
Abstract
Background and aim:
Longer residual limb lengths provide an increased lever arm. Longer residual limbs may produce increased joint moments; the two may be correlated. These correlations have not been evaluated in transfemoral amputees during transitional movements. Correlations between residual limb length and involved side joint moment could contribute to justification supporting maximal residual limb length preservation. This study investigated possible correlations between hip or knee moment and residual limb length.
Technique:
Hip and knee joint moments were determined while 21 transfemoral amputees performed sitting and standing movements and then evaluated for correlation with residual limb length.
Discussion:
Residual limb length was not correlated with either knee or involved side hip moments during sit to stand or stand to sit. Conversely, weak inverse correlations (p < 0.05) existed between sound hip moment magnitude and residual limb length. These correlations suggest that in community ambulating transfemoral amputees, longer residual limb length could decrease sound hip kinetic burden during transitional movement. Beyond correlations between residual limb length and sound hip transitional movement kinetics, there are other considerations in determining residual limb length during amputation.
Clinical relevance
This study examines relationships between lower limb joint moments and residual limb length related to sit-to-stand and stand-to-sit activities. The results have implications for amputation surgery and rehabilitation.
Background and aim
In transfemoral amputees (TFAs), movement is complicated for many reasons including asymmetry in the direction and magnitude of forces, selected motor control strategies, and residual limb length (RLL). This is true in stressful transitional movements such as sit to stand and stand to sit. 1 Fundamental biomechanical analyses indicate that longer RLLs increase the length of the lever arm producing joint moments; 2 therefore, correlations may exist between RLL and involved side lower limb joint moments.
Presently, no empirical tests have determined whether correlations exist between RLL and prosthetic side hip or knee moments during transitional movements in TFAs. Such correlations could support justification of preserving maximal RLL at the point of amputation, if circumstances permit. Therefore, this project sought to determine whether correlations exist between hip or knee moment of either side and RLL during sit to stand and stand to sit. Specifically, we hypothesized involved side joint moments would be increased with longer residual limbs.
Technique
Subjects
The University of South Florida Institutional Review Board approved the protocol. A total of 21 TFA subjects provided informed consent. Subjects’ prosthetic knees, feet, and suspension mechanisms varied (Table 1). Eligibility criteria are summarized in Table 1.
Amputee subject demographic data and inclusion criteria.
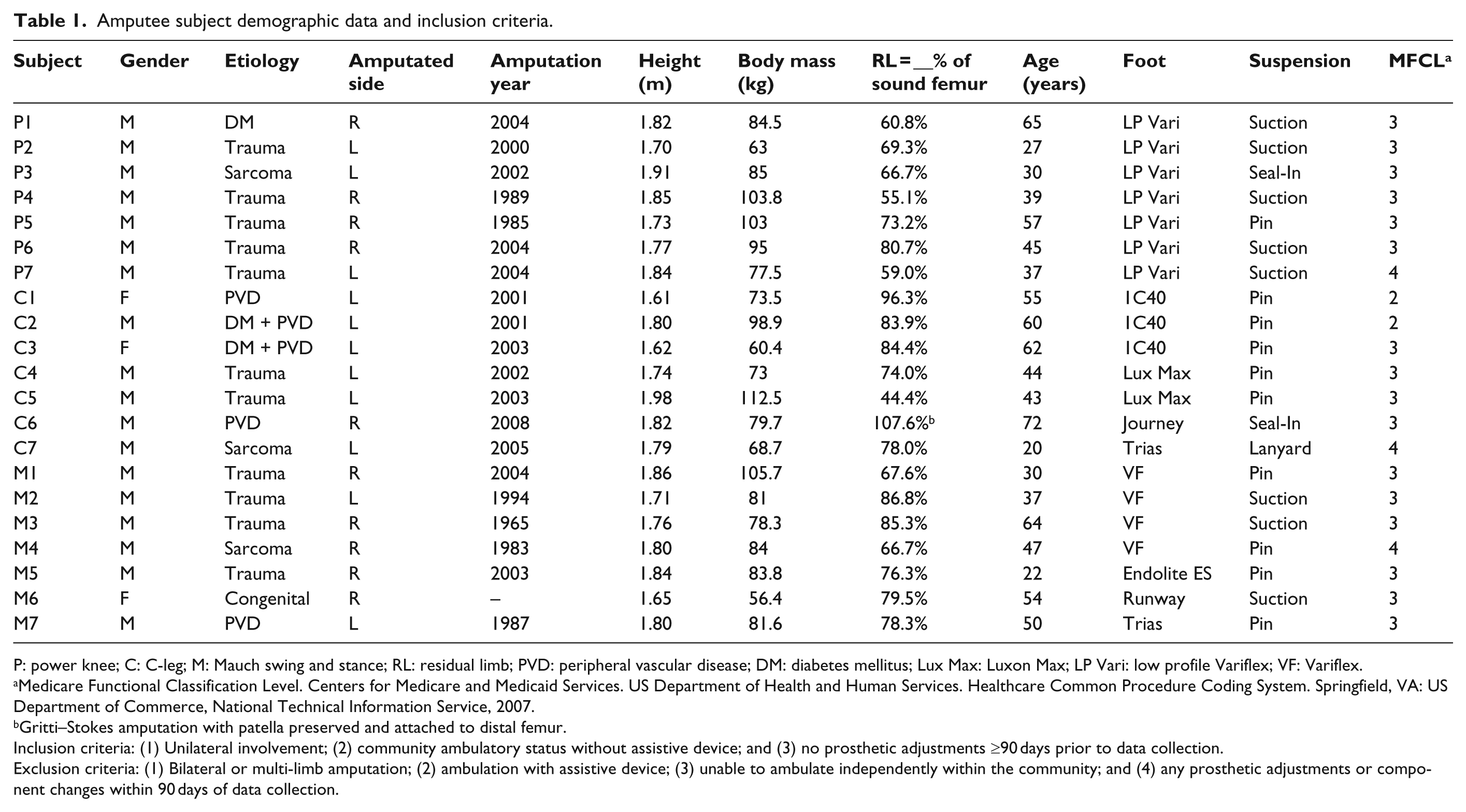
P: power knee; C: C-leg; M: Mauch swing and stance; RL: residual limb; PVD: peripheral vascular disease; DM: diabetes mellitus; Lux Max: Luxon Max; LP Vari: low profile Variflex; VF: Variflex.
Medicare Functional Classification Level. Centers for Medicare and Medicaid Services. US Department of Health and Human Services. Healthcare Common Procedure Coding System. Springfield, VA: US Department of Commerce, National Technical Information Service, 2007.
Gritti–Stokes amputation with patella preserved and attached to distal femur.
Inclusion criteria: (1) Unilateral involvement; (2) community ambulatory status without assistive device; and (3) no prosthetic adjustments ≥90 days prior to data collection.
Exclusion criteria: (1) Bilateral or multi-limb amputation; (2) ambulation with assistive device; (3) unable to ambulate independently within the community; and (4) any prosthetic adjustments or component changes within 90 days of data collection.
Testing protocol
Detailed procedures and data from the kinetic asymmetry analyses are reported elsewhere. 1 An eight-camera Vicon (Oxford, UK ) motion analysis system and two AMTI (Watertown, MA, USA) multi-axis force plates were used for data collection. Reflective markers (12 mm) were affixed to subjects’ trunks and extremities. Prior to motion analysis, anthropometric measurements were collected. 1 Manufacturer-recommended techniques were used to calibrate the motion analysis system prior to each subject’s data collection. The average of three trials per task was used to decrease variance.
Research design and analytical procedures
A cross-sectional design was used. Observational motion analysis measurements were obtained for sit-to-stand and stand-to-sit tasks and then correlated with subjects’ anthropometric values. Subjects stood up from and sat down on a platform individually adjusted to a 90 ±5° knee flexion angle and performed three repetitions of each task. Subjects were asked not to use hands to assist and to place and maintain each foot on a force plate the entire time to record each foot’s respective ground reaction force (GRF). The calculated point of maximum vertical acceleration of the body’s center of gravity was used as a data extraction point. 1 The GRFs and hip and knee moments were measured and/or calculated at the extraction point and referred to as peak values. Peak values extracted for previous kinetic asymmetry analyses 1 were utilized for the present correlation analysis.
In this analysis, RLLs (% of sound femur: hand measure distance from ischial tuberosity to the end of the residual limb with distal soft tissue compressed) were evaluated for correlation with sagittal hip and knee moments (normalized to body mass and height (N/kg)). In the sagittal plane, hip and knee movements occur in opposite directions (i.e. vectors) in order to stand up and/or sit down. Therefore, positive values for joint moments indicate an internal extension moment, whereas negative values indicate an internal flexion moment.
Statistical analysis
Statistical analysis software (SPSS. IBM. Armonk, NY, USA) was used to calculate correlations. Pearson product–moment correlation was used to determine strength of relationships during sit to stand and stand to sit.
Definitions for correlation values between 0 (not correlated) and ±1.0 (perfectly correlated) vary. For example, Kubiszyn and Borich 3 identify a correlation of ±0.85 as strong, ±0.42 as moderate, and ±0.22 as weak. Furthermore, what may be considered strong for one data set may be weak for another. Zou et al. 4 identified correlations of ±0.80 as strong, ±0.50 as moderate, and ±0.20 as weak. We considered correlations of 0 to ±0.49 as weak, ±0.50 to 0.79 as moderate, and ±0.80 to 1.00 as strong. Statistical significance was set at p ≤ 0.05.
Results
Correlations observed during sit to stand and stand to sit between RLL and prosthetic side knee and hip moments were weak at r = −0.10 and −0.14 (Figure 1(a) and (b); p > 0.05) and r = −0.15 and −0.15 (Figure 1(c) and (d); p > 0.05), respectively. Similarly, correlations observed during sit to stand and stand to sit between RLL and sound side knee moments were also weak at r = −0.07 and −0.19, respectively (Figure 2(a) and (c)). Correlations observed during sit to stand and stand to sit between RLL and sound side hip moments were also weak at r = −0.45 and −0.47; however, both were statistically significant (p < 0.05; Figure 2(b) and (d)).
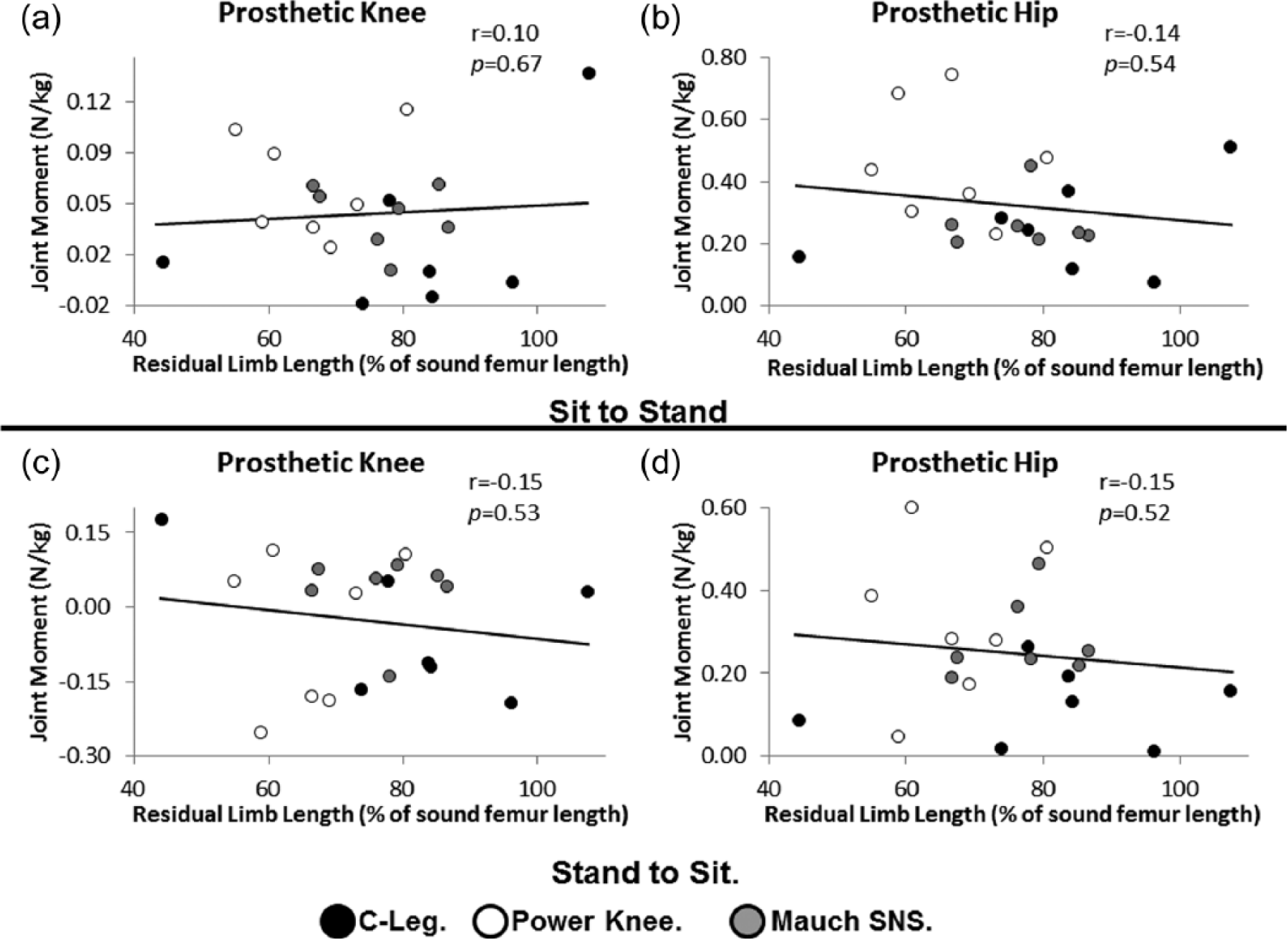
Correlations between joint moments (y-axis; normalized to body mass and height: N/kg) and residual limb length (x-axis; % of sound femur length): (a) prosthetic knee moment: sit to stand, (b) prosthetic hip moment: sit to stand, (c) prosthetic knee moment: stand to sit, and (d) prosthetic hip moment: stand to sit.
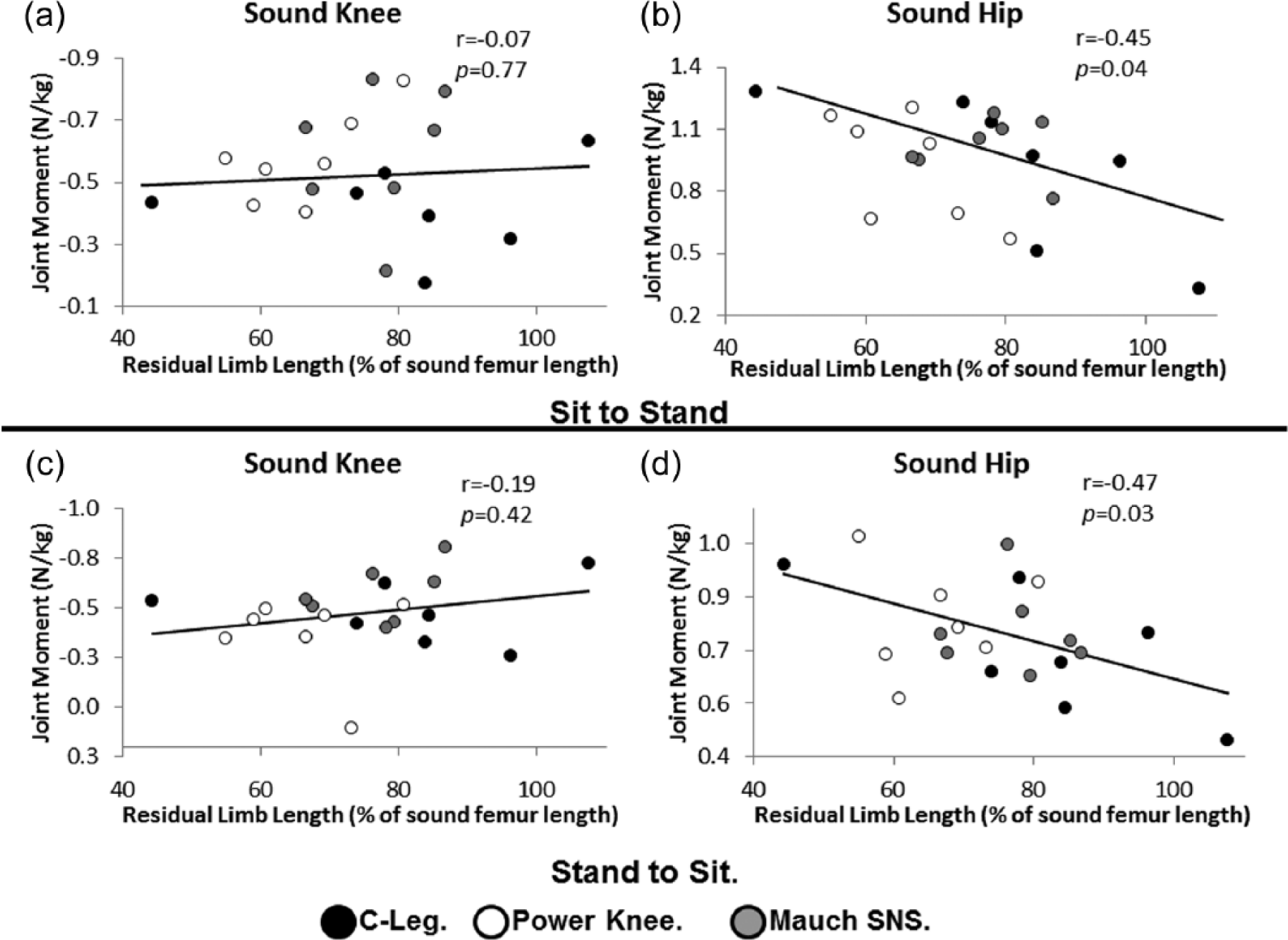
Correlations between joint moments (y-axis; normalized to body mass and height: N/kg) and residual limb length (x-axis; % of sound femur length): (a) sound knee moment: sit to stand, (b) sound hip moment: sit to stand, (c) sound knee moment: stand to sit, and (d) sound hip moment: stand to sit.
Discussion
Bioenergetic studies suggest that longer RLL may increase gait efficiency. 5 Based on this and fundamental biomechanical principles, 2 we hypothesized during transitional movements, increased RLL and prosthetic side joint moments would be correlated. This hypothesis was not supported, as prosthetic side joint moments and RLL were not significantly correlated. Baum et al. 6 similarly found no correlation between transfemoral limb length and spatiotemporal or biomechanical gait parameters. Collectively, these findings could be interpreted to mean there is little relationship between positive functional outcomes and RLL relative to the involved side. Furthermore, involved side knee moments tended to be near zero or at times oppositely oriented relative to the sound knee moment suggesting the prosthetic knees contributed little to the transitional movements. In some instances, prosthetic side joint moments seemed to resist the intended movement. Although sound side knee moment magnitudes were nearly an order of magnitude larger than those of the involved side (Figures 1(a) vs 2(a) and 1(c) vs 2(c)), correlations were similarly weak between RLL and the sound knee. Conversely, these data demonstrate that the sound side hip may benefit from a longer RLL in that those with shorter RLL utilized greater sound side hip moment during sitting and standing tasks. Said differently, those with longer RLL completed sitting and standing tasks while depending less upon the sound hip suggesting other joints may contribute more moment to these motions.
The extent to which RLL influences function remains unclear. Waters et al. 5 reported gait bioenergetics between differing amputation levels (i.e. transtibial, transfemoral) as opposed to different RLLs within a single amputation level (i.e. short vs long transfemoral). Their findings suggest those with longer residual limbs ambulate more efficiently. However, clinical decision-making regarding RLL would be further informed with a gait bioenergetic study evaluating the effect of RLL within a single amputation level. In the more recent study 6 correlating RLL and gait parameters, while limb length was within the TFA level, mean time from amputation was <1 year (range 0.3–2.7 year). 6 Evaluating gait quality <1 year post amputation likely results in the observation of amputees still developing a motor control strategy for their gait. This likely confounds the effect of RLL on gait efficiency and biomechanics with the effect of motor learning on gait quality. Similar confounding could occur if a sample of subjects with recent TFA were observed completing tasks of functional strength such as sit to stand and stand to sit. Such confounding can be ruled out given this study’s participants were farther from the time of amputation (11.2 ±10.5 years).
Other forms of sample heterogeneity also influence functional performance. For instance, our results may be confounded by differences in subjects’ physical functional capacity since 6 of 21 (29%) were elderly with comorbid vascular and/or metabolic disease. Another consideration is that subjects were not strength-tested. This study only considered relationships between RLL and joint moment in a task requiring functional strength and weak correlations were observed. However, an isometric dynamometry test could show stronger relationships between RLL and strength at other joints beyond the sound side hip in a sample of TFAs of homogeneous etiology.
This study demonstrates that RLL and sound side hip moments are weakly but significantly related (inversely) during sitting down and standing up. Implications are that those with longer RLL may use less sound hip moment while rising from and returning to sitting; however, other potential benefits warrant consideration. These may include increased surface area for load distribution,7,8 proprioception, and prosthetic control. 9 Future work should investigate these as reasons for preserving as much anatomy as possible when elective or emergent amputations are considered.
Limitations and future considerations
Study limitations include that subjects’ strength was not measured with dynamometry, and strength clearly affects forces necessary to sit down and stand up. Furthermore, in this sample, the majority of RLLs were >50% and subjects were predominantly at the Medicare Functional Classification Level (MFCL) 3. Potentially, RLLs <50% and other MFCLs could affect results. Additionally, several factors introduce errors and variation in joint moment calculation. These include accuracy of joint center estimation due to marker placement and movement, as well as instrument error. Furthermore, joint moments were determined at defined extraction points and referred to as peak values. These kinetic peaks approximated maximal acceleration and deceleration. Different correlation values may result if joint moments were calculated outside of peak values. Potential future methodology could evaluate correlations using absolute angular impulse, possibly enabling comparison of the entire moment profile as opposed to a single discrete point within it.
Because kinetic differences between prosthetic knee types studied were not profound and variance was high, 1 this study evaluated the entire sample as a single group as opposed to comparing by knee type. Another consideration regarding knee type is that this analysis was conducted under the assumption that each knee type’s inertial properties were the same. However, the prosthetic knees’ masses differed; thus, it is likely their inertial properties also differed.
Given the heterogeneity in subject characteristics and relatively small sample size, study power is a concern. Consequently, further data analyses by age group and amputation etiology were not possible. Therefore, the analysis to determine whether the force required for these activities changes as a result of age and amputation etiology was not done but merits further investigation.
Conclusion
Sound hip moments demonstrated weak but significant correlations with RLL in TFAs during sit to stand and stand to sit. In addition to these correlations of RLL to sound hip moments during transitional movement, multiple additional factors merit consideration when determining RLL within an amputation level.
Key points
In sit to stand and stand to sit in TFAs, sound side hip moments demonstrate weak but significant correlations with RLL. Therefore, longer RLL could minimize sound hip stress during transitional movements.
Weak correlations have been reported with regard to TFA gait biomechanics and RLL. 6
Other factors likely also merit consideration regarding the determination of RLL at the point of amputation such as surface area for load distribution,7,8 proprioception, and prosthetic control. 9 However, there are many confounding variables that could potentially affect these outcomes, and limb length determination should be made on a case-by-case basis.
Study results are most generalizable to community ambulating TFAs with longer residual limbs (i.e. ≥50% of sound femur length).
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.