
Abstract
Background:
Chronic ankle instability as a prevalent consequence of ankle sprain causes various impairments such as balance and postural control deficits. Foot orthoses are one of the common interventions for rehabilitation of patients with chronic ankle instability.
Objectives:
To investigate the effect of custom-molded foot orthoses with textured surfaces on dynamic balance of chronic ankle instability patients and to compare their effects with other types of foot orthoses.
Study design:
This is a repeated measure design.
Methods:
A total of 30 participants were recruited based on the guideline introduced by the International Ankle Consortium. The effect of prefabricated, custom-molded, and custom-molded with textured surface foot orthoses was evaluated on dynamic balance by the Star Excursion Balance Test. Normalized reach distances in anteromedial, medial, and posteromedial directions of the test were computed to be used for statistical analysis.
Results:
The foot orthoses increased reach distances compared to the no-orthosis conditions in all three directions. The custom-molded with textured surface foot orthosis has significant differences compared with prefabricated foot orthosis (p = 0.001) in all measured directions and with custom-molded foot orthosis (p < 0.01) in medial and posteromedial directions.
Conclusion:
Foot orthoses improve reach distances in patients with chronic ankle instability. Custom-molded with textured surface foot orthosis has a more pronounced effect compared with other foot orthoses.
Clinical relevance
The custom-molded foot orthosis with textured surface could be an effective device to improve dynamic balance in chronic ankle instability (CAI) patients. It may be considered as an efficient intervention to reduce ankle sprain recurrence in these individuals, although further research should be conducted.
Background
Ankle sprain is among the most common sport-related injuries that affect athletes. Most ankle sprains are caused by sudden flexion and inversion of the ankle joint, which impairs the lateral ligamentous structure. 1 Spraining in an injured ankle has a tendency to recur and such repeated injury can cause chronic ankle instability (CAI). 2 Research works have shown that up to 74% of patients who experience an acute lateral ankle sprain suffer from CAI. 3 The CAI is characterized by recurring ankle “giving way,” perceived instability, ligamentous laxity, pain, swelling, and weakness. 4 Reduced function, inability to compete, and negative psychological effects impact athletes with the CAI. 5 Ankle joint osteoarthritis could also be the long-term effect of the CAI. 6
Static and dynamic postural control deficits are well-documented consequences of CAI.7,8 Restoration of balance and postural control are fundamental in rehabilitation of ankle instability. 9 Orthotic devices are common therapeutic modalities that are used in CAI patients. Various orthotic devices such as ankle support and foot orthoses (FOs) have been suggested for improving postural control deficits in these patients.8,10
Many studies confirm the efficacy of ankle supports in postural stability enhancement,10,11 but these devices limit the ankle joint motion and they may have the potential to damage knee joints due to possible changes in the lower-extremity close kinematic chain.12,13 FOs are another accepted orthotics interventions for preventing the reoccurrence of ankle sprain and improving ankle stability in patients with CAI. These devices are more considered due to their adjustability, cost-effectiveness, ease of use, and convenience, especially for athletes.8,14
The effects of FOs on balance and postural control of CAI patients have been addressed in various studies. Hamlyn et al. 14 showed that the prefabricated FO improved the static postural stability in CAI patients. Sesma et al. 8 revealed the beneficial effect of custom-molded FOs on the Star Excursion Balance Test (SEBT) performance in patients with CAI. Furthermore, McKeon et al. 15 found that the textured FO had a detrimental effect on the time-to-boundary test. Contrary to the consensus in literature about effectiveness of FOs on improvement of dynamic balance in CAI patients, it is not clear which ones have the most efficiency.
Each FO, based on its design, has a specific action mechanism that impacts the final effect of the device. FOs could be purposed to control foot motions, reduce biomechanical stresses, and/or support the arches of the foot. 16 In addition to providing mechanical stability, FOs also may also target to increase proprioceptive inputs, increasing the contact area at the plantar surface of the foot and stimulating cutaneous and skin plantar receptors. 17
Among introduced FOs, custom-molded FOs and textured insoles have been examined more closely in research works. Custom-molded FOs had more emphasis on restoring normal foot alignment, while the textured insoles have been investigated to influence somatosensory systems. CAI patients may face various insufficiencies (functional, mechanical, or both) that may not be treated optimally with the same types of FOs. Adding a textured surface into the custom-molded FO could perhaps increase the beneficial effect of the orthosis for such patients. As far as the authors are aware, there is no study in the literature that has investigated the supplementary effect of custom-molded FOs with a textured surface on dynamic balance of CAI patients.
Also, despite many studies have compared the effect of FOs on static and dynamic postural control in individuals with acute lateral ankle sprain,18,19 no study has compared the effects of such orthoses on the dynamic postural stability of CAI patients. Therefore, the purpose of this study was to evaluate and compare the effect of a prefabricated FO, a custom-molded FO, and a custom-molded with textured surface FO on dynamic postural control of individuals with CAI to find more efficient FO.
Methods
A total of 35 physical education students with CAI were recruited for this study. Five participants left the study between the casting and testing period due to re-injury or disinclination to participate in the research. The characteristics of the participants are shown in Table 1.
Participant demographics.
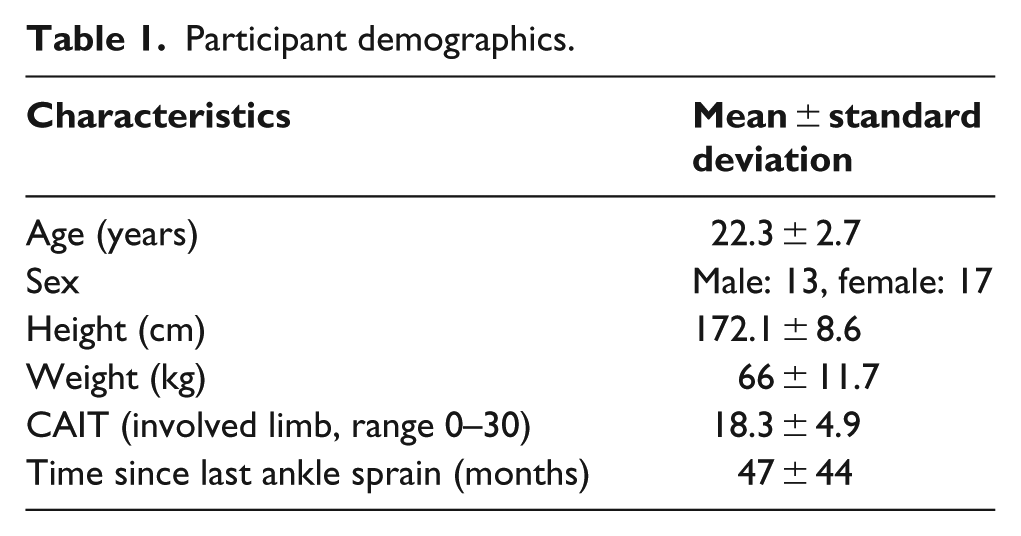
The selection of participants was based on the guideline introduced by the International Ankle Consortium. 20 The individuals must have at least one significant ankle sprain that had occurred 12 months or more prior to the study, with continuing feeling of instability and/or ankle giving way. They reported at least two times feeling of giving way in the 6 months leading to the study and the last ankle sprain occurrence was at least 3 months before the study. All participants acquired a score of less than 24 from the Cumberland Ankle Instability Tool (CAIT). In addition, the participants had no history of surgeries, fractures, or acute injures on the musculoskeletal structures of their lower extremity. They also had no uncorrected visual impairment, vestibular or respiratory disorders, or anything that influences their balance such as medicines. This study has been approved by the University of Social Welfare and Rehabilitation sciences ethics committee.
Three types of FOs are used in this study (Figure 1). The first FO was a prefabricated, full-length, semi-rigid insole (Slimflex; Algeos UK Ltd, Liverpool, UK) manufactured with ethylene-vinyl acetate (EVA). Its deep heel cup is designed to support the heel-and-subtalar joint. A custom-molded FO, which was made of 3-mm-thickness polyethylene, was considered as the second option. It was extended to the metatarsal head and the depth of its heel cup was considered 2 cm to support the heel better. This FO was trimmed medially and laterally beneath the malleolus to support medial and lateral longitudinal arches. An impression of the foot was made for fabrication of the custom-molded FO. The third FO was prepared by adding a layer of 3-mm-thick EVA foam (shore A50) with raised semi-circular points with 3 mm diameter, 1 mm height, and center distances of 5 mm to the inner surface of the custom-molded FO. 21

The investigated foot orthoses: (a) custom-molded with textured surface foot orthosis, (b) custom-molded foot orthosis, and (c) prefabricated foot orthosis.
Following the consent of individuals with CAI to participate in the study, they were investigated regarding the inclusion and exclusion criteria, and they were asked to fill out the Persian version of the CAIT questionnaire for evaluation of any functional instability. 22 In the next step, a negative cast of the foot was made by a professional orthotist for fabrication of the custom-molded FO. In order to minimize inconsistency, all castings were done by one orthotist. The impression was made while the patient was seated with the subtalar joint in the neutral position, the midtarsal in maximum pronation, and the first ray in neutral.
Since it has been mentioned that static tests might not challenge the postural control system enough and they might not reflect the real situation of activity daily living, therefore, in this study, the SEBT was used to quantify the dynamic postural stability of the athletes. 8 The efficiency of the SEBT to detect balance deficits associated with musculoskeletal injuries like CAI has been verified previously. 23
The SEBT has eight reach directions with a 45° radius from one another with respect to the center. The measurement of dynamic postural control is inferred from how far a participant can reach while maintaining a base of support. Participants performed the test by standing in the middle of a testing grid, placing the geometric center of the stance foot meticulously aligned with the intersection of the lines, and reaching with unaffected foot as far as possible along the desirable direction, and then returning to the starting position. The anteromedial (AM), medial (M), and posteromedial (PM) directions were used in this study based on Hertel et al.’s 24 suggestion that these directions are more affected in patients with CAI. The examiner marked the point where the most distal part of the foot touched on the line and measured its distance to the center of the test in centimeters with a tape measure. Each participant performed three successful reaches for each of the three directions of the SEBT. Prior to formal testing, six practice trials were performed in each direction to prevent the learning effects expressed by Hertel et al. 25
The trial was discarded and repeated if the participants placed excessive weight on the reaching limb, removed the stance foot from the starting position, or lost their balance. Reach distance was normalized to the participants’ leg length in accordance with previously established methods. 26
All participants performed the SEBT without FOs and with any of the prefabricated FO, custom-molded FO, and custom-molded with Textured surface FO while wearing their own athletic shoes. All these four conditions were chosen on a random basis. Rest periods of 30 s, 2 min, and 5 min were considered, respectively, for between trials, between each direction, and between the orthotic conditions to minimize the effect of fatigue.
The SPSS 16 software (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Mean of three trials of normalized reach distance with various FO conditions for each direction was calculated and a repeated measures analysis of variance (ANOVA) was run for each direction. Bonferroni adjustment method was used to assess multiple comparisons. The alpha level was set as 0.05.
Results
Mean and standard deviation (SD) values of normalized reach distance in the M, AM, and PM directions for the CAI participants are shown in Table 2. Repeated measures ANOVA with 95% confidence interval showed significant differences for all orthotic conditions in each of the three directions of the SEBT (p < 0.05).
Mean and standard deviation of CAI patients normalized reach distance in three directions for four orthotic conditions.
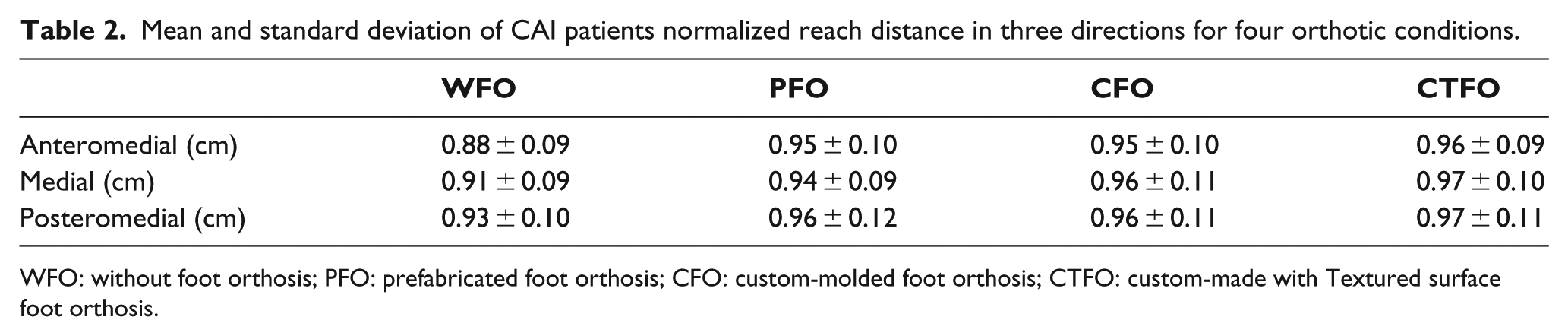
WFO: without foot orthosis; PFO: prefabricated foot orthosis; CFO: custom-molded foot orthosis; CTFO: custom-made with Textured surface foot orthosis.
The post hoc analysis revealed statistically significant differences between orthotic conditions for all reach directions (Table 3). The pair-wise comparison showed that reach distances are larger in all orthotic conditions compared to no-orthosis conditions in the AM, M, and PM directions (p < 0.001). According to the comparison between three FOs, there was a greater reach distance in the custom-molded with textured surface compared with prefabricated FO in the AM, M, and PM directions (p = 0.001). Also, custom-molded with textured surface acquired significantly higher reach distances compared with custom-molded FO in the M and PM directions (p < 0.01). However, there is no difference between any other orthotic conditions in any of three tested directions.
Pair-wise comparison of orthotic conditions for reaches distance in three directions.
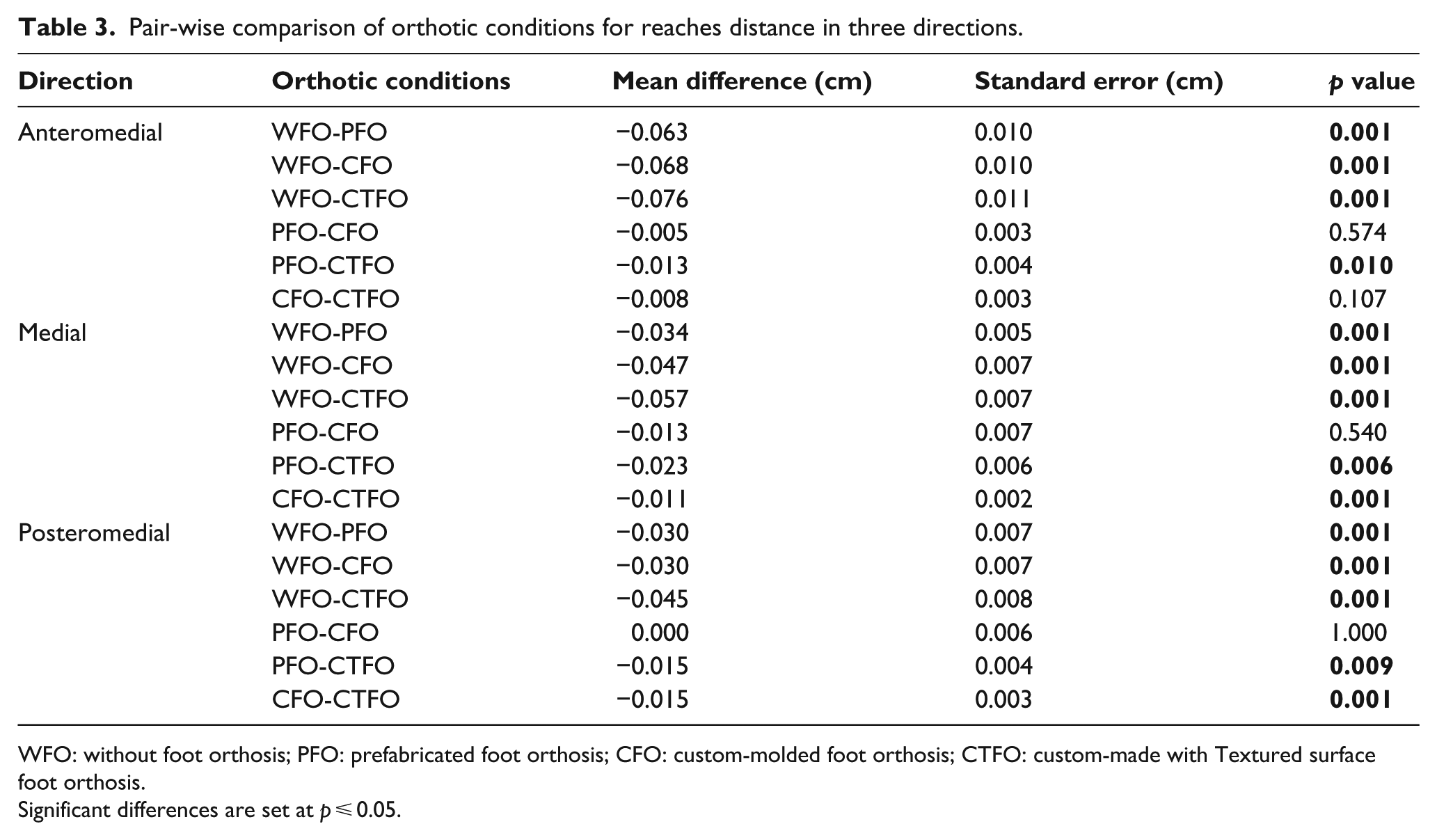
WFO: without foot orthosis; PFO: prefabricated foot orthosis; CFO: custom-molded foot orthosis; CTFO: custom-made with Textured surface foot orthosis.
Significant differences are set at p ⩽ 0.05.
Discussion
Based on the result of this study, all three types of FOs have significant effects on dynamic postural control as measured by the SEBT in patients with CAI. The results also demonstrated a greater effect of the custom-molded with textured surface compared with the prefabricated FO in all three test directions and a greater effect compared with the custom-molded FO in the M and PM directions.
The primary finding of this study was the increase in the reach distance of the CAI patient as a result of using the FOs. This result is in line with previous research which has shown the effectiveness of FOs on the postural control of the CAI patients. It has been suggested that the FOs provide both mechanical and functional changes in the foot and ankle complex of patients with CAI.27,28
It has been emphasized that the prefabricated FO with a deep heel cup can support the subtalar joint in the single limb stance better and can improve postural control in CAI patients. 14
The deep heel cup and calcaneal support of the FOs used in this study can improve the bony congruency of the subtalar joint. The more stable biomechanical position of the subtalar joint may contribute to the improvement of postural control. 29 In addition, lateral ankle sprains create excessive subtalar joint motion and can cause standing talar tilt in the talocrural joint. 30
The second finding of this study was the superiority of the custom-molded with textured surface FO in improving the SEBT performance of patients with CAI in comparison with custom-molded and prefabricated FOs. As all of the three orthoses provide considerable heel cup, it seems that the improvement of the dynamic postural control by application of the custom-molded with textured surface FO may be due to the addition of the textured surface to orthosis.
The positive effect of the textured insole on the improvement of balance has been shown in previous studies.31,32 The proprioception deficit is one of the most common findings in patients with CAI. 33 Standing on the textured surfaces could stimulate the skin plantar receptors of the foot and create changes in the afferent inputs and considerably decrease the postural sway. 21 Corbin et al. 31 proposed a theory that textured insoles are able to compensate the diminished sensory input in patients with poor postural control by surrogating the afferent input from the plantar surface of the foot.
The effectiveness of the custom-molded FO on the SEBT performance in CAI patients was proposed previously. 8 It was suggested that the custom-molded FO enhances the ankle joint mechanoreceptors by restricting the undesirable foot-and-ankle joint motion and providing a better structural support in ankle-injured patients. 27 On the other hand, Orteza et al. 18 demonstrated that the custom-molded FO had a positive effect on improving the standing balance performance in acute ankle-sprained patients, while the prefabricated FO did not. This is the reason for adding the textured surface to the custom-molded FO in this study.
The greater effect of the custom-molded with textured surface FO compared with the custom-molded FO and the prefabricated FO can suggest that the additive effect of these conditions can potentially lead to better performance of FOs on dynamic postural control in patients with CAI. In the recent literature, textured surfaces have been mostly used on bare feet or added into the shoes. The combination of these features may explain the superiority of the custom-molded with textured surface FO in enhancing the SEBT performance compared with other FOs in this study. As there were no differences between the custom-molded and prefabricated FOs in this study, combining the prefabricated FO with the textured surface could be investigated in the future studies.
Since this is the first to compare the effect of FOs on dynamic postural control with using the SEBT in patients with CAI, a direct comparison with other studies is difficult. Orteza et al. 18 found that the custom-molded FO improved the balance in patients with acute ankle sprain, but the prefabricated FO did not. Also, Hertel et al. 19 proposed that none of the five insoles used in their study were effective on improving postural sway after acute ankle sprain. It should be noted that these studies compared the effect of FOs in the static condition which is different from the conditions that were investigated in this study.
It is important to note that this study faced some limitations as well. The current research investigated just the immediate effect of FOs on dynamic postural control and did not evaluate patients’ comfort, functional performance, or injury reduction risk. Future studies should evaluate the long-term effects of the application of these devices. In addition, the individuals participating in the study were young patients and the achieved results might not be applicable to all ages.
Conclusion
The prefabricated, custom-molded, and custom-molded with textured surface FOs can improve the dynamic performance of athletes with CAI. The custom-molded with textured FO is the better choice than two other mentioned FOs to prescribe for these patients, as this FO has greater effect on improving the reach distance of the SEBT directions.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.