
Abstract
Background:
Charcot–Marie–Tooth disease is an inherited neuropathy causing progressive weakness, foot deformity and difficulty walking. Clinical anecdotes suggest orthoses designed on the ‘sensorimotor’ paradigm are beneficial for improving gait in Charcot–Marie–Tooth disease.
Objectives:
Investigate the effect of sensorimotor orthoses on in-shoe and lower limb biomechanics in adults with Charcot–Marie–Tooth disease.
Study design:
Randomised, repeated-measures, exploratory study.
Methods:
Eight males and two females with Charcot–Marie–Tooth disease aged 31–68 years fitted with pedorthic shoes and custom-made sensorimotor orthoses were randomly tested at baseline and after 4 weeks of adaptation. In-shoe three-dimensional multi-segment foot and lower limb kinematics and kinetics were collected as were plantar pressures, electromyography and self-reported comfort, stability, cushioning and preference.
Results:
Compared to the shoe only condition, sensorimotor orthoses increased midfoot eversion and plantarflexion, increased ankle eversion and produced small but significant changes at the knee and hip indicating increased internal rotation. The orthoses increased medial ground reaction forces and increased pressure at the heel, midfoot and toes. There were minimal effects on electromyography. The sensorimotor orthoses were rated higher for comfort, cushioning, stability and preference.
Conclusion:
Sensorimotor orthoses produced changes in kinematic, kinetic and pressure variables in adults with Charcot–Marie–Tooth disease and were regarded as more comfortable, cushioned and stable during walking.
Clinical relevance
In this study, the walking ability of patients with Charcot–Marie–Tooth disease improved with the use of foot orthoses designed according to the sensorimotor paradigm. However, the mechanism of action appears to be primarily mechanical in origin. Randomised controlled trials are necessary to evaluate the long-term patient-reported outcomes of sensorimotor orthoses.
Background
Charcot–Marie–Tooth (CMT) disease is the most common hereditary peripheral nerve disorder, with an incidence of 1 in 2500. 1 CMT is characterised by motor and sensory neuropathy progressing proximally from the extremities resulting in weakness, sensory loss, foot deformity, lateral ankle instability, problems with balance and difficulty walking. 2 The cardinal manifestation of the most common type of the disease (CMT1A) is a cavovarus foot deformity which is believed to occur due to intrinsic foot weakness and progressive selective weakening of the extrinsic foot and ankle musculature.3,4
Currently, there are few effective treatments for patients with CMT and management is focused on maintaining function through rehabilitative therapy, foot orthoses and orthopaedic surgery. 5 Ankle foot orthoses (AFOs) are routinely prescribed for patients with CMT to improve balance and gait stability and to reduce foot drop during the swing phase of gait. 5 However, patient acceptance of AFOs in CMT is poor due to discomfort and their conspicuous design drawing attention to the patient’s disability. 6 Due to this poor patient approval of AFOs, research into comfortable and less noticeable management options to improve walking ability of patients with CMT is required, such as in-shoe foot orthoses. In-shoe foot orthoses have been shown to reduce foot pain and redistribute plantar pressures in people with a cavovarus deformity due to CMT as well as other aetiologies. 7
Foot orthoses are conventionally designed around the mechanical principle of supporting the medial longitudinal arch to alter plantar pressure and skeletal alignment. However, there is evidence that sensorimotor alterations may also be an important factor. 8 The ‘sensorimotor orthotic’ paradigm has been proposed whereby foot orthoses are designed on the principle of altering sensory input to the plantar surface of the foot thereby changing muscle activation patterns. 9 One sensorimotor adaptation theory describes how ‘elements’ on the foot orthoses (e.g. forefoot valgus posting or lateral rearfoot padding) increase local pressures which are detected by cutaneous receptors, muscle spindles or Golgi apparatus modulating afferent information transferred to the interneuron pool. Resulting spinal and supraspinal adaptations change the underlying motor programme and efferent drive to the muscle. 9
However, the ‘sensorimotor orthotic’ paradigm, originally described by German orthopaedic shoemaker Meister Lothar Jahrling, is yet to receive widespread acceptance outside Germany, central Europe and to some extent Japan. This is because there have been no randomised trials, few peer-reviewed reports in English and only small cross-sectional studies showing modest effects in children with in-toeing gait, 10 ankle equinus in cerebral palsy and habitual toe walkers. 11 Well-designed biomechanical studies are required to understand the physiological response of the body to sensorimotor orthoses before randomised controlled trials can be undertaken to determine efficacy. Clinical anecdotes suggest that foot orthoses designed on the sensorimotor paradigm improve the walking ability of patients with CMT. However, no research has been undertaken to evaluate sensorimotor orthoses in patients with CMT. Therefore, the aim of this study was to investigate the effect of sensorimotor orthoses on in-shoe and lower limb kinematics, kinetics, electromyography (EMG), plantar pressure and self-reported outcomes in 10 adults with CMT.
Methods
Participants
Participants were recruited in New South Wales, Australia, by advertisements through the CMT Association of Australia. Eligible participants were males and females aged between 18 and 70 years diagnosed with CMT by genetic testing, nerve conduction studies or familial inheritance with confirmed clinical testing. Participants were excluded if they were currently using AFOs or walking aids (e.g. walking sticks and frames); had previous bone or articular surgery to the foot or ankle; medical conditions other than CMT that affect peripheral sensation or balance, for example, diabetes mellitus, history of foot ulceration; currently using anticoagulant medication, for example, warfarin; or pregnant at the time of the study. Participant’s foot alignment was assessed weight-bearing using the validated Foot Posture Index that classifies feet along a continuum of cavus (−12 to −1), normal (0 to +5) and planus (+6 to +12) features. 12 The study was approved by the university Human Research Ethics Committee (Project Number: 2013/252).
Interventions
Participants were fitted with a correctly sized pair of unisex prefabricated pedorthic shoes with a standard ethylene-vinyl acetate (EVA) insole (Gadean Walker Stretch, Malaga, WA, Australia). Each participant was provided with a custom-made pair of sensorimotor orthoses prescribed and manufactured by an experienced Pedorthist (KW). The shoes and orthoses worn by participants in the study are shown in Figure 1. Each foot of each participant was assessed for range of motion, degree of possible alignment improvement and skin sensitivities to direct the height and placement of the ‘elements’. The design of the elements was consistent across the cohort although the prominence and placement of the elements varied between individuals based on foot morphology. The elements included a forefoot valgus post, large cuboid notch designed to apply pressure on the peroneal tendons and a medial prominence to place pressure on the tibialis posterior tendon insertion at the navicular. Larger elements were applied if there was a lower risk of skin irritation (no participants exhibited skin irritations either before or during the study). Then, a weight-bearing Harris mat imprint and foam impression was taken for each foot. The foam impression was scanned using a three-dimensional (3D) projection scanner (ParoScan 3D; Paromed Vertriebs GmbH & Co. KG, Neubeuern, Germany) and the orthoses were designed with a computer-aided design (CAD) package based on each participant’s assessment. The orthoses were milled from an EVA block with a hardness of 45 shore A, and a flexible 1 mm flat polypropylene base was applied.
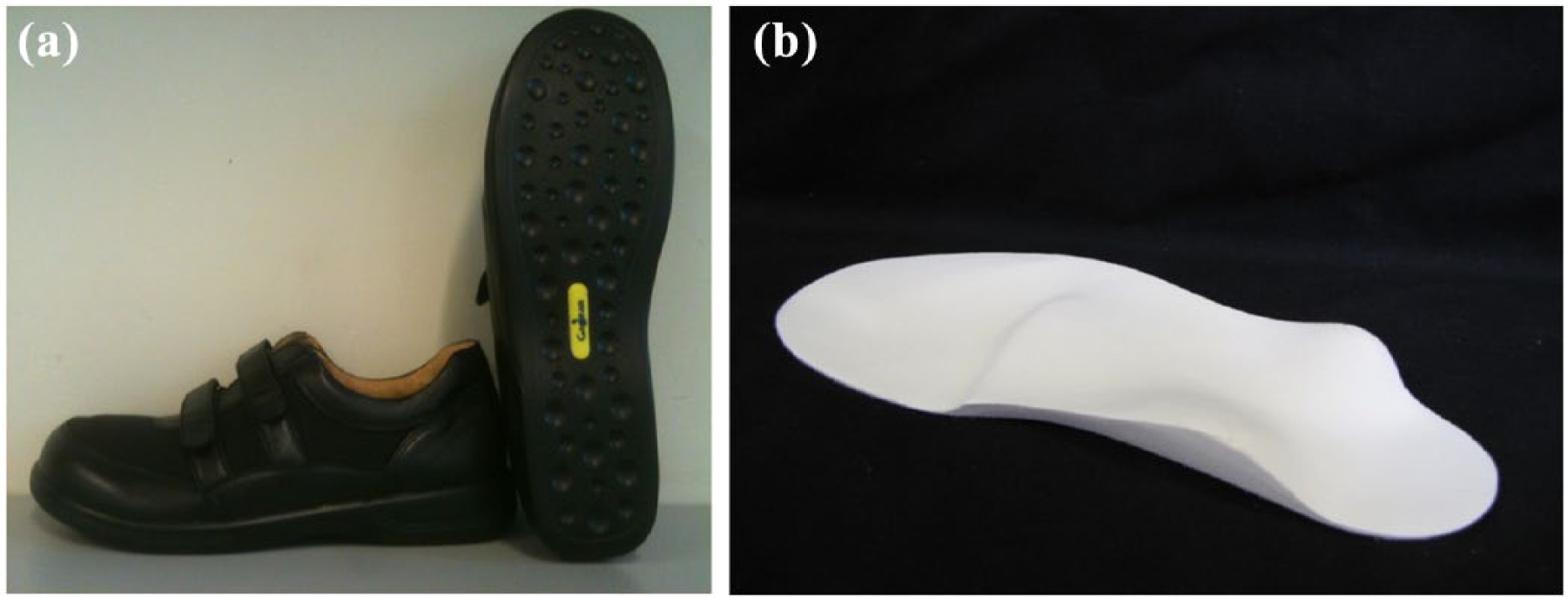
The shoes and orthoses worn by participants in the study: (a) Pedorthic shoes (Gadean Walker, Malaga, WA, Australia) and (b) custom-made sensorimotor orthoses.
Participants were provided with the shoes and orthoses to wear-in during a 4-week adaptation period. Participants were instructed to increase the time they wore the orthoses in their provided shoes by 1 h each day until they could wear the orthoses all day, according to a previous standardised protocol. 7 Data were collected at the time of fitting (baseline) and after the 4-week adaptation period (follow-up). Testing order for the shoe and shoe/orthoses conditions was randomised at each visit using four unique computer-generated codes for each participant.
Experimental protocol
To ensure a natural gait pattern and to prevent targeting of the force plate, participants walked at a self-selected velocity along a 12-m walkway. Five successful trials, in which the participant landed completely on the force plate, were recorded in each condition. Following the collection of spatiotemporal, kinematic, kinetic and EMG data, in-shoe plantar pressures were collected while participants completed two laps of the 12-m walkway at a comfortable self-selected velocity. Participants were given a 5-min acclimatisation period in each condition before collection of the kinematic, kinetic, EMG and plantar pressure variables.
Spatiotemporal, kinematics, kinetics and EMG
A 14-camera motion analysis system (Cortex 2.1; Motion Analysis Corporation, Santa Rosa, CA, USA) with a sampling rate of 200 Hz was used to calculate 3D trajectories of 13 mm diameter retro-reflective markers. Motion was calculated using the biomechanical software package KinTrak 7.0 (University of Calgary, Calgary, AB, Canada). Prior to the calculation of motion, the coordinate trajectories of the markers were filtered at 5 Hz (walking) 13 with a low-pass zero phase shift fourth-order Butterworth filter. Processed data were time-normalised by linear interpolation to the stance phase and ensemble-averaged across trials and participants. Discrete variables were analysed for stance and the loading period which was defined as the first 50% of stance.
Motion at the first metatarsophalangeal joint (MTPJ), midfoot and ankle joints was calculated using our previously described model, 14 in which the ankle and midfoot joints have 3 degrees of freedom, while the first MTPJ has 1 angular degree of freedom. The multi-segment foot model is based on one used previously in adults with healthy and pathological feet13,15,16 and has been shown to have moderate to high inter-session reliability.13,15 The midfoot joint axis was defined based on fluoroscopy research validating skin markers overlying the navicular and first metatarsal head to model sagittal plane forefoot motion. 17 Knee and hip motion was calculated according to International Society of Biomechanics (ISB) recommendations. 18 The joint axes of rotation and the relative segments are described in Figure 2.
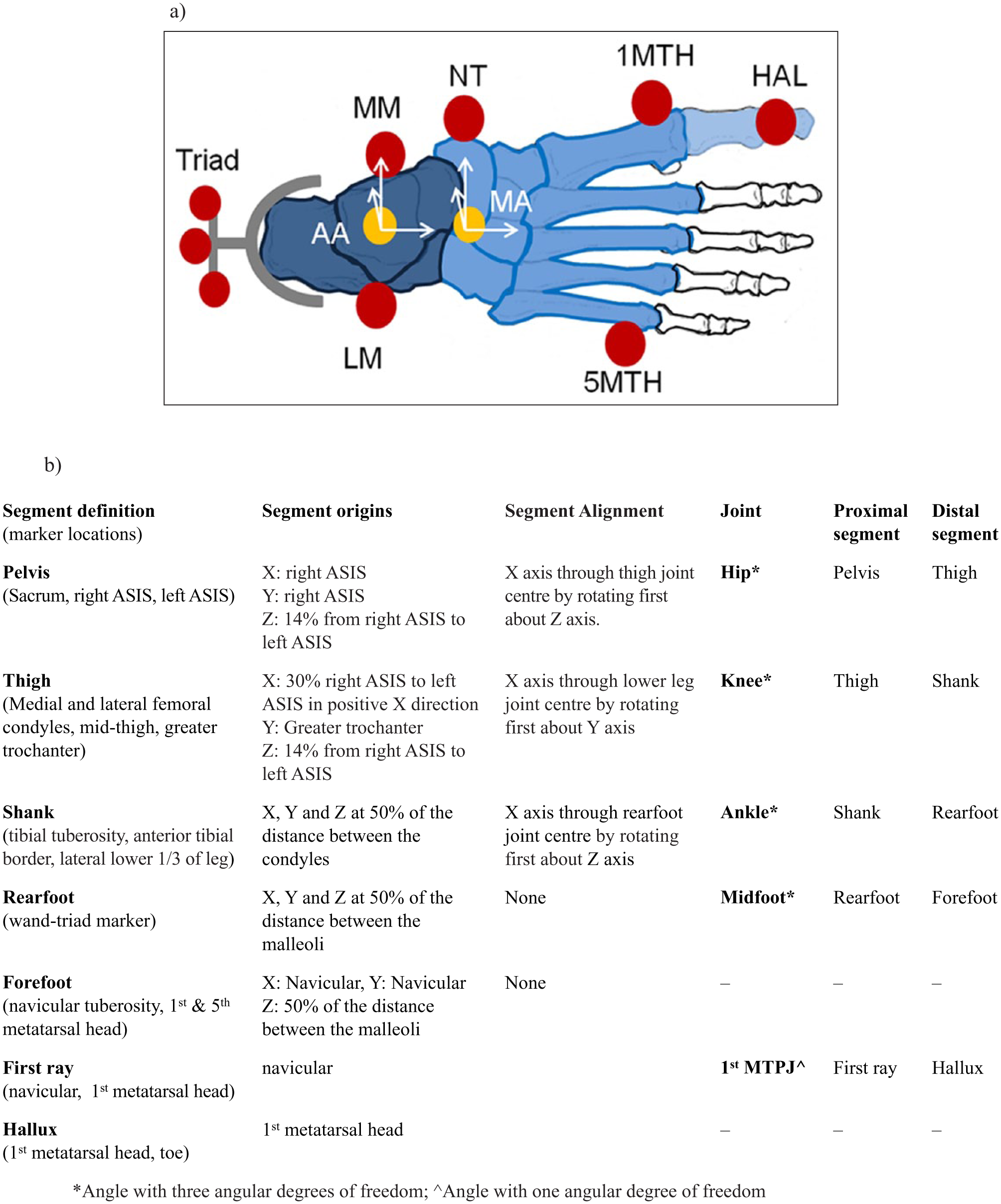
(a) Depiction of the marker locations and joint axes origins used to quantify midfoot and ankle joint complex motion. The rearfoot segment is depicted in dark grey/blue, while the forefoot segment is shown in light grey/blue. The marker locations are shown in red and are the rearfoot wand triad (Triad), medial malleolus (MM), lateral malleolus (LM), navicular tuberosity (NT), first metatarsal head (1 MTH), fifth metatarsal head (5 MTH) and hallux (HAL). The ankle joint complex (AA) and midfoot axes (MA) origins are shown in yellow. (b) Definitions of the segments, marker locations and joints axes origins used to quantify hip knee, ankle joint complex, midfoot and first MTPJ motion.
Segment motion was calculated with respect to a barefoot standing reference position in which participants stood in relaxed stance with both feet aligned with the laboratory X axis. During both barefoot and shod conditions, motion of the rearfoot segment was defined by a detachable wand triad marker. Wand-based markers are commonly used to measure 3D rearfoot kinematics. 19 In the shod condition, the wand triad, hallux, navicular, and first and fifth metatarsal head markers extended through holes in the upper of the shoe with dimensions of 17 mm by 25 mm. 19 Holes of this dimension have been shown to not adversely alter the integrity of upper of the shoe. 19 The hallux, navicular, and first and fifth metatarsal head markers were attached by strong self-centring magnets to magnetic bases attached to the skin. The use of the detachable rearfoot wand triad and magnetic markers ensured marker placement was not altered between barefoot and shod conditions, as the bases for the markers remained in place during the data collection process.
Ground reaction force (GRF) data were recorded at 1000 Hz from a single force plate (Kistler™ Model 9281B; Kistler, Winterthur, Switzerland). The vertical GRF data were used to define stance phase. Kinetic data were normalised to participant’s body weight and are expressed as percent body weight (%BW). Spatiotemporal parameters were calculated from the kinematic and kinetic data.
Surface EMG of the vastus lateralis, medial gastrocnemius, tibialis anterior, peroneus longus and soleus was collected at 1000 Hz (Telemyo 2400R; Noraxon, Inc., Phoenix, AZ, USA). Electrode preparation and application were applied according to the recommendations of Surface ElectroMyoGraphy for the Non-Invasive Assessment of Muscles (SENIAM). 20 Data were band-pass filtered at 20–500 Hz, and rectified and filtered again with a zero-phase low-pass filter with a cut off frequency of 10 Hz to produce the linear envelope EMG. 21
In-shoe plantar pressure
In-shoe plantar pressures were collected with a Pedar-mobile in-shoe system (Novel GmbH, Munich, Germany) at 50 Hz. The Pedar-mobile in-shoe system is an accurate, reliable and valid measure of in-shoe plantar pressures.22,23 Nine straight line walking steps from the right foot were randomly selected in the Novel software (Novel GmbH). The foot was then divided into five anatomically and clinically relevant regions of the foot including rearfoot, midfoot, forefoot, hallux and toes using a Novel automask (Novel GmbH). For each region of the foot, peak pressure, contact area, contact time and begin of contact (% of contact) were analysed.
Self-reported outcome measures
Self-reported comfort, cushioning and stability were collected using a valid and reliable questionnaire at the baseline and follow-up visits. 24 The questionnaire contains a series of 100 mm visual analogue scales with labelled anchors, for example, ‘not comfortable at all’ to ‘most comfortable imaginable’. 24 At the conclusion of data collection at each visit participants were asked to nominate which shoe or shoe/orthoses condition they felt most stable and which condition they preferred overall.
Statistical analysis
Descriptive statistics and normality of data distribution were computed in SPSS v22.0 (IBM SPSS Statistics for Windows, Armonk, NY, USA). Consequently paired sample t-tests were undertaken to assess significance between shoe and shoe/orthoses conditions at the baseline and follow-up visits. The alpha value was set at 0.05. A Bonferroni correction was not undertaken to reduce the chance of a type II error. 25 The authors acknowledge that this increases the risk of a type I error.
Results
Participants
Of the 22 participants who volunteered for the study, 10 fulfilled the inclusion criteria. The study sample consisted of eight men and two women aged 31–68 years. The physical characteristics of the study cohort are shown in Table 1. CMT genetic subtypes were as follows: 40% type 1A, 20% type X1-5 and 40% unidentified gene. Eight participants exhibited a cavus foot type with a Foot Posture Index between −1 and −12, and two participants had a planus foot type with a Foot Posture Index of +8. After the adaptation period, eight participants returned for follow-up data collection. One participant could not be contacted, while the other could not return due to work commitments.
Physical characteristics of the study participants.
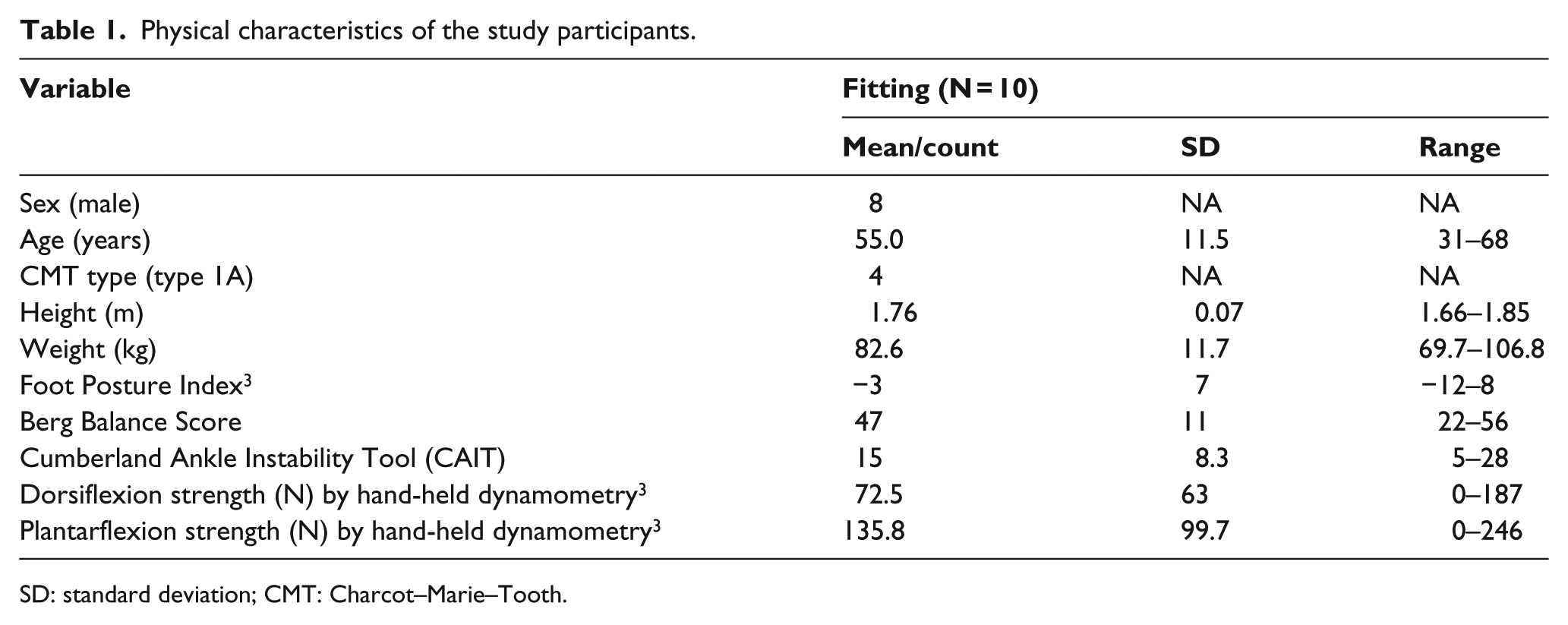
SD: standard deviation; CMT: Charcot–Marie–Tooth.
Spatiotemporal, kinematics, kinetics and EMG
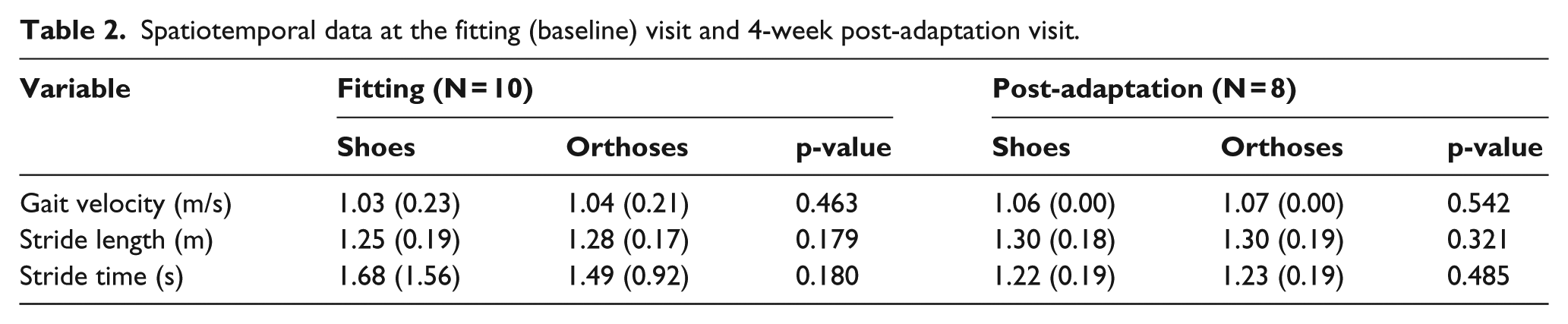
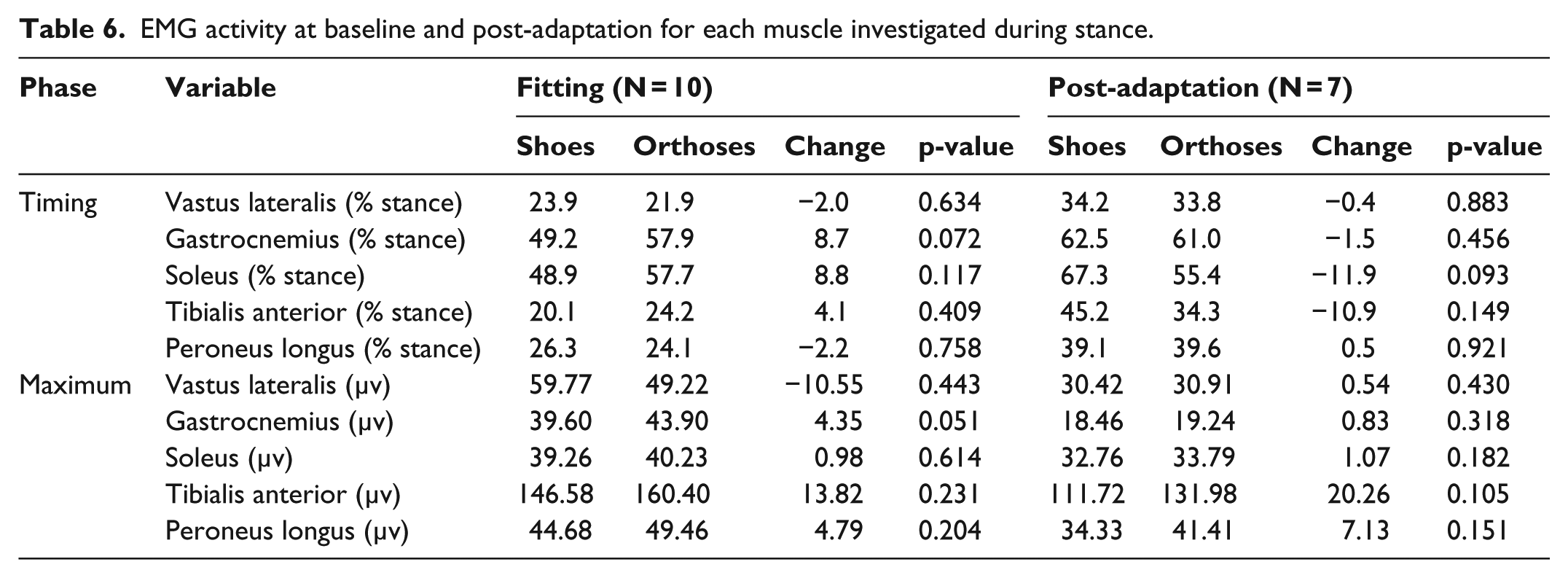
There were no significant differences in spatiotemporal walking parameters during kinematic data collection for either condition at either time point (Table 2). There were many significant kinematic changes with orthoses at baseline (Table 3) and at the post-adaptation follow-up (Table 4) visits. The main changes with sensorimotor orthoses included the following: increased midfoot plantarflexion and eversion, and increased ankle eversion during loading. There were small but significant changes at the knee and hip indicating increased internal rotation. With regard to kinetics, there were small increases in the peak and mean medial force while walking in the orthoses (Table 5). There were minimal changes in EMG activity between shoe and shoe/orthoses at either time point (Table 6).
Spatiotemporal data at the fitting (baseline) visit and 4-week post-adaptation visit.
Kinematic data at the fitting (baseline) visit (N = 10).
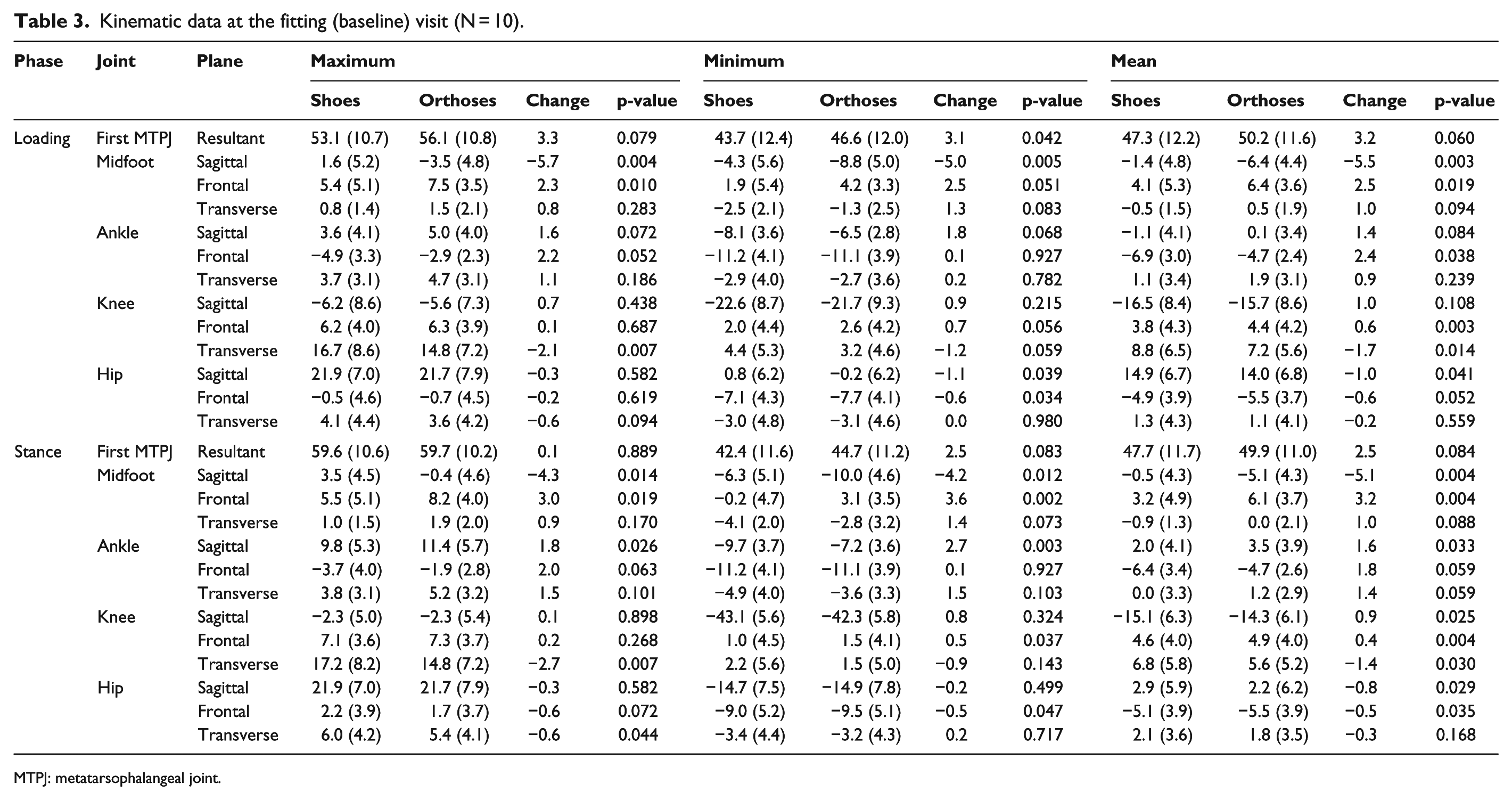
MTPJ: metatarsophalangeal joint.
Kinematic data at the 4-week post-adaptation visit (N = 8).
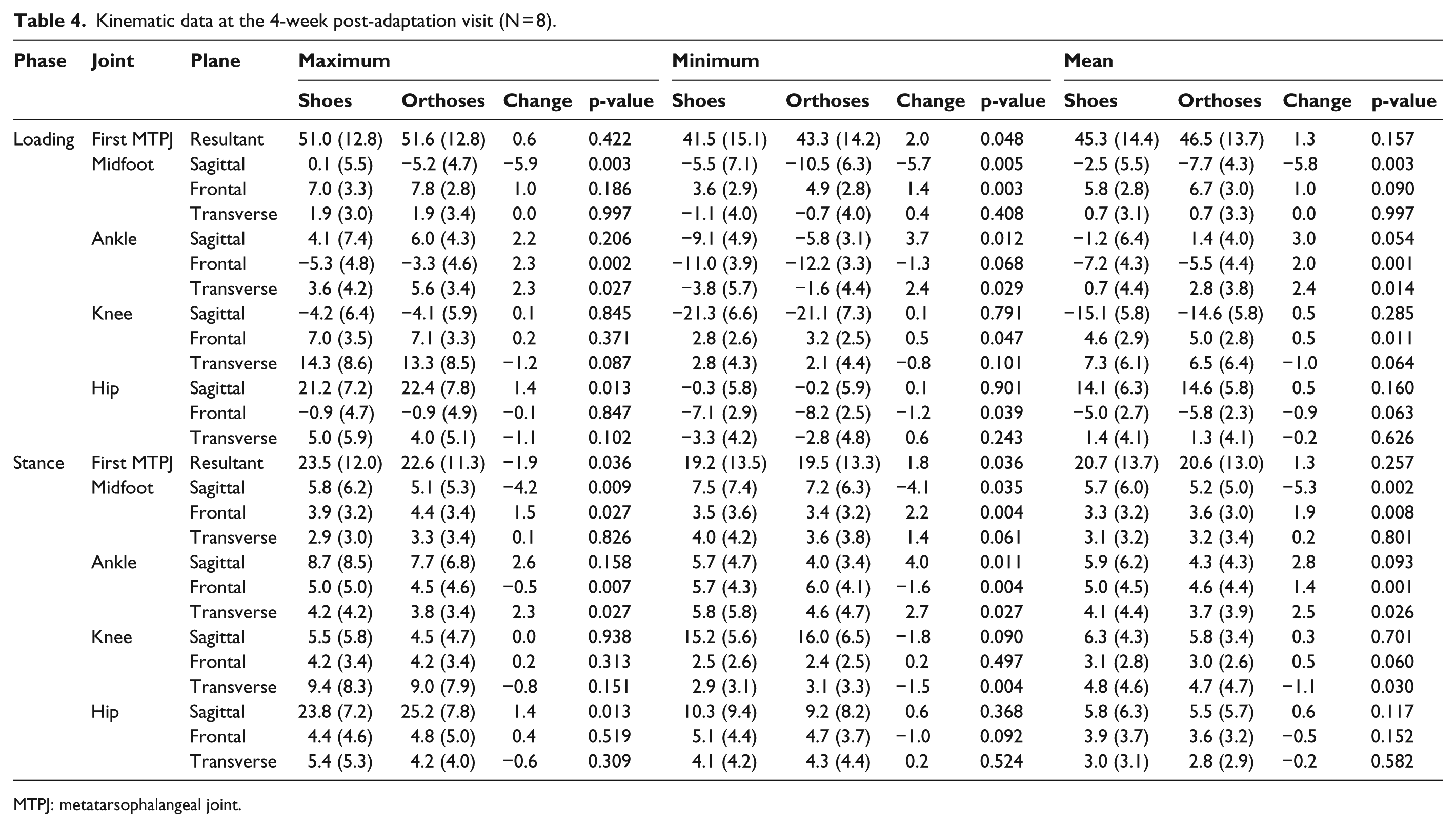
MTPJ: metatarsophalangeal joint.
Kinetic data at the fitting (baseline) visit and 4-week post-adaptation visit.
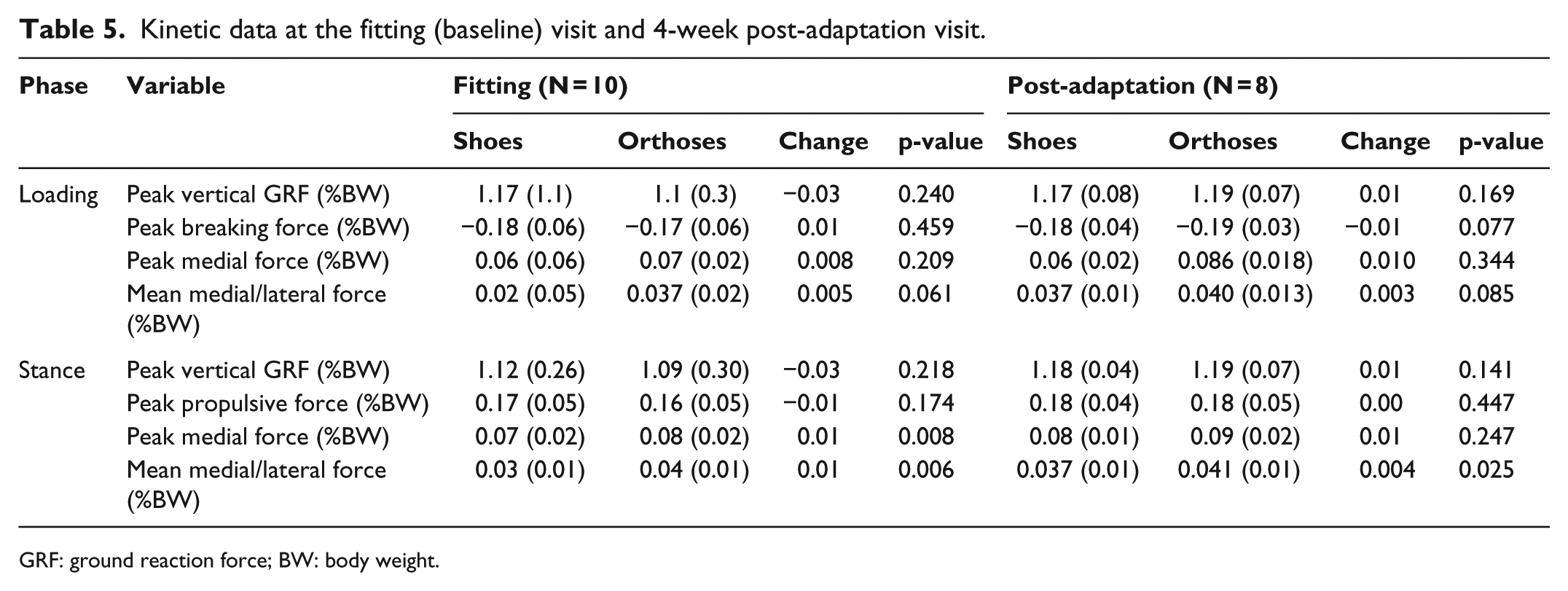
GRF: ground reaction force; BW: body weight.
EMG activity at baseline and post-adaptation for each muscle investigated during stance.
In-shoe plantar pressure
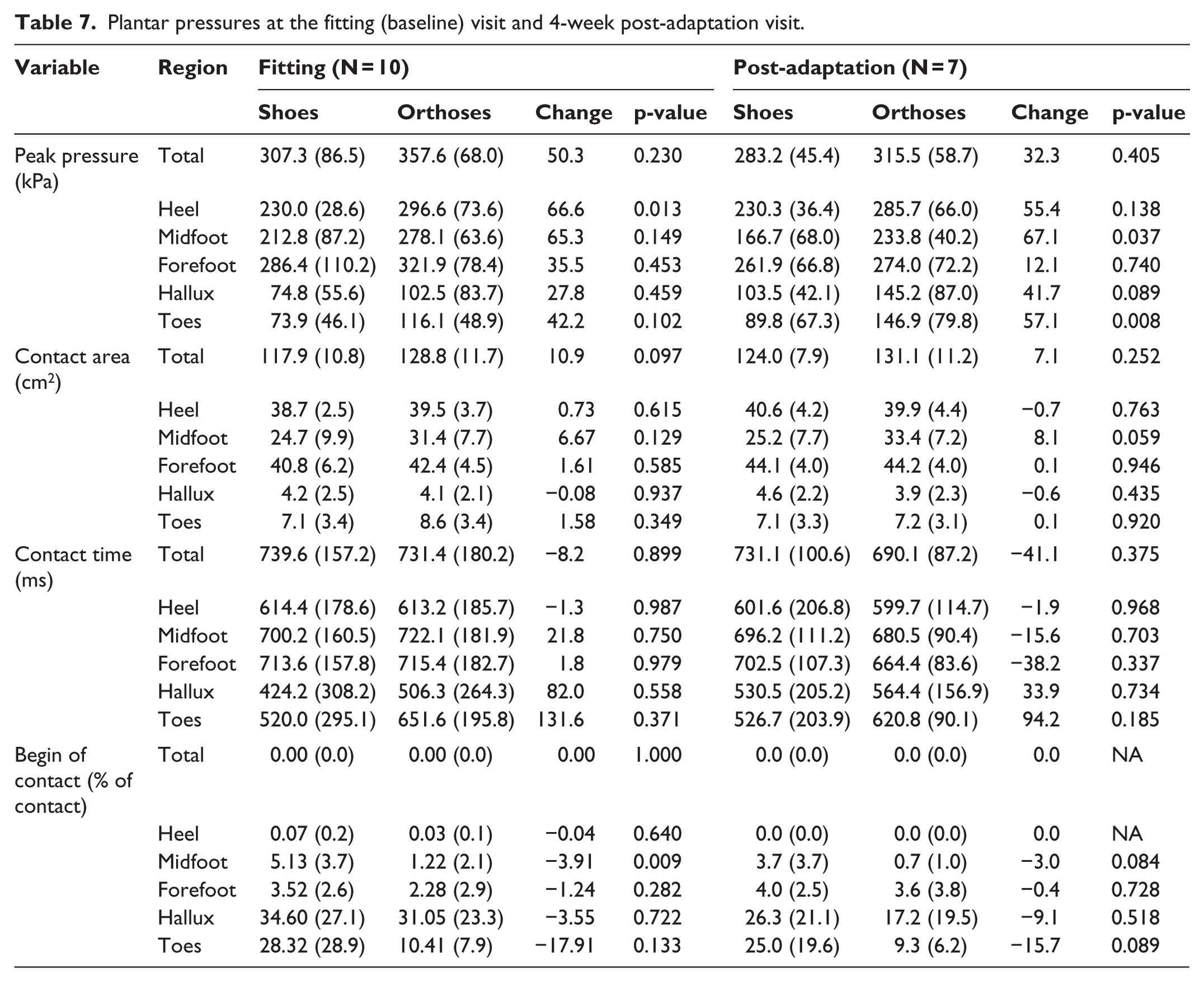
With orthoses, peak pressure significantly increased at the heel at baseline, and midfoot and toes at the post-adaptation follow-up (Table 7). Contact area and contact time did not differ between conditions at either time point, although the beginning of midfoot contact as a percentage of contact time was significantly earlier with orthoses.
Plantar pressures at the fitting (baseline) visit and 4-week post-adaptation visit.
Self-reported outcome measures
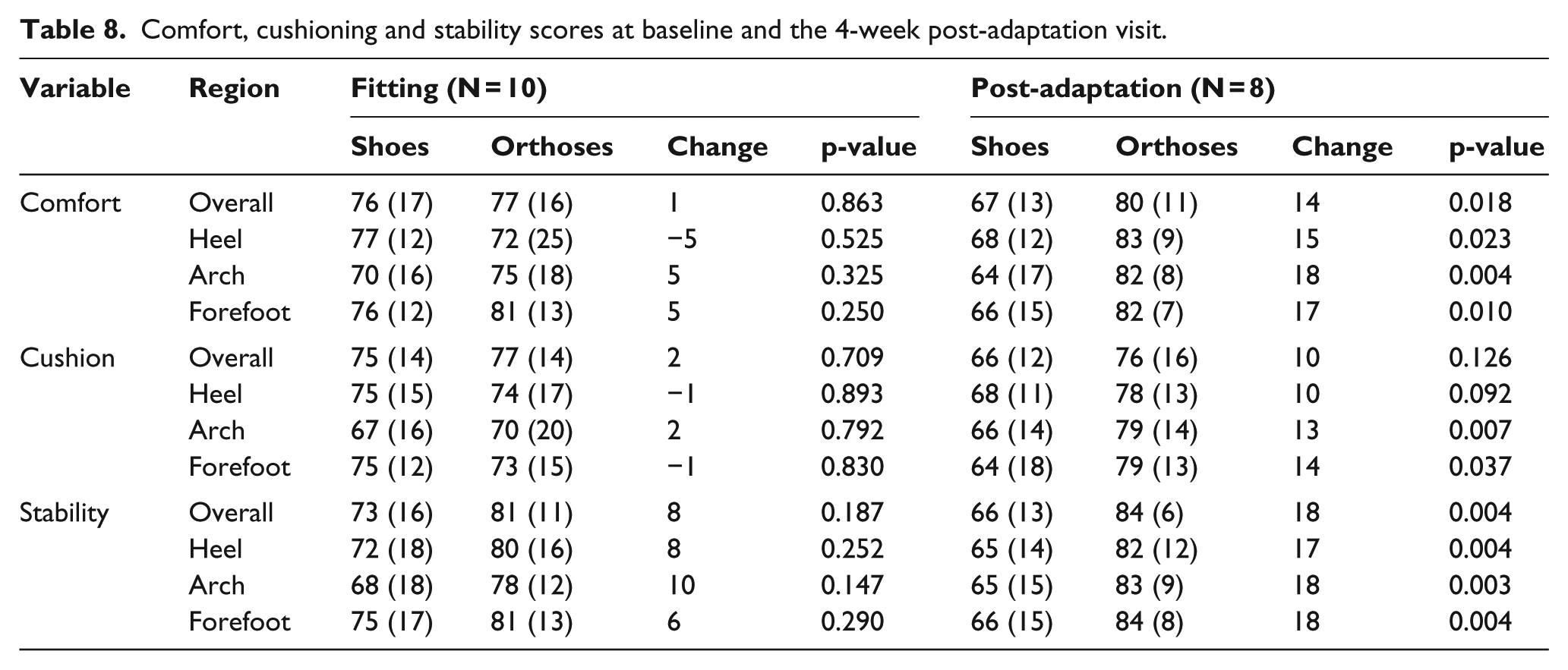
Stability and comfort scores at baseline did not differ between conditions; however, they significantly favoured the orthoses for all regions of the foot at follow-up (Table 8). Cushioning scores were higher with orthoses for the arch and forefoot post-adaptation (Table 8). At baseline, six participants preferred the orthoses overall, while at follow-up, all eight participants preferred the orthoses overall.
Comfort, cushioning and stability scores at baseline and the 4-week post-adaptation visit.
Discussion
The main findings from this study are that sensorimotor orthoses alter midfoot and ankle kinematics during walking in adults with CMT and have limited effects on spatiotemporal, kinetic and muscle activity patterns. Increases in plantar pressure at the ‘element’ sites suggest the primary mechanism of the sensorimotor orthoses for patients with CMT is mechanical in origin. Compared to the shoe only condition, the sensorimotor orthoses increased midfoot eversion and plantarflexion due to the forefoot valgus element and increased ankle eversion due to the lateral cuboid notch rearfoot element.
The sensorimotor adaptation mechanism is thought to increase efferent drive to the muscle. 9 However, we did not find this to be the case as there were minimal effects on EMG. This might have been due to the severe neuropathy of CMT causing substantial and irreversible muscle atrophy or fatty infiltration precluding the measurement of intact motor units. The reduced proprioception and cavovarus foot deformity associated with CMT might have also resulted in the limited neuromuscular response, or the sensorimotor adaption was not detected because we did not measure EMG of all foot muscles. Although it has been conceded that the exact neural pathways, and spinal and supraspinal modulations concerning the ‘sensorimotor paradigm’ is not entirely clear. 9
The clinical implication of sensorimotor orthoses increasing midfoot eversion and plantarflexion, and increasing ankle eversion in patients with CMT is encouraging. These biomechanical effects are desirable for realigning the cavovarus foot deformity, reducing chronic ankle instability and improving balance problems often reported by patients with CMT. The low profile of the sensorimotor orthoses is likely to increase adherence in patients who do not require the use of AFOs. Importantly the self-reported participant outcomes after 4 weeks consistently and significantly favoured the sensorimotor orthoses. As such, further investigation into the association between patient-reported outcomes and the mechanical/neuromuscular mechanisms of sensorimotor orthoses is eagerly anticipated.
This study is not without limitation. Small sample size, lack of a control group (and associated blinding) and relatively short adaptation period are limitations to the study design. The exploratory nature of this study meant that a large number of statistical comparisons were undertaken on a relatively small sample size leading to an increased risk of type I error. As such, some of the small changes may be statistical anomalies; however, the changes at the midfoot and ankle were large and consistent. A well-powered randomised controlled trial is necessary to evaluate the long-term benefits of sensorimotor orthoses.
Conclusion
There are few effective treatments for patients with CMT. This study shows that sensorimotor orthoses produce some significant biomechanical changes and are regarded as more comfortable, cushioned and stable during walking, compared to a shoe only condition.
Footnotes
Acknowledgements
The authors would like to thank Ray Patton for his technical assistance in the data collection process. We thank the CMT Association of Australia for assistance with participant recruitment.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
Karl-Heinz Schott C Ped has a trademark on sensomotoric® orthoses which are designed on the sensorimotor paradigm. The authors report no other disclosures.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.