
Abstract
Background:
Proprioceptive neuromuscular stimulating insoles are increasingly applied in treating functional complaints, chronic pain, foot disorders and so on.
Objectives:
To evaluate rasterstereography as a tool in objectifying postural changes resulting from neuromuscular afferent stimulation and proprioceptive neuromuscular stimulating insoles and to compare the respective effects on posture.
Study design:
This is a prospective experimental study.
Methods:
A total of 27 healthy volunteers were consecutively exposed to six different varying intense neuromuscular afferent stimulating test conditions at three different times. One test condition featured proprioceptive neuromuscular stimulating insoles. In each test condition, a sequence of 12 rasterstereographic recordings of back shape was documented. Changes between six different test conditions and over time for 14 posture characterising parameters were investigated, for example, trunk inclination, pelvic torsion, lateral deviation of the spine’s amplitude or sagittal spinal curve.
Results:
Standard deviation of our rasterstereographic measurements (±2.67 mm) was better than in most comparable reference values. Different neuromuscular stimuli were found to provoke significant changes to various posture parameters, including trunk inclination, pelvic torsion and so on ( each p < 0.001, F-tests). Proprioceptive neuromuscular stimulating insoles induced significant changes for parameter lateral deviation of the spine’s amplitude (p = 0.03).
Conclusion:
Neuromuscular afferent stimulation and proprioceptive neuromuscular stimulating insoles induce postural changes, which can be detected reliably by rasterstereography.
Clinical relevance
We demonstrated that rasterstereography – a radiation-free imaging modality – enables visualisation and documentation of subtle postural changes induced by varying intense neuromuscular afferent stimulation and the application of proprioceptive neuromuscular stimulating insoles.
Background
Proprioceptive neuromuscular stimulating insoles (PNSI) have been stated to alter posture.1–11 Furthermore, PNSI are considered to be beneficial for patients with neurological disabilities,2,4 orthopaedic foot disorders 3 as well as postoperative discomfort, 6 and they are said to reduce chronic pain in patients with musculoskeletal complaints. 5 Therefore, common aches and conditions, such as splayfoot, knee or lower back pain, neck myogelosis, jaw grinding or headaches,2–8 are being treated using PNSI.
Neurophysiologically PNSI are explained to modulate the neuronal afferent signals by stimulating proprioceptive receptor organs in the foot, for example, muscle spindles. Following cerebral integration, the altered afferences cause a complex modulation of muscle activity3,5–8,11–13 and thereby an alteration of posture. Correspondingly, following the concept of proprioception, various authors5,11,13 also implied that sensomotoric stimulation of the equilibrium organ, stereoscopic vision and the jaw joint effect posture. Although PNSI are widely applied as orthotic therapeutic insoles,1–15 their suspected effects on posture have not been generally accepted or rejected by orthopaedic school of thought or central health insurance due to a lack of methodical research.
Numerous diagnostic means, for example, electromyography or pedography, 14 patient inquiry, 7 gait analysis and muscle power assessment 15 or evaluation of sagittal trunk curvature, 9 have been applied in objectifying the effects of PNSI. Nevertheless, none have been accepted as the reference standard.
Rasterstereography16,17 is a radiation-free three-dimensional (3D) imaging modality which assesses various posture describing parameters (trunk inclination (ti), lordotic angle (la), pelvic tilt (pti), etc.). Rasterstereography has been proven to detect changes of surface profile in the sub-millimetre range. 18 Moreover, rasterstereography has been demonstrated to provide clinically practicable 3D back shape information for the monitoring of scoliosis patients.19–21 Furthermore, spinal deviations resulting from craniofacial morphology variations have been correlated precisely applying rasterstereography.22,23 In theory and in accordance with previous research,16–23 rasterstereography should be sensitive enough to reliably measure expected effects on posture due to neuromuscular stimulation and PNSI. Expected effects are investigated by 14 different postural parameters, characterising the frontal, horizontal and lateral planes, which are targeted by different neuromuscular afferent stimulations and PNSI.
In previous research, rasterstereography has been applied to try to objectify the effects of PNSI.5–7,9 However, these studies do have limitations, either in the experimental setup, 5 in the limited number of evaluated rasterstereographic posture parameters, 9 or they are case reports.6,7 Additionally, no one has evaluated whether rasterstereography is a feasible means to detect and objectify postural change derived from supposedly various intense stimulation of neuromuscular afferent receptor organs. However, there is no generally accepted scaling for the intensity of neuromuscular afferent stimulation. By stimulating different afferences (in the foot as well as in the jaw joint) with varying severities (active muscle contraction vs passive adjustment of joint position and muscle tension), we conclude that they are of varying intensities.
We conducted an experimental study with the working hypothesis that varying intense neuromuscular afferent stimulation and PNSI provoke different postural reactions that can be detected and compared utilising rasterstereography in a prospective manner.
Methods
Study group
The Institutional Review Board of the University Erlangen Nuremberg approved the study, and all experiments were in accordance with the Helsinki Declaration. A total of 27 healthy adults (8 women, 19 men, mean age: 29.6 years) were recruited. They gave their informed consent prior to the experimental procedure.
Rasterstereography
The Rasterstereograph Formetric III (Diers International GmbH, Schlangenbad, Germany) was used to scan the patients. The system was set up, tested and approved by the manufacturer. Patients were examined following the suppliers recommendations (Figure 1).
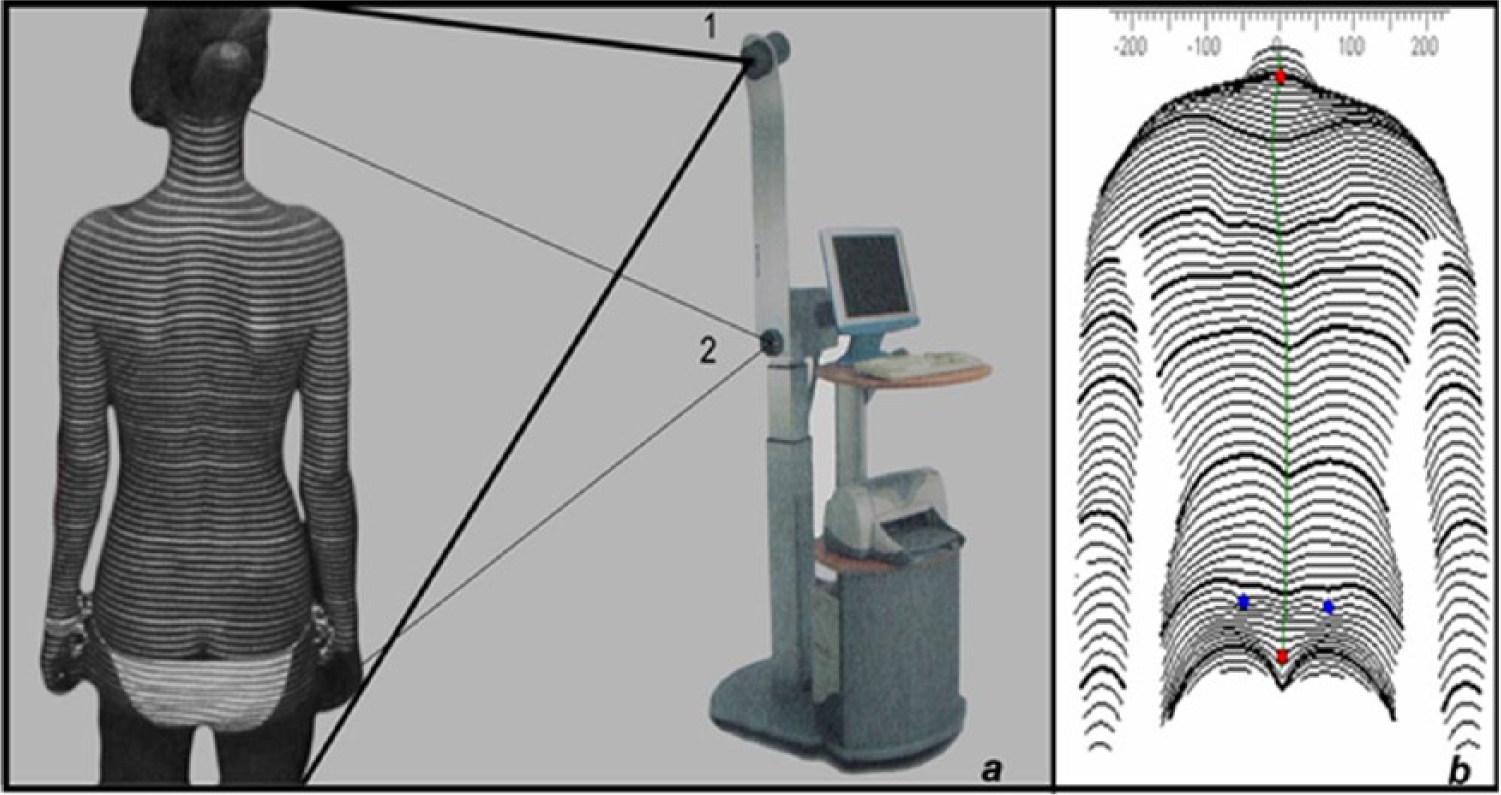
(a) Rasterstereographic measurement setup. Rasterstereography (Rasterstereograph Formetric III; Diers International GmbH, Schlangenbad, Germany) provides optical three-dimensional (3D) back surface measurements. It consists of (1) a detector camera and (2) a light projector. The measurement system projects horizontal parallel lines of white light onto the patient’s back. The uneven back surface distorts these lines, and the camera detects the distorted pattern from a different angle of view as compared to the location of the projector. This reveals precise shape information. The projection and scanning is performed synchronously in 0.04 s. The short measurement time eliminates errors from patient movement or breathing. (b) The system’s software utilises sophisticated mathematical shape analysis algorithms and reconstructs the 3D shape of the spine. This allows the localisation of the anatomical landmarks of the processus spinosi and the left and right spina iliaca posterior superior (pelvic dimples).
Based on an extensive literature review,16–29 we selected 14 different rasterstereographic posture parameters that have been shown to demonstrate postural changes representing movement in all three spatial directions for our investigation. Different parameters are specifically dedicated to investigate movements of the hips (e.g. pti, pelvic torsion (pto) and pelvic rotation (pr)), movements of the lower back (e.g. flèche lombaire (fl) and la) and upper back (e.g. flèche cervicale (fc) and kyphotic angle (ka)) as well as symmetry of the whole spine in the different spatial directions (sagittal: ti, fc, fl, ka and la; frontal: pti, rotation of back surface to the left (brl), rotation of back surface to the right (brr), back surface rotation’s amplitude (bra), lateral deviation of the spine to the left (ldl), lateral deviation of the spine to the right (ldr) and lateral deviation of the spine’s amplitude (lda); plane: the axial: pto and pr) (see online supplementary material).
We suppose that these 14 parameters provide a comprehensive representation and characterisation of posture. Therefore, postural changes due to neuromuscular afferent stimulation are expected to have an effect on these parameters. To evaluate accuracy and reliability of rasterstereographic measurements, the intra-individual distance in millimetre of distance between left and right lumbar dimples (DL-DR) was documented with every measurement.
PNSI
The PNSI utilised in this study (MedReflexx®; München, Germany) feature nine firm-elastic pads arranged according to the short foot muscles. 11 The proprioceptive stimulus can be individually adjusted by adapting the pressure in each firm-elastic pad (Figure 2). An expert (10 years of experience) in the use of PNSI manually adjusted the pad pressure to the starting pressure level that is usually adopted during therapy. This afferent (proprioceptive) stimulation changes its intensity while walking due to strain and relief in every step.5–7

Examined proprioceptive neuromuscular stimulating insoles (PNSI) (MedReflexx) feature nine firm-elastic pads which can be individually fitted, and their pressure can be adapted during therapy.
Test conditions
Proprioceptive stimulation was tested by six different test conditions in a fixed order representing one test row. Derived from the implications by Pfaff, 5 Fusco 11 and Bricot 13 concerning the effects of proprioceptive stimulation on different receptor organs and respective alteration of posture, we stimulated afferences in the foot and jaw joint and evaluated active intentional and passive undeliberate stimulations. During the stance in these test conditions, the rasterstereographic back measurements were taken.
Test condition 1: habitual posture (HP) – the subject stands barefoot in a normal relaxed stance. This provides the rasterstereographic measurements that were taken as a reference compared to the other test conditions.
Test condition 2: foot elevation (FE) – the subject stands barefoot, left foot on the ground, while the right foot stands on a 10-mm thick plank. This exclusive one-sided foot elevation is expected to distort the proprioceptive afferent neuromuscular system and cause quasi-continuous functional movements of the hip and possibly the spine. Based on previous work24–26 with similar experiments, alterations in pelvis position (namely, pto) are expected. Furthermore, we expect this pelvic torsion to consequently cause movement of the spine in the frontal plane (e.g. lda). However, this has not been demonstrated before. Therefore, we examine significantly more posture parameters than Drerup et al.24,26 and Meyer zu Bentrup 25 in previous work.
Test condition 3: Janda’s short foot (JS) – the subject stands barefoot and is instructed to firmly plantar flex all toes and simultaneously press them hard into the ground. This is a proprioceptive foot muscle exercise termed ‘Janda’s short foot’ according to its inventor. 27 Pfaff 28 claims that condition JS stimulates the foot’s afferences in a comparable fashion as PNSI, resulting in similar cerebrifugal modulation of afferences and comparable alteration in posture. Due to forceful muscle contraction of the foot and its connected muscle chains, condition JS is anticipated to modify posture in all three dimensions: for example, trunk inclination and spinal curvature (sagittal plane), pelvic torsion and rotation (axial plane) pelvic tilt, as well as possibly lateral deviation of the spine (frontal plane) due to a more forceful activation of subjects’ dominant leg.
Test condition 4: loose jaw (LJ) – normal relaxed barefoot stance, combined with a dental cotton roll held loosely between the mandibular and maxillary dental arches on the right side of the jaw. By separating the jaw and altering the joint position, this condition is supposed to modulate the tension of the masseter muscle and its adjacent neck and back muscles. According to the concept of proprioception,13,29 altered joint position and muscle tension cause modulation of the neuromuscular afferences inducing an alteration in cerebral efferent signal which, therefore, induce an alteration of posture. Condition LJ is expected, among others, to alter thoracic curvature as measured by flèche cervicale or back surface rotation.
Test condition 5: bite (BT) – normal relaxed barefoot stance with a forceful bite onto the dental cotton roll placed between the mandibular and maxillary dental arches on the right side of the jaw. This one-sided muscle contraction is believed to affect posture parameters primarily representing the frontal plane.
Test condition 6: stance with PNSI (PNSI) – normal relaxed barefoot stance on a pair of PNSI. Each subject received PNSI which were fitted to individual shoe sizes. The pressure in each of the nine firm-elastic pads was manually adjusted to the starting pressure level that is usually adopted during therapy. This was performed by an expert with 10 years of experience in the use of PNSI. We expect to detect an alteration of posture parameters similar to the ones altered in test condition JS. With test condition PNSI inducing passive reflectory movement, we do not expect to see similar change in amplitude compared to the active and most intense stimulation in JS.
Experimental protocol
The sequence of measurements is set up using three independent single test rows. Each test row is conducted with a 1 h break in-between. Every test row includes three separate sets of data acquisition for every subject in all six test conditions, each with a 1 min break. Each set of data acquisition contains four single rasterstereographic measurements (Figure 3). In total, 216 different measurements were taken from each subject.
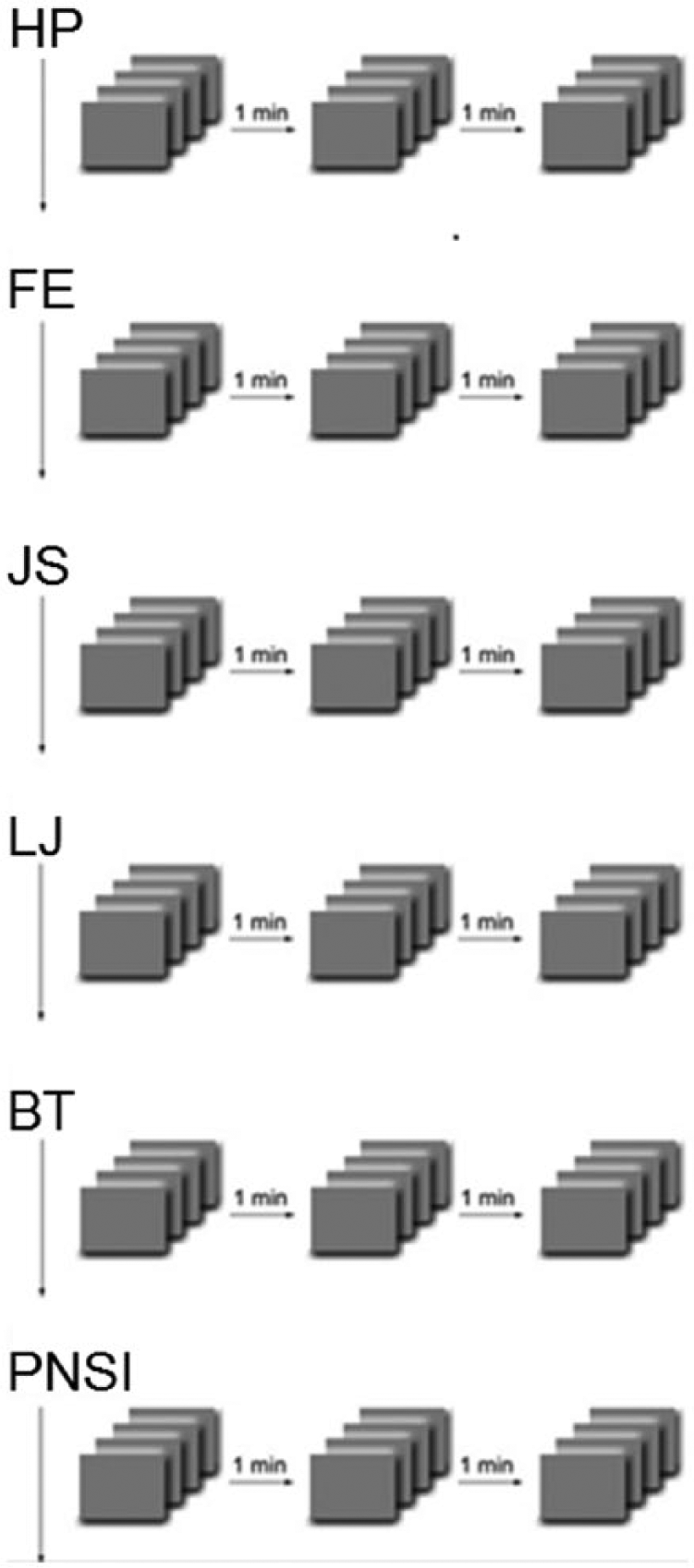
Experimental protocol: four single rasterstereographic measurements are taken in each of the three sets of data acquisitions with 1 min break in-between, for all six test conditions. In the experimental setup, three test rows are performed with 1 h break in-between.
Data analysis
Individual repeated measures within a test row were averaged and served as outcome variables for further analyses. The data are presented as mean (±standard deviation) referring to the measures either regarding a specific test condition in general or a specific test condition at the assigned time point (test row). In order to compare the six test conditions, boxplots are displayed. Due to the model assumption of normality, Box–Cox transformation was applied for trunk inclination (ti), right and left back surface rotation (brr and brl) and lateral deviation amplitude (lda). Furthermore, only positive values of pelvic inclination (pi), flèche cervicale (fc), kyphotic angle (ka) and lordotic angle (la) were analysed as a result of excluding outliers. To detect differences among the test rows and conditions, a mixed linear model with test row and condition as fixed effects and patient as random effect was performed for each of the remaining posture parameters. The p values of the F-test for the fixed effects were gained. If the F-test was significant, corresponding pairwise Tukey–Kramer post-hoc tests were conducted. All hypothesis tests were two-sided, and a p value less than 0.05 was considered statistically significant. Reliability was investigated utilising the standard deviation (in millimetres) of the collective intra-individual DL-DR. This value has been established by previous rasterstereographic studies as the parameter for measurement accuracy.24,25,30–32
Statistical analyses were carried out using the SAS program version 9.2 (SAS Institute, Cary, NC, USA), and graphs were produced with the R system for statistical computing (version 2.11.1; R Development Core Team, Vienna, Austria).
Results
Reliability analysis
The standard deviation of the collective intra-individual distance of DL-DR was ±2.67 mm. This indicates that in each individual, the distance between the two lumbar dimples was detected with good precision.
Separate evaluation of the posture parameters
Trunk inclination (ti): parameter ti differed statistically significantly between the six test conditions (p < 0.0001, F-test). In particular, condition JS leads to a significantly higher trunk inclination angle than all other test conditions (p < 0.0001). Hence, in condition JS, the subjects are tilted more forward. Mean values of the angle of the trunk varied between 3.27° ± 2.40° for HP and 4.54° ± 2.99° for JS (Figure 4).
Flèche lombaire (fl): among the test conditions, statistically significant differences were present (p < 0.0001, F-test). A smaller fl was apparent for JS in comparison to the remaining conditions (p < 0.0001) (Figure 5).
Flèche cervicale (fc): similar results concerning the test conditions were obtained for fl (p < 0.0001, F-test). Significant differences were found for JS compared to each of the remaining conditions (p < 0.0001).
Pelvic tilt (pti): positive values of pti varied significantly among the test conditions (p = 0.001, F-test). More precisely, differences were apparent for JS in comparison to HP (p < 0.01), LJ (p < 0.01) and BT (p = 0.03). Mean values of positive pelvis inclination were 17.25° ± 4.83° for JS, 15.43° ± 6.12° for HP, 15.84° ± 5.79° for LJ and 16.04° ± 5.28° for BT.
Pelvic torsion (pto): the F-test revealed significant differences between the test conditions (p < 0.0001). In comparison to all other conditions, smaller values of the pelvis torsion were observed for FE (p < 0.0001).
Lateral deviation of the spine’s amplitude (lda): the absolute deviation amplitude was proven to differ significantly among the six test conditions (p < 0.01, F-test). The deviation in condition FE was significantly higher than in conditions JS (p < 0.01) and PNSI (p = 0.03). On average, amplitudes of 17.03 ± 7.19 mm for FE, 15.41 ± 7.70 mm for PNSI and 14.75 ± 6.82 mm for JS were measured.
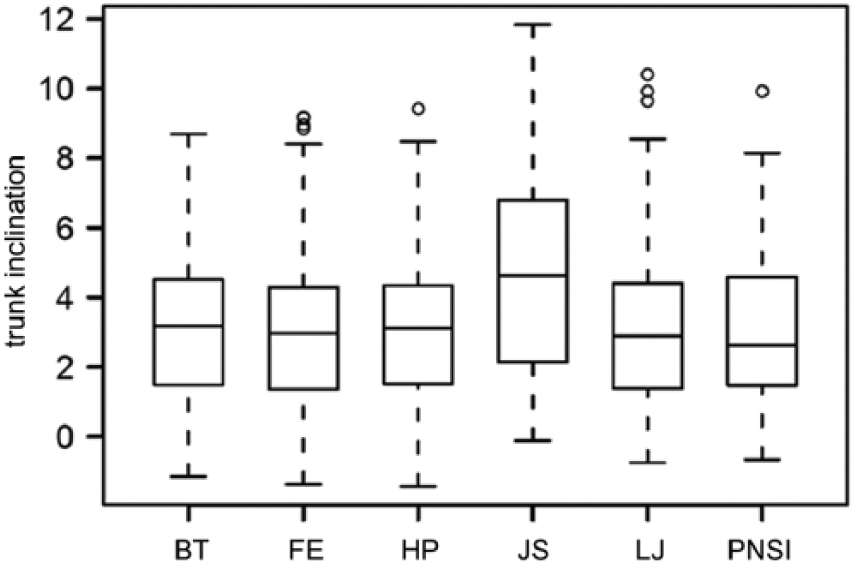
Boxplot featuring the results for parameter trunk inclination (ti) in degree in all six test conditions: bite (BT), foot elevation (FE), habitual posture (HP), short foot according to Janda (JS), loose jaw (LJ) and proprioceptive insoles (PNSI).
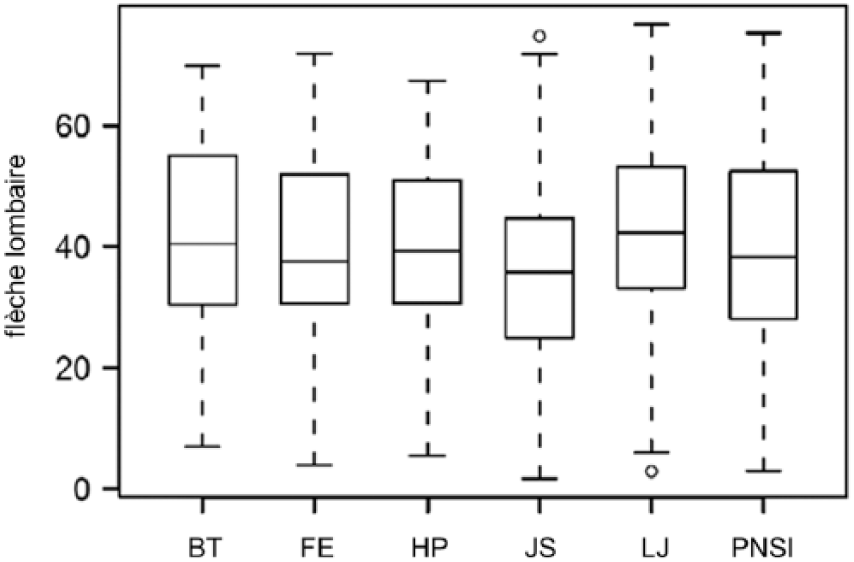
Boxplot featuring the results for parameter flèche lombaire (fl) in millimetre in all six test conditions: bite (BT), foot elevation (FE), habitual posture (HP), short foot according to Janda (JS), loose jaw (LJ) and proprioceptive insoles (PNSI).
Evaluation over the three different points in time
Studying the temporal sequence of tests, significant differences between the three examination times for ti (p < 0.01, F-test), fc (p = 0.02, F-test), fl (p < 0.0001, F-test) and lda (p = 0.03, F-test) were revealed. Mean values of ti decreased from the first row (3.81° ± 2.62°) to the last row (3.15° ± 2.47°) with p < 0.01; fl increased from the first row (38.40 ± 15.62 mm) to the second row (40.28 ± 15.55 mm) with p < 0.01, and even more to the last row (41.59 ± 14.75 mm) with p < 0.001; lda increased from the second to the third test row with p = 0.03 from 15.52 ± 7.69 mm to 16.14 ± 7.24 mm.
Further analysis
No relevant evidence for an association between the other parameters (la, ka, pr, brl, brr, bra, ldl and ldr) and the test conditions or test rows was apparent.
Discussion
One objective of this study was to evaluate how reliably rasterstereography can objectify postural changes induced by different neuromuscular afferent stimulation and PNSI. In order to investigate whether our rasterstereographic measurements are sound and reveal conclusive data, we examined the standard deviation of a rasterstereographic precision parameter. Previous works have found the deviation of the intra-individual distance DL-DR as the precision parameter for the evaluation of standard deviation. This study demonstrates a standard deviation of 2.67 mm for DL-DR. Comparing our standard deviations with previous studies which produced a DL-DR of 4.6 mm, 25 1.04 mm 31 or 1.8 mm, 32 the accuracy of this study can be rated as being good. As this proves the accuracy of our experimental setup and rasterstereographic measurements, we also conclude our measured postural parameters to be accurate. Our study stands in consistency with previous research,16–23,29–33 which demonstrates the method of rasterstereography to be able to measure postural parameters in a clinical setting.
Another objective was to investigate whether rasterstereography can detect postural alteration resulting from neuromuscular stimulation. Therefore, we implemented test conditions with various intense stimuli (JS vs PNSI; LJ vs BT) and stimulated afferent proprioceptive receptors in the foot and jaw.
We proved JS to provoke the biggest alteration in posture. For this test condition, we detected an increased trunk inclination with a high level of significance. We found an increased forward ti of about 1.3° in the mean together with significantly smaller fl and bigger fc (Figure 6). A similar alteration of measured parameters regarding posture alterations in dependence of Matthias test was demonstrated by Drerup et al. 30 and Betsch et al. 31 Our research demonstrates that the well-known phenomenon of various stimuli inducing different afferences 34 can be quantified by rasterstereographic measurements. Alterations of posture were proven for biomechanical (test condition FE) and neuromuscular proprioceptive stimuli (test conditions JS and PNSI).
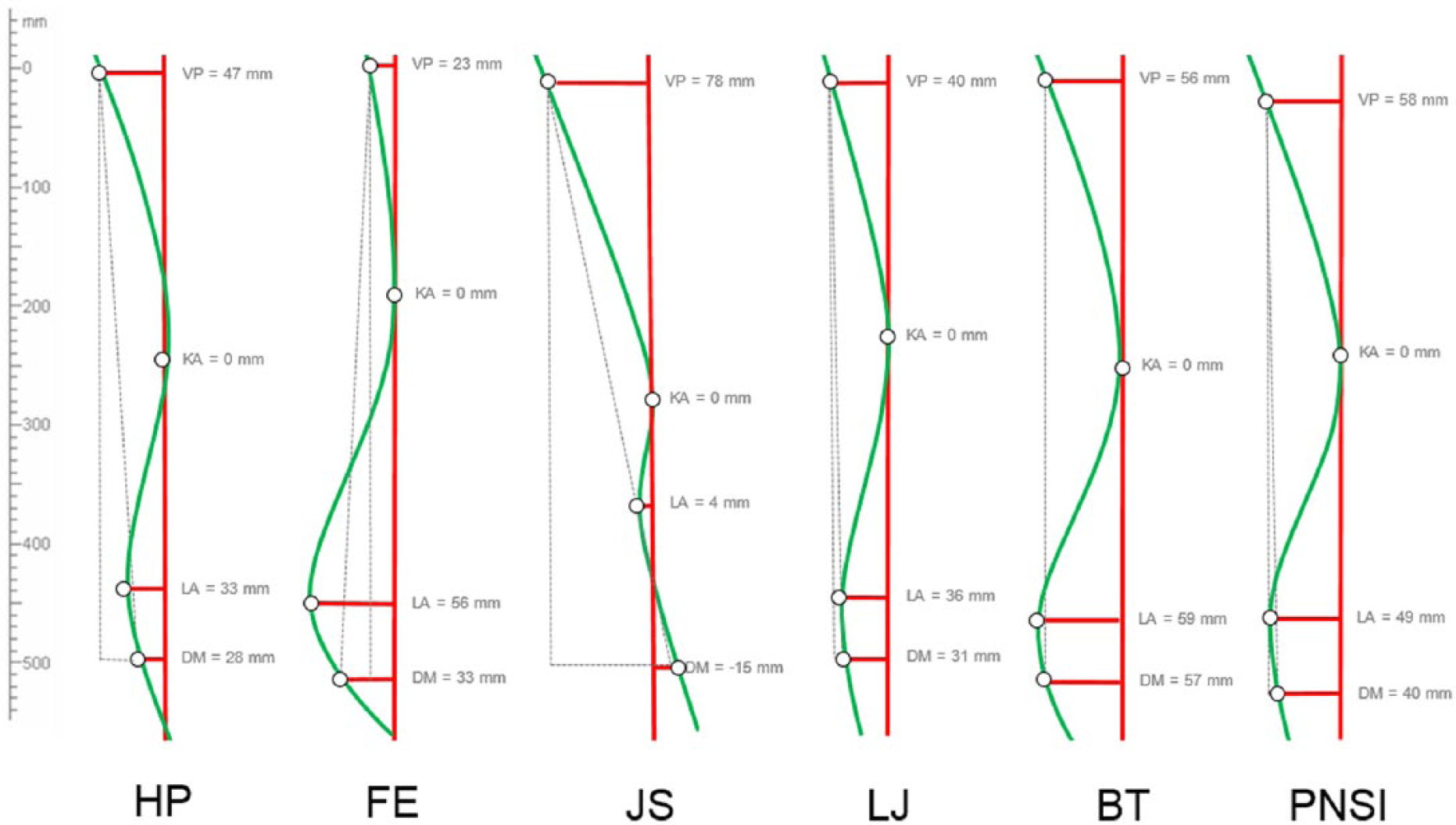
Sagittal profile changes of a subject in the study comparing (a) test condition habitual posture (HP) with (b) test condition short foot according to Janda (JS).
A further objective of this investigation was to evaluate whether rasterstereography serves as a tool in objectifying postural change provoked by PNSI. PNSI are claimed to be a dynamic active stimulator due to varied afferent stimuli during walking (similar to barefoot walking on natural surface). Furthermore, in theory, PNSI are said to have similar effects on the foot muscles as the proprioceptive exercise JS in our test condition.5,12,25 Therefore, postural changes should be similar to those documented in condition JS.
In our study, significant postural alteration was revealed for lateral spinal movement for test conditions PNSI and JS (both vs FE). Furthermore, postural reactions for both test conditions were aligned in the same direction, since lda reduced in both test conditions, which made them comparable in form. Moreover, for various posture parameters (pto, pti, pr, fc, fl, la and ka), slight but not statistically significant postural changes were found for conditions PNSI versus HP. It revealed in a comparable way the postural alterations detected between conditions JS and HP. As expected, parameters representing pelvis positioning and spinal curvature were affected by conditions JS and PNSI. However, our findings indicate differing intensities. In contrast to JS, no significant differences for ti, ldl or ldr were detected. We believe that this supports our interpretation of JS and PNSI as stimulating in a similar way but in different intensities. Therefore, we conclude that the obviously small subconscious insole stimulus is not as intense as an active intentional contraction of foot muscles, and therefore, the postural changes are smaller. Nevertheless, effects to posture from PNSI were observed reproducibly. Therefore, follow-up studies regarding the postural effects of neuromuscular stimulating insoles should, in contrast to previous studies, 9 include all posture parameters presented in this study.
It has to be emphasised that this study was exclusively designed to investigate reproducible immediate short-term effects of neuromuscular stimulating insoles on posture. This study with a 1-h interval between test rows demonstrated significant postural changes over time for ti, fc, fl and lda. In clinical practice, patients were PNSI continuously for 8–10 weeks6,7 Furthermore, patients being treated with PNSI usually have one to two adjustments to pad pressure before their posture is re-evaluated rasterstereographically. So far, no long-term study has investigated the postural effects of PNSI. However, as demonstrated by this study, the method of rasterstereography supplies the ability to monitor postural effects caused by PNSI in long-term studies. Furthermore, long-term research can be directed at systematically analysing different rasterstereographic posture parameters in order to establish a scoring system for a simple evaluation of proprioceptive effects on posture.
Conclusion
We proved that varying intense neuromuscular afferent stimulations alter posture and demonstrated that PNSI to elicit immediate effects on posture. All these postural reactions were reliably and reproducibly detected utilising rasterstereography. This reveals the clinical relevance and necessity of utilising this non-invasive clinical diagnostic test for posture evaluation, for example, when monitoring the therapeutical effects of PNSI.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.