
Abstract
Background:
External devices are used to manage musculoskeletal pathologies by altering loading of the foot, which could result in altered muscle activity that could have therapeutic benefits.
Objectives:
To establish if evidence exists that footwear, foot orthoses and taping alter lower limb muscle activity during walking and running.
Study design:
Systematic literature review.
Methods:
CINAHL, MEDLINE, ScienceDirect, SPORTDiscus and Web of Science databases were searched. Quality assessment was performed using guidelines for assessing healthcare interventions and electromyography methodology.
Results:
Thirty-one studies were included: 22 related to footwear, eight foot orthoses and one taping. In walking, (1) rocker footwear apparently decreases tibialis anterior activity and increases triceps surae activity, (2) orthoses could decrease activity of tibialis posterior and increase activity of peroneus longus and (3) other footwear and taping effects are unclear.
Conclusion:
Modifications in shoe or orthosis design in the sagittal or frontal plane can alter activation in walking of muscles acting primarily in these planes. Adequately powered research with kinematic and kinetic data is needed to explain the presence/absence of changes in muscle activation with external devices.
Clinical relevance
This review provides some evidence that foot orthoses can reduce tibialis posterior activity, potentially benefitting specific musculoskeletal pathologies.
Background
Musculoskeletal pathologies occur when structures experience more load than they can withstand. 1 If external loads are altered by a therapeutic device, there should be a corresponding change in internal muscle-tendon forces, joint loading, the potential for injury, and the rate and likelihood of healing. For example, foot orthoses (FOs) that decrease loading at the rearfoot could decrease activity of the tibialis posterior (TP) muscle and subsequently reduce strain of the TP tendon, a structure vulnerable to tendinopathy. 2 Clinicians can influence the forces applied to feet and muscles/tendons using footwear, FOs and taping.
Footwear that may have therapeutic benefits by altering loading of the foot include ‘motion control’ shoes (typically running shoes), and rocker/rollover shoes. While motion control shoes with dual density midsoles reduce calcaneal eversion by 2.77° (p < 0.001, 95% confidence interval (CI) = 1.74° to 3.81°), 3 whether these changes impact on muscle function and injury risk is unknown. Under the ‘preferred movement pathway’ theory, 4 footwear or FOs reduce muscle activity and metabolic demand4,5 by promoting the path of ‘least resistance’ and reduce injury risk.4–6 However, muscle activity could also increase to keep foot kinematics within the preferred pathway. 6 Rocker or rollover shoes have outsoles curved in the sagittal plane and alter the contact area between the shoe and floor, plantar load, external sagittal plane joint moments, and thereafter muscular responses and joint motion. 7 A recent review, however, found few statistically significant effects of the Masai Barefoot Technology (MBT) shoes on lower limb muscles. 8 The effect of other rocker and motion control footwear on electromyography (EMG) data has not been reviewed, so the use of these specialised shoes for treatment and injury prevention is unclear.
FOs redistribute plantar pressure, altering external joint moments, internal joint moments (from muscles and connective tissue) and foot motion. Examples include insoles with rearfoot wedges and arch supports, 9 also known as ‘anti-pronation’ FOs or medial posted FOs. Although FOs reduce peak rearfoot eversion by 2.08°−2.35° (p ⩽ 0.004) depending on their design, 3 such small changes may not be clinically meaningful. 10 FOs can change ankle moments11–13 with peak and mean ankle eversion moments reduced by 1.1% ± 1.1% (p = 0.003) and 2.3% ± 2.1% (p < 0.001) per 2° of medial posting, respectively. 13 Such changes would alter the requirements of tissues acting antagonistically to the external moments, including muscles. The evidence for changes in muscle function with FOs that alter joint kinematics and kinetics is important in understanding injury risk and tissue repair.
Low-Dye taping is a temporary intervention for conditions supposedly associated with foot pronation or flat-arched feet,14,15 theoretically applying tension to the skin using tape offloads structures in the medial arch.3,14,16 Taping has been reported to only reduce foot pronation by a non-significant 1.50° (p = 0.19, 95% CI = −0.73° to 3.73°). 3 Plantar sensory stimulation is considered an important difference between FOs and taping since changes in afferent feedback due to tape might alter muscle activation. 14 However, there is no evidence to support this theory.
Prior reviews investigating the effects of footwear, FOs and taping did not compare device effects.8,16,17 Also, approaches to searching and appraisal of literature were variable and underpin the need for a more comprehensive review. Indeed, limitations of prior studies include low power, inadequate reporting of EMG procedures and low external validity.16,17 A review of foot posture, FOs and footwear by Murley et al. 17 allowed comparisons to a barefoot control, which is less clinically generalisable than a shod control and the review was broad, including all types of FOs and inserts and all footwear, not just that intended to alter foot biomechanics. The present review includes only FOs with a medial arch profile and/or medial heel/foot wedge in order to improve our understanding of the relationship between medial FOs and muscle activity. Furthermore, the recent review of MBT footwear did not assess the quality of EMG data reporting, limiting our understanding of the strength of the evidence identified. 8 Several studies on the effect of external devices on EMG have been published since these reviews, some of which have reported detailed EMG methods, 18 thus further justifying an update on the literature consensus. The aim of this systematic review was to investigate the level of evidence from any study design that investigated whether footwear, FOs and taping alter lower limb EMG during walking and running, irrespective of health status.
Methods
Search strategy
A systematic, electronic database search was performed by reviewer J.R. using CINAHL (1982–2017), MEDLINE (1950–2017), ScienceDirect, SPORTDiscus (1985–2017) and Web of Science (1900–2017) in October 2015 and updated in March 2019. The review conformed to the PRISMA guidelines for systematic reviews; however, we were unable to account for biases like publication bias. 19 Searched words are included Table 1. Lines (1)–(3) were combined using ‘AND’ with lines (4) and (5). Additional sources were identified from published reviews and the reference lists of studies that passed the quality screening.
Inputs to the electronic databases (all databases).
EMG: electromyography; iEMG: integrated electromyography.
Lines (1)–(3) were combined using ‘AND’ with lines (4) and (5). * denotes a wildcard
Inclusion criteria
The search results were assessed for eligibility based on titles and abstracts of original, full text articles using the following inclusion criteria:
A clearly defined amplitude, timing or frequency EMG outcome measure from muscles of the lower limb.
A fully specified independent variable of any footwear designed with modifications in the shape or material of the sole (including a negative heel, but excluding high heels, ankle braces and ankle destabilisation devices), FOs/insoles (orthosis had a medial arch profile and or medial heel/foot wedge, excluding lateral wedges and ankle-FOs) and taping about the foot/ankle intended to reduce foot pronation (excluding Kinesio taping).
Measures were made during level walking or running.
The footwear, FOs or taping experimental conditions were compared with a shod control condition.
For FOs and taping experimental conditions trials were performed in shoes, not sandals, with all the standard components of a shoe that brace the FOs.
Participants were free from conditions affecting the neurological systems.
Data were analysed from a minimum of three trials per condition.
Full text was published in English, French or German (due to available expertise).
Sample size of n > 1.
Only studies on locomotion were included since major theories on mechanisms of therapeutic effect of external devices relate to gait not standing. 20 Studies that only compared the device to barefoot were excluded because EMG amplitude can increase due to shoes alone and FOs versus barefoot (+30% and +30% to 38% respectively in tibialis anterior (TA)). 21 Articles were excluded if there were less than three trials per condition because without contradictory evidence, this was considered the minimum required for quality data. We did not restrict studies to a specific population as we took a mechanistic approach to understanding potential effects of external devices on muscle activity.
Quality assessment
To maintain quality standards in this systematic review, the articles that met the inclusion criteria were subject to two levels of quality assessment (Table 2), performed independently by reviewers J.R. and E.P. performed independently. After studies were assessed, the two reviewers met to discuss discrepancies. When discrepancies persisted these were discussed with a third reviewer (L.B.) and a final score obtained.
Quality assessment criteria checklists.
EMG: electromyography; RMS: root mean square; FO: foot orthoses; SENIAM: surface EMG for non-invasive assessment of muscles.
The first stage focussed on the quality of the EMG methodology based on external standards of reporting, 24 plus controlling locomotion velocity (since velocity can affect EMG). 23 Studies scored a 1 or 0 depending on whether the criteria were fulfilled or not, and the results were summated and expressed as a percentage. Studies achieving less than 50% were excluded.
The second stage of assessment was based on a modified subset of a checklist for rating clinical interventions. 25 Studies were given 1 or 0 depending on whether each criteria was fulfilled, with the total score expressed as a percentage and studies that scored less than 50% were excluded.
Results
Search results
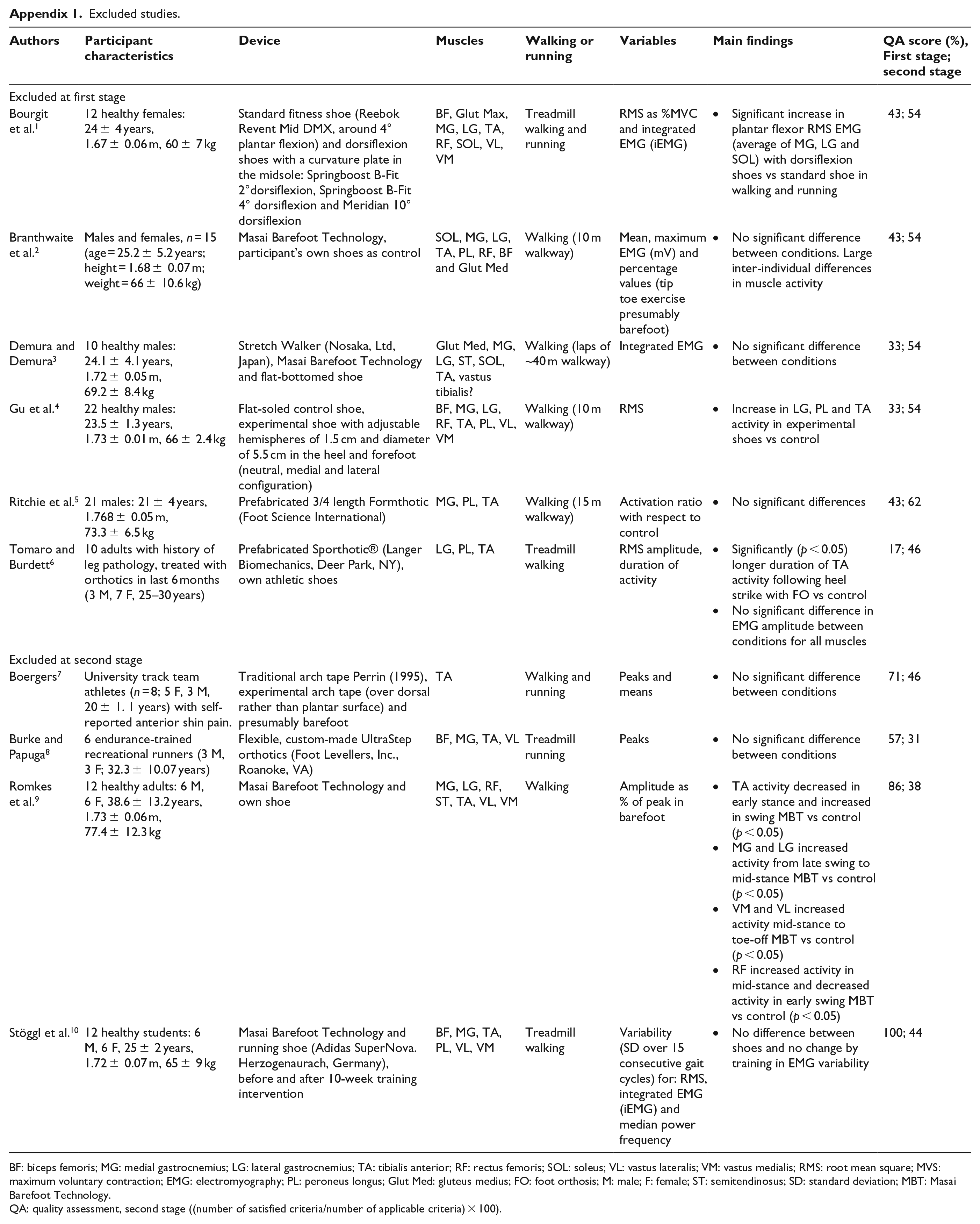
A flow chart of the selection process from identification to screening, and eligibility and inclusion 19 is presented in Figure 1; six studies were excluded based on EMG quality and four studies were excluded based on study design quality. A total of 31 studies were included, of these, 22 related to footwear and 8 to FOs. Key themes of footwear studies were running shoes, rocker footwear, APOS-Therapy shoes26,27 and the Reebok EasyTone® shoe. Only one taping study (low-Dye) was identified which passed quality assessment. No study from additional sources met the inclusion criteria. Two studies were translated from German, but did not meet the inclusion criteria. Most studies included healthy, often recreationally active participants, except two studies involving participants with knee pain/knee osteoarthritis,28,29 one with running related overuse injuries 30 and one with Achilles tendinopathy. 31 Summaries of included studies are in Tables 3 and 4 and excluded studies in the Appendix 1.
Study selection flow chart.
Summary of studies on the effect of footwear (n = 22) and taping (n = 1) on lower limb muscle activity.
ARV = average rectified value, LE = lower extremity, M = male, F = female, RMS = root mean square, TP = tibialis posterior, TA = tibialis anterior, SOL = soleus, PL = peroneus longus, MG = medial gastrocnemius, LG = lateral gastrocnemius, AT = Achilles tendinopathy, VL = vastus lateralis, VM = vastus medialis, BF = biceps femoris, Glut Med = gluteus medius, Glut Max = gluteus maximus, ES = erector spinae, RF = rectus femoris, ST = semitendinosus, MBT = Masai Barefoot Technology, OA = osteoarthritis. QA = quality assessment, for first and second stage ((number of satisfied criteria/number of applicable criteria)*100).
Summary of studies on the effect of foot orthoses (n = 8) on lower limb muscle activity.
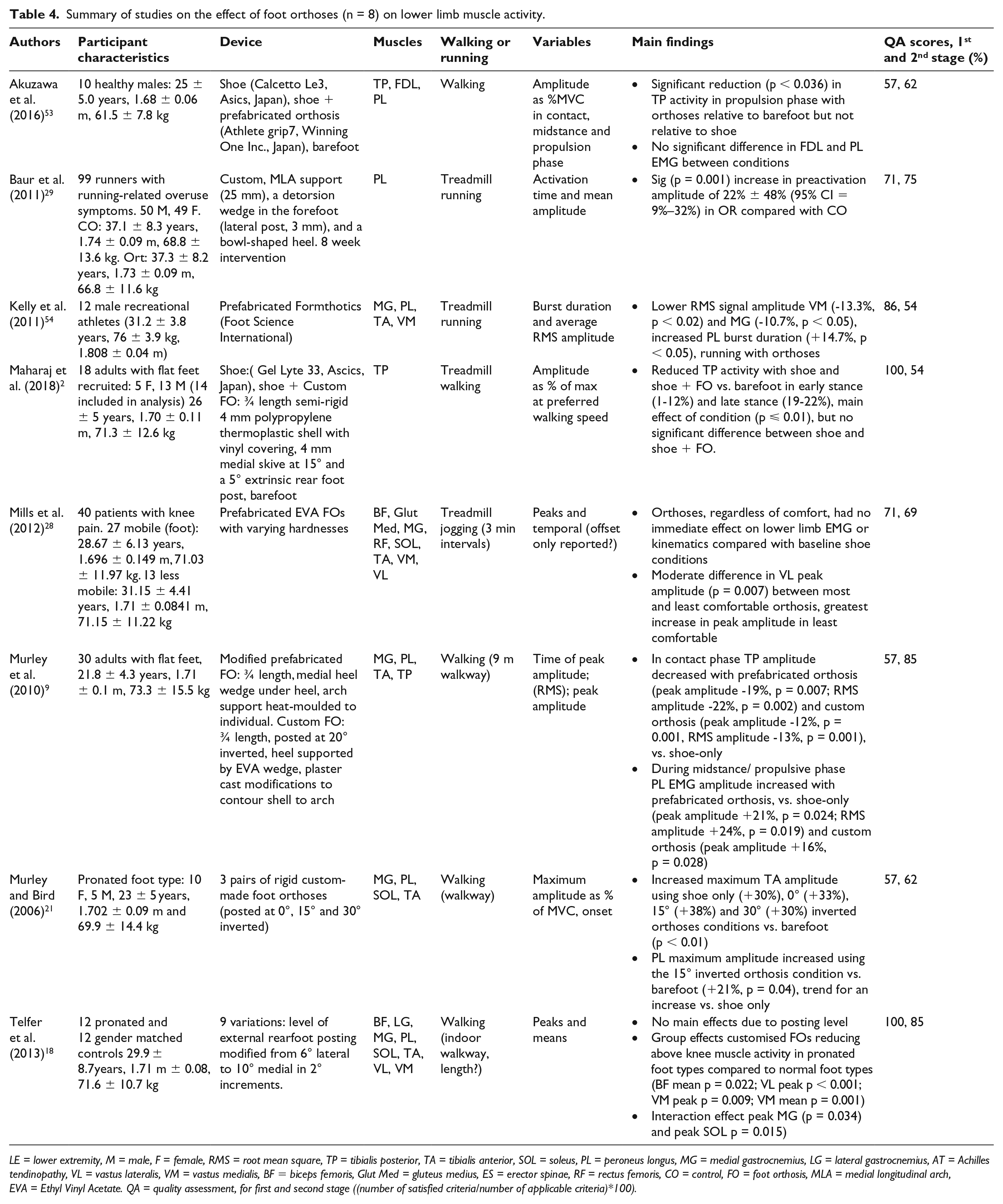
LE = lower extremity, M = male, F = female, RMS = root mean square, TP = tibialis posterior, TA = tibialis anterior, SOL = soleus, PL = peroneus longus, MG = medial gastrocnemius, LG = lateral gastrocnemius, AT = Achilles tendinopathy, VL = vastus lateralis, VM = vastus medialis, BF = biceps femoris, Glut Med = gluteus medius, ES = erector spinae, RF = rectus femoris, CO = control, FO = foot orthosis, MLA = medial longitudinal arch, EVA = Ethyl Vinyl Acetate. QA = quality assessment, for first and second stage ((number of satisfied criteria/number of applicable criteria)*100).
Quality assessment
The included studies scored 50–100 on EMG quality (mean ± standard deviation (SD): 75 ± 13). Unfulfilled criteria for EMG quality spanned categories 1–6. Almost all studies were deemed to have provided adequate details on normalisation where appropriate, although none as detailed as published recommendations, for example, training to produce a maximum voluntary contraction (MVC). 24 Of included studies, 14/31 did not specify EMG sensor fixation and 13/31 did not control velocity.
Based on the second stage of quality assessment, the included studies were generally of moderate quality (scored 54–85, mean ± SD: 64 ± 9). Excluded studies scored 31–46 (mean ± SD: 40 ± 7). Many studies did not report device material, participant and assessor blinding, statistical analysis or power analysis. Variability was not reported in 3/4 of excluded studies. In addition, condition randomisation was absent in 8/31 of the included studies and 2/4 of the excluded studies.
Overview of included studies
Footwear
Running shoes
A stability running shoe with a dual-density medial post and foot bridge had no effect on EMG activity during walking versus a standard flexible shoe for the peroneus longus (PL), medial gastrocnemius (MG), soleus, TA and TP. 52 However, a motion control running shoe with a dual-density midsole (firmer material on the medial versus lateral side) reduced mean TA and PL activity and delayed fatigue during running 50 versus a cushioned running shoe. Delayed fatigue was demonstrated by maintained median frequency of TA and PL during a 10-km run.
A shoe with a medial wedge (3 cm thick on the medial side, 2 cm thick on the lateral side) increased mean TA amplitude by 16% during treadmill running versus a neutral shoe, 36 but not during overground running. 46 The activity of the gastrocnemii, soleus, PL and TP were not affected by medial or lateral wedges.36,46 However, TP EMG data were only available for four participants due to measurement difficulties.36,46
The relative timing of vastus medialis (VM) and vastus lateralis (VL) activation during running was compared between a motion control running shoe with a dual-density midsole and a cushioning running shoe. 45 This comparison was made based on the premise that delayed onset of VM with respect to VL is associated with patellofemoral pain. 45 The authors normalised EMG signals to a ‘duty cycle’ (defined in the animal literature as stance expressed as a percentage of step cycle, that is, stance + swing). 35 In the motion control shoe, activation of VM occurred ~5.3% (95% CI = 4.5% to 6.1%) of a duty cycle earlier than VL (during a 10-km run). In contrast, VM activation occurred ~4.6% (95% CI = 3.9% to 5.3%) later than VL in the neutral shoe. 45 The implications of the findings are limited by the ambiguity of the reporting of the methods.
Rocker footwear
TA amplitude in early stance in walking reduced by ~30%–40% (p < 0.05) with rocker footwear like MBT, which is curved under the heel in the sagittal plane, versus flat heeled conventional footwear.7,47,55 There was also a trend towards reduced TA EMG intensity when walking in MBT versus a running shoe. 49 A modified shoe with a forefoot rocker only increased peak TA activity in walking (by 20%–35%, p < 0.001, p = 0.015 respectively), but not in running.31,44 The shoe did not alter triceps surae (TS) activity in late stance during either walking or running.31,44
Increased PL activity throughout stance (e.g. 50% at loading response, p = 0.02) has been shown with MBT. 55 Other footwear in that study, including FitFlopsTM, designed to be unstable in the sagittal plane, increased peroneal activity during pre-swing. However, later work found no difference in PL activity with FitFlops 51 or difference in co-contraction with regular flip-flops. 48 A minimalist shoe reduced TA activity and increased plantar flexion in early stance relative to control footwear, however walking speed was also slower. 34
Changes in TS activity during loading response with rocker footwear are opposite to that of TA.7,55 The integral of the EMG profile in rocker footwear was 8%–13% (p < 0.05) greater than the control shoe for the soleus and 5.5%–8% for the MG (significant for MBT, p < 0.05, but not other rocker shoe, p > 0.05). 7 Similarly, integrated EMG of MG was 6%–16% (p < 0.05) higher and 8%–23% (p < 0.01) higher in soleus in a rocker shoe compared with a regular walking shoe in treadmill walking. 38 There was also a trend towards increased MG EMG intensity walking in MBT compared with a running shoe in another study. 49 Activation of MG was unaffected when wearing a FitFlop sandal with a variable density sole.43,55
Studies recording quadriceps activation during walking have generally found no effect of rocker footwear.7,47,49,55 However, increased activation of VL and greater co-contraction of vastii and MG across stance was found in MBT.32,33 Activation of biceps femoris or rectus femoris was unaltered by a FitFlop sandal. 43 Stiff soled safety shoes significantly increased VL, biceps femoris and TA activity relative to a soft-soled trainer. 41
APOS-Therapy shoes
APOS-Therapy shoes have adjustable domes on the sole allowing manipulation of centre of pressure (COP) position and external joint moments.26,27 In females with knee osteoarthritis, a lateral shift in the sole domes and COP reduced averaged TA EMG amplitude in pre-swing versus a neutral dome configuration. 28 The EMG amplitude of the lateral gastrocnemius increased with a medial shift in COP and decreased with a lateral shift in COP due to APOS-Therapy shoes (compared with neutral). 28
Reebok EasyTone shoe
The Reebok EasyTone shoe, designed to be unstable with balance pods, did not alter muscle activation in walking of any thigh, shank or gluteal muscles.32,37,39
Foot orthoses
There is some limited evidence that FOs decrease activity of TP in early stance and increase activity of PL in mid-late stance.9,21 Peak amplitude and root mean square (RMS) amplitude of TP during loading response was shown to reduce by 19% (p = 0.007) and 22% (p = 0.002), respectively, with custom FOs, and 12% (p < 0.001) and 13% (p = 0.001), respectively, with prefabricated FOs. 9 Whereas PL activity increased in midstance with a prefabricated FOs (peak amplitude + 21%, p = 0.024; RMS amplitude + 24%, p = 0.019) and a custom FOs (peak amplitude + 16%, p = 0.028) compared with a shoe only. Maximum PL amplitude has also been shown to increase in walking by 19% for pronated individuals when wearing 15° inverted FOs versus shoes alone (p < 0.05). 21 However, PL amplitude does not appear to increase linearly with wedging magnitude.18,21 Another two studies found TP activity was not significantly different between the footwear and FOs conditions (p > 0.05), although there was a decrease of around 10% (p < 0.05) from barefoot to shod and shod with either a prefabricated or custom FOs, which was not considered clinically generalisable in this review.2,40 However, in the study that recorded kinematics and kinetics, there was also no effect of FOs on subtalar joint displacement or supination moment relative to the shoe condition. 2 There was no difference in flexor digitorum longus or PL activity between conditions. 40
As for TA and TS, most evidence indicates magnitude and timing of activation is unchanged by wearing FOs during walking and running.18,21,29,53 One study found there was a tendency for FOs to decrease TA activation during walking versus a shoe only (effect size 0.18–0.29, for custom and prefabricated FOs respectively), although the result was not statistically significant. 9
Activity of PL may also increase with FOs during running. In one study, 99 runners with an overuse injury were assigned to customised FOs or no FOs. 30 In treadmill running, there was a significant increase (p = 0.003) in PL pre-activation amplitude (EMG activity prior to foot contact) after 2 months of wearing FOs, but not in the control patient group. 30 It is unclear whether change was in barefoot running or the running shoes or both. Another study reported a 14.7% (p < 0.05) greater duration of PL activity (the muscle was active for longer) during running with prefabricated FOs compared with no FOs as well as lower average MG and VM RMS amplitude with FOs versus no FOs. 53
Low-dye taping
In the only study included involving taping a significant delay (5%–7%, p = 0.001) in onset times of VM, VL and gluteus medius was found during shod running with low-Dye tape compared with control taping. 54
Discussion
The aim of this review was to establish if there is evidence that footwear, FOs and taping alter muscle activity of the lower limb during walking and running. The effect of running shoe design, FitFlops sandals and low-Dye taping on muscle activity is unclear, while rocker/rollover shoes appear to affect muscle activity of MG and TS.7,38,55 There is evidence, albeit limited, that FOs decrease activity of TP in early stance, 9 which could be beneficial in treating posterior tibial tendon dysfunction (PTTD). Activity of PL may increase in mid-late stance,9,21 otherwise FOs do not appear to alter EMG of lower limb muscles.9,18,21,29
Footwear
Running shoes
The effect of running shoe design on muscle activity remains unclear due to uncertainty regarding whether the shoes tested were effective in changing loading. No study investigating the effects of running shoe design on EMG during walking or running collected simultaneous kinematics or kinetics.45,50,52 Without kinetic data, we cannot determine if the footwear changed loading of the foot, which might sometimes explain the absence of change in EMG. Concurrent collection of kinetic and EMG data would also be useful to establish if the difference between a nil effect of motion control shoes in walking and a reduction in fatigue during running are due to the greater forces in running, foot strike patterns or different shoe properties.50,52
Similarly, sagittal plane kinematics were not reported in studies involving a medial wedged shoe.36,46 Wedging could increase ankle plantar flexion and increase demand on TA, potentially explaining the 16% increase in TA amplitude during treadmill running compared with a neutral shoe. 36 Perhaps a medial wedged shoe is substantially different to a motion control running shoe with a dual-density midsole if the effects of the wedge are not isolated to the frontal plane.
Rocker footwear
Footwear that shifts the COP anteriorly at heel contact reduces TA amplitude between initial contact and into midstance.7,47,55 An anterior shift in the COP increased the external dorsiflexion moment, resulting in a more dorsiflexed ankle and less work required from TA to control plantar flexion after initial contact. 7 Increased external dorsiflexion moment/increased internal plantar flexion moment in early stance would also account for the increases in TS activity with some rocker footwear.7,38,55 Potentially, the increased PL activity in MBT shoes 55 is due to the need for PL to contribute to sagittal plane moments. In contrast, the increase in TA activity in walking with the shoe with the modified forefoot rocker31,44 might be explained by the greater mass and sole thickness of the modified shoe versus the control. As TA is active in swing, greater activity during early stance could result from the greater moment of inertia not the sole curvature.
Rocker footwear have been shown to reduce internal plantar flexion moment in late stance, which could be beneficial for offloading the Achilles tendon when treating Achilles tendinopathy.8,31,44 However, reduced internal plantar flexion moment in late stance is not necessarily coupled to reduced TS activity in the same phase.31,44,55 This could be because peak of MG activity is earlier in stance than the peak of the internal plantar flexion moment, 7 and the energy recoil of the Achilles tendon is in terminal stance. Thus, reduced loading of the Achilles tendon suggested by a reduced internal plantar flexion moment may still be beneficial in treating Achilles tendinopathy.
The curved sole of rocker footwear purportedly reduces contact area with the ground and thus reduces stability. Increased co-activation from TA and TS in early stance with MBT may increase ankle stability to compensate. 7 The induced instability is assumed to increase movement variability and activate muscles required to maintain balance and control movement. 42 Greater movement variability could be beneficial in managing chronic injury if it reduced the repetitive loading of injured structures. 56 Conversely, increased co-activation increases joint loading. 57 Consequently, the clinical implications of altered muscle activation and reduced internal plantar flexion with rocker footwear remains unestablished. In addition, there was no effect of the modified rocker shoe on pain in individuals with chronic Achilles tendinopathy, and randomised clinical trials are necessary to evaluate the therapeutic effect of rocker footwear. 31
APOS-Therapy shoes
Reduced TA and increased TS activation with APOS-Therapy shoes could be relevant to those with TS and Achilles injury, anterior compartment syndrome and intermittent claudication, but any implications remain speculative.
Foot orthoses
There is some limited evidence that FOs decrease activity of TP in early stance and increase activity of PL in mid-late stance,9,21 but otherwise there appears to be a lack of effect of FOs on lower limb muscle activity during walking.9,18,21,29,53
As the primary invertor of the foot TP acts eccentrically during early stance to generate an inversion moment that opposes the external eversion moment, and helps control rearfoot eversion. It also acts concentrically to support foot supination later in stance. 58 If FOs increase the external inversion moment, they might reduce required internal inversion moments, reducing TP activity. Reduced TP activation could mean less force through the TP tendon which could facilitate healing in pathologies like PTTD. The limited amount of evidence on the effect of FOs on TP is likely because indwelling EMG is required to measure TP activity. Further research with adequate power and concurrent collection of kinematic and kinetic data is needed to relate kinetic and kinematic changes to muscle activation.
A linear dose-response to extrinsic rearfoot posting during walking has been demonstrated in kinematic, kinetic and plantar pressure variables, but without a corresponding effect on any EMG-related muscle activity in the calf muscles (including PL), quadriceps or hamstrings.13,18 Maximum PL amplitude did increase in walking by 19% for pronated individuals when wearing 15° inverted FOs versus shoes alone, but again without a linear dose-response to magnitude of wedging. 21 The lack of a dose response to medial rearfoot wedging could infer that the FOs exert their effect on PL due to changes in load under the medial longitudinal arch rather than the rearfoot. 21 The midfoot is in contact with the ground during midstance and the heel is unloading. 59 Similarly, in later work by Murley and colleagues, flat-footed participants increased PL activity in midstance with prefabricated FOs (peak amplitude + 21%, p = 0.024; RMS amplitude + 24%, p = 0.019) and custom FOs (peak amplitude + 16%, p = 0.028) compared with a shoe only. 9 The original authors speculated that increased PL EMG amplitude resulted from the foot being more laterally unstable. If FOs increased the external inversion moment, greater PL EMG activation may be needed to maintain equilibrium. As PL is the antagonist of TP, if FOs reduced TP EMG activity this would possibly be accompanied by increased PL EMG activity. However, TP and PL activity do not necessarily represent equal opposing inversion and eversion moments, respectively, due to additional muscle tendon parameters 60 and different moment arms.
Although FOs may increase amplitude and duration of PL activity during running,30,53 the literature is limited by low between-session reliability of PL EMG.61–63 Reported poor inter-session reliability of EMG data from PL reduces confidence in EMG results collected weeks apart.61–63 Amplitude of an EMG signal varies not only due to the detection of different motor units, but because of variable skin-electrode impedance between sessions. 64 Variability in amplitude between sessions could affect the ability to detect changes in duration of muscle activity due to FOs using threshold methods. As measurements were taken in separate sessions without mention of normalisation30,53 comparing EMG measures could be beyond this technique. In addition, electrode placement in one study 30 followed the methods of Winter and Yack 65 (50% of the distance between the fibular head and lateral malleolus, rather than 25% of the distance recommended by surface EMG for non-invasive assessment of muscles (SENIAM)). 22 A distal shift in surface electrode placement over PL of 2 cm increases the presence of crosstalk, likely from TA. 66 Given that PL is most active in mid-late stance, while TA is active prior to foot contact to enable a dorsiflexed ankle position at initial contact, potentially muscle activity reported as pre-activation of PL was actually crosstalk from TA.
Foot orthoses designed to reduce the external eversion moment at the subtalar joint would theoretically decrease the internal inversion moment required from the invertor muscles limiting eversion. The TA has an inversion moment arm when the foot is inverted, as at initial contact, 67 therefore FOs that reduce the eversion moment might also reduce TA activity. The conclusion of the review by Murley et al. 17 preceding the work of Telfer et al.13,18 that FOs may increase activation of the TA should be reconsidered. Studies that found FOs increase TA activity had notable limitations. As Murley et al. 17 identified, a significant increase in EMG activation was not always supported by confidence intervals. Many studies did not simultaneously collect kinematic and kinetic data, so we cannot relate any change (or lack of) in EMG to other changes in biomechanics, or evaluate the intervention in the context of the ‘preferred movement pathway’ theory. For example, an extrinsic medial rearfoot wedge could place the foot in a more plantar flexed position since the heel is lifted in the shoe, perhaps increasing demand on the TA in the sagittal plane after initial contact. 36 Without kinematic and kinetic data and with variable changes in EMG, the implications of this finding are limited. As TA is not the principal invertor of the foot and its main role is dorsiflexion, perhaps any effect is too small to detect, or too variable depending upon the action of the other invertor muscles (i.e. posterior leg muscles passing medial to the ankle) and foot position. Also, as the only ankle dorsiflexor, TA function is unlikely to be compromised with more alternative invertor muscles available. Overall, the majority of studies have found FOs do not change TA activity significantly, in some cases FOs may decrease TA activity, but any effect is subtle.
Literature limitations
TP is the largest invertor, but given fine-wire EMG can be challenging few studies have investigated its function, or intrinsic muscle activity. Furthermore, the magnitude of change in muscle activity that is clinically meaningful is unknown, thus significant effects of external devices on EMG does not reveal clinically beneficial effects. EMG is only a measure of electrical activity not force production, nor mechanical work in the muscle-tendon unit. In addition, differences in electrode types, signal processing, normalisation and outcome variables make establishing a consensus regarding the meaning of changes in EMG difficult. Guidelines describe methods of EMG processing, but are not a universal best practice. 24
Research investigating FOs used various materials and designs, and the descriptions of FOs were limited (no excluded study provided detail on this criteria). Studies used a mixture of customised and prefabricated FOs and both FOs with modifications only in the rearfoot and FOs with additional modifications in the arch and forefoot. Whether isolated modifications in specific FOs geometry could lead to specific changes in EMG is unclear. In addition several studies may have also been inadequately powered. A final observation is that studies generally focus on the immediate effect of external devices, yet muscle function could change over time. Longitudinal EMG studies are difficult, but other approaches such as muscle morphology have proven sensitive to footwear.68,69
Review limitations
While the quality assessment allowed the review to be based on studies of at least moderate quality, failing criteria could reflect inadequacy in reporting and not whether appropriate procedures were followed. 17 In addition, database searches from one reviewer and the score of 50% as a threshold for inclusion could be considered subjective. Furthermore, each criteria was given equal weighting when some could be more influential than others. For instance blinding might be unrealistic, as so-called sham FOs can exert mechanical effects 70 and potentially influence EMG. Conversely, lack of randomisation could invalidate results due to an order effect and be grounds for exclusion alone. Nonetheless, outcomes of the excluded studies were largely in agreement with those included, except one which found a significantly longer duration (p < 0.05) of TA activity following foot contact with FOs versus control. 71
Footwear outside the inclusion criteria could alter loading of the foot and subsequent muscle activity. However a general review of footwear would be far broader and by restricting our search to footwear that aims to alter foot/ankle motion with modifications in sole construction, findings can be more directly related to the other devices reviewed. This review focused on muscle activation, however devices could have other effects on soft tissue, like the capacity of the series elastic element of TP to absorb energy in early stance. 58
The review included studies with heterogeneous injury status and foot postures. The response to an intervention may vary with pathology. However the evidence that Achilles tendinopathy, for example, alters muscle activation is conflicting.72,73 Few of the studies included patient populations and those that did not provide healthy controls and foot posture was often not reported. Consequently sub-group comparisons were not possible.
Conclusion
Modifications in shoe or FOs design in the sagittal or frontal plane can alter activation in walking of muscles acting primarily in these planes. Adequately powered research with kinematic and kinetic data is needed to explain the presence/absence of changes in muscle activation with external devices.
Supplemental Material
Quality_assessment_supplementary_data – Supplemental material for A systematic review of the effect of footwear, foot orthoses and taping on lower limb muscle activity during walking and running
Supplemental material, Quality_assessment_supplementary_data for A systematic review of the effect of footwear, foot orthoses and taping on lower limb muscle activity during walking and running by Joanna Reeves, Richard Jones, Anmin Liu, Leah Bent, Emma Plater and Christopher Nester in Prosthetics and Orthotics International
Footnotes
Appendix
Excluded studies.
| Authors | Participant characteristics | Device | Muscles | Walking or running | Variables | Main findings | QA score (%), First stage; second stage |
|---|---|---|---|---|---|---|---|
| Excluded at first stage | |||||||
| Bourgit et al. 1 | 12 healthy females: 24 ± 4 years, 1.67 ± 0.06 m, 60 ± 7 kg | Standard fitness shoe (Reebok Revent Mid DMX, around 4° plantar flexion) and dorsiflexion shoes with a curvature plate in the midsole: Springboost B-Fit 2°dorsiflexion, Springboost B-Fit 4° dorsiflexion and Meridian 10° dorsiflexion | BF, Glut Max, MG, LG, TA, RF, SOL, VL, VM | Treadmill walking and running | RMS as %MVC and integrated EMG (iEMG) | • Significant increase in plantar flexor RMS EMG (average of MG, LG and SOL) with dorsiflexion shoes vs standard shoe in walking and running | 43; 54 |
| Branthwaite et al. 2 | Males and females, n = 15 (age = 25.2 ± 5.2 years; height = 1.68 ± 0.07 m; weight = 66 ± 10.6 kg) | Masai Barefoot Technology, participant’s own shoes as control | SOL, MG, LG, TA, PL, RF, BF and Glut Med | Walking (10 m walkway) | Mean, maximum EMG (mV) and percentage values (tip toe exercise presumably barefoot) | • No significant difference between conditions. Large inter-individual differences in muscle activity | 43; 54 |
| Demura and Demura 3 | 10 healthy males: 24.1 ± 4.1 years, 1.72 ± 0.05 m, 69.2 ± 8.4 kg | Stretch Walker (Nosaka, Ltd, Japan), Masai Barefoot Technology and flat-bottomed shoe | Glut Med, MG, LG, ST, SOL, TA, vastus tibialis? | Walking (laps of ~40 m walkway) | Integrated EMG | • No significant difference between conditions | 33; 54 |
| Gu et al. 4 | 22 healthy males: 23.5 ± 1.3 years, 1.73 ± 0.01 m, 66 ± 2.4 kg | Flat-soled control shoe, experimental shoe with adjustable hemispheres of 1.5 cm and diameter of 5.5 cm in the heel and forefoot (neutral, medial and lateral configuration) | BF, MG, LG, RF, TA, PL, VL, VM | Walking (10 m walkway) | RMS | • Increase in LG, PL and TA activity in experimental shoes vs control | 33; 54 |
| Ritchie et al. 5 | 21 males: 21 ± 4 years, 1.768 ± 0.05 m, 73.3 ± 6.5 kg | Prefabricated 3/4 length Formthotic (Foot Science International) | MG, PL, TA | Walking (15 m walkway) | Activation ratio with respect to control | • No significant differences | 43; 62 |
| Tomaro and Burdett 6 | 10 adults with history of leg pathology, treated with orthotics in last 6 months (3 M, 7 F, 25–30 years) | Prefabricated Sporthotic® (Langer Biomechanics, Deer Park, NY), own athletic shoes | LG, PL, TA | Treadmill walking | RMS amplitude, duration of activity | • Significantly (p < 0.05) longer duration of TA activity following heel strike with FO vs control • No significant difference in EMG amplitude between conditions for all muscles |
17; 46 |
| Excluded at second stage | |||||||
| Boergers 7 | University track team athletes (n = 8; 5 F, 3 M, 20 ± 1. 1 years) with self-reported anterior shin pain. | Traditional arch tape Perrin (1995), experimental arch tape (over dorsal rather than plantar surface) and presumably barefoot | TA | Walking and running | Peaks and means | • No significant difference between conditions | 71; 46 |
| Burke and Papuga 8 | 6 endurance-trained recreational runners (3 M, 3 F; 32.3 ± 10.07 years) | Flexible, custom-made UltraStep orthotics (Foot Levellers, Inc., Roanoke, VA) | BF, MG, TA, VL | Treadmill running | Peaks | • No significant difference between conditions | 57; 31 |
| Romkes et al. 9 | 12 healthy adults: 6 M, 6 F, 38.6 ± 13.2 years, 1.73 ± 0.06 m, 77.4 ± 12.3 kg | Masai Barefoot Technology and own shoe | MG, LG, RF, ST, TA, VL, VM | Walking | Amplitude as % of peak in barefoot | • TA activity decreased in early stance and increased in swing MBT vs control (p < 0.05) • MG and LG increased activity from late swing to mid-stance MBT vs control (p < 0.05) • VM and VL increased activity mid-stance to toe-off MBT vs control (p < 0.05) • RF increased activity in mid-stance and decreased activity in early swing MBT vs control (p < 0.05) |
86; 38 |
| Stöggl et al. 10 | 12 healthy students: 6 M, 6 F, 25 ± 2 years, 1.72 ± 0.07 m, 65 ± 9 kg | Masai Barefoot Technology and running shoe (Adidas SuperNova. Herzogenaurach, Germany), before and after 10-week training intervention | BF, MG, TA, PL, VL, VM | Treadmill walking | Variability (SD over 15 consecutive gait cycles) for: RMS, integrated EMG (iEMG) and median power frequency | • No difference between shoes and no change by training in EMG variability | 100; 44 |
BF: biceps femoris; MG: medial gastrocnemius; LG: lateral gastrocnemius; TA: tibialis anterior; RF: rectus femoris; SOL: soleus; VL: vastus lateralis; VM: vastus medialis; RMS: root mean square; MVS: maximum voluntary contraction; EMG: electromyography; PL: peroneus longus; Glut Med: gluteus medius; FO: foot orthosis; M: male; F: female; ST: semitendinosus; SD: standard deviation; MBT: Masai Barefoot Technology.
QA: quality assessment, second stage ((number of satisfied criteria/number of applicable criteria) × 100).
Acknowledgements
We wish to thank Dr. Henrike Greaves (Liverpool John Moores University) for her assistance in translating articles to English from German.
Author contributions
The review was conducted by JR. The preparation of the manuscript was supervised by CN. All authors were involved in the drafting and approving of the manuscript.
Declaration of conflicting interests
CN owns equity in Salfordinsole Healthcare Ltd. (Nuneaton, UK) that manufactures foot orthoses. Other authors have no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental Material is available online for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.