
Abstract
Background: Discrepancies exist in the current literature for bracing of spinal curvature conditions. This can be explained by the diversity of brace types, the different curve patterns and the various measurement methods and instruments.
Objectives: The aim of this study was the analysis of the corrective forces exerted by a dynamic derotation brace (DDB), at the skin-brace interface, altering the strap tension and body posture.
Study Design: We analysed the direct forces exerted by a DDB’s main pad, on 44 (38 girls, 6 boys) idiopathic scoliotic patients. Twenty-seven patients had a single right thoracic and 17 a single left or right thoracolumbar curve.
Methods: We used the F-Socket 9801 pressure sensor and the MatScan Research BETA STAM 6.30 software, while patients adopted nine different postures. The patients were divided into three different groups: those who wore the brace for the first time, those who were changing their brace for a new one, and those who were having adjustments made to their existing brace.
Results: These patients who were having adjustments made to their existing brace caused the highest mean exerted force. Changes in strap tension and body posture resulted in statistically significant alterations of the interface pressure and the forces exerted on the patient’s body.
Conclusions: Tightening the brace’s straps always produces a significant force increase, independent of the body posture and the curve type. Also there are some body postures which significantly modify the exerted force. The body posture of maximum inspiration for thoracolumbar curves and, additionally, prone and lying left for thoracic curves.
Clinical relevance
Analysis of forces does not provide information on the correction of spinal curvature, but seem to be helpfully trying to achieve the brace’s optimal fit and the best therapeutic result.
Background
One of the interconnected factors which relate to the degree of the spinal correction, are the forces acting through the pads of the brace upon the body. When worn for an appropriate length of time, scoliosis braces can stop the scoliotic process from progressing and at least maintain the scoliotic curves to that seen on initial orthotic treatment. 1 However, it is not uncommon for the brace treatment to be unsuccessful in achieving this goal. The main reason may be the unsuitable corrective forces, exerted by the brace. The magnitude of these corrective forces for optimal curve correction is still not determined. A few studies have tried to determine these corrective forces, for various types of brace, acting upon the body during the brace treatment, using different types of measurement systems.1-2 Mac-Thiong et al. 1 using a mat made of force-sensing transducers, tried to determine the strap tension associated with optimal Boston brace interface forces. Aubin et al.2 used straps instrumented with load cells and tightened at four tensions in order to determine the variations in strap tension in different patient positions. For both papers, the adequate corrective force was crucial to the success of brace treatment.
Few authors have sought to measure forces or pressures at the skin-brace interface. Van den Hout et al. 3 measured the exerted forces using the electronic PEDAR measuring device (Novel, Germany) and Pham et al. 4 the pressures using the Tekscan ClinSeat Type 5315 Sensor. Dynamic analyses of the exerted forces or the distribution of the pressure for a variety of body postures have been performed by Aubin et al.2, Van den Hout et al., 3 Pham et al., 4 Cochran and Waugh 5 and Wong and Evans. 6 However, there were great disparities between the published data, which can probably be explained by the diversity of brace types studied, the different curve patterns and the various measurement methods and instruments. No papers were found which analysed the forces exerted by a DDB or the distribution of pressure where forces were applied. This makes the comparison between previous different studies very difficult.
The DDB used in this study is a custom-made, underarm spinal orthosis extending from underneath the axilla to the pelvis, featuring aluminium pressure blades, set to produce derotating and anti-rotating effects on the thorax and trunk of scoliosis patients. The main body of the brace is made of one 3-mm thick piece of polyvinylchloride (PVC). It opens at the back and is fastened with four straps. The DDB was designed to correct scoliotic curve-types commonly classified as thoracic, thoracolumbar, lumbar and double major (thoracic and lumbar). 7 The function of the DDB follows concepts of passive and active deformity correction. The brace provides mechanical support to the patient body (passive correction) and the patients pull their body away from the pressure sites (active correction). The DDB corrects the scoliotic curve through the application of forces which are transmitted to the spinal column mainly through the inner main pad, and the rest of the pads. 7
When the brace is applied, the derotating pressure blades exert anteriorly-directed forces at their fixation points and posteriorly-directed forces under the opposite half of the brace. The magnitude of the forces applied by the derotating pressure blades is added to the correcting forces already exerted by the brace at the area of the main pad, and can be controlled by changing the angle of the pressure blades backwards and the strap tension. 7
In this study we measured the direct corrective forces exerted by the main pad of the brace, working upon the body, by using a pressure sensor and the TekScan software, altering the strap tension and analyzing the variation of these forces with body posture and investigating the connection of its efficacy with the parameters of strap tension, body posture, the magnitude of the exerted forces and the fitting of the brace on the patient. This hardware and software system is already frequently used in podiatry, and has proven its value in that field. 8 Our purpose was to establish the practicability of this system as a useful tool in studies on DDB treatment and furthermore, the DDB to become one of the most successful scoliotic braces.
Methods
The study was performed on 44 patients (38 girls, 6 boys), who attended the Department of Scoliosis & Spine, KAT Hospital, Athens, Greece, Ideal Scoliosis Centre, Athens, Greece and Ortho-Foot Centre, Nicosia, Cyprus, for a regular check-up and braces correction, or an appointment to wear the brace for the first time. All were asked to participate and they were selected according to the following criteria: a) patients presenting confirmed idiopathic scoliosis; b) aged 10 years and over, with a Cobb angle ranging from 20° to 40° in the absence of the brace, c) wearing a DDB (Figures 1A and 1B); and d) there were available recent posteroanterior and lateral standing thoracolumbar spine radiographs with and without the brace after six months of brace use, for a recommended wearing time of 23 hours per day.
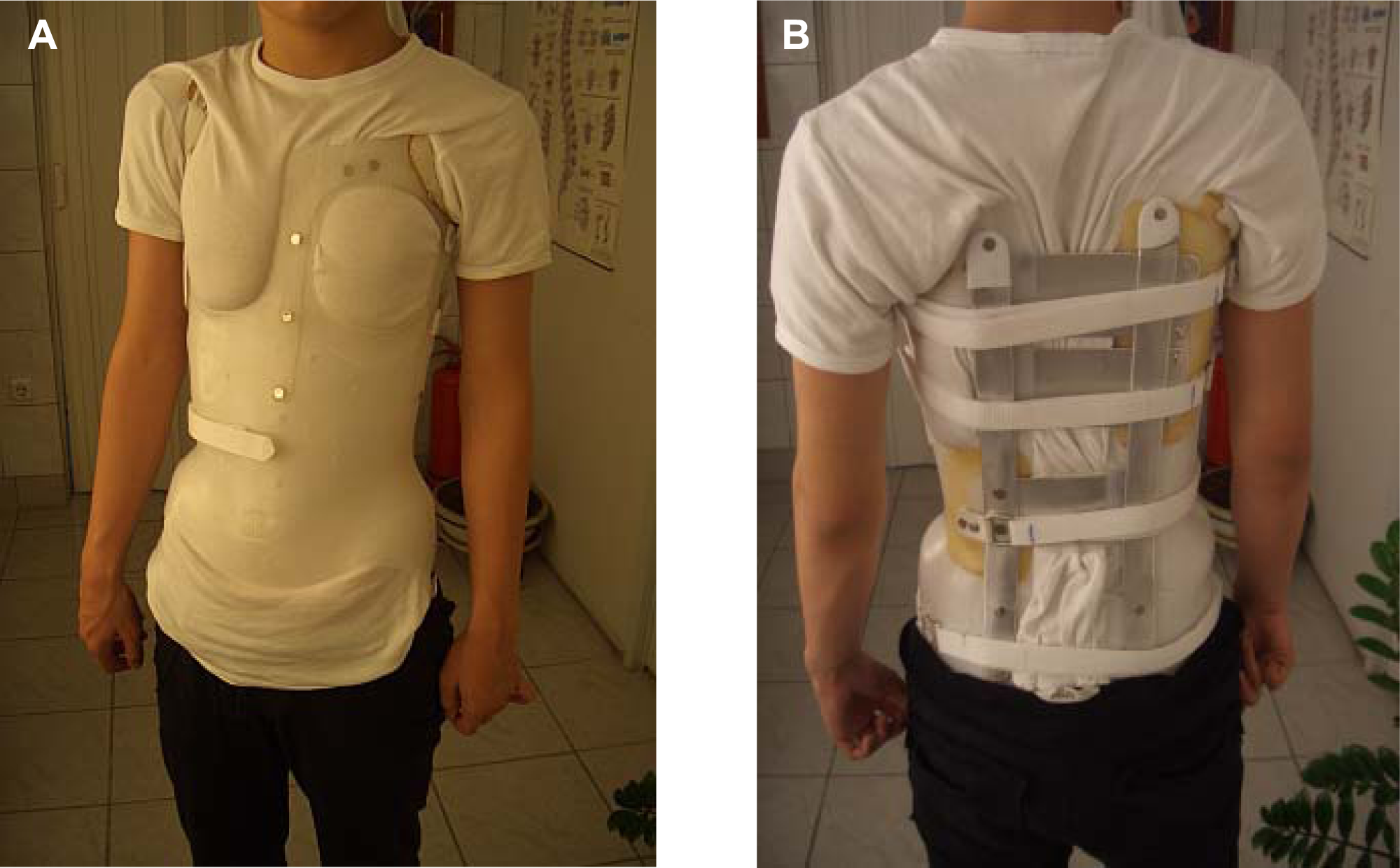
The two sides of the dynamic derotation brace.
The patients’ mean age was 13.8±1.8 years (10–17.2 years); height 1.6±0.1 m (1.4–1.8 m) and weight 51.4±10.0 kg (36–80 kg) with Risser sign of 0–4 with mean value of 3.5. Twenty-seven patients had right thoracic curves, nine had right and eight left thoracolumbar curves. With the brace the mean Cobb angle for all the patients was 19.5±5.7° (13°–32°), and in the absence of the brace, was 27.8±6.1° (20°–40°).
The acquisition of the pressure generated by the brace was performed using an F-Socket 9801 pressure sensor connected to the Evolution Sensor Handle with attached USB cable (TekScan, Boston MA, USA) (Figure 2). The sensor presents as a 62.2 x 7.6-cm mat, with a thickness of 0.017 mm. It consists of 96 sensors, and can be trimmed into six independent sensing strips. The total sensing area covered 154.8 cm2 providing a resolution of 0.62 cells per cm2.
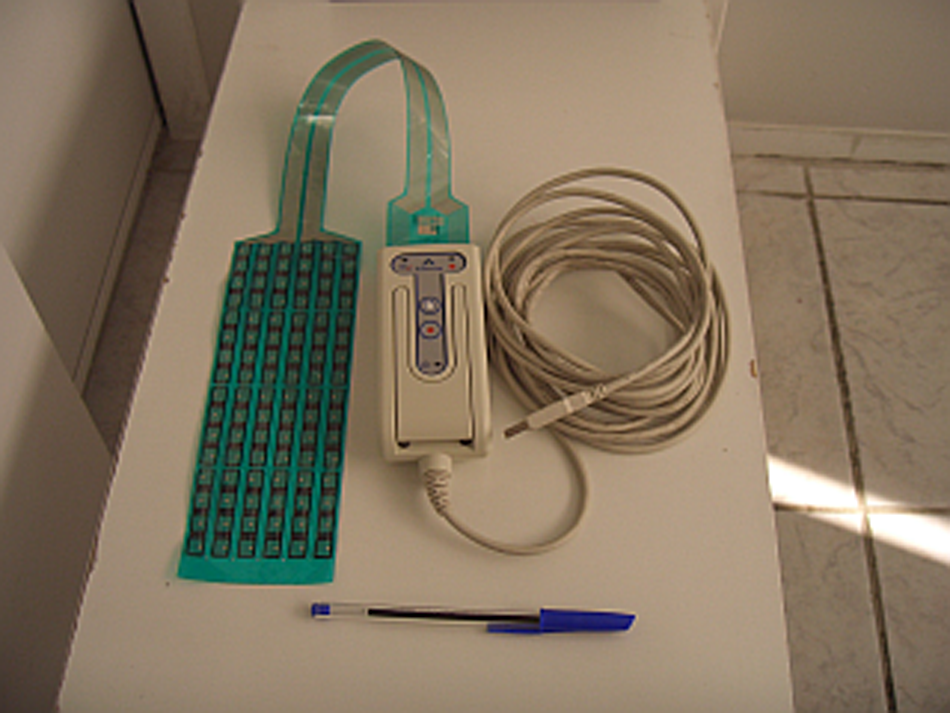
The Evolution Sensor Handle with attached USB cable.
Before the acquisitions, the sensor was calibrated five times according to the manufacturer’s instructions, using five healthy adolescents of varying body weight and the calibration files were saved.8-10 For each patient’s acquisition, the calibration file of the person with the nearest body weight was used. The sensor has been validated in another application in the past. 11 The F-Socket mat was placed between the patient’s back and the inner surface of the brace, exactly at the area where the main pad is positioned, without compromising the corrective mechanism of the brace and without harming and annoying the patient (Figure 3). We decided to limit our force measurements to the main pad area which correct the scoliotic curve, according to the DDB’s mechanical principles. The main pad is always placed against the apex of the hump and the sensor was placed to encompass at the same time the apex of the hump and the position of the pad placement. Its main role is to exert high forces on scoliotic curve. The mean force is what was measured with the centre of the force being always placed into the sensor area. This centre was different for every patient and represents the centre for all the exerted forces. The same brace maker fitted all the braces according to the instructions of the clinicians.
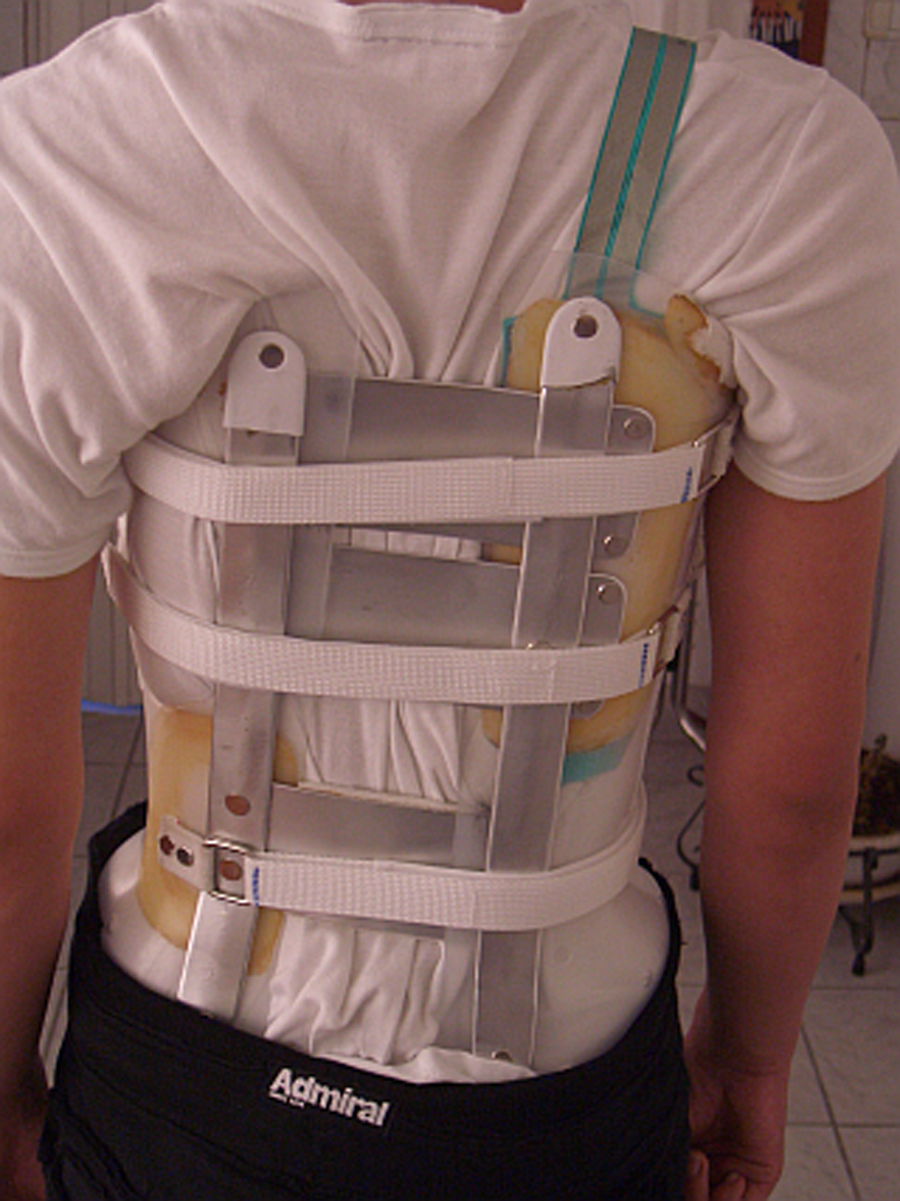
The F-socket placement.
Before the pressure acquisition, we placed a mark on the straps, for the minimum and the maximum point of the strap tension.
After positioning the sensor, every patient was asked to assume a series of nine postures corresponding to everyday tasks: standing (while breathing normally), standing with maximum inspiration, standing with maximum expiration, sitting having the knees at 90°, walking, lying supine, lying prone, lying on the right side and lastly lying on the left side. Pressure values were recorded for 15 sec at 13 Hz and the total investigation time for every patient was approximately 20 minutes (Figure 4). The same investigator performed all the measurements.2 The measurements were processed with the MatScan Research BETA STAM 6.30 software (TekScan, Boston MA, USA).
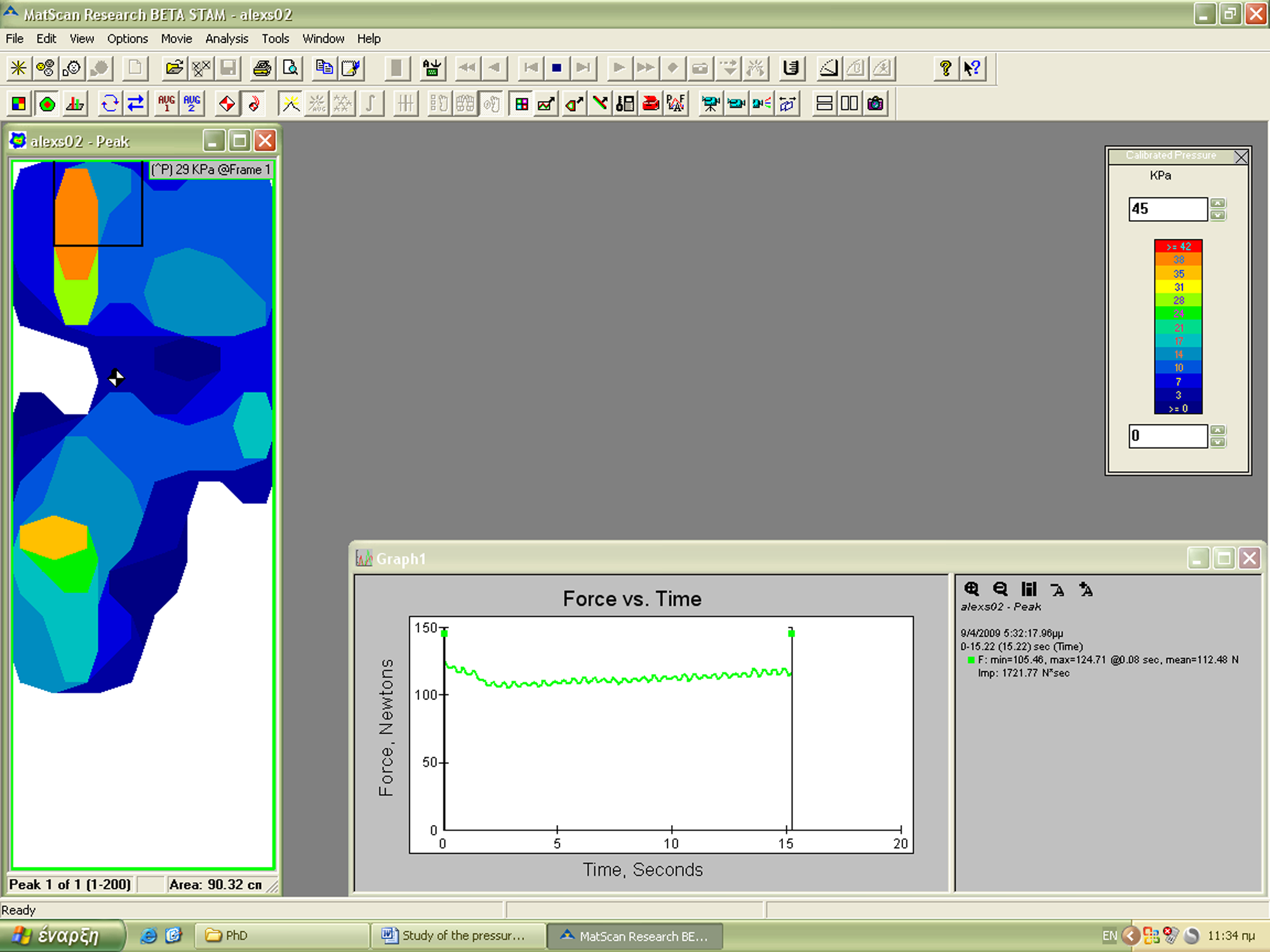
Forces at the area of the pad and the graph.
Statistical data analysis was carried out using SPSS software, version 17.0 (SPSS Inc., Chicago IL, USA). We compared the mean corrective force in a standing position with the corrective force in the other postures using t-test for paired samples. ANOVA was used to compare the mean force for different curve value groups of patients. Pearson’s and Spearman’s correlation coefficient was used to analyze the relationship between the mean force value in the standing position and the radiographic degree of the achieved scoliosis correction. The significance threshold was set to 0.05.
Results
The mean force values for the two types of curve during the nine postures are given in Table 1. It is clear that the mean force is higher, for all the body postures, when the strap tension is at the maximum, for both thoracic and thoracolumbar curves. Also, for all the body postures and for both maximum and minimum strap tension, the mean force value is higher for thoracic curves.
Mean force during the nine postures for all the types of curves.
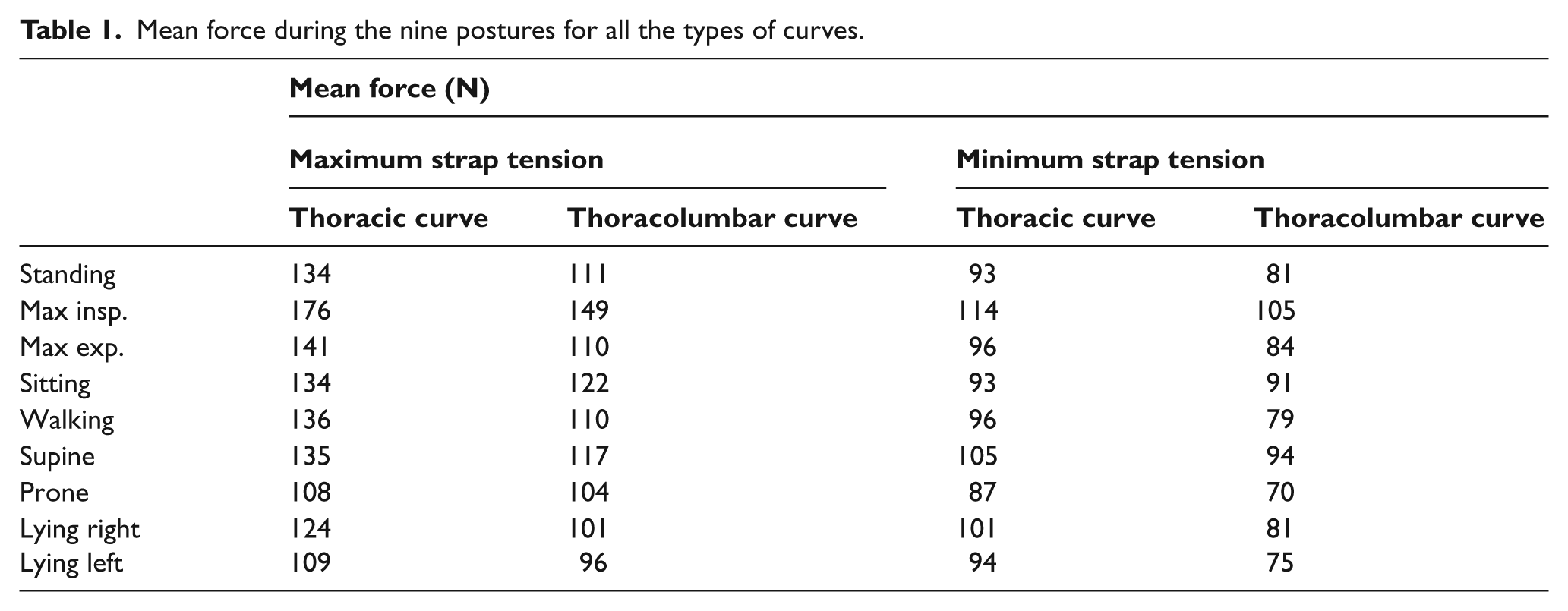
We observed a significant force increase at the moment of maximum inspiration (p<0.005) compared to the standing posture for all the curve types and for both maximum and minimum strap tension. There was not a significant change of the mean force during maximum expiration (p=0.1) whatever the curve pattern and the strap tension was, except the case of thoracic curve with maximum strap tension (p<0.05).
There was not a significant change in the force values in the sitting posture or while walking, except the case of thoracolumbar curve and in the sitting posture for minimum strap tension (p=0.006). For the patients with thoracolumbar curves, there was not a significant change for the force value for all the body postures, except during maximum inspiration, as it was mentioned earlier, and during sitting (p<0.05) and lying supine (p<0.005) but only for minimum strap tension. For the patients with thoracic curve there was significant force reduction during prone (p<0.05) and lying on the left (p<0.005) when the strap tension was maximum.
For thoracolumbar curves, comparing the mean force value between supine and prone, there was a significant difference for both maximum and minimum strap tension (p<0.05). Also, between lying on the right and on the left, there was no significant difference (p>0.2). On the other hand, for thoracic curves, comparing the force value between the same body postures, there was significant difference, p<0.004 and p<0.05 respectively.
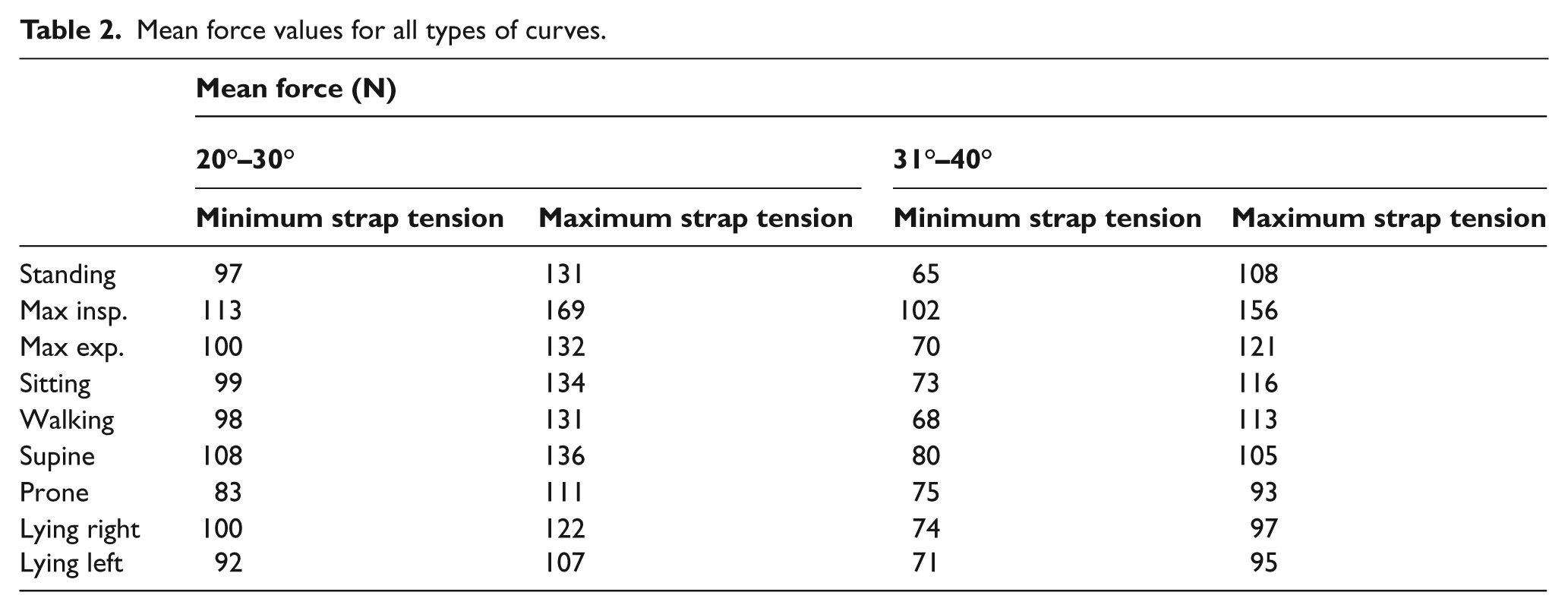
In Table 2 we can see the mean force values for every body posture for both minimum and maximum strap tension, after dividing the patients into two groups. The first group had patients with curves from 20° to 30° and the second, patients with curves from 31° to 40°. For all the body postures and whatever the strap tension was, the mean force value is higher for the first group, but there is not any significant correlation between the exerted force and the type of group (r=0.04, p=0.8).
Mean force values for all types of curves.
Comparing all the patients’ characteristics, we can see that 86% of them were girls, totally for all the types of curve. Also, 64% of them had thoracic curve, 20% thoracolumbar right and the rest 16%, left. The only criteria used in order to select the patients were mentioned earlier in this paper.
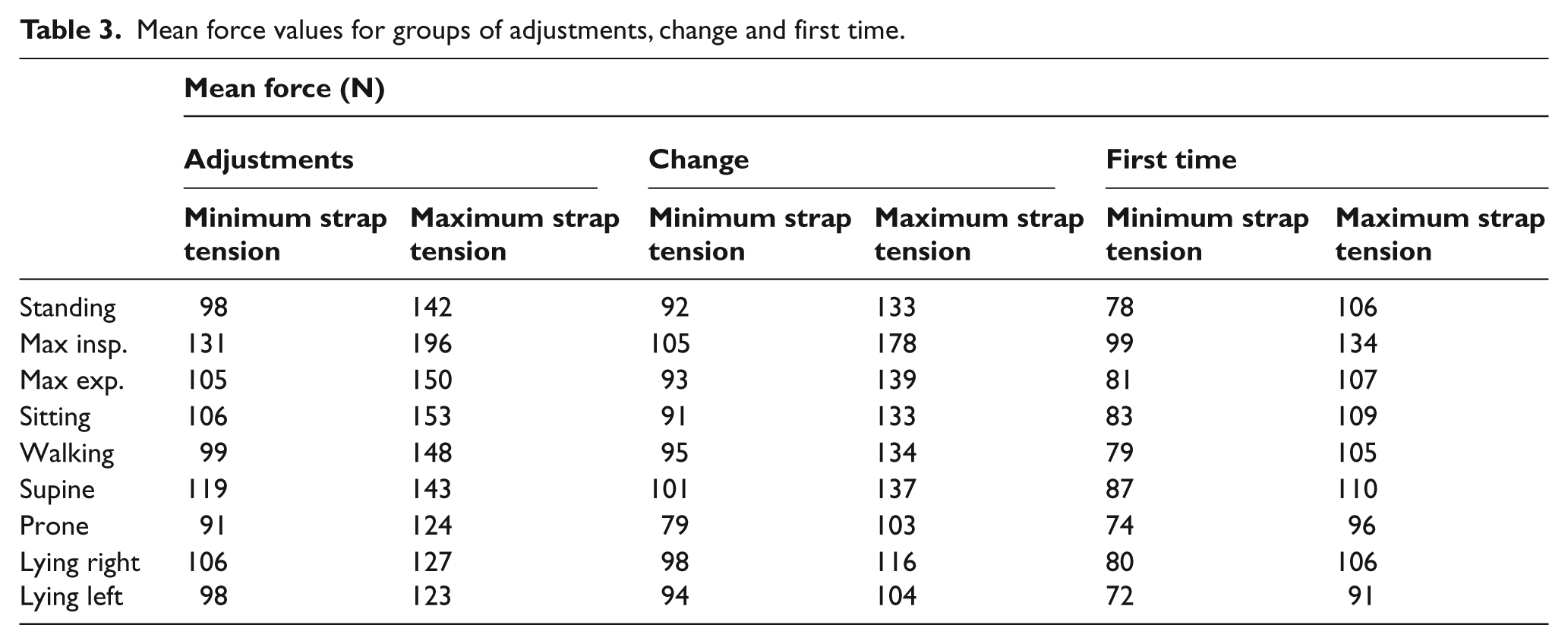
For the third group of patients, some handmade adjustments were made on the brace. These adjustments had to do with the change of the pads, the straps or the fixation of discomfort problems. The angulation of the pressure blades is also one of the adjustments, and was done by very experienced and certified ortotists and prosthetists. After the adjustments were made on a brace, the mean force value, whatever the strap tension was, was the highest compared to the mean force value for a changed, or for a first time use, brace, for all types of curves (Table 3). At the same time the mean force value for the first time use brace was the lowest compared to the rest of the situations. Though, there was no significant correlation between the exerted force and the type of patient group (first, second and third) for all patients (r=0.10, p=0.53).
Mean force values for groups of adjustments, change and first time.
Also, in the standing position and for both thoracic and thoracolumbar curves, there is no significant correlation between the mean force and the degree of the achieved radiographic scoliosis correction (r=0.02, p=0.94 and r=0.28, p=0.40 respectively). For thoracic curves the degree of correction was 25.60±2.08% (-3.00 to 29.30%) and for thoracolumbar curves 31.06±4.56% (20.00 to 43.70%) after six months of brace use, for 23 hours per day.
Lastly, during the measurements of walking for all the types of curve, there was a significant progressive reduction (p<0.05) of the mean force value.
Discussion
Strap tension appears to have a considerable impact on the magnitude of the exerted forces. For both thoracic and thoracolumbar curves there is a significant increase of the mean force, comparing the value for maximum to minimum strap tension (p<0.05) for all the body postures. Pham et al. 4 studying the pressures applied by a Chêneau brace demonstrated similar results having a significant increase of the mean pressure upon tightening the straps. Wong and Evans 6 also found the same for a Milwaukee brace.
Except at the position of maximum inspiration, for both thoracic and thoracolumbar curves and for minimum strap tension, the maximum mean force value was apparent when the patient was supine, and the minimum mean force value when the patient was prone.
We observed a significant increase in main pad forces at the moment of maximum inspiration (p<0.05) whatever the strap tension and the curve pattern. Also, there was a significant change (p<0.05) of the mean force value during the maximum expiration, for thoracic curves and only when the strap tension was maximum. Pham et al. 4 and Cotė 12 found a significant change in the pressure during maximum expiration whatever the strap tension was.
In lying postures and for both thoracic and thoracolumbar curves, the supine posture led to the highest mean force. For thoracic curves and for maximum strap tension there was a significant reduction of the mean force value for prone (p<0.05) and lying left (p<0.005) but not any significant change for supine and lying right. Van den Hout et al. 3 found exactly the opposite, studying the Boston brace, but without being clear about the curve pattern. Wong and Evans 6 evidenced for right thoracic curve that lying right offered the best correction effect for a Milwaukee brace. Complementary to the above we observed a patients’ discomfort during lying right and when the strap tension was maximum. There is a need for handmade adjustments to the brace in order to solve this discomfort problem.
Overall, we observed that the mean force was lower for thoracolumbar than for thoracic curves, whatever the position and the strap tension. However, according to Mouilleseaux, 13 thoracolumbar curves respond better to orthopaedic treatment than do thoracic curves, something which resulted from our findings too, for the degree of correction after six months of brace use for 23 hours per day.
It was also observed that during walking for all the types of curve, there was a significant progressive reduction (p<0.05) of the force value, because of the change of the brace’s right position and the brace straps’ stretching. 14 Aubin et al.2 who quantified the strap tension noted a reduction of the strap tension during activity, which explain the reduction we noticed. So, during everyday activities, the strap tension must be checked, in order to be the appropriate, independently of the body posture and the patient’s activity.
Lastly, today the DDB production is based on a pre-trimmed positive plastic trunk template produced after laser scanning of the patient. A blueprint is thus designed, which is a systematic way of analysing the curve and applying the appropriate force vectors. Although formally recruited for the study, non-cooperation by the patient can lead to measurements errors. In some cases, it was not possible to include the patients’ results for data analysis for this reason. However, in some cases it was possible to rectify the brace during fitting. Also, the straps’ stretching occurring after the brace use for a few months, make necessary the strap tension checking and sometimes changing the straps with new, for optimal result. 14
We did not find any significant change for the force value between standing and maximum expiration. On the contrary, Pham et al. 4 and Coté 12 evidenced significant reduction of the pressure whatever the brace strap tension and the curve pattern was.
We did not find a significant correlation between the mean force in the standing posture and the degree of curve correction for either thoracic or thoracolumbar curves (r=0.02, p=0.94 and r=0.28, p=0.40 respectively). Further consideration of the results and further experiment work are necessary.
Overall, the goal of this study was to make the F-socket sensor and the appropriate Tekscan software, a useful tool in studying pressure distribution on the main pad area, and also in calculating the exerted forces, in order to determine in the future their appropriate values and find the best way of achieving therapy of scoliosis using a DDB. However, the force magnitude alone, it is not enough to determine the degree of correction achieved.3,15 The combination of different factors is what gives the optimal therapeutic result and improves the brace’s efficacy. These factors are: the appropriate magnitude of the exerted force, the right strap tension, the optimal fit of the brace on the patient and the type of curve. This paper proved that DDB is primarily an active brace. The body posture for both thoracic and thoracolumbar curves and being more adjective for thoracolumbar curves, does not gives a significant difference of exerted forces (except the maximum inspiration) which means that the patients can follow their daily programme without compromising, in combination with the fact that DDB improve the clinical and cosmetic condition of the patient. 7
In the near future we will be in the position to include in our data measurements of patients with double major (thoracic and lumbar) scoliosis.
Conclusion
The TekScan system enabled us to measure the forces applied to the trunk by the DDB at the expected area. The use of this pressure measurement device might be in the future a useful tool in order to evaluate a brace’s biomechanical behaviour and help in achieving more effective treatment of the scoliotic patients.
There are body postures which significantly modify the exerted force from the brace; it seems that the maximum inspiration for thoracolumbar curves and prone and lying left for thoracic curves. Of course the body posture of maximum inspiration is not a situation of long duration during the day, but something which happens rarely. So the statistically significant change of the exerted force is not an important fact.
Tightening the brace’s straps always produces a significant force increase, whatever the body posture and the curve type are. It would be really interesting to quantify the strap tensions of our braces, in order to investigate if there is any correlation with the degree of correction of the scoliosis curve. There is a natural trend toward lower forces during activity, so strap adjustment during the day seems to be necessary and useful. In the future, we hope to investigate the relationship between exerted force and applied pressure, for a greater number of patients and for more curve patterns.
Lastly, independently of the patient group, almost all the patients, more or less, saw an improvement in their clinical condition after the use of the DDB for a short or a long period, with the aim of a reduction of the curve degree. Only one patient’s clinical condition was worse and another one had an absolutely stable clinical condition after six months of the DDB’s use.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.