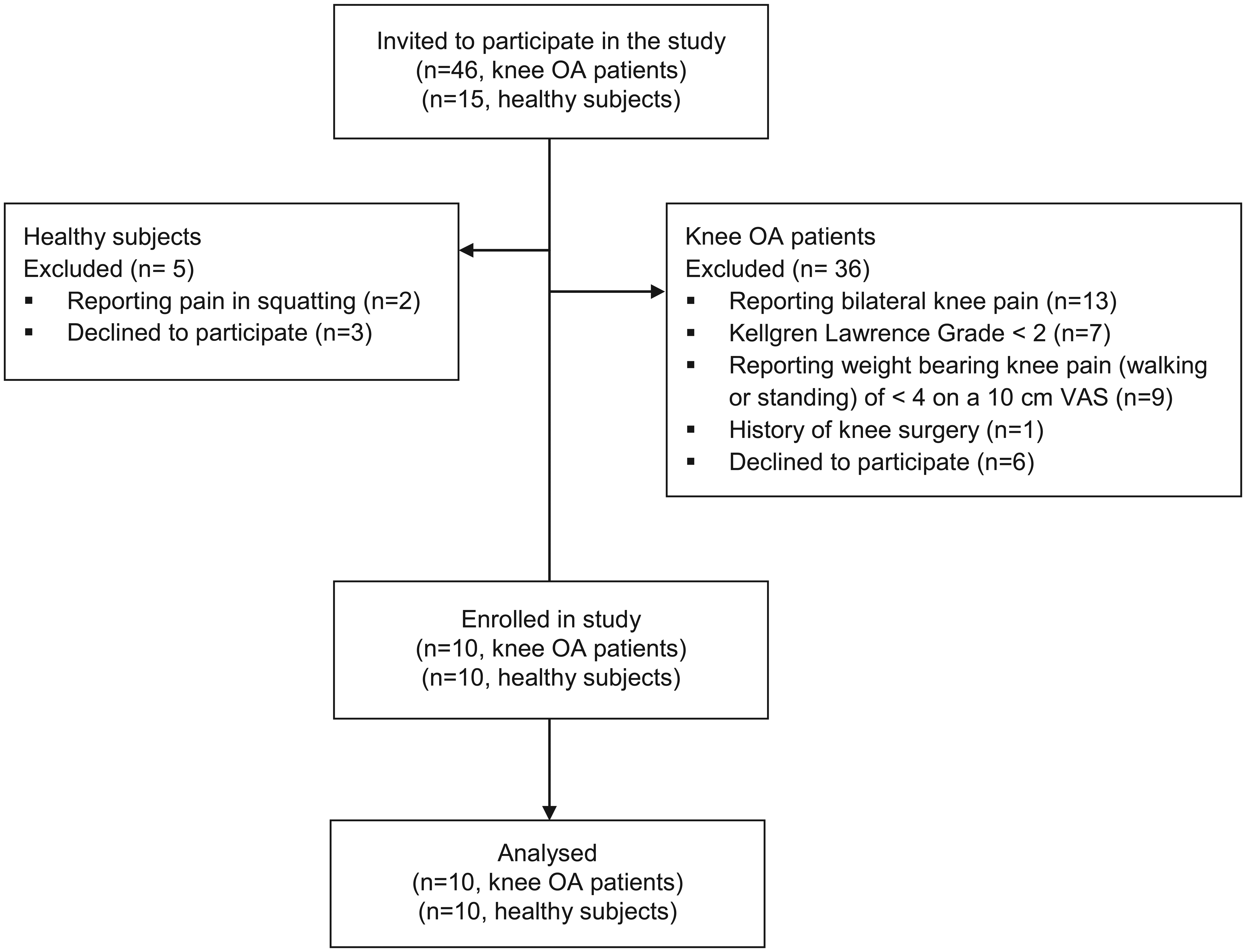
Flow diagram of the study.
Ethical approval was obtained from the ethical committee of the Dokuz Eylül University. All subjects signed an informed consent before participating in this study.
Intervention
The PTS (Diz Tendon Bandı; Morsa Cyberg Orthopedic Products, İstanbul, Türkiye) that we used was made of neoprene with a Velcro fastener (Figure 2). The same investigator placed all the straps. Straps were wrapped around the affected knee just below the patella of the knee OA patients as commonly prescribed.11,13 In healthy subjects, straps were placed around the knee of leg which bore less body weight. The length of the strap was adjusted from posterior by the Velcro fastener until it fitted the leg properly. It was placed carefully not to restrict the knee movement or circulation.

The patellar tendon strap used in this study.
Procedure
Data were collected in four categories: subjects’ demographics (age, gender, height, body weight, and body mass index), medical information, measures of WBA while squatting, and knee pain intensity in knee OA patients.
Knee pain intensity
The intensity of subjective knee pain was measured using VAS, which has been widely used in diverse adult populations, including those with arthritic knee. The scale consisted of a 10-cm horizontal line, with the left extreme indicating “no pain” or 0 and right extreme indicating “pain as bad as it could be (i.e. unbearable pain)” or 10. To avoid clustering of scores around a preferred numeric value, numbers were not located on the scale. 20 Patients were instructed to make a mark on a horizontal line to indicate the intensity of the knee pain they experienced at the time of assessment. The mark on the line was measured from the left using a ruler. The score is determined by measuring the distance (cm) on the 10-cm line between the “no pain” anchor and the patient’s mark. Pain intensity was assessed during squatting both without and with PTS, respectively. Patients were not able to see their previous scores when being reassessed.
Squat test and WBA
WBA was assessed using a weight-bearing squat test of the Balance Master System (NeuroCom version 8.1; International, Inc., Clackamas, Oregon, USA). The assessment procedure was completed according to the manufacturer’s instructions. 21 The weight-bearing squat test was repeated twice: first, without wearing PTS and then with PTS. The Balance Master System is a tool to provide quantitative assessment of balance ability and specific movement characteristics during functional activities. This system has been used in the previous studies.7,22 All weight-bearing squat tests were performed on a long force platform comprising two force plates. Force sensors under the force plates measure the vertical forces exerted by the subjects’ feet. This test quantifies the percentage of body weight borne by each leg with the patient standing in three different positions as standing at 0° (knees fully extended), 30°, and 60° of knee flexion. First, every subject was barefoot on a force platform in standing position. In a standing position, they placed feet symmetrically to the reference places on each force plate according to the Balance Master System’s instructions. The patients were instructed to look forward and stand erect and then squat in two positions of knee flexion (30° and 60°). Prior to testing, movement pattern during the test was explained to the subjects. All testing was administered by the primary investigator. However, a second investigator fixed the goniometer on the subject to measure the knee angle. A standard goniometer was used to verify knee flexion angle at each position. We used two trials for the each angle (0°, 30°, and 60° of knee flexion). The first trial was intended to serve as a familiarization with the test and the second trial was recorded as the data point.23,24
WBA is the relative amount of weight borne by each limb during the weight-bearing squat test, expressed as a percentage. It was calculated using the following formula
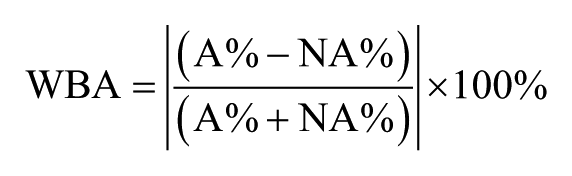
where A and NA represent affected and non-affected sides, respectively. This formula shows the absolute WBA, which indicates absolute differences between the limbs.
Statistical analysis
Statistical analyses were performed using the SPSS software version 15.0 (SPSS Inc., Chicago, IL, USA). Non-parametric tests were deemed more appropriate for statistical analysis due to the small sample size. Medians and interquartile ranges (25th–75th percentile) were used for descriptive analyses of quantitative variables. Wilcoxon signed rank test was used to compare the values of WBA at standing and during squatting with and without PTS. The Mann–Whitney U test was used to compare the descriptive data and decrease in WBA values immediately after wearing PTS during standing–squatting between knee OA patients and healthy subjects. The Chi-square test or Fisher’s exact test was used to compare proportions in different groups. Finally, G*Power (version 3.1.9.2) was used to conduct a post hoc power analysis and calculate the effect sizes. The significance level was set at 0.05.
Results
This study included a total of 10 knee OA patients and 10 healthy subjects. The baseline descriptive data of the participants are presented in Table 1. The baseline WBA values during 30° and 60° of squatting were higher in knee OA patients than in healthy subjects (p < 0.05; Table 1).
Baseline descriptive data of knee OA patients (n = 10) and healthy subjects (n = 10).
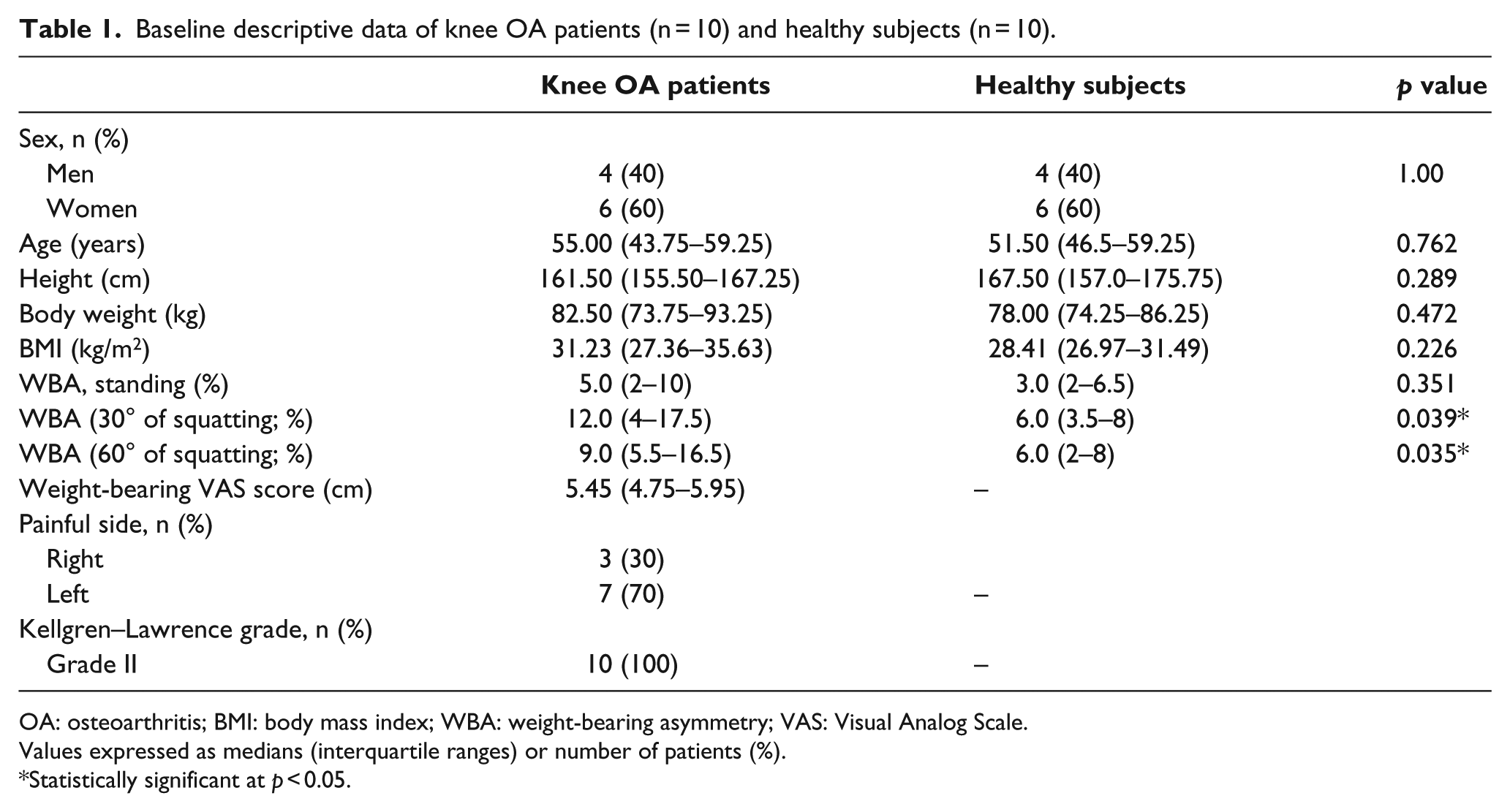
OA: osteoarthritis; BMI: body mass index; WBA: weight-bearing asymmetry; VAS: Visual Analog Scale.
Values expressed as medians (interquartile ranges) or number of patients (%).
Statistically significant at p < 0.05.
WBA values
Changes in WBA values after wearing PTS during standing and squatting are shown in Table 2. With the PTS, the median WBA value during standing was not significantly changed in both groups. The results demonstrated that the WBA between the affected and non-affected sides during 30° and 60° of squatting was decreased immediately with wearing PTS in knee OA patients, but this change was not significant (Table 2; p > 0.05).
Changes in weight-bearing asymmetry values before and immediately after fitting patellar tendon strap (PTS) during standing and squatting.
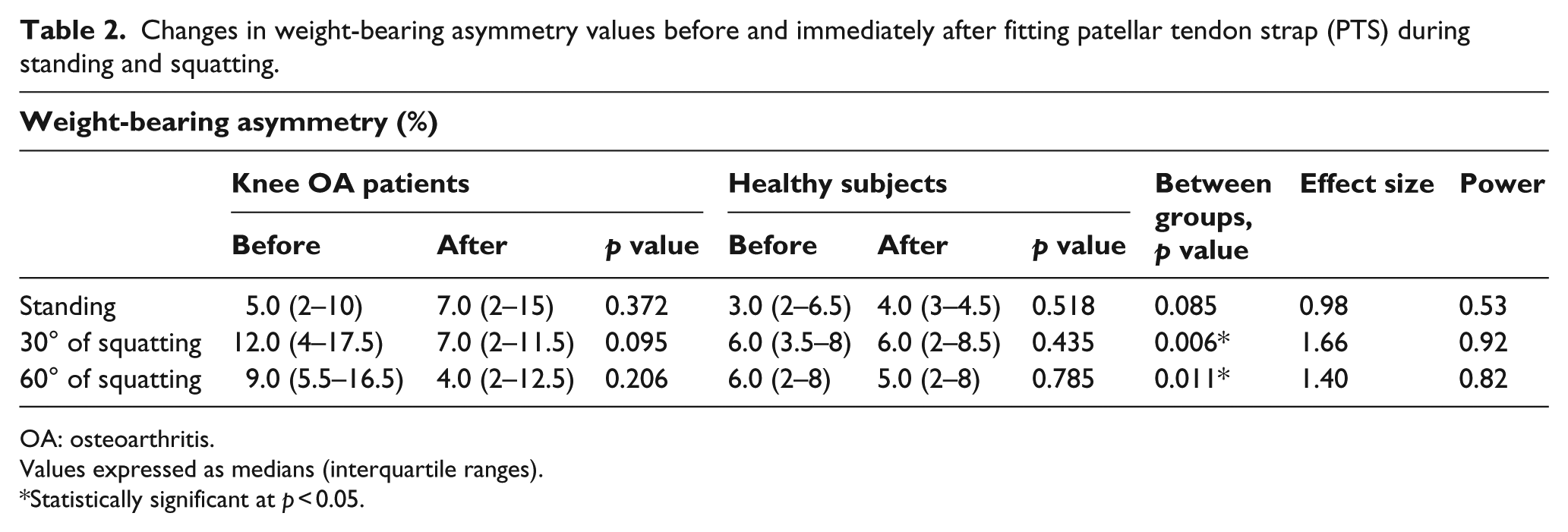
OA: osteoarthritis.
Values expressed as medians (interquartile ranges).
Statistically significant at p < 0.05.
When the two groups were compared, the decrease in WBA values immediately after fitting PTS during 30° and 60° of squatting tests were significantly higher in knee OA patients than in healthy subjects (Table 2; p < 0.05). The effect size and post hoc power analysis report is tabulated in Table 2.
Figures 3 and 4 show that there was an increase in percentage of body weight borne by the affected knee with PTS during 30° and 60° of squatting but the difference was not statistically significant (p > 0.05).
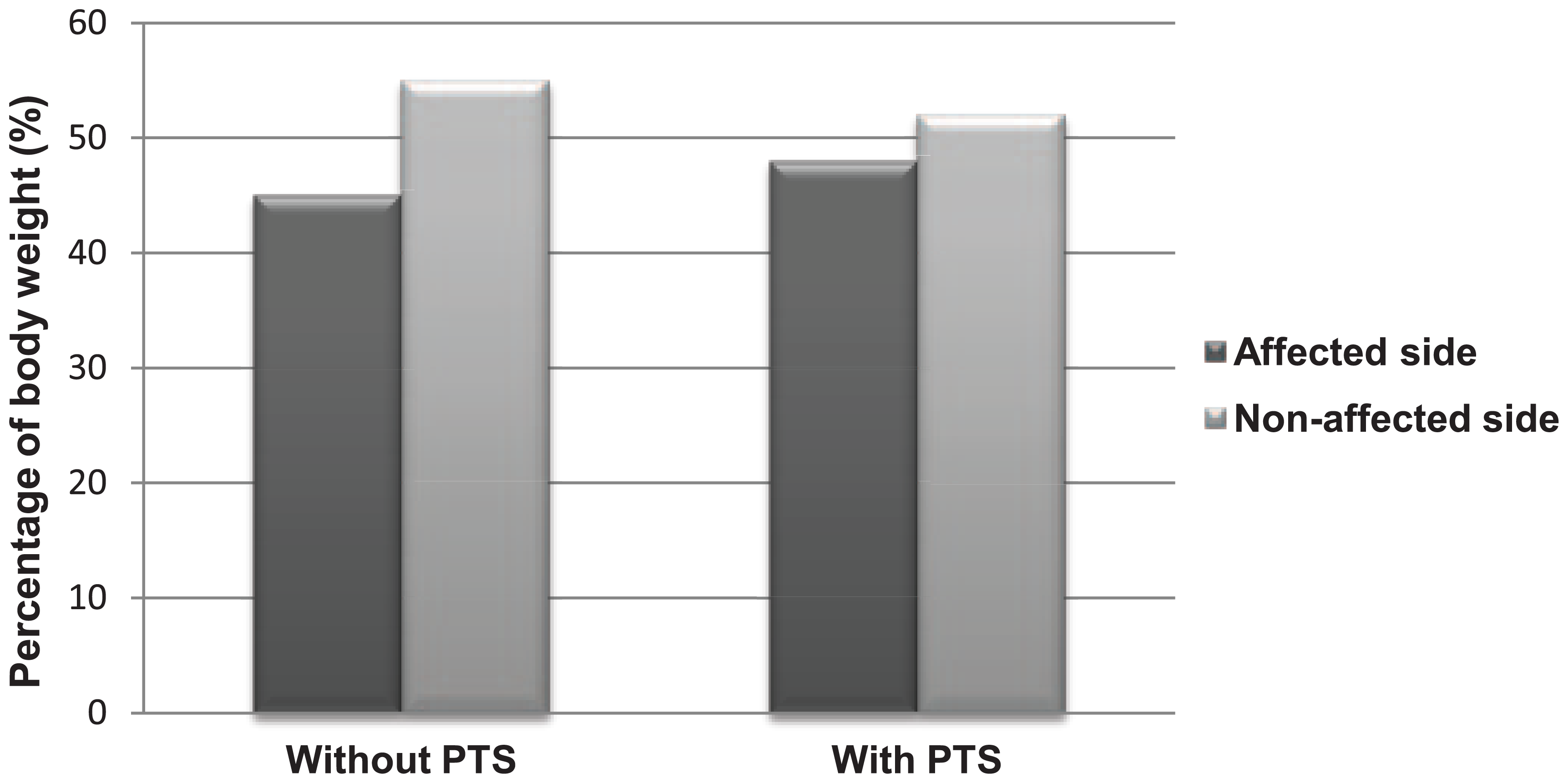
Percentage of body weight borne by affected and non-affected sides during squatting at 30° of knee flexion in knee OA patients. No significant difference between the unstrapped and strapped conditions. Values are expressed as medians.
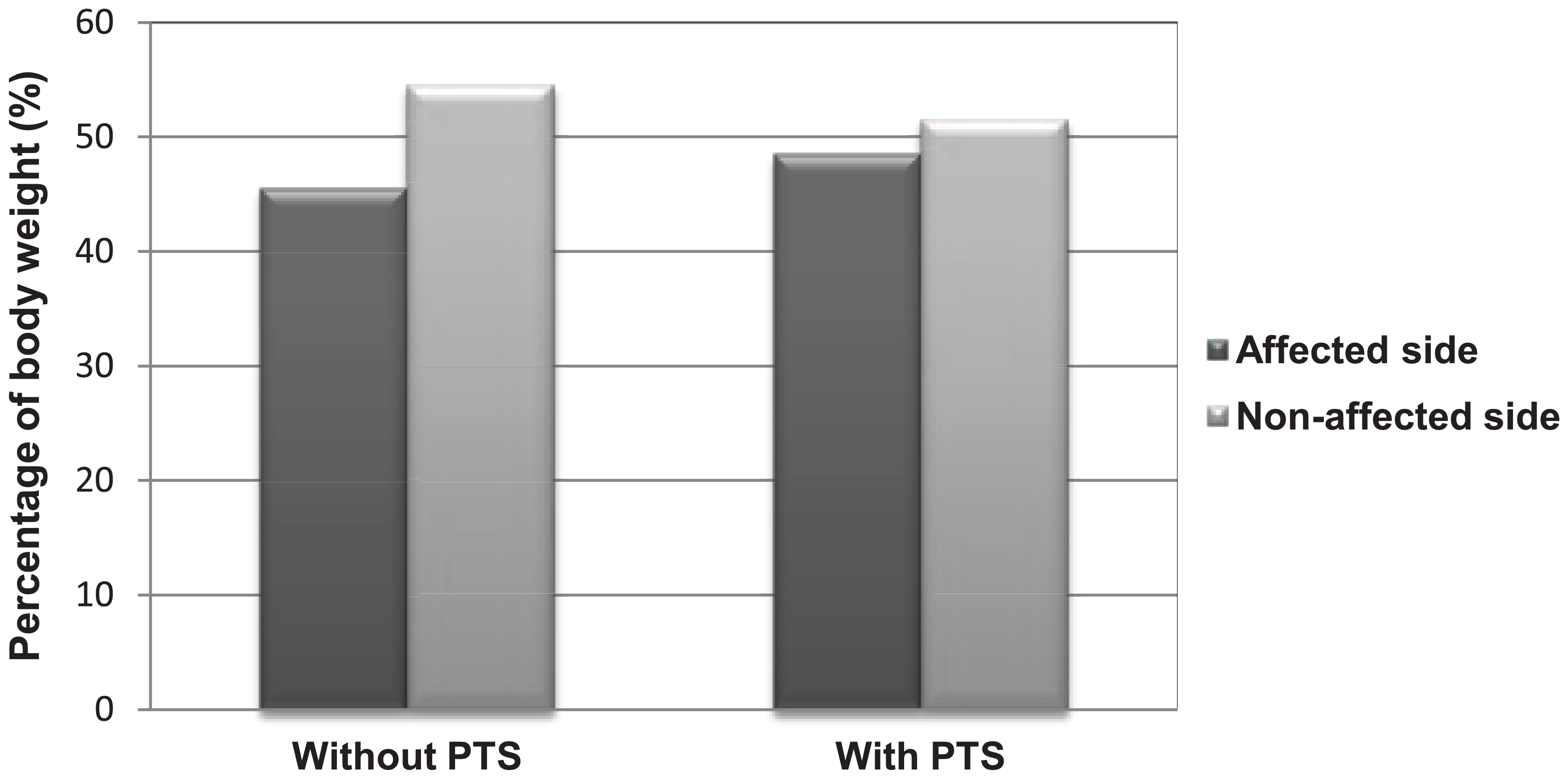
Percentage of body weight borne by affected and non-affected sides during squatting at 60° of knee flexion in knee OA patients. No significant difference between the unstrapped and strapped condition. Values are expressed as medians.
Reported pain intensity
Reported pain intensity was similar in unstrapped (median = 6.00) and strapped (median = 5.70) conditions in knee OA patients (p = 0.066).
Discussion
It was hypothesized that wearing PTS on the affected side in patients with unilateral knee OA would immediately decrease the WBA during 30° and 60° of squatting. We have found supporting results to our hypothesis since the decrease in WBA immediately after wearing PTS during 30° and 60° of squatting test was significantly greater in knee OA patients than in healthy subjects.
The results of this study revealed that people with knee OA involved in the study bore approximately 45% of their body weight on their affected knee and 55% on the unaffected side during 30° and 60° squatting (Figures 3 and 4). WBA during various functional tasks in relation to knee OA has been well documented in previous studies.18,22,25,26 Recently, Christiansen and Stevens-Lapsley 27 have demonstrated that people with knee OA loaded their affected limb on average at 87% of the non-affected limb during a five times sit-to-stand test. In addition, according to the study by Lim and Lee, 22 elderly women with knee OA bore less weight on their affected side with significant differences during squatting movement. The acceptable body weight percentage for healthy individuals is within ±7% of equal weight on the both sides over the full range of squatting positions. 21 The healthy control group in this study maintained their WBA within 7% for all of the testing positions (Table 2). The knee OA patients indicated 5% WBA during standing, while they reached 12% and 9% for 30° and 60° of squatting, respectively. This shows that weight-bearing differences are not detectable in less challenging positions as standing. 21 Moreover, Rossi et al. reported that standing position was not a good indicator of how patients with total knee arthroplasty distribute their body weight on both lower extremities. They suggested to use squatting movement to clinicians to get information on disability after arthroplasty surgery. 7
Strategies to reduce WBA during daily functional tasks such as squatting should receive a great deal of interest, since it has been reported that asymmetrical loading of body weight distribution may lead to secondary physical impairments such as OA of the unaffected side. 28 Arendt et al. 29 emphasized that the strongest modifiable risk factor for knee OA development and progression is chronic biomechanical abnormalities of the knee joint that may include biomechanically over weight loading on the knee. Moreover, WBA potentially increases the risk of further injuries and falls. 19 Squatting, involved in most of the daily activities, is a task that places greater demand on the individual knee joint and may cause more inter-limb WBAs compared with less demanding activities. Minimizing the WBA during squatting movement may help preserve the healthy condition of the unaffected side. 17 It is important to note that pain has been accused of causing a WBA during weight-bearing activities in people with unilateral musculoskeletal problems as knee OA. 18
Since PTS has long been used as a part of conservative management techniques of knee pain resulting from a variety of conditions related to knee joint,5,11,14,30,31 we planned to test its usefulness in people with unilateral knee OA. The underlying mechanism of using PTS in knee pain management is partially explained by several changes related with the patella, 13 but still how this improvement in pain relief occurs is unclear. In this study, PTS had been thought to be a possible treatment approach to reduce pain and therefore it was expected that PTS might also have a positive effect on WBA during squatting in people with knee OA. Unexpectedly, PTS applied on the affected knee did not influence the reported pain intensity arising from osteoarthritic knee of the patients. However, the results showed that people with knee OA in our study were immediately able to reduce inter-limb WBA at 30° and 60° squatting after PTS intervention compared to baseline values and significantly higher than the healthy control group. Reduced weight bearing on one leg is not caused by only pain, it may also reflect proprioceptive or strength loss of the affected limb. 21 Regardless of pain, PTS had some minor impact on inter-limb WBA during squatting movement. In that case, PTS on the affected knee might have improved periarticular sensorimotor function and proprioception, 32 therefore more symmetrical weight bearing might be achieved. De Vries et al. 33 demonstrated that a patellar strap improved the proprioception of the knee joint even in healthy individuals. Unfortunately we did not check proprioceptive and strength loss of the affected knee in this study.
There were some other limitations to this study. We did not randomize the order of intervention throughout testing, and all subjects began the testing procedure with an unstrapped condition. However, we chose to study the no strap condition prior to the strap condition because this order is aligned with the application of this treatment strategy. This assessment order might have affected the performance of patients. All the patients met with the inclusion criteria were included in the study regardless of their WBA percentages before testing. Future studies with larger sample size without these limitations are required.
However, so far no studies have assessed the effect of using these straps during squatting in people with knee OA although they primarily suffer from movement evoked knee pain. This pilot study is the first one that draws attention to the use of PTS during squatting with osteoarthritic knee. We cannot speculate on the usefulness of wearing PTS in people with knee OA for activities involving squatting based on our results, but we can suggest that future researches with larger sample sizes investigating the effect of PTS on WBA during functional activities in people with knee OA are highly warranted. Recalling that Osteoarthritis Research Society International and The European League Against Rheumatism strongly advocate the non-pharmacological approaches for treating OA,34,35 it is important to conduct studies investigating the effectiveness of such treatment methods. PTS is superior to other types of knee braces in terms of simple design, easy fitting, and affordable cost. 12 Further studies focusing on individuals with knee OA will help to identify movement alterations and potential benefits of wearing PTS in this population.
Conclusion
In conclusion, this pilot study provides new insight into the use of PTS in patients with knee OA. Our findings showed that use of PTS in people with knee OA led to more reduction in WBA during squatting movement compared to healthy individuals. Although there is a wide range of use of PTS in knee pain management, studies that investigate the effect of wearing PTS on physical functions are lacking. Hence, further studies should be conducted to verify the effect of PTS on physical functions of people with knee OA.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.