
Abstract
Background and Aim:
The socket reaction moments are directly measured at the base of a socket and may be useful for fitting a prosthesis. Previous studies have focused on the effect of prosthetic alignment changes on them. The aim of this study was to explore their range at clinically perceived optimal alignment by investigating the individual differences.
Technique:
In total, 11 amputees using unilateral transtibial prostheses with solid-ankle-cushion-heel (SACH) feet were recruited. The socket reaction moments were measured using a custom instrumented prosthesis alignment component and plotted. Eight variables that were related to their magnitude (N m/kg) and timing (% stance of event) as well as cadence (steps/minute) were calculated for each amputee. Their mean, standard deviation, maximum value, minimum value, and range were subsequently analyzed.
Discussion:
This study may serve as a foundation to explore the range of individual differences in socket reaction moments in transtibial prostheses.
Clinical relevance
Socket reaction moments can be conveniently measured in the clinical setting. Prosthetists could potentially use them as one of the criteria to align prosthesis in addition to observational gait analysis and amputees perception.
Background and aim
Direct measurement of kinetic gait parameters using a load cell integrated to prosthesis may enable convenient quantitative gait analysis in the clinic, and its technique has been explored for various prosthetic devices.1–3 It allows collecting data during various activities without a need for a complex motion analysis laboratory where tested subjects’ activities are restricted by the environment. Socket reaction moments are directly measured at the base of a socket and may represent how a residual limb is loaded inside the socket of transtibial prostheses.4,5 In the sagittal plane, a flexion moment at early stance is followed by an extension moment throughout the rest of stance. In the coronal (frontal) plane, a varus moment is generally dominant during mid-stance. The socket reaction moments are similar to the ankle moment of the prosthesis demonstrated using a three-dimensional (3D) computerized motion analysis system.6,7
The alignment of the transtibial prosthesis has systematic effects on the socket reaction moments.2,8 Therefore, it was suggested that prosthetists could potentially use them to align the transtibial prosthesis. However, it is known that individual responses to alignment changes could be unique.3,9 It is also expected that an optimal alignment of the transtibial prosthesis is somewhat unique to each amputee. Therefore, analyzing the individual differences may provide prosthetists additional information to use the socket reaction moments for prosthetic alignment. The ability to measure socket reaction moments may also be useful for promoting smooth and efficient gait as well as reducing discomfort at a residual limb–socket interface, although additional work is required to support these claims. Investigating the range of individual differences of the socket reaction moment in clinically aligned prosthesis may contribute to a personalized care for amputees based on evidence. The aim of this study was to explore the range of socket reaction moments by investigating the individual differences at clinically perceived optimal alignment agreed upon by a prosthetist and an amputee.
Technique
Subjects
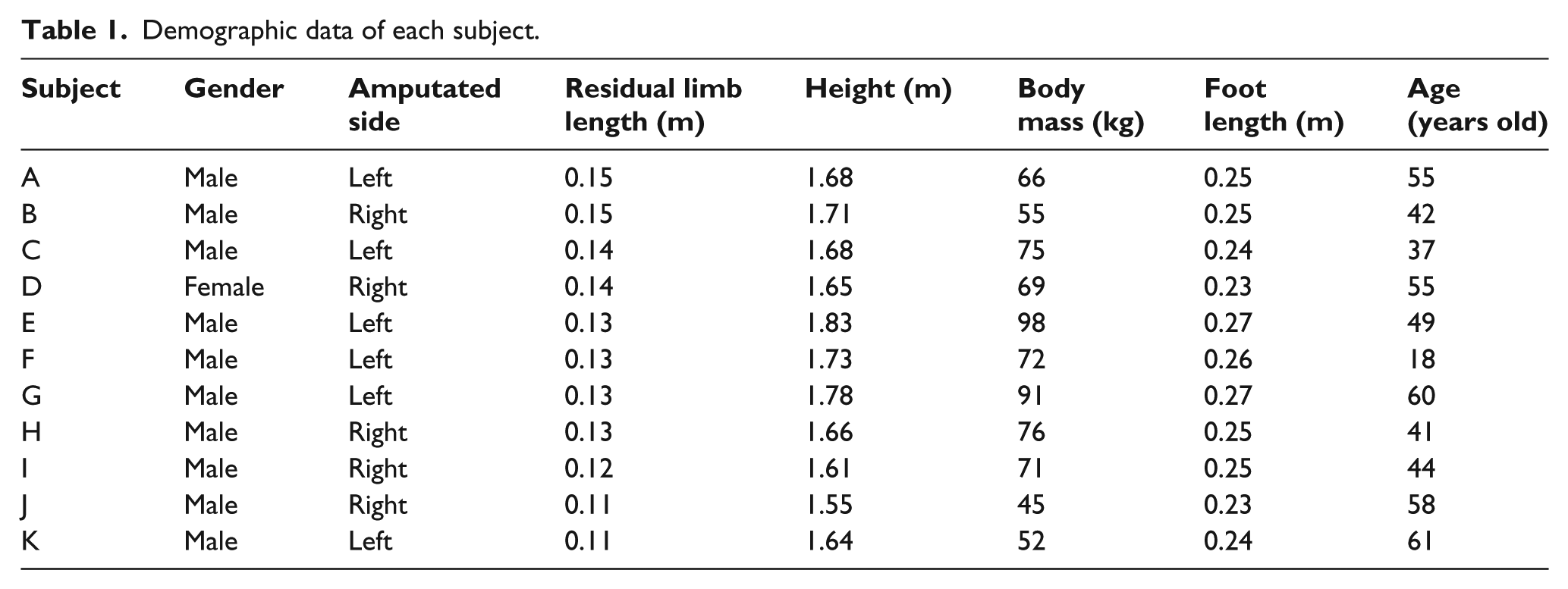
In total, 11 individuals with unilateral transtibial amputation (47(13) years old; 1 female/10 males; mean height: 1.68(0.08) m; mean mass: 70(16) kg) who were users of modular endoskeletal prosthesis with solid-ankle-cushion-heel (SACH) foot in their daily life participated in this study (Table 1). They were community ambulators and used their prosthesis at least for a year, had bilateral normal range of motion, and walked without additional assistive devices. In total, 10 subjects had amputation due to trauma and 1 due to peripheral vascular disease. The study was approved by the Human Subjects Ethics Committee of The Hong Kong Polytechnic University, and informed consent was obtained from each subject.
Demographic data of each subject.
Procedure
A custom instrumented prosthesis alignment component was installed at the base of each amputee’s socket to measure the socket reaction moments.2,5 It was constructed with (1) tilt sensors, (2) force transducer unit with load cells, (3) sagittal and coronal angle and translation and transverse rotation adjuster, and (4) modular prosthesis pyramid connectors (Figure 1). For each subject, a single prosthetist adjusted the alignment of the prosthesis until there was agreement between the subject and the prosthetist. This alignment was defined as the clinically perceived optimal alignment for each amputee according to the current clinical standard practice. Each subject was instructed to walk at a self-selected walking speed. The data were collected wirelessly at the sampling frequency of 100 Hz.
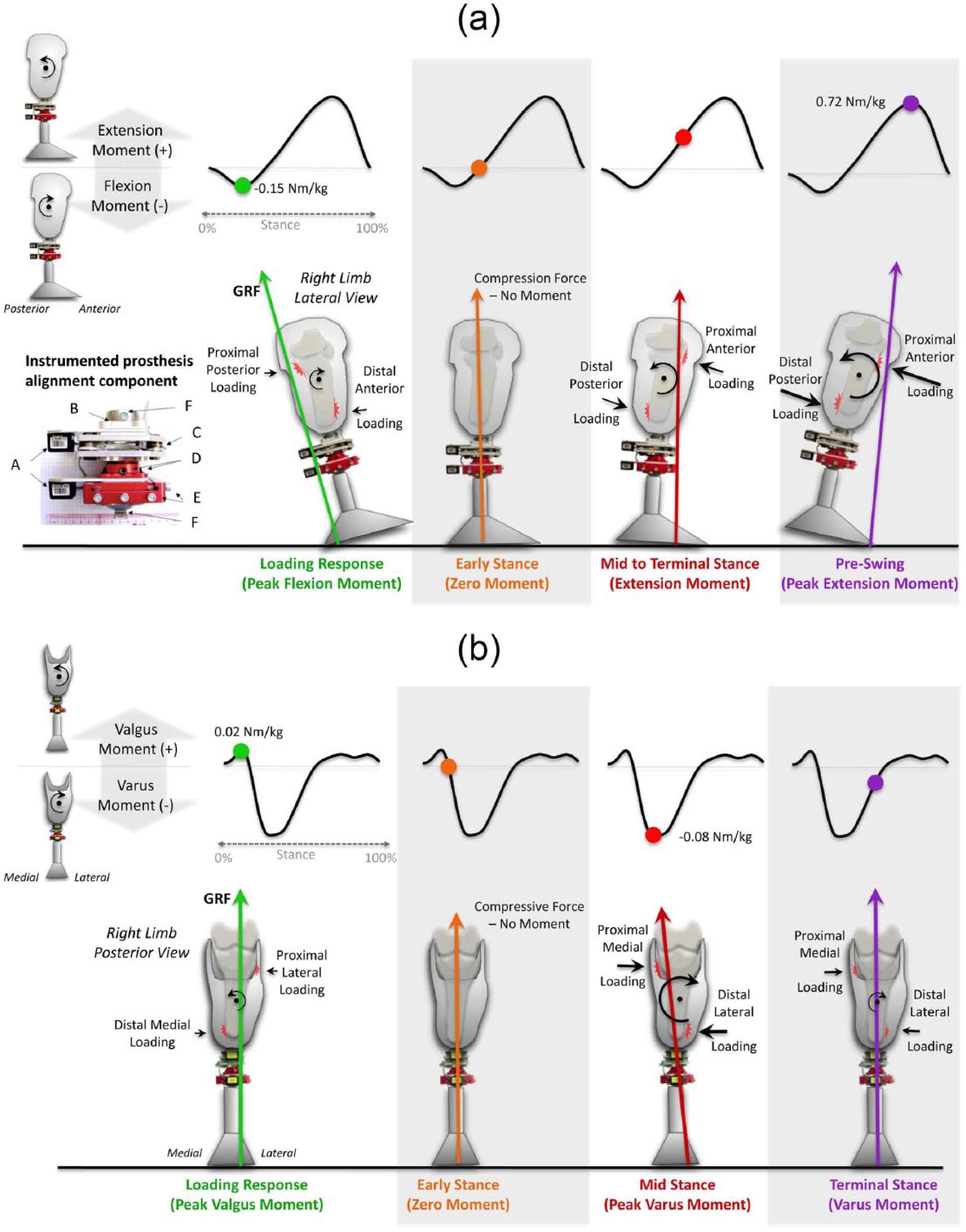
The theoretical relationship between the socket reaction moments and ground reaction forces during stance: 2 (a) sagittal socket reaction moments and ground reaction forces and (b) coronal socket reaction moments and ground reaction forces. The instrumented prosthesis alignment component is constructed with the following components: A: tilt sensors; B: transverse rotation adjuster; C: force transducer; D: sagittal and coronal angle adjuster; E: sagittal and coronal translation adjuster; F: modular prosthesis connectors.
Data analysis
The socket reaction moments were temporally normalized to stance with 1% increments using an interpolation with a cubic spline function, and the moments data from three consecutive steps were averaged and normalized to each subject’s body mass (N m/kg). Figure 1 presents the theoretical relationship between the socket reaction moments and ground reaction forces throughout stance. 2 Eight variables of the socket reaction moments were subsequently extracted (Table 2; Figure 2). From the sagittal socket reaction moment data, three variables related to the magnitude were extracted: peak flexion moment, moment at 45% of stance phase, and peak extension moment, while three variables related to the timing (% stance of event) were also extracted: peak flexion moment point, zero-cross point at which a flexion moment changes to an extension moment, and peak extension moment point. From the coronal data, two variables were extracted: moment at 30% of stance phase and moment at 75% of stance. Finally, cadence was also calculated based on the duration of the socket reaction moments across the gait cycle and presented in steps/minute. Rationales for selecting these parameters are detailed elsewhere. 2
Individual data of the eight socket reaction moment parameters and cadence.
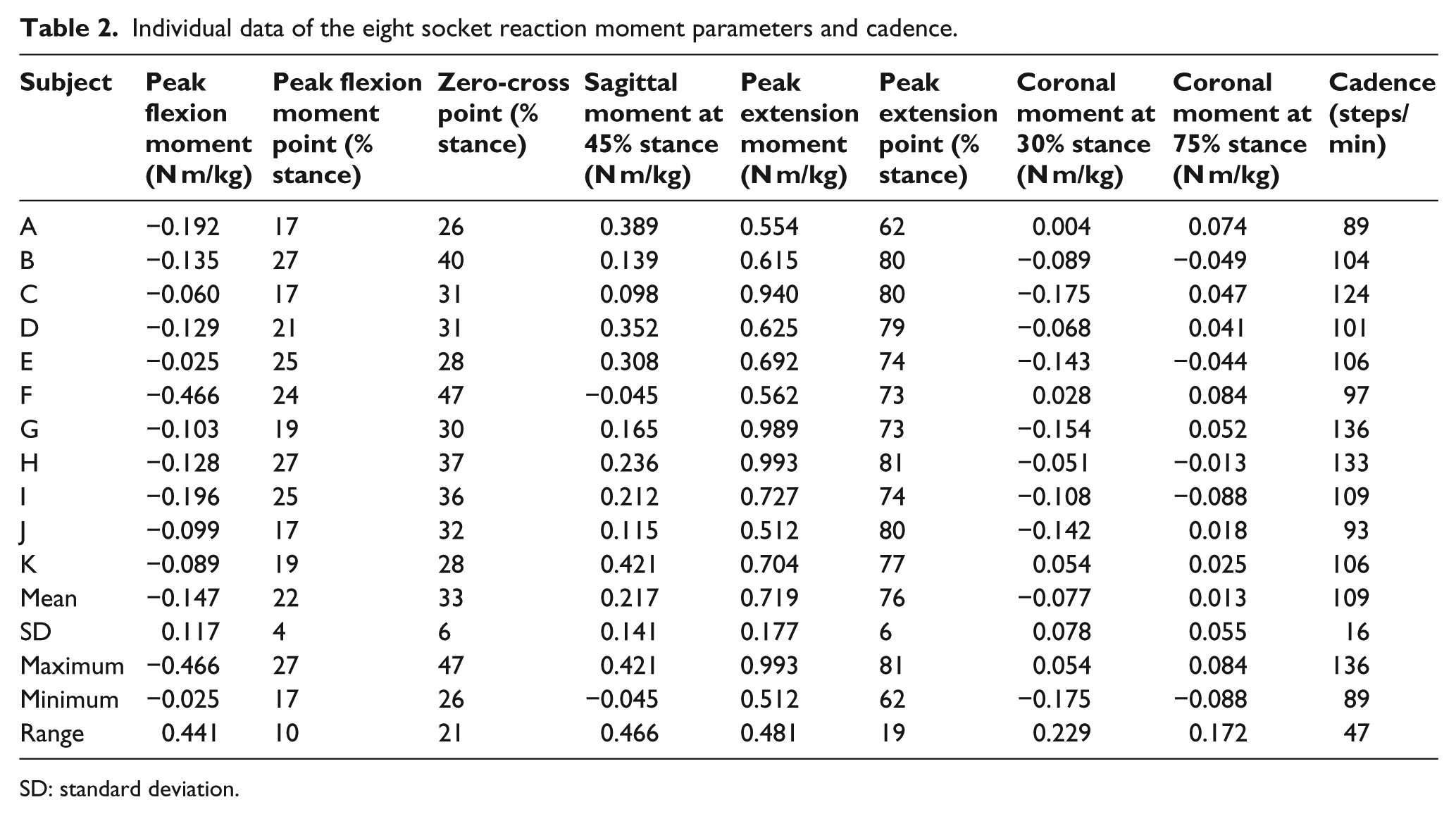
SD: standard deviation.
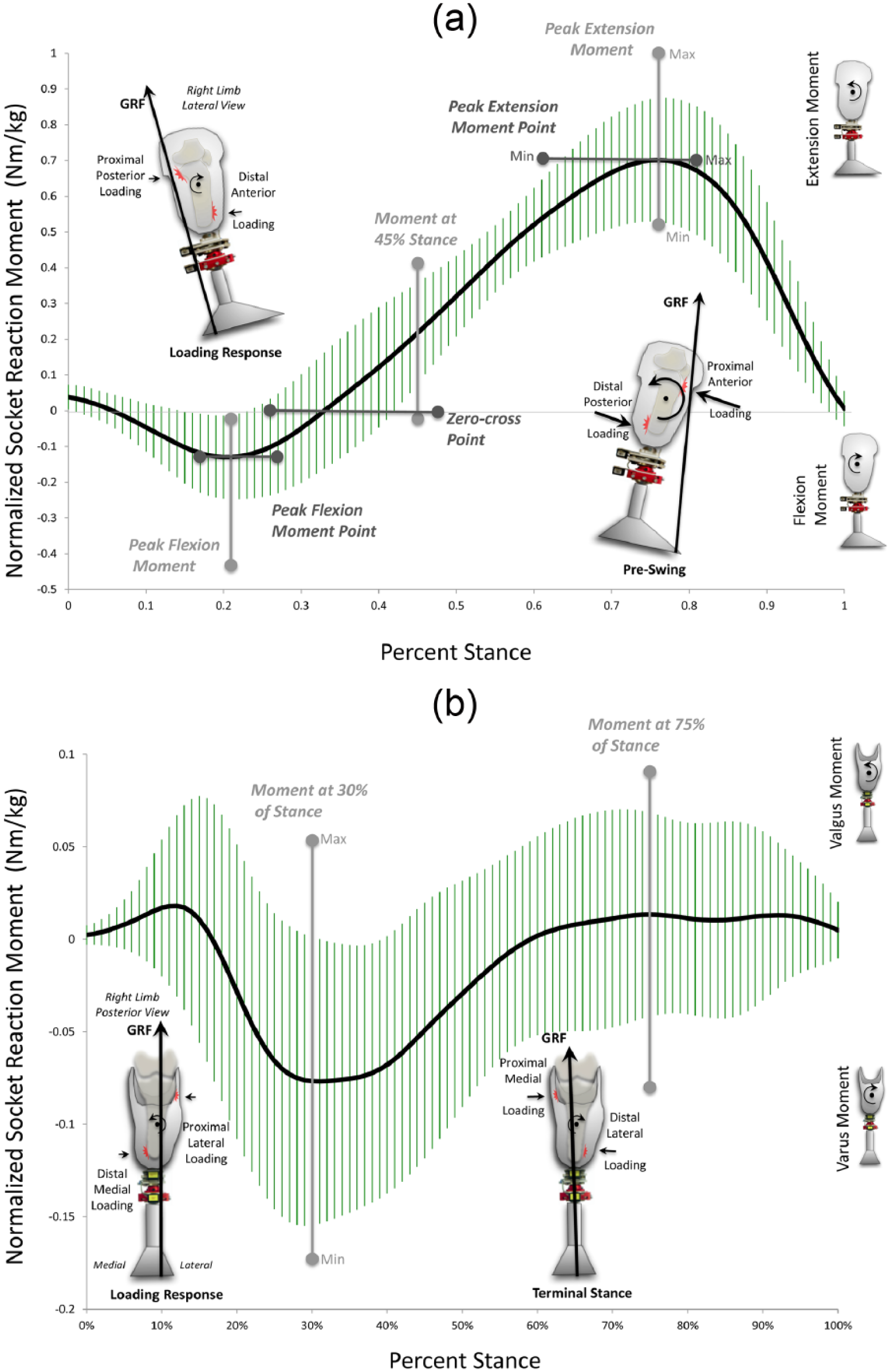
Mean normalized socket reaction moments with standard deviations as a function of % stance in transtibial prostheses with SACH feet: (a) sagittal socket reaction moment and (b) coronal socket reaction moment. The maximum and minimum values for each socket reaction moment parameter are also presented. The mean peak flexion and extension moments in this figure may not exactly match the calculated mean peak moments in Table 2. The moment curve of this figure contains temporal variability in the peak timing whereas the mean in Table 2 was calculated from each amputee’s peak value regardless of timing.
Measurement outcome
The mean socket reaction moments with standard deviations in the sagittal and coronal planes were plotted as a function of % stance (Figure 2). This plot represents the range of the socket reaction moments derived from the 11 amputees at clinically perceived optimal alignment. Individual data (mean, standard deviation, maximum, minimum, and range) of the eight socket reaction moment variables and cadence were presented in Table 2. The maximum and minimum values for each socket reaction moment parameter were also presented in Figure 2.
Discussion
This study investigated the individual differences of the socket reaction moments at the clinically perceived optimal alignment in 11 amputees using transtibial prostheses with SACH feet. The alignment determined based on the agreement between the prosthetist and amputee might not have been the “true” optimal alignment, but this has been the accepted clinical practice standard. Thus, there is a possibility that the socket reaction moment data of some individuals may not necessary represent those under the “true” optimal alignment. Additional measures such as socket interface pressures, symmetry with the intact limb, or pelvic list could be used to validate this alignment choice. However, individual data presented in Table 2 would serve as a valuable reference of potential individual differences in current clinical practice.
Biomechanically, the optimal alignment may allow amputees the most energy efficient and smooth gait with maximum comfort. The ultimate goal of our research is to find how the socket reaction moments can contribute to achieve this through improved fitting of prosthesis. Therefore, it is important to define what constitutes the “true” optimal alignment and to investigate its relationship with the socket reaction moments in future work.
Ultimately, it is necessary to construct a database of the socket reaction moments collected by direct prosthetic measurement technique from a large number of amputees, so that prosthetists could target for their normal range when aligning prosthesis in addition to their subjective judgments based on observational gait analysis and perception of amputees. This study would serve as foundation for this endeavor. A custom direct measurement device paired with this database could potentially aid prosthetists at different levels of skills and experiences to provide consistent alignment service and prosthetic component choice. However, it is important to note that some individuals did not necessarily fit within the mean ± standard deviations range in some parameters (Figure 2).
The pattern of the sagittal socket reaction moments was similar to the prosthetic ankle moment calculated from inverse dynamics.6,7 Mean peak plantarflexion moment ranged approximately from −0.2 to −0.4 N m/kg, while mean peak dorsiflexion moment ranged approximately from 0.6 to 1.3 N m/kg in previous studies investigating prostheses using a computerized gait laboratory.7,10 In this study, the peak flexion moment ranged from −0.025 to −0.466 N m/kg (mean: −0.147(0.117)N m/kg) and the peak extension moment ranged from 0.512 to 0.993 N m/kg (mean: 0.719(0.177)N m/kg) across the amputees. However, direct measurement may not be directly comparable to inverse dynamics that requires modeling assumptions and skills of placing markers.
Individual differences may be attributed to prosthetic feet, gait patterns, or demographic characteristics. All subjects used SACH feet in this study. Each subject walked at a self-selected walking speed, and the range of cadence was 89–136 steps/minute, suggesting a possible wide difference in gait speed. The gait speed may influence the socket reaction moments as it affects the ankle moment. 11 It was shown that the peak extension moment had a significant correlation (Person’s r = 0.982; p < 0.01) with cadence in this group of amputees. 9 Collecting data at a self-selected gait speed would be a clinically reasonable approach because it is not realistic to have amputees walk at a specific gait speed when aligning prosthesis in the clinic. However, it is a limitation of this study that gait speed was not measured. The residual limb length, height, and foot length did not appear to be directly related to individual differences in the socket reaction moments (Table 1).
Each amputee’s gait pattern is unique. For instance, Subject 2’s gait pattern was uniquely characterized with a strong and prolonged first rocker of stance, which was reflected in the peak flexion moment and zero-cross point (Table 2). Moreover, the standard deviations of the coronal moments were large throughout stance phase (Figure 2(b)). How individual gait patterns may affect the socket reaction moments needs to be further investigated using a 3D computerized gait laboratory. The relationship between the socket reaction moments and socket interface pressures should also be verified (Figure 1(a) and (b)). This study focused on the measurement of the moments; however, forces may be important contributors for pressure distributions on the residual limb. 12 A future study should also investigate the effects of mechanical properties of prosthetic components, such as feet and shock absorbers as well as shoes on the socket reaction moments. Finally, the socket reaction moments should be measured not only in the gait laboratory but also in other environments under various activities.
Key points
Socket reaction moments can be conveniently measured in the clinic.
The range of individual differences at clinically perceived optimal alignment was presented.
Socket reaction moments could potentially aid prosthetists align prosthesis.
Additional data from a large number of amputees are needed to construct database of the socket reaction moments.
Footnotes
Author contribution
All authors contributed equally in the preparation of this article.
Declaration of conflicting interests
The authors declare no conflict of interest.
Funding
This project was supported by an internal research grant of The Hong Kong Polytechnic University.