
Abstract
Background:
Chronic ankle instability is associated with neuromechanical changes and poor postural stability. Despite variety of mechanisms of foot and ankle orthoses, almost none apply comprehensive mechanisms to improve postural control in all subgroups of chronic ankle instability patients.
Objectives:
The purpose of this study was to investigate the effect of an ankle support implementing combined mechanisms to improve postural control in chronic ankle instability patients.
Study design:
Cross-sectional study.
Methods:
An ankle support with combined mechanism was designed based on most effective action mechanisms of foot and ankle orthoses. The effect of this orthosis on postural control was evaluated in 20 participants with chronic ankle instability and 20 matched healthy participants. The single-limb stance balance test was measured in both groups with and without the new orthosis using a force platform.
Results:
The results showed that application of combined mechanism ankle support significantly improved all postural sway parameters in chronic ankle instability patients. There were no differences in means of investigated parameters with and without the orthosis in the healthy group. No statistically significant differences were found in postural sway between chronic ankle instability patients and healthy participants after applying the combined mechanism ankle support.
Conclusion:
The combined mechanism ankle support is effective in improving static postural control of chronic ankle instability patients to close to the postural sway of healthy individual. the orthosis had no adverse effects on balance performance of healthy individuals.
Clinical relevance
Application of the combined mechanism ankle support for patients with chronic ankle instability is effective in improving static balance. This may be helpful in reduction of recurrence of ankle sprain although further research about dynamic conditions is needed.
Background
The postural control system preserves postural equilibrium during all motor activities. 1 The postural control system utilizes multisensory integrated information (vestibular, visual, and somatosensory) and the body’s internal orientation to regulate body’s position in space. 2
Postural control impairments are common in patients with various orthopedic injuries, such as lumbosacral pain, anterior cruciate ligament injuries, and ankle sprains. 3 Postural stability deficits are suggested as risk factors after ankle sprains. 4 One of the most important consequences of ankle sprain is chronic ankle instability (CAI) that is associated with poor postural stability. 5
CAI is characterized by ankle pain, instability, giving way, and recurrent ankle sprain and may cause withdrawing from sport and occupational activities in some cases.6,7 Due to the high prevalence and impact of CAI on society and the healthcare system, substantial research has been conducted into prevention, treatment, and rehabilitation of CAI and its corresponding consequences.
Previous studies speculated that recurrent episodes of instability are due to neuromechanical changes in performance of motor tasks in CAI patients.8,9 CAI patients are not homogeneous. Various categorical descriptions have been introduced for this population. All CAI patients have a history of an initial ankle sprain, but secondary complications might differ according to functional or mechanical insufficiencies. Several studies show that there are more subgroups of these patients than those were suggested by Hertel’s 10 original model consisting of three subgroups. Hiller et al. 11 suggested seven subgroups of individuals with CAI by refining the model of categorizing CAI. This difference among these classifications is dependant on mechanical or functional insufficiency caused by initial ankle sprain and should be considered in selecting best prevention and treatment method for these patients.
Restoration of balance and postural control are fundamental in rehabilitation of ankle instability. As CAI is related to neuromechanical changes, the aim should be to restore normal neuromechanical control. 12 Early rehabilitation phases including improvement of postural control, positional sense, and postural reflex could be effective in decreasing recurrence of injury. 13 Different therapeutic treatments are available for CAI patients to address deficits. Orthotic devices are common interventions to prevent reoccurrence of ankle sprain and improve ankle stability in patients with CAI due to their adjustability, cost-effectiveness, ease-of-use and convenience.14–16
Many studies have addressed the effect of orthotic devices on postural control of individuals with and without a history of ankle sprain and those categorized in different subgroups of CAI. One of these devices is an ankle brace which could improve mediolateral (ML) support for the ankle complex. These types of orthoses confer a significant restriction of ankle inversion that limits excessive ankle range of motion (ROM) in the sagittal and frontal planes.14,17 Also, they may provide more favorable alignment prior to initial contact, decreased angular velocity, and change in neuromuscular activity.18,19 Moreover, ankle supports not only provide mechanical stability but also increase proprioceptive inputs by stimulating cutaneous and joint mechanoreceptor and skin plantar receptors.20,21 Foot orthoses maintain hind foot alignment in a more natural position and decrease ROM of the subtalar joint. 22 These devices also could improve function of ligamentous mechanoreceptors and increase afferent signals delivered to the mechanoreceptors or skin receptors. Furthermore, they enhance tactile sensation in the plantar surface of the foot and reduce muscle strain at the ankle. 23
Despite variety in action mechanisms of foot and ankle orthoses, none could apply all the above mechanisms to improve postural control in all subgroups of CAI patients. Prescribing orthoses for these patients needs specific customization because of variability in CAI patients, as mentioned previously, due to existent mechanical and/or functional insufficiency. The customization process is costly and time-consuming. For these reasons, using an orthotic device that could provide a comprehensive mechanism to improve CAI patients’ deficits may be helpful. The aim of this study was to evaluate an orthotic device that could apply most effective mechanisms for improving postural control in CAI patients with different insufficiencies.
Methods
The related literature that investigated effects of various foot and ankle supports on balance and postural control in subjects with history of ankle sprain and different subgroups of CAI were reviewed. Results of this review indicated that the most efficient mechanisms can be classified into three categories including realigning foot or ankle joints, structural support of foot and ankle complex, and improving sensotactile and sensorimotor function.17–27
In next step, more detailed studies were performed to find the best available methods to exert these mechanisms. In this regard, molded foot orthoses were found as the best devices to realign foot and ankle joints by maintaining their neutral position at the subtalar joint.22,23 Also, the investigations indicated that ankle braces with stirrup form design, for example, Element (DeRoyal Industries, Inc., Rowell, TN, USA), Ankle X (McDavid, Woodridge, IL, USA) and Richie Brace Standard (Richie Brace, Inc., Seal Beach, CA, USA), could provide the best ML support for the foot and ankle complex.14,28 In order to improve sensotactile and sensorimotor function, soft ankle supports, for example, Mueller Soft Brace (Mueller Sports Medicine, Inc., Prairie du Sac, WI, USA), RocketSoc Neoprene (DonJoy Orthopedics, Vista, CA, USA), and Arizona Ankle Orthosis (PRO Orthopedic Devices, Inc., Tucson, AZ, USA), were found to be more effective than other orthoses.19,27
An ankle support that could encompass various characteristics of these orthotic types was planned. The ankle support was designed as a custom-made orthosis with three separate sections of footplate, ML stirrup support, and soft ankle sleeve. The footplate section was drafted to maintain hind foot neutral position and support the medial longitudinal arch while extending two-thirds along the plantar foot surface. The footplate was incorporated into the stirrup form sections to provide an integrated base. This combination was done by extending the footplate to the malleolus level medially and laterally. These extensions were designed to make free hinged joints with two medial and lateral shells that covered lower third of the leg. The sleeve section was custom sewn based on ankle and foot dimensions. Two pockets were designed in both sides of the sleeve to encompass medial and lateral support shells. A figure of eight lift strap was included to secure the orthosis around the ankle and increase ankle joint internal pressure to improve sensorimotor function (Figure 1). Appendix A (supplementary material) describes the fabrication process of the Combined Mechanism Ankle Support (CMAS) with more details.

Measuring postural sway during single-limb stance with CMAS orthosis.
A total of 20 patients with CAI and 20 healthy matched individuals were recruited from university communities to evaluate the effect of CMAS orthosis on their postural control. The participants were selected based on the inclusion and exclusion criteria that were suggested by the International Ankle Consortium. The inclusion criteria for the CAI group were at least one significant ankle sprain with continuing feeling of instability and/or ankle giving way. They should acquire a c score of <24 from Cumberland Ankle Instability Tool (CAIT), <90% from activities of daily living subscale, and <80% from sport subscale of Foot and Ankle Ability Measure (FAAM). The healthy individuals were included in the study when there was no history of ankle sprain, sensation of giving way, acquired CAIT score of >27, FAAM score of >90%, and >80% for activities of daily living and sport subscales, respectively. The exclusion criteria for both groups were history of previous surgeries to the musculoskeletal structures, fracture in either lower extremity or acute injury to musculoskeletal structures of other joints of the lower extremity in the previous 3 months. No participant had experience of orthotic use. The characteristics of participants are displayed in Table 1. All participants signed an informed consent that was approved by the University of Social Welfare and Rehabilitation Sciences.
Participant demographics.
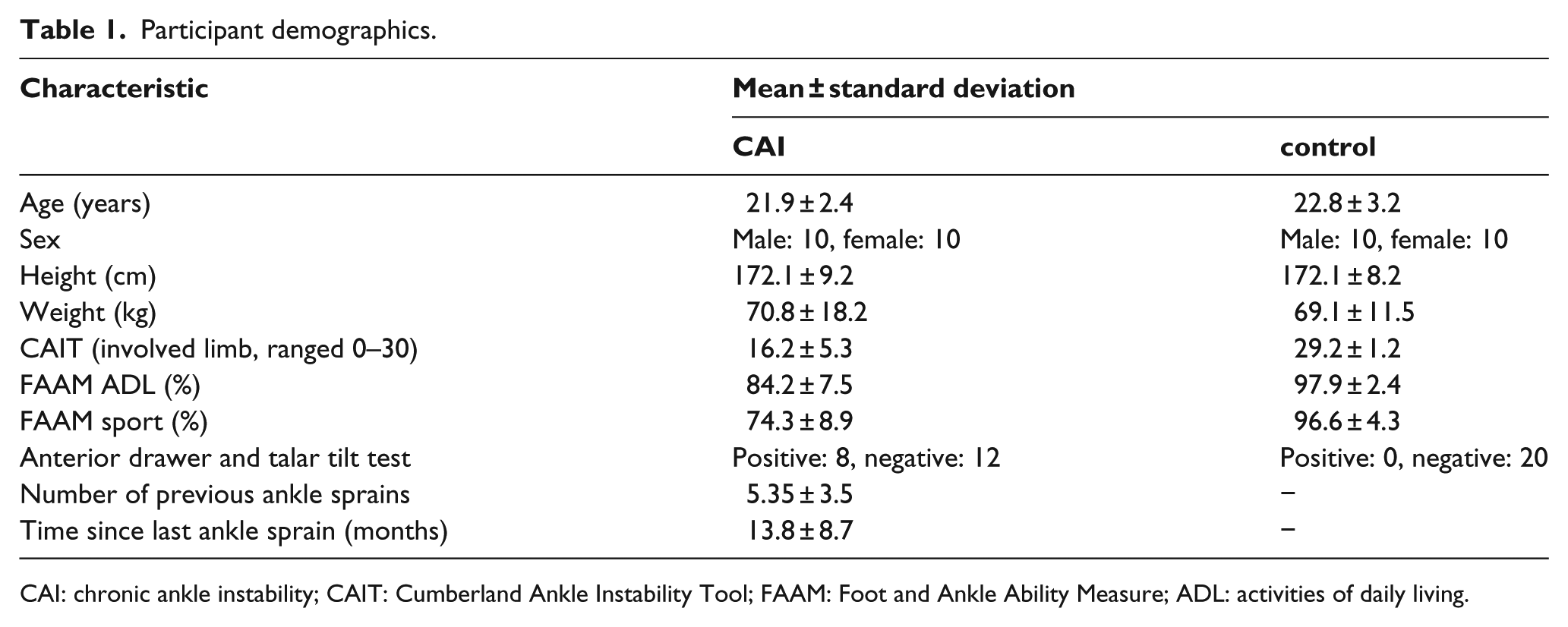
CAI: chronic ankle instability; CAIT: Cumberland Ankle Instability Tool; FAAM: Foot and Ankle Ability Measure; ADL: activities of daily living.
Each participant was evaluated in two separate sessions. In the first session, a professional practitioner checked the participants regarding the inclusion and exclusion criteria and asked them to complete CAIT and FAAM questionnaires for evaluation of any functional instability and the level of disability, respectively. The talar tilt and anterior drawer tests were also performed to investigate presence of any mechanical instability. The anterior drawer test was performed by pulling the calcaneous and talus in the anterior direction while stabilizing the distal tibia and fibula. This test evaluates the integrity of the anterior talofibular ligament. The talar tilt test, that assessed the calcaneofibular ligament, was performed by inverting the calcaneous and talus while stabilizing the distal tibia and fibula. 29 In the next step, a negative cast of the foot was made by a professional orthotist for fabrication of the orthosis.
After preparation of the ankle support, the postural control of participants was evaluated in a separate session. To gather center of pressure (COP) data, a Kistler 9286 BA piezoelectric force platform, Kistler 9865 charge amplifier, and Kistler 5691 A data logger (Kistler, Winterthur, Switzerland) were used.
Before starting the test session, each patient practiced with their own fabricated CMAS for 15 min. Participants were instructed to adopt single-leg stance with their involved limb on the force platform. They were asked to look forward and hold their unsupported leg approximately in 30° of hip flexion and 90° of knee flexion. The participants preserved this position for 25 s. The trials were discarded and repeated if the unsupported leg touched the weight-bearing foot or force platform. Three trials were performed in each with and without orthosis condition. Rest periods of 30 s between trials and 2 min between conditions were considered to minimize fatigue effects. The orders of conditions were selected randomly for each person to control possible practice effects.
The force platform signals were sampled at 100 Hz. The obtained signals were filtered with a fourth-order zero-phase Butterworth low-pass filter with a cut-off frequency of 5 Hz. For computing COP parameters, mean total velocity, phase plane portrait, and standard deviation (SD) of velocity in anteroposterior (AP) and ML directions, the data were exported to EXCEL. The phase plane portrait considered both amplitude and velocity in analysis and infolded static and dynamic aspects of postural control. 30 These COP parameters were selected due to their capability of measuring different aspects of postural behavior and their respective high reliability. 3
The mean for the three trials of COP parameters in each condition was used for statistical analysis. Independent t-tests were used to compare measured parameters between CAI and healthy individuals. Paired sample t-tests were done to compare measured parameters between orthosis and no orthosis conditions. Modified Bonferroni was used to adjust multiple test alpha levels to maintain experiment-wise p ⩽ 0.05. All data were analyzed using SPSS version 16.0 (SPSS, Inc., Chicago, IL, USA).
Results
There were no statistically significant differences between CAI and healthy participants related to matched characteristics, age (p = 0.29), height (p = 0.97), and weight (p = 0.35). In contrast, statistically significant differences were found between the two groups for CAIT, FAAM activities of daily living, and FAAM sport score (p < 0.001).
In single-leg stance without orthosis, all postural sway parameters of CAI patients were significantly more than the healthy group (p < 0.01). Although the results show higher postural sway in CAI group with CMAS orthosis, no significant difference was found between healthy and CAI groups with CMAS orthosis. Also, all sway parameters in CAI patients with CMAS orthosis were lower than without CMAS orthosis condition. These differences were significantly lower than alpha level of 0.02. In addition, there were no significant differences in the healthy group between two orthotic conditions (Table 2).
Mean (SD) of sway parameters with associated p value for CAI and control group in with/without orthosis conditions.
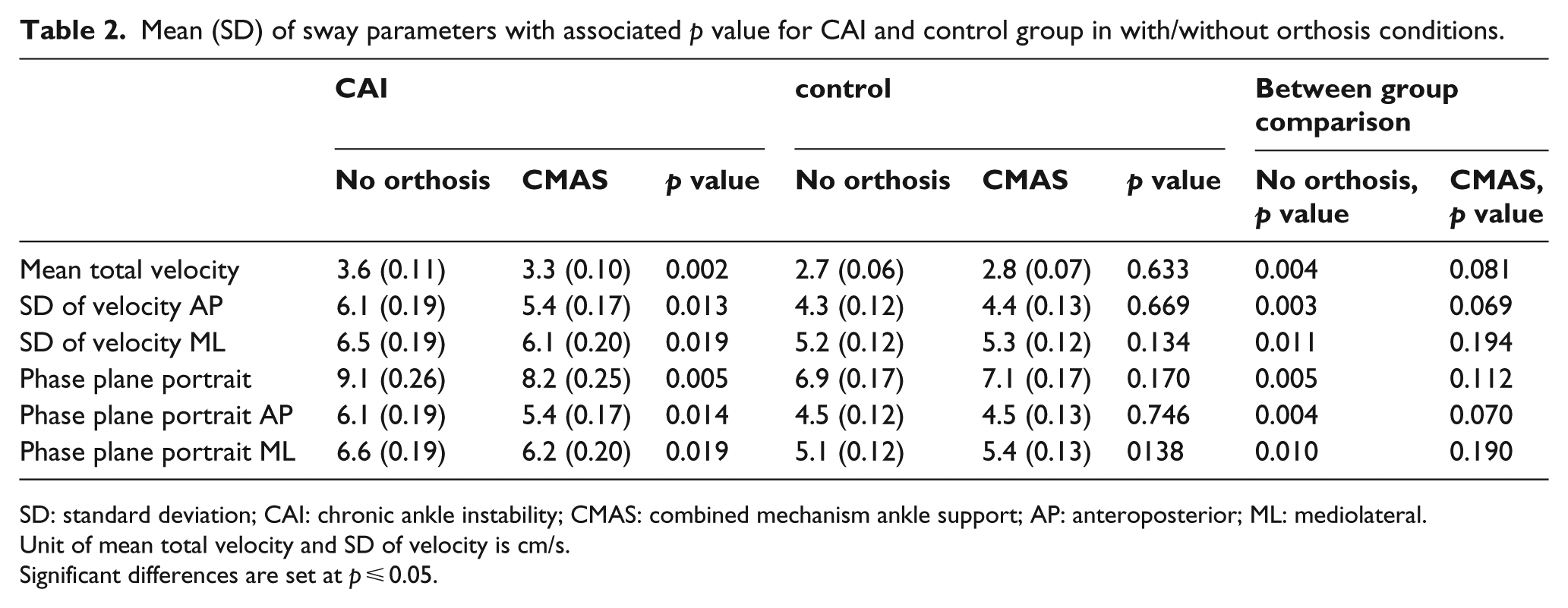
SD: standard deviation; CAI: chronic ankle instability; CMAS: combined mechanism ankle support; AP: anteroposterior; ML: mediolateral.
Unit of mean total velocity and SD of velocity is cm/s.
Significant differences are set at p ⩽ 0.05.
Discussion
The CMAS orthosis was purposed to provide a comprehensive action mechanism for improving postural control deficit of CAI patients. As mentioned above, this orthosis was designed and fabricated based on most accepted and effective action mechanisms recommended in previous studies. The aim of the design was to provide ML support for the ankle complex, control excessive ROM, maintain the subtalar jpoint and hind foot in neutral alignment, and provide sensotactial and proprio-ceptive stimulation. With respect to these objectives, appropriate components and materials were selected and the orthosis was fabricated.
The design of CMAS is similar to other stirrup form orthoses (DeRoyal Element, McDavid Ankle X, and Richie Brace Standard). The main characteristic that differentiates the CMAS from others is the application of combined mechanisms in its design. The footplate section of CMAS, unlike DeRoyal Element and McDavid Ankle X, is fabricated based on the patient’s foot cast to provide better subtalar control. Also, a modified ankle joint base is considered in this design to place the hinge axis in more anatomical position. The joints were formed on platforms that were constructed on the patient’s plaster mold at the malleolus level. In addition, unlike DeRoyal Element and Richie Brace Standard, the CMAS benefits from a sleeve section that is designed to provide sensotactial and proprioceptive stimulation. Moreover, as an exclusive feature of the CMAS design, a figure of eight lift strap was added to increase internal joint pressure.
Since the ultimate goal of the CMAS orthosis was to improve postural control in CAI patients, its impact on postural sway measurements were chosen as the definitive outcome in this study. The postural sway parameters were assessed in healthy individuals in addition to CAI patients to address the need for use of a healthy reference group in evaluation of postural impairments.27,31 The CAI group had lower scores of CAIT and FAAM questionnaires that were significantly different from scores acquired by healthy group. All evaluated postural sway parameters were significantly higher in the CAI group than healthy participants. The results of this are study in general agreement with the previous literature which demonstrated that CAI patients had more postural instability rather than healthy individuals.1,9,12 This supports the conclusion that postural control deficits are associated with CAI patients.
The healthy group demonstrated no significant difference in investigated parameters with and without orthotic use. This result was in line with findings of other studies that demonstrated soft and semirigid ankle orthoses have no effect on postural sway of healthy participants.32,33 No change in postural sway of healthy individuals after application of orthosis may be due to optimal stability in this group. 32 Although Hadadi et al. 27 reported that soft and semirigid ankle orthoses had adverse effect on postural sway of healthy individuals, no similar effect was seen in this study for CMAS orthosis. This may be because of differences in the designs of orthoses in the two studies.
Evaluation of sway parameters related to velocity (mean total velocity, SD of velocity in AP and ML directions) in CAI patients before and after application of CMAS orthosis demonstrated that there were significant differences between the two conditions. The means of these measures were lower after applications of the CMAS orthosis. Similar results were obtained for total phase plane portrait and phase plane portrait in AP and ML directions. These results indicate that CMAS orthosis may be effective in improving postural control in individuals with CAI. Similar findings were reported by previous investigators that evaluated the influence of ankle and foot orthoses on postural sway within some subgroups of CAI patients. Although they investigated patients with functional ankle instability (FAI), Hadadi et al. 27 found improved postural control by using the Arizona ankle orthosis and active ankle brace, with a more pronounced effect observed while wearing a soft orthosis in this type of ankle instability. They suggested that enhancement of mechanical support and proprioceptive or exteroceptive input may be achieved by these orthoses. Hamlyn et al., 24 who investigated the effect of a quick comfort insole on postural stability, demonstrated that prefabricated orthoses can be considered as a treatment method to improve postural stability in patients with FAI. They hypothesized that these orthoses may improve postural stability by placing the hind foot in a more stable position. It seems that the CMAS orthosis, by providing similar mechanisms, was effective in decreasing postural sway in CAI individuals in this study.
No significant differences in postural sway parameters between healthy and CAI group were found after application of the CMAS orthosis in this study. Although the means of all evaluated parameters with the new orthosis in the CAI group were higher than in the healthy group, no statistically significant differences were found. As previous literature demonstrated, CAI patients have mechanical and/or functional insufficiencies that are caused by structural loss of ankle ligaments, abnormal alignment of ankle and hind foot, and loss of neuromuscular control after ankle sprain.8–10 The CMAS orthosis was designed to meet most of these demands. Therefore, each section of this orthosis was considered to address one or two of the above requirements. For example, the foot section was designed to restore subtalar and hind foot alignments; the stirrup form of its rigid section was designed to structurally support the ankle complex, and the sleeve part was constructed to stimulate skin and muscle mechanoreceptors. The results demonstratee that this orthosis was effective in improving balance and decreasing postural sway of CAI patients to values close to a normal population.
This study has some limitations. The effect of the CMAS orthosis was investigated on static postural control in single-limb stance. Evaluation of the new orthosis in more dynamic conditions may better reflect its effect on dynamic postural stability. In this study, immediate effects of the orthosis on postural sway were investigated. Further research is needed to specify long-term effects of this orthosis on balance control. Also, comparison of the CMAS orthosis with other types of foot and ankle orthoses is required to discern its therapeutic value. Future studies should be carried out to investigate influence of this orthosis on other aspects, apart from postural control, such as mechanical stability.
Conclusion
The CMAS orthosis was designed to address mechanical and functional insufficiencies that are associated with CAI patients to improve postural control in these patients. This orthosis decreased postural sway in CAI individuals, but had no significant effect on a healthy group. The CMAS orthosis is an effective device for improvement of static balance in CAI patients.
Footnotes
Acknowledgements
The experiment was conducted in Biomechanics Lab of University of Social Welfare and Rehabilitation Sciences.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by University of Social Welfare and Rehabilitation Sciences.