
Abstract
Background:
Contractures of Achilles tendons and gastrocnemius muscle deteriorate the performance in daily living activities of patients with neuromuscular diseases. Ankle–foot orthoses help to prevent the progression of deformities and to obtain optimal position of the joints to support standing and walking.
Objective:
To investigate the relationship between orthotic usage and functional activities in pediatric patients with different neuromuscular diseases.
Study design:
Retrospective study.
Methods:
A total of 127 subjects’ physical assessment forms were analyzed. Functional level, type of orthoses, falling frequencies, ankle joint range of motion, and timed performance tests were examined in two consecutive dates with an interval of 3 months.
Results:
A total of 91 patients were using orthoses while 36 patients were not within assessment dates. A total of 64 of 91 (70.3%) patients were diagnosed with Duchenne muscular dystrophy. A total of 81 (89.0%) subjects were using plastic ankle–foot orthoses for positioning at nights and 10 (11%) were using different types of the orthoses (knee–ankle–foot orthoses, dynamic ankle–foot orthoses, and so on) for gait in the study group.
Conclusions:
Night ankle–foot orthoses were not found to be effective directly on functional performance in children with neuromuscular diseases, although they protect ankle from contractures and may help to correct gait and balance.
Clinical relevance
This retrospective study shows that the positive effects of using an ankle–foot orthosis at night are not reflected in the functional performance of children with neuromuscular diseases. This may be due to the progressive deteriorating nature of the disease.
Background
Neuromuscular disorders (NMDs) are heterogenic group of hereditary or acquired diseases, which are derived from different parts of the motor unit, such as neuromuscular junction, muscle, and peripheral motor neuron. Primary disorders of the muscle such as muscular dystrophies, anterior horn cell diseases such as spinal muscular atrophies (SMAs), and diseases that affect peripheral nerves like neuropathies are the most frequent disorders of childhood in this group.1–3 World Federation of Neurology listed the most frequent hereditary neuromuscular diseases such as Duchenne muscular dystrophy (DMD), Becker muscular dystrophy (BMD), facioscapulohumeral (FSH) muscular dystrophy, limb girdle muscular dystrophy (LGMD), SMA, and hereditary motor and sensory neuropathy (HMSN). 4
Several health problems including orthopedic, respiratory, cardiovascular, nutritional, and gastrointestinal cause disabilities affecting daily living activities, mobility, motor performance, and quality of life of children with NMDs.5–7 The most frequent orthopedic problems of pediatric patients with NMDs are contractures, especially located in Achilles tendons and gastrocnemius muscle, which may occur asymmetrical from the very beginning of the disease process because of the asymmetric muscle weakness and cause the deterioration of pelvic obliquity and at last scoliosis.5,8–10 Hip and knee contractures are also problematic from the very early stages of most seen NMDs.8,10 It is important to maintain the symmetrical joint positions and flexible joints from the earliest period to preserve independent and functional ambulation and hip symmetry or provide appropriate seating position for nonambulant patients and to prevent scoliosis, which may cause the deterioration of respiratory functions.5,9,11 Other orthopedic problems are foot drop, which affects normal gait and balance in upright standing position and causes increased energy expenditure and reduced endurance; ankle–foot contractures causing equines; and pes cavus such as seen in Charcot–Marie–Tooth (CMT) disease and FSH muscular dystrophy.2,12
There are surgical and conservative treatment options for the above-mentioned orthopedic problems. Complications of surgical treatments (tendon lengthening, release techniques, arthrodesis, corrective procedures, and so on) for correction of the deformity, such as difficulty in using anesthetic agents due to poor respiratory function and cardiomyopathy, postoperative pain, aggravated weakness, the need for bracing after surgery, and loss of ambulation after surgery because of lower extremity muscle weakness and poor support of weak upper extremity muscles due to incorrect timing for this type of treatment, are some of the reasons why conservative treatment with orthosis and passive/active stretching and strengthening exercises may be preferred in some cases.6,8,13
Knee–ankle–foot orthoses (KAFOs) and ankle–foot orthoses (AFOs) are the most used orthoses in the conservative treatment of NMDs to prolong independent ambulation when gait becomes problematic because of proximal muscle weakness and muscle–tendon contractures. KAFOs and AFOs also help to prevent the progression of deformities and obtain optimal position of the joints to support standing and walking.2,5,8,13–17 AFOs were shown to be beneficial for both patients with distal and proximal muscle weakness and were effective in enhancing standing balance and posture.2,6,18 Articulated plastic AFOs limiting plantar flexion and assisting dorsal flexion of the ankle are effective in patients with peripheral neuropathy and distal weakness like patients with CMT disease who have insufficient dorsal flexor strength at the initial contact of heel during gait. 19 Positive effects on psychosocial coping mechanisms provided by prolongation of independent walking with KAFOs for pediatric patients with NMDs and their families have also been reported. 14
This study was planned to investigate the relationship between orthotic usage and functional activities in a heterogenous group of pediatric patients with NMDs, based on the hypothesis that orthotic usage may effect the physical performance in daily living activities of pediatric patients with NMDs.
Methods
The study was performed with retrospective design by analyzing the physical assessment forms of pediatric patients with NMDs. The ethical approval was granted from the department of Hacettepe University, Ethics Committee. The assessment forms were recorded with an interval of 3 months in a reference center for neuromuscular diseases in Turkey.
Subjects were divided into two groups as patients with NMDs who used orthoses [Group 1 (study group)] and patients with NMDs who do not use orthoses [Group 2 (control group)]. The inclusion criteria of the study for the study group were as follows:
Subjects who were diagnosed with one of the NMDs listed by the World Federation of Neurology 4 by a neurologist;
Subjects who were ambulant between the dates of at least two assessments;
Subjects who were using functional, supportive, or positioning orthoses;
Subjects who had two timed performance test records while using the orthoses within the assessment dates with an interval of 3 months.
The subjects who had the same inclusion criteria except for orthotic usage were included in the control group. The exclusion criteria were as follows:
Subjects who have a diagnosis concerning systemic and/or upper motor neuron disorders;
Subjects who had undergone lower extremity surgery before;
Subjects who were nonambulant and who stopped independent walking between two assessment dates were excluded from the study.
Functional levels of the subjects were determined using the Brooke Lower Extremity Functional Classification. 20 This classification was created on the basis of the Vignos scale to determine the functional status of lower extremity of DMD patients in clinical assessment.20,21 This functional classification groups the patients within 1–10 functional levels. Level 1 (the child walks and climbs stairs independently) shows the best functional motor performance, and Level 10 (dependent to the bed) shows the worst functional motor performance of children with NMDs. Types of the orthoses used by the subjects and orthotic usage period were recorded in the assessments.
These children were able to walk by means of using compensatory movements (e.g. ankle plantar flexion for knee extension, and lordosis to compensate the loss of hip extension). Our aim was only to prevent ankle plantar flexion from becoming a fixed equinus deformity. Therefore, we only measured the range of ankle movement. Ankle range of movement of the subjects was measured using a goniometer, and limitation of the ankle joint was recorded as right and left in two assessments.
The time elapsed during performance tests including 10m walking, standing from sitting position, supine and prone positions, sitting from standing position, and climbing up and down five steps was measured in seconds. Timed performance tests have been used by specialists to determine the functional status of the children affected by a neuromuscular disease with daily functional activities and also to specify the effects of a specific treatment approach including gene therapies or any other novel therapy methods. It is also found to be a valid and reliable outcome measure for DMD.7,20,22 The weekly falling frequencies of the subjects were also recorded by asking their families during clinical assessments.
The patients did not receive any individual physiotherapy treatment during the period of the study. They were all followed with previously given routine physiotherapy home program including the combination of stretching, strengthening, and aerobic exercises.
The subjects who use orthoses in daily living activities were allowed to use their devices during timed performance tests (10 m walking and climbing up and down five steps). The above-mentioned evaluations of the subjects who use orthoses (study group) and who do not use orthoses (control group) between at least two consecutive assessment dates with an interval of 3 months were taken into consideration for statistical analysis.
Statistical analysis
Means and standard deviations were recorded from the quantitative data of the study and control groups, while the frequencies were calculated from qualitative data (diagnosis, functional levels, steroid usage, and type of the orthoses). The intragroup comparisons of the first and second assessments were made using Wilcoxon signed-rank test. Mann–Whitney U test was used for intergroup comparisons. A p value of 0.05 is accepted.
Results
A total of 91 subjects who used orthoses between two consecutive assessment dates with an interval of 3 months were included in the study group, while 36 subjects who have not used any orthoses between these dates were included in the control group. A total of 82 (90.1%) of 91 subjects were male and 9 (9.9%) subjects were female in the study group. A total of 25 (69.4%) of 36 subjects were male and 11 (30.6%) subjects were female in the control group. A total of 81 (89.0%) subjects were using solid plastic AFOs for positioning at nights and 10 (11%) were using different types of the orthoses (KAFOs, dynamic AFOs, and so on) for gait in the study group.
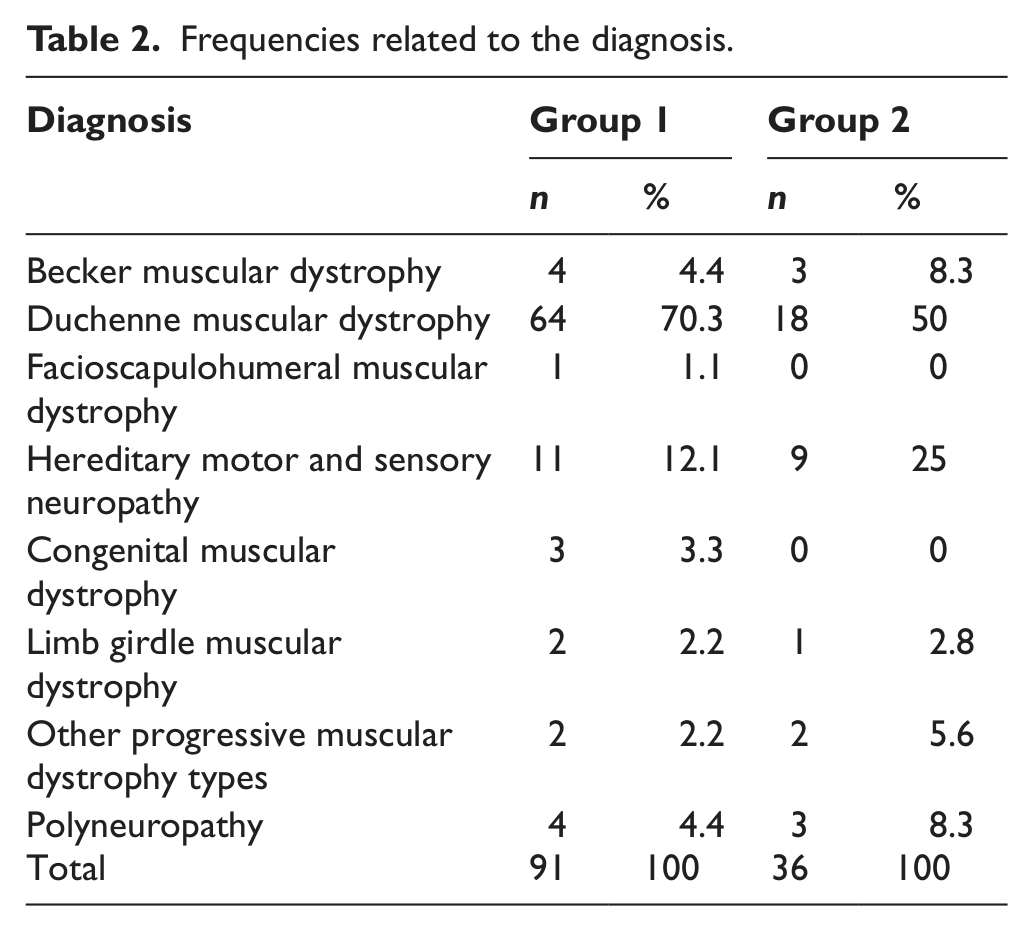
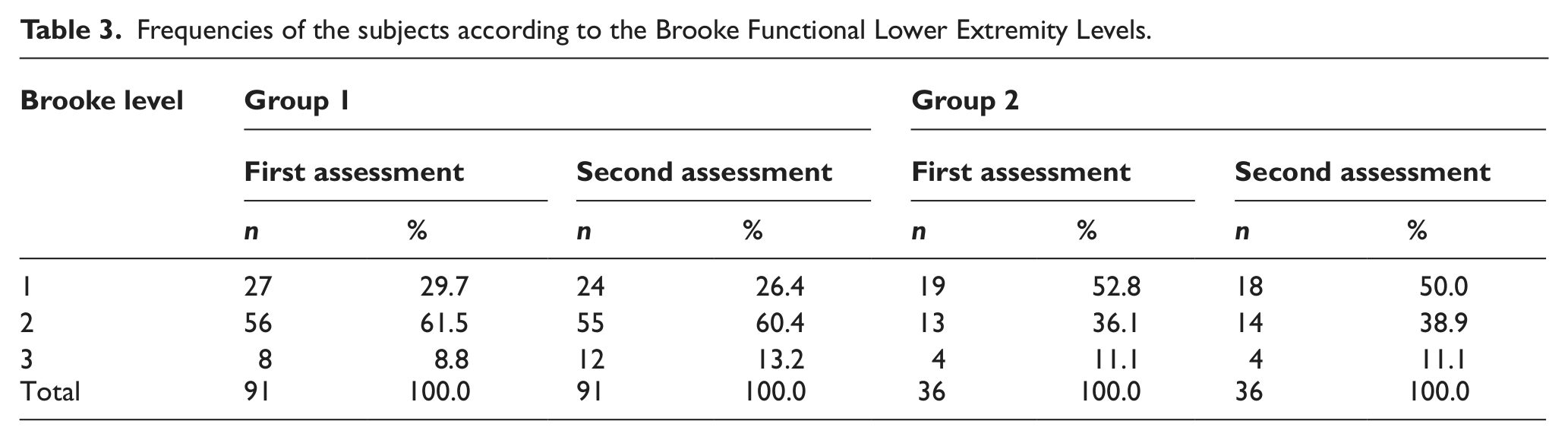
The demographic characteristics of the subjects including height, weight, age, and total orthotic usage duration are given in Table 1. Frequencies of the diagnosis and functional levels (according to Brooke Functional Classifications) of groups are given in Tables 2 and 3.
Demographic data of the subjects in the study (Group 1) and control groups (Group 2).
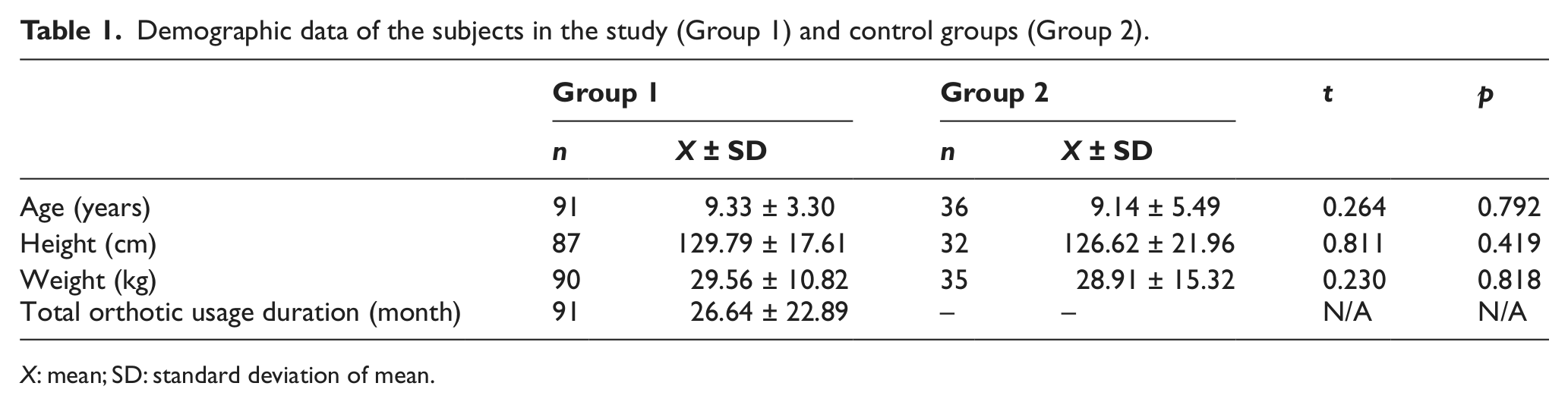
X: mean; SD: standard deviation of mean.
Frequencies related to the diagnosis.
Frequencies of the subjects according to the Brooke Functional Lower Extremity Levels.
The time elapsed during standing from supine and prone positions and climbing up five steps showed statistically significant increase between the first and the second assessments of the study group (p < 0.05) (Table 4). None of the assessed parameters showed statistically significant differences between the first and second assessments in the control group (p > 0.05) (Table 5). The comparison of the two groups according to the first and second assessments is given in Table 6.
Comparison of the first and second assessments of the study group (Wilcoxon signed-rank test).
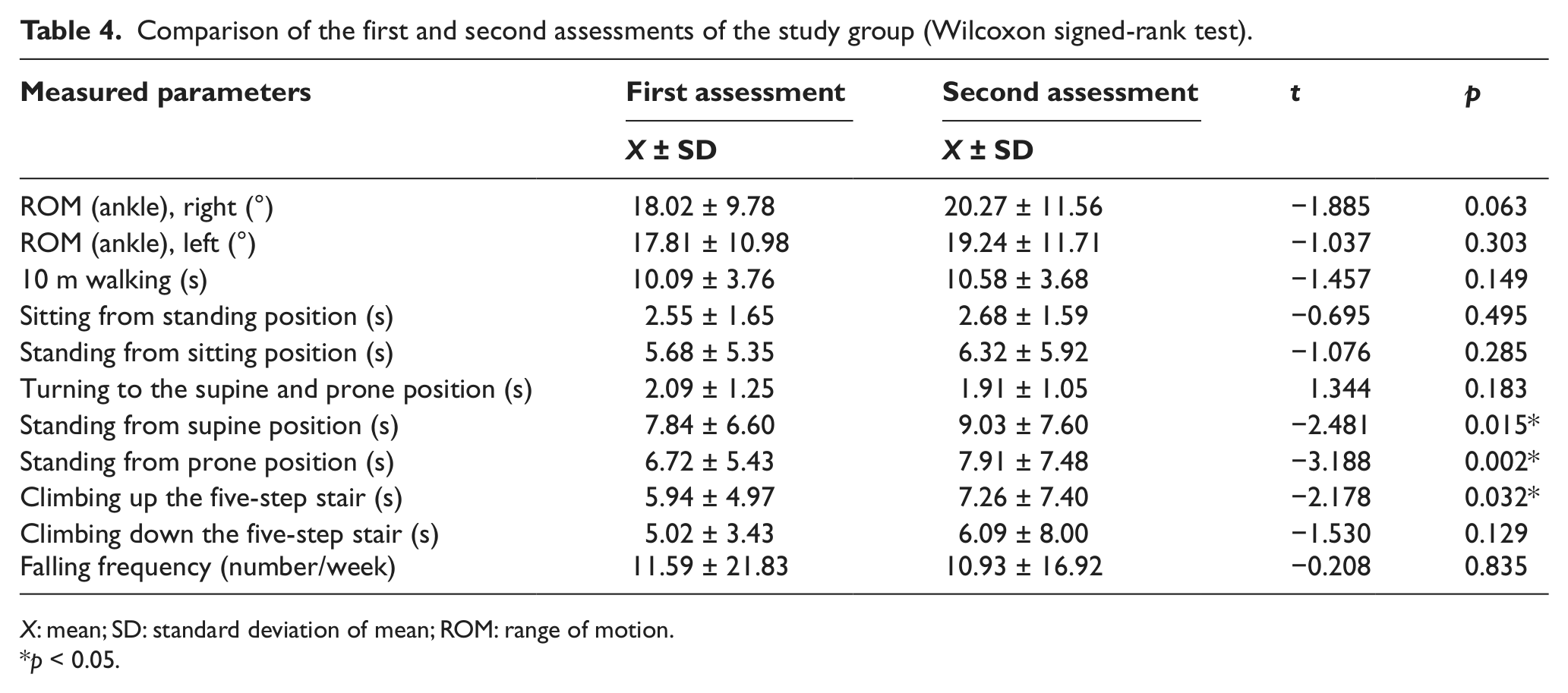
X: mean; SD: standard deviation of mean; ROM: range of motion.
p < 0.05.
Comparison of the first and second measurements of the control group (Wilcoxon signed-rank test).
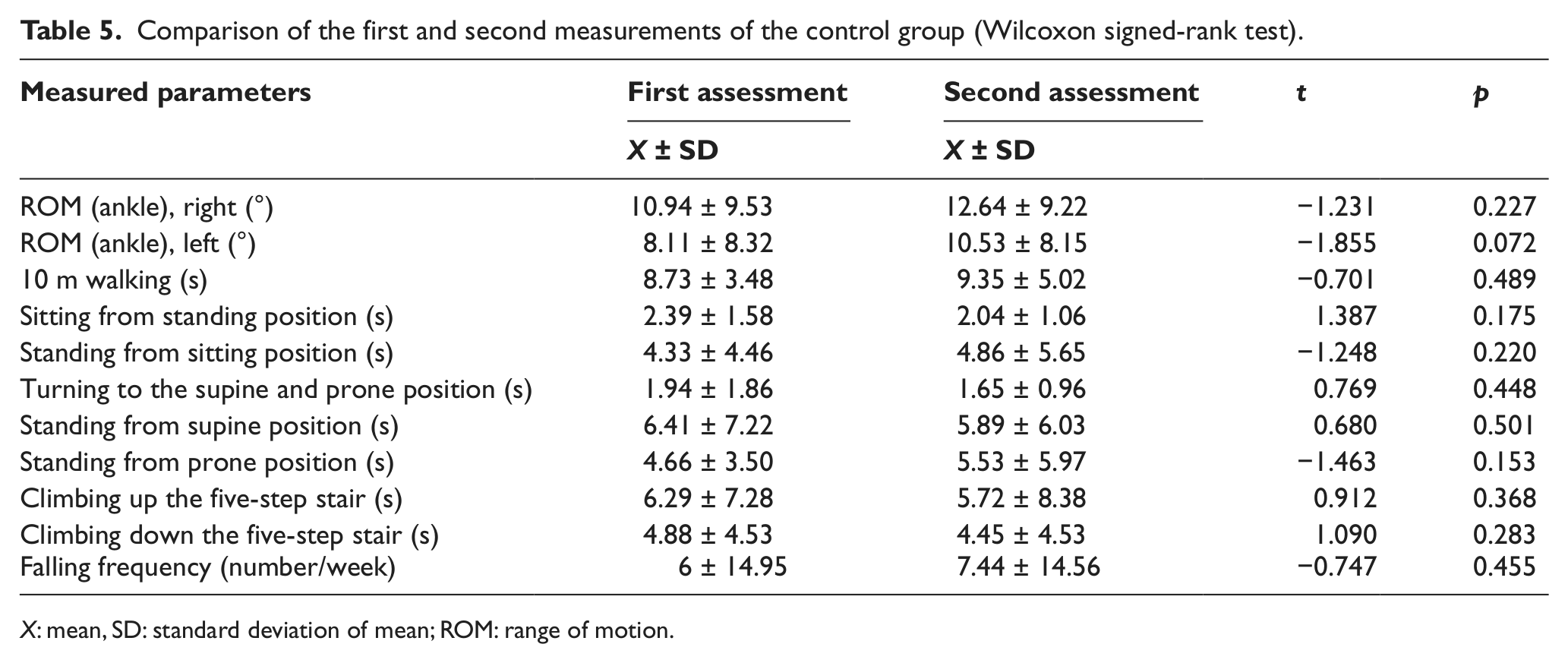
X: mean, SD: standard deviation of mean; ROM: range of motion.
Comparison of the two groups according to the first and second assessments (Mann–Whitney U test).
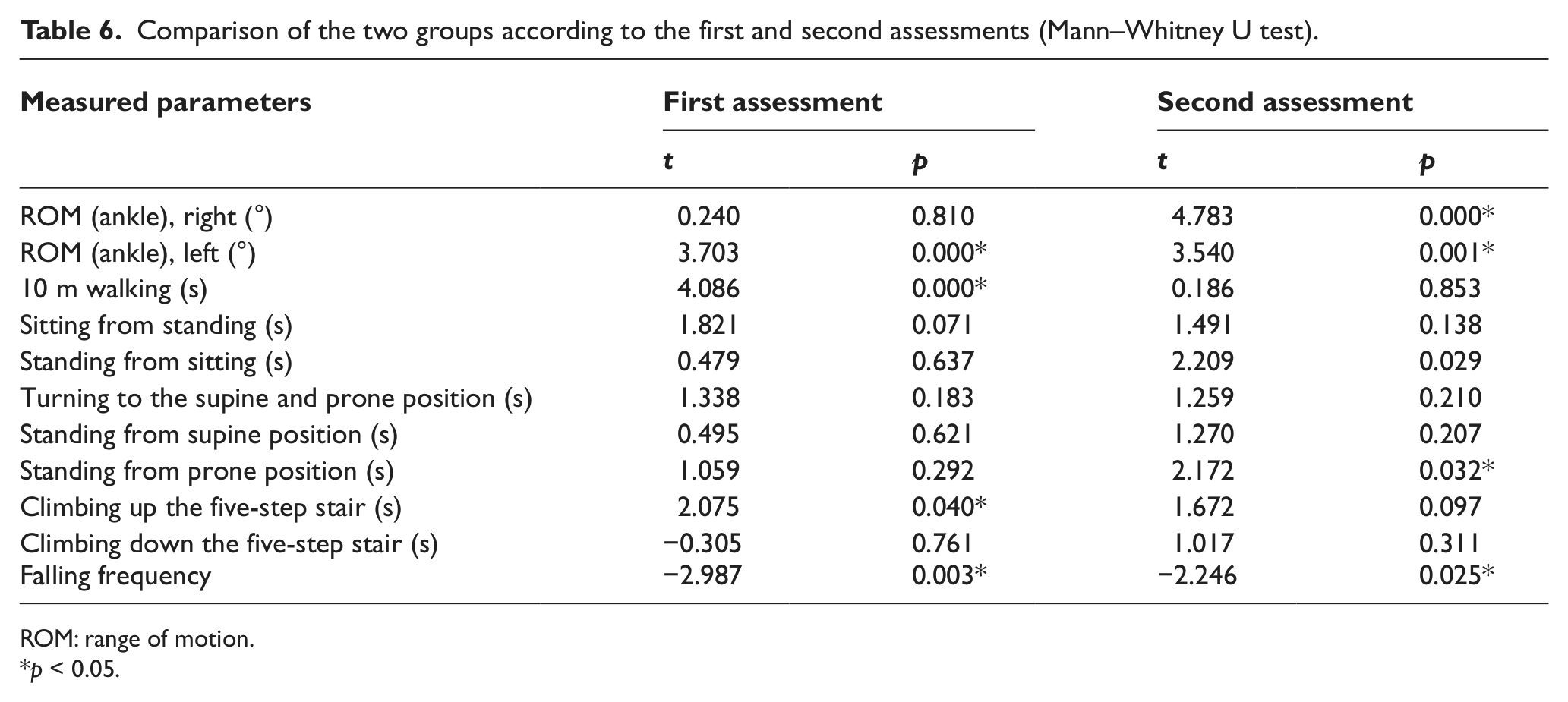
ROM: range of motion.
p < 0.05.
Discussions
This study was planned to investigate the relationship between orthotic usage and functional activities in a heterogenic group of pediatric patients with NMDs. Age-matched two groups whose diagnoses were one of the types of the NMDs were assessed two times with an interval of 3 months for functional status, ankle joint range of motion (ROM), timed performances, and falling frequency.
The functional levels of the children in the study group (using orthoses) were not as good as the children in the control group (not using orthoses). This is because of the prescription time of orthoses in NMDs. The deterioration in muscle and joint ROM becomes visible as the disease progresses and the child develops.5,23,24 Therefore, the need of the orthoses increases as the functional status worsen.
Orthoses are usually prescribed to maintain a plantigrade foot for ambulation, to protect skin and joints, and to distribute the weight over the foot until the disease progresses to a stage where the child becomes bedridden. 25 Most of the studies in the literature investigate the effects of the KAFOs on independent ambulation in children with DMD.14,17,26,27 KAFOs are usually prescribed at the time when the DMD child is prone to lose the ability of standing and walking independently. At this time, KAFOs were found to extend upright ambulation period for an average of 2 years.26,28 Taktak and Bowker 17 investigated the effects of modular KAFO usage in nine children with DMD between the ages of 5 and 13 years in their study. Modular KAFOs were found to be 23% lighter and 10% energy saving during gait. A 8% increase in walking speed was also reported when compared to existing KAFOs of the children. 17 In our study, KAFOs were not indicated to most of the children because of the early stage of their disease, and the results showed that the majority of the subjects were diagnosed as DMD and using AFOs for positioning in our clinic.
Scott et al. 24 assessed joint contractures and functional ambulation during 3 years with an interval of 3–4 months in DMD patients. In their study, early and continuous usage of AFOs was found to slow the contracture development and improve walking ability. 24 Plantar flexor contracture of the ankle is a common risk in all neuromuscular diseases. The equinus position of the ankle impedes heel contact and increases fore-foot contact, and consequently, the gravity line and ground reaction forces pass in front of the knee joint, behind the hip joint. Compensatory gait occurs and results in impaired ambulation. 6 In DMD, serious contractures may occur before the age of 9 years. Night splints were proven to decrease ankle joint limitations.29,30 In the study performed with 25 CMT patients with drop foot, patients declared that AFOs corrected the standing and walking posture, although they had poor compliance and less comfort with AFOs. 31 Patients with CMT are usually using the daytime AFOs to improve their walking ability, avoid falling, and prevent secondary gait pathologies because of foot drop. 12 Patients also have cosmetic concerns. Patients with CMT complain that daytime AFOs highlight their disability. 31 These studies show that AFOs are necessary to prevent the formation of contractures from the very beginning of the disease and to maintain walking ability, although they are not comfortable and less acceptable by patients with neuromuscular diseases. In our study, subjects were mostly using AFOs (89%) at night to position their ankle joints and avoid contractures. Despite this, they had the same complaints that AFOs were not comfortable and disturbed them during sleep.
Continuous usage of appropriate AFOs was assessed for CMT and DMD patients in the literature.23,32 Appropriate AFOs, which were prescribed on time, were found to provide body alignment and stability of the limbs passively and control the posture and gait indirectly in both the CMT and the DMD groups.23,32 While controlling deformity, correction of the balance and gait should also be considered for AFO prescription. 32 In our study group, subjects who were using orthoses (89% of the subjects used plastic AFOs and 11% used other types of orthoses like KAFOs, dynamic AFOs, and so on) maintained their functional status and ankle ROM between evaluation dates. Standing from the sitting and/or supine position is the indicator of the gait performance. Ankle dorsal flexors are important to transfer the body weight to the front. In muscular dystrophies, this ability is limited by ankle contractures. 33 The decrease in the duration of timed performance tests as standing from sitting, prone and supine positions and five steps climbing, which were the indicators of performance, AFOs were thought to improve weight distribution of the foot by means of a plantigrade contact during ambulation. The correction of body alignment provided by AFOs and the progressive characterization of the disease might be a cause of slowdown in performance time. Therefore, the quality of gait and balance could be recovered while the functional activity period was extending with disease progression.
Conclusion
It is important to prescribe appropriate orthoses on time, especially in the very beginning of the disease course after diagnosis to prevent joint limitations and contractures, maintain independent ambulation as long as possible, correct the secondary gait pathologies of muscle weakness, and improve balance in pediatric neuromuscular diseases. Night AFOs are not found to be effective on the development of functional performance in children with neuromuscular diseases, and the hypothesis of the study was rejected. Nevertheless; functional performance may be corrected and recovered using orthoses on time, but the progressive characterization of most of the NMDs may not allow improvement in performance. Despite poor compliance, night AFOs are effective in protecting ankle from contractures and may help to correct gait and balance. The short period of screening the evaluations (3 months) and the lack of biomechanical screening of ankle are seen as limitations of the study.
Footnotes
Conflict of interests
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.