
Abstract
Background:
A medial meniscal tear is a common knee injury, especially following an anterior cruciate ligament injury. Decreasing the compressive force on the medial meniscus during dynamic activities using an unloader knee brace could reduce meniscal strain, effectively reducing injury risk and/or severity.
Objectives:
To investigate the efficacy of two unloader knee braces on medial meniscus strain during dynamic activities in intact & deficient anterior cruciate ligament states.
Study design:
Combined in vivo/in vitro study.
Methods:
In vivo knee kinematics and muscle force profiles from a healthy individual performing single/doubleleg squats and walking motions were simulated on 10 cadaveric specimens using a dynamic knee simulator system. Simulations were performed on knees in unbraced and braced scenarios, with and without the anterior cruciate ligament. Anterior and posterior medial meniscal strains were measured.
Results:
Two different braces each showed a significant reduction in the posteromedial meniscal strain (p ⩽ 0.01) in an intact anterior cruciate ligament state. Neither brace mirrored this result for the anteromedial strain (p > 0.05). In the deficient anterior cruciate ligament state, the braces had no significant effect on strain (p > 0.05).
Conclusion:
Two unloader knee braces effectively reduced strain in the medial meniscus with an intact anterior cruciate ligament during dynamic activities. Neither brace made a significant reduction in strain for anterior cruciate ligament-deficient knees.
Clinical relevance
Unloader knee braces could be used to reduce the medial meniscus strain following meniscal surgery and during rehabilitation in patients with an isolated medial meniscus injury. However, these braces cannot be recommended for this purpose in patients with an anterior cruciate ligament deficiency.
Background
The knee’s lateral and medial menisci improve stability and articulation within the femorotibial joint, aid in shock absorption, distribute compressive axial loads applied by the femur and provide joint lubrication and proprioception. 1 Meniscus injuries are common sports- and non-sports-related knee injuries, second only to anterior cruciate ligament (ACL) injuries. Furthermore, these injuries have an incidence of 60–70 per 100,000 patients affecting young, active individuals and can occur in isolation or in tandem with other injuries such as ACL tears.2–4 Studies have shown the medial meniscus is affected more than the lateral due to differences in meniscal anatomy and articular geometry.5,6
An ACL deficiency causes four times the typical amount of anterior tibial translation (ATT) and consequently places additional demands on the medial meniscus to act as the knee’s primary stabilizer in the anterior–posterior, internal–external and varus–valgus directions.7,8 Allen et al. 9 have shown this increased demand causes higher resultant forces and strains on the medial meniscus and this increased strain over a prolonged period may lead to subsequent meniscal injury and altered joint contact mechanics. 10 A torn medial meniscus cannot effectively distribute joint compressive forces within the compartment, and the increased load and displacement experienced by the meniscus elevates the risk of medial osteoarthritis. 11
Currently, only certain types of meniscal tears are amenable to repair. 12 Most successful surgeries require a 4-month recovery period, where the tissue needs to be protected from further damage and non-operative methods are often limited to exercise regiments, physical therapy and/or weight loss. 13
Unloader braces are a rehabilitation option prescribed to patients with unicompartmental osteoarthritis. They are intended to apply an external unloading moment to reduce stress on the affected joint. 14 With medial osteoarthritis, the applied valgus moment is meant to unload the medial compartment and provide pain relief. While these braces have shown positive effects in clinical trials regarding pain,15,16 their effect on the medial meniscal strain remains unclear. Kutzner et al. 17 showed in vivo reductions in medial compartmental joint loads with two valgus (unloader) braces during gait and stair climbing activities, although no strain measurements were made. By unloading the medial compartment, it is possible the meniscal strain may also decrease. Thus, it is important to understand the effect of these braces on strain, since unloader braces could effectively reduce the risk of a meniscus injury in patients with an ACL deficiency and in those undergoing rehabilitation following meniscal surgery, with or without an ACL.
Studies, such as Seitz et al., 18 measured meniscal strain and joint pressure under a partial meniscectomy condition on 10 cadaver knees at various knee angles. Similarly, Jones et al. 19 measured in vitro medial meniscus strain by applying a compressive load to the knee joint at full extension and 30° flexion in intact and torn meniscal scenarios. In both studies, the ACL was left intact and a brace was not considered. Hollis et al. 20 is a rare example of meniscal strain measurement considering an ACL-intact versus ACL-deficient states. The authors showed an increase in strain when the ACL was transected. However, only a single loading condition was considered and braces were not studied.
Muscle forces and ligament health play an important role in joint stability and equilibrium. 21 An injury to the ACL can lead to alterations in the biomechanical properties and behaviours of structures surrounding the injury site. 22 Thus, muscle force patterns are highly relevant when simulating dynamic knee activities, especially in an injured ACL state. Presently, studies on meniscal strain have not considered dynamic loading scenarios, muscle force patterns or ACL health on the effect of unloader knee braces. This study investigates the effect of two commercially available unloader knee braces on medial meniscal strain during typical rehabilitation activities, with dynamic loading conditions, in an ACL-intact and ACL-deficient state. The rebound cartilage (RC) and unloader fit (UF) braces (Ossur Canada, Richmond, BC, Canada) have three-point leverage designs intended to apply a valgus moment to unload the medial joint. The RC brace is designed to apply a larger valgus moment than the UF brace. A combined in vivo, in silico and in vitro dynamic approach developed by previous works23–26 is used in this study to investigate three activities of typical daily living including a two-legged squat (2LS), one-legged squat (1LS) and walk (WLK). This study hypothesizes the following: i. Unloader knee braces decrease the strain in the medial meniscus during dynamic activities. ii. The RC brace produces lower meniscal strain values than the UF brace.
Methodology
This research has been approved by the office of research ethics at the University of Waterloo, ensuring standard and ethical principles of research. Written informed consent for participation and publication has been obtained. In vivo motion capture using the Optotrack motion tracking system (Northern Digital Inc., Waterloo, ON, Canada) was performed on a healthy 28-year-old female participant performing 2LS, WLK and 1LS activities. The participant was instructed to perform the activities at a natural pace, resulting in a walking speed of 1.9 steps/s and a 2LS and 1LS with maximum flexion angles of 83° and 81° in 1.8 s, respectively. 26 Walking is a necessary mobility function of any healthy individual; whereas, 2LS and 1LS are early and late injury rehabilitation exercises in most recovery programmes. 27 A total of 36 body markers were placed on anatomical landmarks in regions including the thorax, pelvis, upper leg, lower leg and feet. Four cameras recorded the marker trajectories while the subject performed the aforementioned activities, at a sampling frequency of 64 Hz. Force plates (AMTI, model OR6-7-2000, Watertown, MA, USA) collected ground reaction forces and moments at a sampling rate of 2048 Hz. The obtained joint kinematic results were comparable to a typical gait pattern.28,29
The marker and ground reaction force data were input into rigid body modelling software OpenSim (Stanford University, Stanford, CA, USA). 30 The collected kinetic and kinematic data were used to create a musculoskeletal lower extremity Gait2392 model (23 degrees of freedom and 92 muscle groups). This model has previously been used to simulate walking, running and single-leg jump landings.25,31–34 Moreover, the muscle activation patterns in this study for the walking trial are similar to validated OpenSim gait simulations using electromyography (EMG). 32 Following inverse kinematics and dynamics, the Residual Reduction Algorithm and Computed Muscle Control were used to calculate muscle forces for each activity.30,35
Ten fresh-frozen unpaired cadaver knees (5 male and 5 female, age: 49.7 ± 8.4 years and body mass index (BMI): 21.5 ± 6.0) were procured from a body donor program and were prepared for experimental testing based on previously developed methodologies.24–26 Initially, a negative mould of the frozen knee was prepared. The knees were thawed and subsequently the skin, subcutaneous tissue and muscle bodies were dissected leaving all ligaments and major muscle tendons intact. Three steel cables were secured at the tendon insertion sites of the quadriceps, hamstring and gastrocnemius muscle groups. Finally, the specimen was placed in the empty mould of the knee created prior to dissection. A liquid foam solution (Sunmate, Dynamic Systems Inc., Leicester, NC, USA) was poured into the mould such that the dissected knee was protected in a foam case. The solidified foam had a medium-firm compressive stiffness of 17.6 N/mm similar to the average stiffness of contracted muscle. 24
The prepared specimen was mounted on the dynamic knee simulator system. 23 Two microminiature displacement sensors (DVRT, MicroStrain, Inc., Burlington, VT, USA) were placed on the posterior medial meniscus (PMM) and anterior medial meniscus (AMM), with the PMM sensor shown in Figure 1. It is essential to note that the sensor was carefully placed and monitored throughout the trial to avoid interference with the brace.
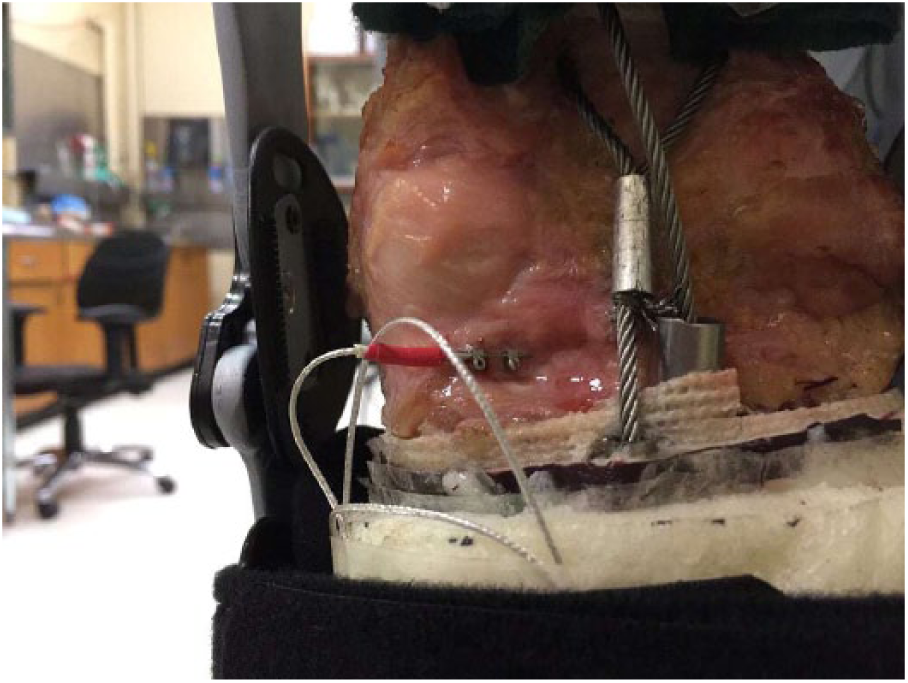
Typical location of the DVRT sensor on the posteromedial medial meniscus in a braced setup.
Time-varying kinematics and muscle forces derived from OpenSim for each of the three activities (2LS, WLK and 1LS) were applied to each specimen in real time. Each activity was repeated in an unbraced (NB) and with the two braces (RC and UF) mounted on the knee, in an ACL-intact state. Subsequently, the ACL was transected using a scalpel, and the trials were repeated. Each activity-brace-ACL combination was tested twice, resulting in a total of 36 trials/specimen, and the average of two trials was used in the data analysis. Figure 2 shows the experimental setup in the WLK stance.
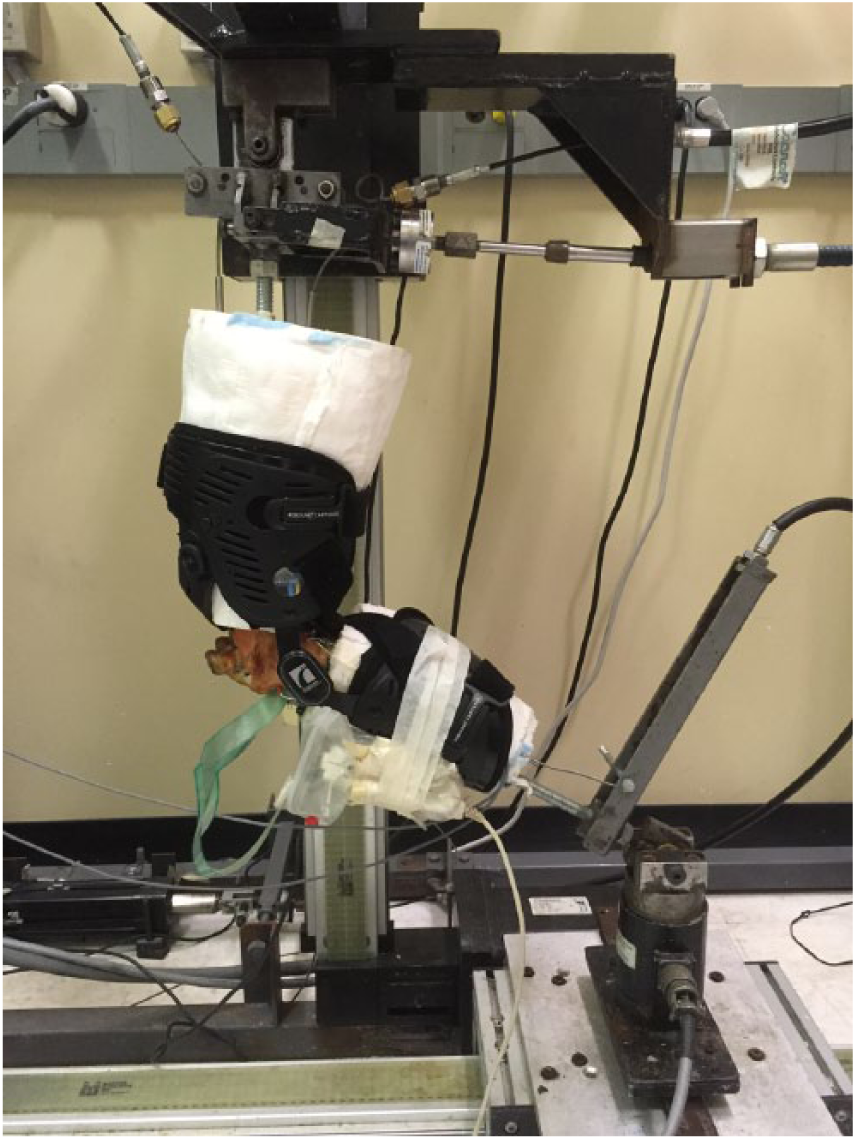
Experimental setup of a right leg in the walk position (mid-swing) for a cadaver mounted with the rebound cartilage (RC) brace.
Meniscal strain values were calculated using the engineering strain formulation with the reference considered as the DVRT length at the initial time point in the NB condition for each activity. Average and peak meniscal strain values were calculated for each simulation. A repeated measures analysis of variance (ANOVA) and a post hoc t-test with a Bonferroni family-wise correction factor (alpha criterion of 0.05) were performed to determine the effect of each brace and their interactions with ACL status (brace*ACL) and activity (brace*Activity). The interaction between all three variables was not considered, as explained in section ‘Results’. To address the second portion of the hypothesis (the strain comparison between the RC and UF braces), an additional ANOVA analysis was done without the NB case.
Results
PMM strain was collected for every specimen while AMM strain was not collected for three specimens due to difficulties with sensor placement on the tissue and sensor interference with the brace. Table 1 shows the mean peak and average PMM strains for all tested specimens, while Table 2 shows the mean peak and average AMM strains. Figures 3 and 4 show the mean strain in the PMM and AMM, respectively, for the NB, RC and UF brace scenarios, in the ACL-intact (Int) and ACL-deficient (Def) states for all three activities.
Mean posterior MM strain ± SD displaying peak and average values for each activity, bracing condition and ACL state (n=10).
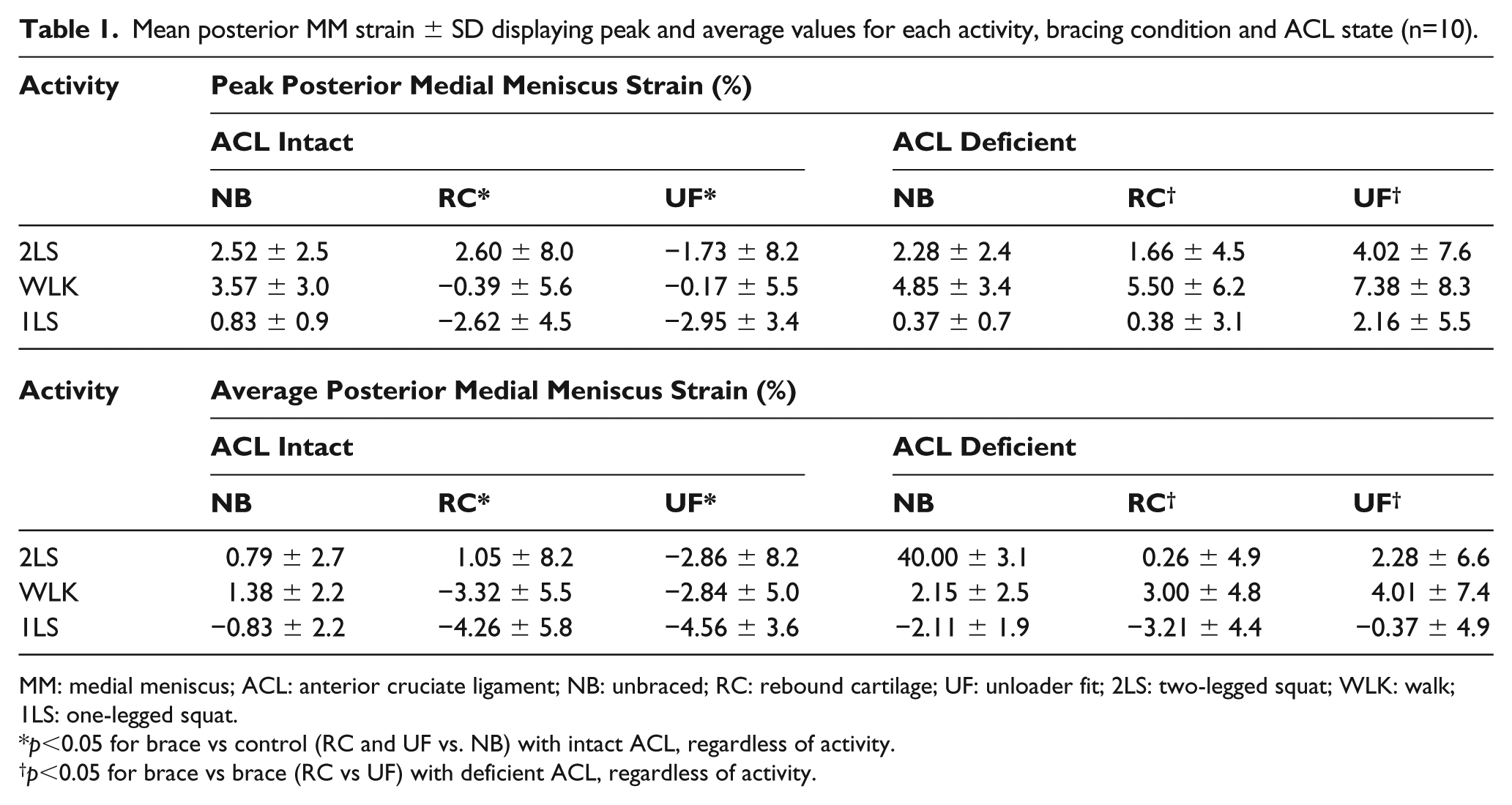
MM: medial meniscus; ACL: anterior cruciate ligament; NB: unbraced; RC: rebound cartilage; UF: unloader fit; 2LS: two-legged squat; WLK: walk; 1LS: one-legged squat.
p<0.05 for brace vs control (RC and UF vs. NB) with intact ACL, regardless of activity.
p<0.05 for brace vs brace (RC vs UF) with deficient ACL, regardless of activity.
Mean anterior MM strain ± SD displaying peak and average values for each activity, bracing condition and ACL state (n=7).
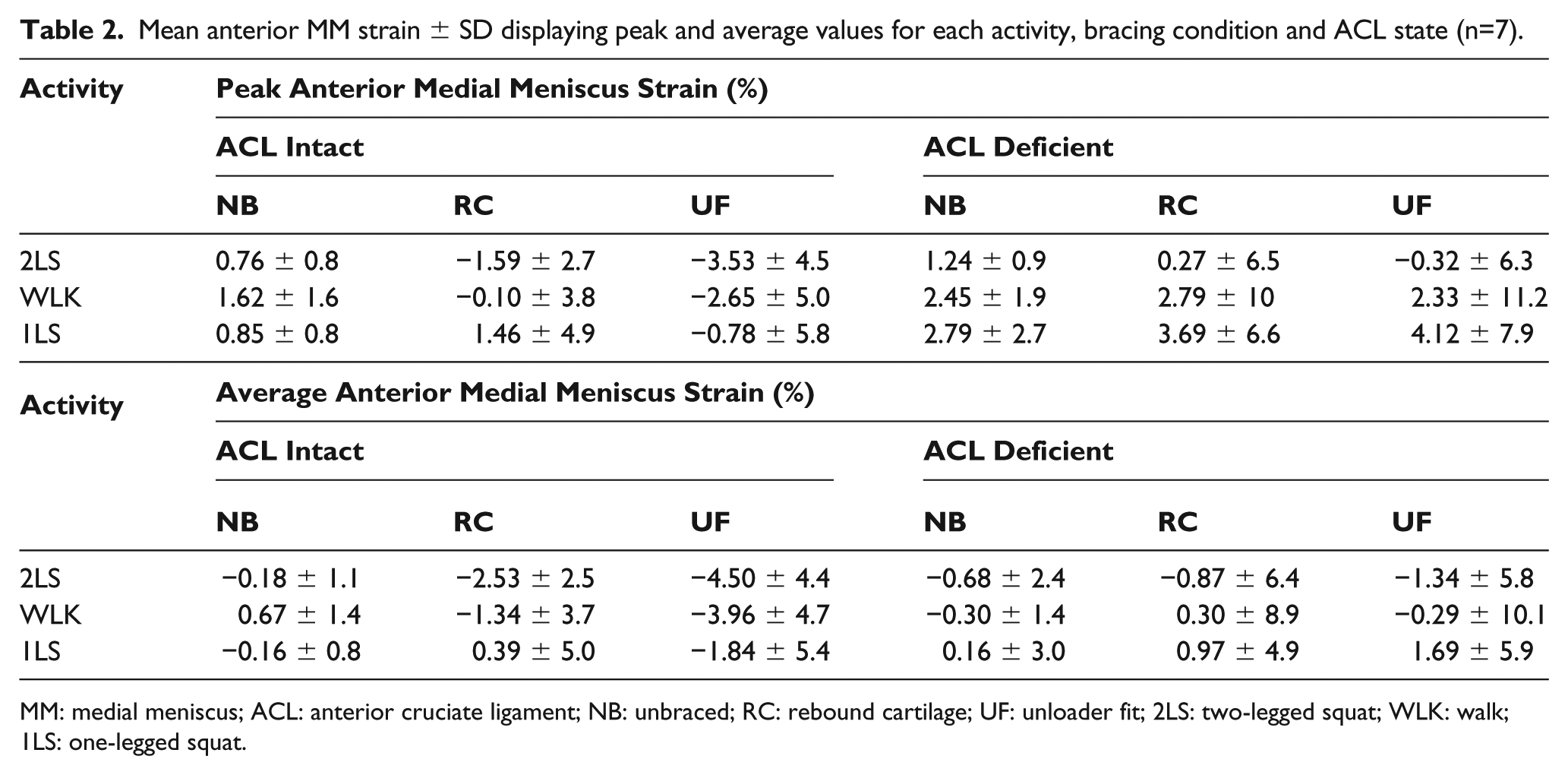
MM: medial meniscus; ACL: anterior cruciate ligament; NB: unbraced; RC: rebound cartilage; UF: unloader fit; 2LS: two-legged squat; WLK: walk; 1LS: one-legged squat.
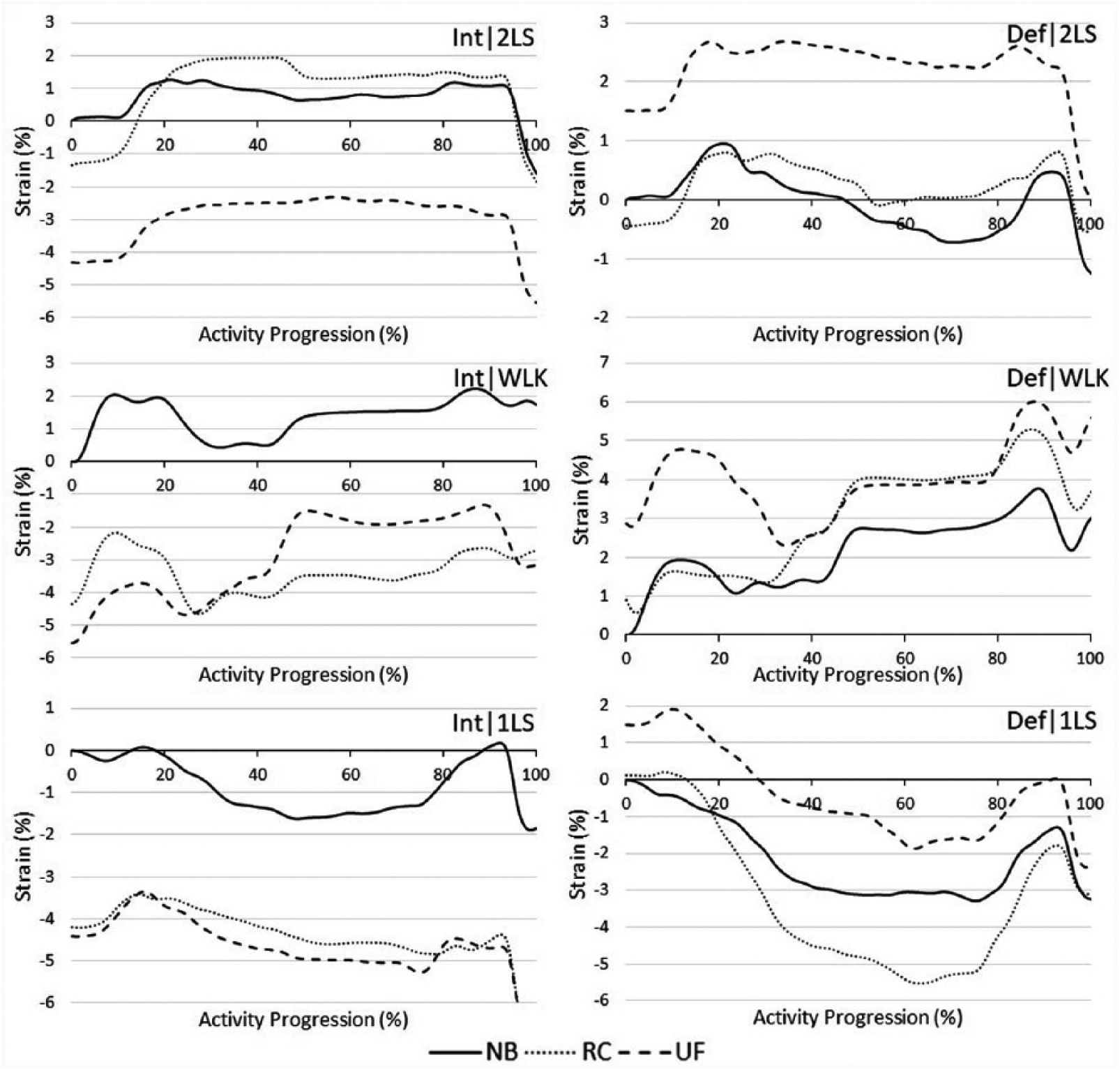
Average posterior medial meniscus strain (n = 10) for ACL-intact and ACL-deficient conditions (Int, Def) in two-legged squat (2LS), walking and one-legged squat (1LS) trials.
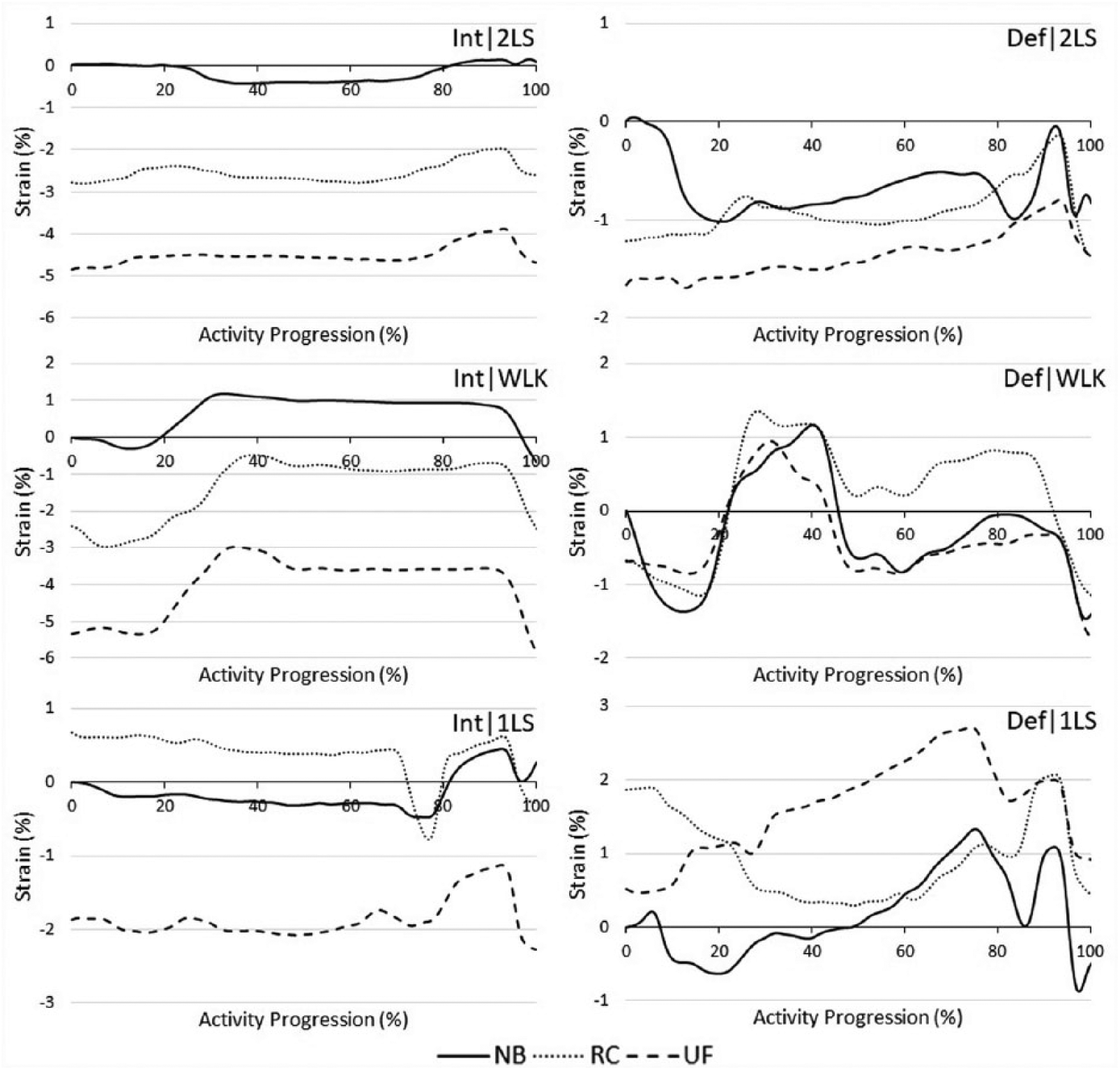
Average anterior medial meniscus strain (n = 7) for ACL-intact and ACL-deficient conditions (Int, Def) in double-leg squat (2LS), walking and single-leg squat (1LS) trials.
The ANOVA results showed significant interactions in certain situations regarding brace*ACL results; whereas, the brace*Activity interaction was insignificant (p > 0.05) in all situations. The brace*ACL*Activity interactions were disregarded since none of the activities showed a significance with the brace. The ANOVA revealed the UF brace had a significant interaction (vs NB control) with ACL status (p < 0.05) in case of peak and average PMM strain. The Bonferroni Post-hoc test showed that the RC and UF braces significantly reduced peak and average PMM strain in the ACL-intact state (p ⩽ 0.01) but not in the ACL-deficient state (p > 0.05), when compared to the NB control case. In case of AMM, neither brace had a significant interaction (vs NB control) with ACL status (p > 0.05). The ANOVA results between braces showed a significant interaction (p < 0.05) for brace*ACL regarding peak and average PMM strains. However, the Post-hoc analysis showed a significant difference between the RC and UF braces only in the ACL-def state (p < 0.05). The AMM strain comparison between the braces was insignificant (p > 0.05) for all interactions.
Discussion
While meniscal strain values have been reported in the literature before, no studies have reported strains during dynamic activities. Furthermore, this is believed to be the first study that investigates the effect of unloader knee braces on meniscal strain. The results clearly show that unloader knee braces reduce the meniscal strain in ACL-intact knees. However, when the ACL is transected, the braces show no effect on the meniscal strain, which could be a plausible cause of increased ATT and instability in the knee.
Posteromedial meniscal strain is regarded as an important measurement parameter since medial meniscus tears in the posterior horn are common and meniscal damage is directly correlated with strain. 36 Thompson et al. 37 stated the medial meniscus translates less than the lateral during flexion; however, since the posterior horn of the medial meniscus has the smallest area (of the four attachment sites) it is the most prone to injury. Few studies have measured the strain in the AMM or commented on its significance. Seitz et al. 18 reported peak hoop strains in the posteromedial and anteromedial meniscus horns of 2.4% and 1.4%, respectively, when 500 N were statically applied in 0° flexion. Kolaczek et al. 38 reported strain values of 3.8% in the posterior meniscus when a compressive load of 1 × Bodyweight was applied at 5° flexion. While the loading conditions from the previous literature were different, the NB results reported in the current study (PMM: 2.6%, AMM: 0.6%) fall within a similar range. Hollis et al. 20 reported posteromedial meniscus strain values of approximately 1.5%–3% (ACL-intact) and 2%–3.5% (ACL-deficient) depending on flexion angle and applied load. This study also shows similar NB strain values of less than 5% for both ACL states. The high degree of variability in the measured meniscal strain in this study is consistent with previous studies.18,38
In Figures 3 and 4, the beginning of each NB trial is set as the reference length of the tissue; thus, positive or negative strains relative to this point are seen as higher or lower, respectively. For example, in Figure 3 (Int, 2LS), the initial strain reading for the NB is 0% strain, while the UF and RC have initial readings of −4.3% and −1.3%, respectively. This negative strain does not indicate the tissue is being compressed, rather it indicates the tissue is under relatively lower tension in comparison to the reference NB scenario.
A visual comparison of the PMM strains in the ACL-intact state (Figure 3), the NB-2LS, NB-WLK and NB-1LS results show higher average strains compared with both (RC and UF) braces, with the exception of the RC-2LS condition. The AMM (Figure 4) shows lower strains for the ACL-intact state for the 2LS and WLK, with both braces. However, the 1LS data do not follow the same pattern. Generally, the braces show lower intact strain values versus the NB scenario and similar or higher strains in the deficient state than the intact, irrespective of the bracing scenario.
Both braces have a positive effect on PMM strain (p < 0.05) with an intact ACL, since a lower strain means a decreased likelihood of meniscal injury. The insignificance (p > 0.05) of the braces in the ACL-deficient state possibly shows the increased instability in the knee is too great for these braces to overcome, since they are not designed to overcome antero-posterior instability. The comparison between ACL states is deemed more pertinent than the differences between the activities performed, since braces are expected to provide the same quality of treatment irrespective of activity performed and it would be counterintuitive to require a patient to use a different brace to alleviate symptoms while walking versus squatting. Moreover, neither brace had a significant interaction with activity (p > 0.05) indicating favourable brace designs.
AMM strain was measured as an additional metric to PMM strain to observe whether strain effects would be consistent among various sections of the tissue. Figure 4 shows a decrease in AMM strain with both braces for 2LS, WLK and 1LS (UF only) with an intact ACL, although these results were not significant. The ANOVA results do not indicate any significance (p > 0.05) for the AMM in any ACL or brace combination. The relevance of the anterior meniscal strain needs to be explored further and perhaps include greater than seven samples to form any substantial conclusions with statistically significant results.
The relationship between meniscal strain and the amount of unloading moment is presently unexplored and this study tested two distinct unloader braces intended to apply different unloading moments. The unloading moment was not quantified; however, according to the manufacturer, the RC brace is more supportive, designed to tighten at a larger flexion angle and capable of generating a larger moment arm about the knee centre than the UF brace. Thus, the RC brace was expected to provide a larger unloading moment and produce lower strain values. This outcome is visually apparent considering the PMM strain in the ACL-deficient state (Figure 3). Furthermore, the RC brace showed significantly lower mean PMM strains than the UF brace (p < 0.05), for peak (RC: 2.5% vs UF: 4.5%) and average (RC: 0.04% vs UF: 2.0%) PMM results. Contrary to expectation, the ACL-intact PMM strain and AMM strains with either ACL states do not show a significant difference (p > 0.05) between the braces. A plausible conclusion is the RC brace does produce lower mean strains than UF strain on the posterior meniscus; yet, this difference was especially significant post-ACL transection when the knee requires greater stability and unloading from an external source.
This study has several limitations. The simulator was limited to sagittal plane motions; thus, any forces in the coronal or transverse planes were not represented. The in vivo force data were retrieved from multiple participants; however, the data from one (uninjured) participant was used for the following reasons. The average in vivo data from multiple participants was highly variable, and the results from the selected participant showed better kinematics compared to the typical population, when validated against multiple sources. Moreover, testing multiple force profiles from different participants would likely exceed the testing limits of the cadaver. For similar reasons, it was not possible within the constraints of this study to capture kinematic muscle force patterns from an additional ACL-deficient participant; thus, the ACL-deficient participants may have a different response with the braces. The cadaver setup used only one compliance value for the foam; whereas, realistically compliance varies based on sex, activity level, muscle activation, age and BMI. A live participant may have a slightly modified interaction with the brace due to various muscle stiffnesses. Furthermore, as with most cadaver studies, the sample size is relatively small and, as a result, the statistical power in cases lacking significance is low. Finally, there exists inter-subject variability with DVRT sensor placement which can affect the results. Careful consideration was taken to dissect and/or suture soft tissues adjacent to the medial meniscus, as well as not disturb the DVRTs when applying the braces. A close-up video recording of the meniscus during the trial was captured to observe for any impingement, during all flexion angles and brace conditions. In spite of these limitations, this study contributes valuable insights on the effect of unloader braces on meniscal strain.
Conclusion
This study presents the effect of two commercially available unloader braces on medial meniscal strain during different dynamic activities and ACL states. The braces decrease posteromedial meniscal strain during the braced conditions in ACL-intact knees. The reduced strain shows the RC and UF braces benefit the medial meniscus during rehabilitation or post-surgical meniscal repair. Moreover, the RC outperformed the UF in ACL-deficient knees. However, since these braces are only effective in the ACL-intact state, presently, they can only be recommended to patients with isolated meniscal tears.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: Micah Nicholls is employed by Ossur Inc., the brace provider. The authors verify that no other conflicts of interest exist.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was funded, in part, by Ossur Canada and Natural Sciences and Engineering Research Council of Canada.