
Abstract
Background:
Rocker outsole shoes are commonly prescribed to patients with diabetic neuropathy to offload a particular area of the foot sole, thereby decreasing the risk of foot ulceration. Contrary to this, some evidence has reported a postural destabilising effect of these shoes in healthy adults.
Objective:
To explore the postural stability of patients with diabetic neuropathy who wear a rocker outsole shoe.
Study design:
Quasi-experimental.
Method:
In total, 17 patients with diabetic neuropathy (aged 49.29 ± 7.48 years; 7 female, 10 males) participated in this study. A Motor Control Test measuring centre of force displacement, response strength scale and response latency in medium and large perturbations was conducted using the EquiTest system to evaluate postural stability while wearing a baseline shoe (without a rocker outsole) or a rocker outsole shoe (with a toe-only rocker sole).
Results:
No significant difference was observed between the shoe conditions in centre of force displacement and response latency of the participants (p > 0.05). The results indicated a significant increase in the response strength scale of participants by the rocker outsole, for medium forward and backward and large forward perturbations (p = 0.014, p = 0.001 and p = 0.027, respectively).
Conclusion:
When the immediate effect is a concern, the rocker outsole shoe did not negatively affect postural stability in patients with diabetic neuropathy.
Clinical relevance
This article will provide objective evidence about the effect of rocker outsole on postural balance in diabetic patients. In prescription of rocker outsole to prevent plantar ulceration of diabetic foot, immediate postural destabilising is not a concern.
Background
Diabetes is one of the most common global neurovascular diseases. The worldwide prevalence of diabetes was reported to be approximately 366 million in 2011, with this figure estimated to rise to 552 million by 2030. 1 Up to 50% of people with diabetes suffer from diabetic peripheral neuropathy, 2 which is a major factor in the development of foot pressure ulcerations.3,4 Around 15% of patients with diabetic neuropathy experience foot ulcers at least once during their life. 5 The annual incidence of foot ulceration in diabetic patients has been reported to be 2%–3% worldwide 6 and 4%–10% in the United States and United Kingdom. 7 This incidence rate increases up to 5%–7.5% among diabetic patients with neuropathy. 8 Almost 85% of lower extremity amputations in patients with diabetes has been reported to occur following foot ulcerations. 5 Moreover, the economic cost of treating diabetic foot ulcers is enormous. 9 In 2007, the treatment of diabetes and its complications cost the United States US$116 billion; at least 33% of these costs were related to the treatment of foot ulcers. 10 Therefore, prevention and appropriate management of foot problems in patients with diabetes are of paramount importance. To prevent ulceration in the foot with diabetic neuropathy, management of pressure distribution at high-risk areas, such as the forefoot, is an established method.11,12 Rocker outsoles are currently the most effective intervention capable of reducing forefoot peak plantar pressure by up to 50%.13–15
Rocker outsoles are commonly prescribed to prevent foot ulcerations in patients with diabetic neuropathy.13,14,16 However, these outsoles have been shown to negatively affect postural stability, at least in healthy young adults through increasing mean values for sway amplitude, range and variance in response to backward perturbation. 17 Moreover, the onset of returning to the first stable position following perturbations was found to be significantly delayed while wearing rocker outsoles. 17 The Functional Stability Margin (FSM), the numerical calculation of the distance between the maximum displacement of centre of mass and the centre of pressure during perturbations, is another postural balance measurement that has been shown to be smaller during rocker outsole use in healthy young adults. 17 Therefore, rocker outsoles may increase the potential for postural imbalance. On the other hand, diabetic peripheral neuropathy has been directly linked to increased fall risk, and patients with diabetic neuropathy have inherent balance problems and deteriorated postural stability.18–20 Therefore, prescription of rocker outsoles to prevent ulcerations may aggravate these patients’ postural stability; however, this has not been evaluated in these patients to date. This study was proposed to investigate the effect of rocker outsole shoes on the postural stability of patients with diabetic neuropathy. It was hypothesised that the rocker outsole would have an immediate destabilising effect on postural stability in patients with diabetic neuropathy.
Methods
Participants
The sample size was calculated using G-Power 21 considering α equal to 0.05 and β equal to 0.2. Postural composite response latency was considered as the main outcome measure, and its standard deviation was calculated on a pilot of five participants while wearing rocker outsole and baseline shoes that was equal to 16.97 and 18.75 ms, respectively. It was determined that a sample of at least 17 participants was required to achieve power of 0.8 for this quasi-experimental study. Inclusion criteria were participants aged between 25 and 55 years; score > 2 on Michigan Neuropathy Screening Instrument (MNSI; this is a 15-item self-administered patient questionnaire adapted from the Neuropathy Symptom Profile of Dyck et al. 22 and a structured foot examination); 23 diabetic duration > 5 years; 24 visual acuity > 20/40 in Snellen chart; 20 normal range of motion of hip, knee and ankle and ability to stand and walk independently without any assistive devices. 25 Structured foot examination of MNSI consists of five specific stages scored from point 0 to point 10 by a specialist physician, which includes foot physical inspection, foot ulcer assessment, vibration perception, ankle stretch reflexes and monofilament testing. Scores greater than 2 show a greater risk of promoting neuropathic foot ulceration. 26 Patients with a history of foot ulceration, deformity, surgery and pain in lower extremities, back pain, hypertension, 20 any musculoskeletal or vestibular disorders 25 and medications interfering with balance 27 were excluded. Patients were recruited from a local university hospital where a specialist physician checked the criteria for each patient. Participants who met the inclusion criteria of the study voluntarily signed a written consent form. Ethics approval was obtained from the ethics committee of the affiliated university.
In total, 17 patients with diabetic neuropathy, 10 female and 7 male and aged 49.29 ± 7.48 years, participated in this study. The characteristics of the participants in regard to age, height, weight, body mass index (BMI), diabetes duration and MNSI score are summarised in Table 1.
Descriptive statistics of age, height, weight, BMI, diabetes duration and MNSI score.
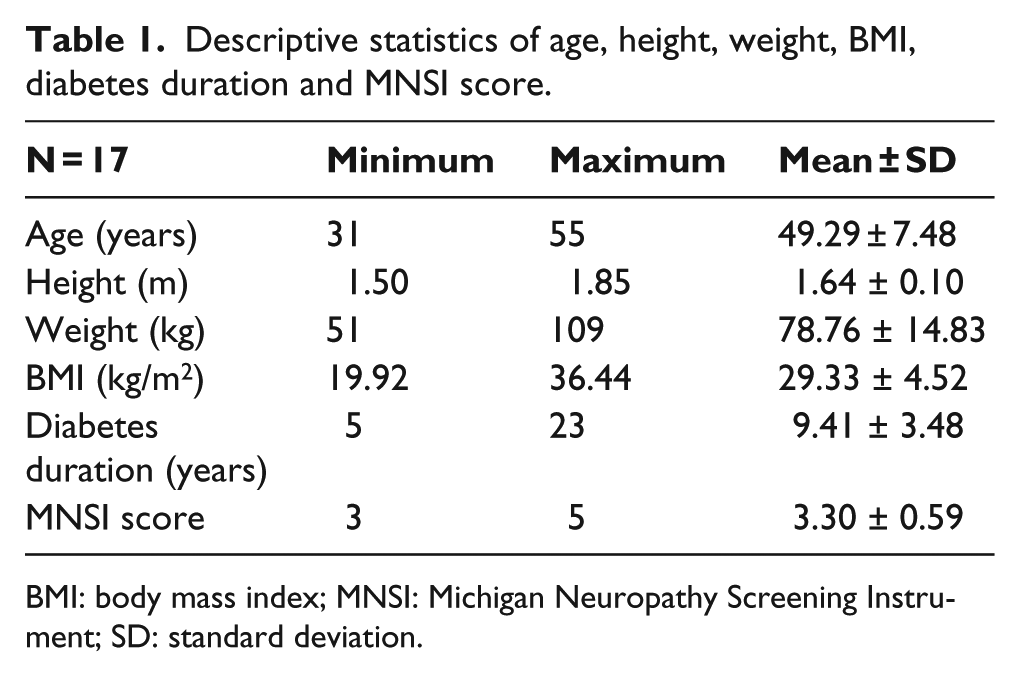
BMI: body mass index; MNSI: Michigan Neuropathy Screening Instrument; SD: standard deviation.
Equipment
Footwear
The rocker outsole shoe consisted of a toe-only rocker outsole fitted to a gymnastic shoe, with seven pairs of different shoe sizes constructed for this study. Since the pure assessment of rocker outsole modification was the aim, a type of shoe (gymnastic shoe) with the least minimal interference was considered for rocker outsole attachment. Gymnastic shoes were previously applied in a number of studies as shoes with almost no interventional effect 28 for simulating barefoot condition.29,30 Regarding the diabetic foot considerations and an emphasised issue that people with diabetes should not walk barefoot, 31 seven pairs of gymnastic shoes with no rocker outsole were used as baseline shoes. As the shoes were the same for all participants, any interference of this type of shoe was the same between subjects and thus could be ignored. The rocker outsoles were made of ethyl vinyl acetate (EVA) with measured standard hardness of 35 on Shore D Durometer Scale (which is approximate to 85 on Shore A Durometer Scale). The height of the outsole was 28 mm from heel to the rocker apex which was positioned at 62.5% of the shoe length. The amount of 62.5% was chosen based on a previous report which had suggested a range of 60%–65% of total shoe length for most effective positioning of the rocker apex. 15 The rocker angle of 23° was also employed based on earlier reports. 16 The rocker outsole shoe similar to rocker outsoles used in previous studies17,32,33 is not defined as a rigid rocker shoe as it did not contain a steel shank, thus the pure effect of rocker outsole was evaluated. All of rocker outsoles were manufactured by a certified orthotist. The participants used both the rocker outsole shoe and the baseline shoe (Figure 1) in a random order.
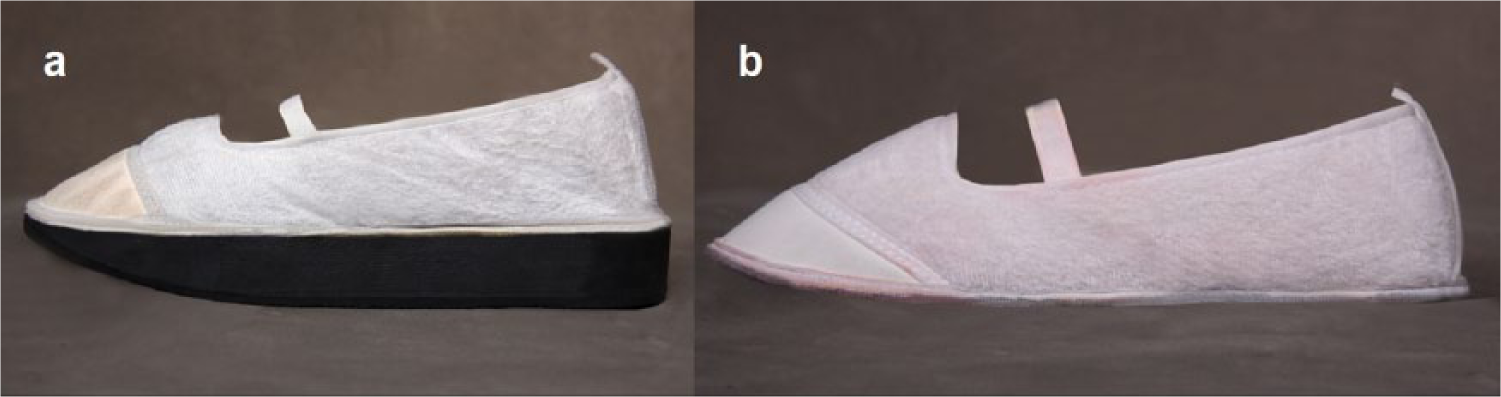
(a) Rocker outsole shoe and (b) baseline shoe.
Procedures
The EquiTest system, a dynamic dual force plate (NeuroCom International, USA), was set to automatically perform the Motor Control Test (MCT) with a sampling rate of 100 Hz. The MCT consists of four horizontal platform perturbations which are medium backward and medium forward and large backward and large forward with three repetitions for each one which made a total of 12 trials. The duration of perturbations was 300 ms for medium and 400 ms for large ones. The speed and magnitude of each perturbation were normalised to the height of the participants. The sway induced by each of the medium and large perturbations has a fixed amount of angular momentum. To counteract this sway, the patient must generate an active force response to stop the induced sway followed by moving the body to equilibrium. 34
Participants were given 15 min to stand and walk with each of the rocker outsole shoe and the baseline shoe in order to become accustomed to them. Appropriate shoe size was selected for each participant. The gymnastic shoes were secured on participants’ feet by an elastic strap closure. Participants were asked to stand on their height-matched location over the platform with their eyes open, looking forward with arms by their sides. A suspension vest was worn by the participants and was attached to the shoulder straps which were fixed on the top of the visual surround, for safety purposes. The shoulder straps were loose enough to avoid interference with the tasks and tight enough to avoid injury in the case of a fall (Figure 2). If any displacement in foot position occurred on the force platform or stepping, the test was stopped and repeated. The centre of force displacement (defined as linear displacement of a single point in which all of the forces exerted by the legs on the platform are combined), response strength scale (reflects the participant’s ability to produce a level of force appropriate for the degree to which the participant has been displaced by each force plate perturbation and defined as an amount of angular momentum in degrees per second imparted by the active force response normalised to body height and weight) and response latency (defined as the time in milliseconds between the onset of force plate perturbation and initiation of the active force response in legs) were recorded. In order to avoid beginning and ending fluctuations, the first and last 10 samples on centre of force were not used.

EquiTest system.
Statistical analysis
Statistical analysis was conducted using SPSS (Version 18; SPSS Inc., Chicago, IL, USA). One sample Kolmogorov–Smirnov analysis was employed to check the normal distribution assumption. As normality was assumed, parametric one-tailed paired t-test was utilised for data analysis. Differences were considered statistically significant when the p value was less than 0.05.
Results
The average centre of force displacements, response strength scales and response latency in the presence of large (forward and backward) and medium (forward and backward) perturbations while using the rocker outsole and baseline shoes were compared. The details of results are presented in Table 2. There were no significant differences in centre of force displacement between the rocker outsole and baseline shoes in all four conditions.
Paired sample t-test results for the centre of force displacement, response strength scale and response latency.
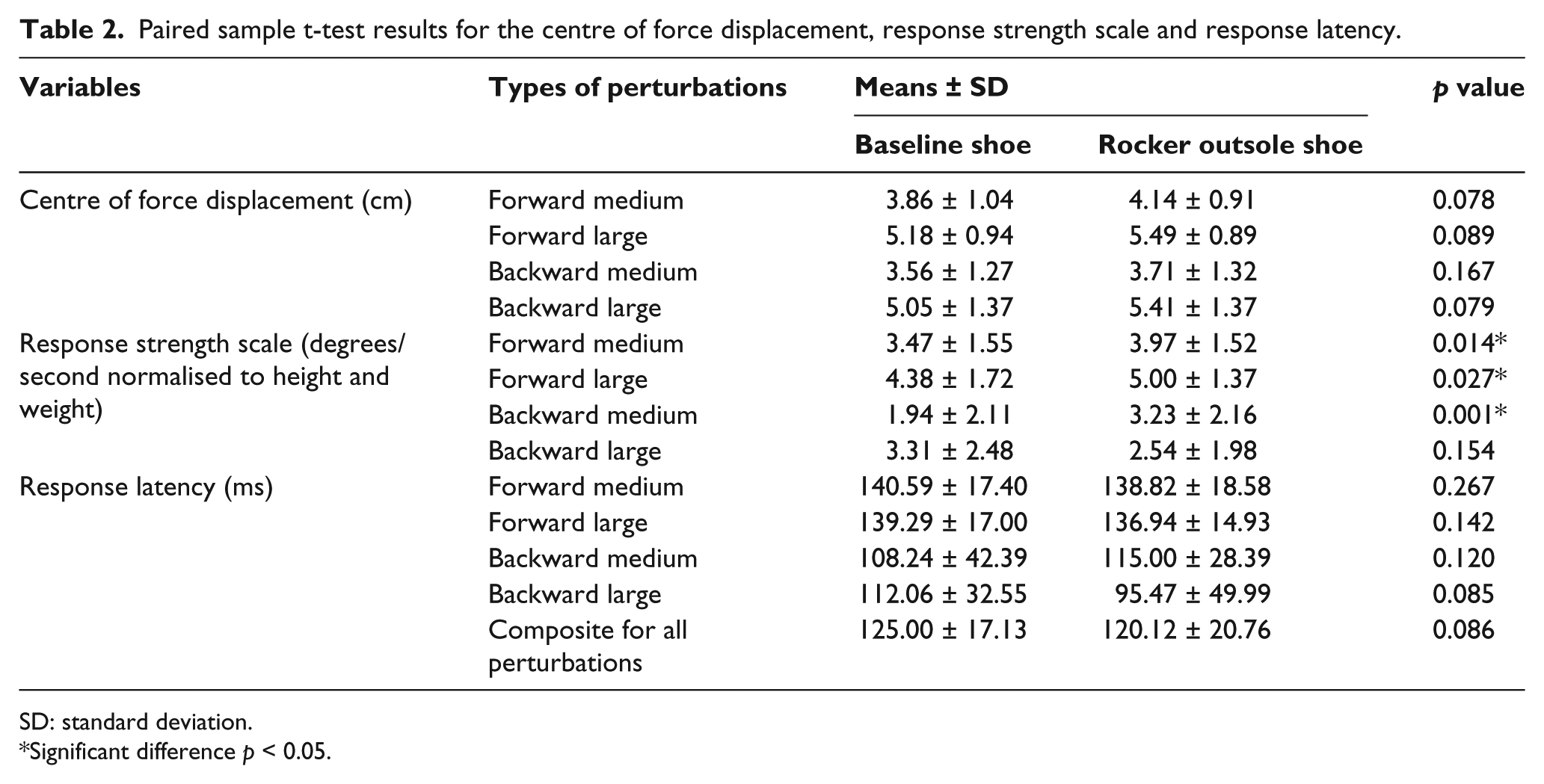
SD: standard deviation.
Significant difference p < 0.05.
However, there was a significant difference between the rocker outsole and baseline shoes for response strength scale in medium perturbation for both backward (p = 0.001) and forward (p = 0.014) perturbations. These differences were also significant for large forward perturbation (p = 0.027) but not for backward perturbation (p = 0.154).
No significant difference was observed for response latency between rocker outsole and baseline shoes in all four conditions and accordingly for the composite response latency (p = 0.171).
Discussion
This study aimed to investigate the postural stability of patients with diabetic neuropathy while they wore a rocker outsole shoe. It was hypothesised that the rocker outsole would have an immediate destabilising effect on postural stability in patients with diabetic neuropathy. Our findings did not demonstrate such a destabilising effect.
The postural balance was measured using centre of force displacement, response strength and response latency. In the literature, EquiTest system normative values for the MCT are only available for the response latency, and, therefore, the results of this study provide some estimated values for patients with diabetic neuropathy. A normal range of postural response latency to an external stimulus is reported to be between 90 and 100 ms in a barefoot condition, 35 whereas our results showed a mean of 125 ms postural response latency to perturbations in patients with diabetic neuropathy while wearing the baseline shoe. This demonstrates an inherent postural response delay in this group of patients irrespective of having baseline or rocker outsole shoes. Rao and Aruin 36 in their investigation of the immediate effect of auxiliary sensory cues on automatic postural responses of patients with diabetic neuropathy found similar results. They showed the mean composite response latency of about 154 ms for these patients, which is much greater than the normal range, and the immediate use of an ankle foot orthoses improved it to a mean of about 147 ms. These results are consistent with the study results of Inglis et al. 37 in which individuals with diabetic neuropathy responded to translational perturbations with a significant delay of almost 20 ms in comparison to control groups. No shoes were worn during test procedures for the mentioned studies. Hence, the innate latency of postural response to unexpected platform perturbations in patients with diabetic neuropathy may be related to a significant decrease of nerve conduction velocity following the peripheral neuropathy. 38
Albright and Woodhull-Smith 17 demonstrated that rocker bottom shoes destabilise the posture of healthy young adults in response to backward perturbation, which is inconsistent with our findings. This contrast can be explained in different ways. On one hand, the types of rocker outsoles used in the study of Albright and Woodhull-Smith were mild rockers and negative heel rockers which are different from the type of rocker outsole applied in our study (i.e. the toe-only rocker). It has been stated that toe-only rockers are the only rocker outsoles indicated either for prevention of metatarsal head ulcers associated with diabetic neuropathy or for patients with proprioception or balance disorders. 39 The mild rocker outsole is characterised by a mild rocker angle at both the heel and toe and is mainly prescribed to reduce the pain associated with early hallux rigidus and replace the decreased motion of the first metatarsal head. The mild rocker outsole is used in conjunction with extended steel shanks when prescribed. 39 The negative heel rocker outsole in which the height of the outsole under the heel is the same as, or lesser than the height under the ball of the foot, shifts weight-bearing forces to the hindfoot and midfoot. This type of rocker outsole is commonly prescribed for patients who feel unstable with the normal height of other rocker outsoles or in higher heeled shoes. 39 On the other hand, the observed difference might be related to the nature of the postural stability system in patients with diabetic neuropathy who inherently have deteriorated balance. It is possible that the negative impact of the rocker outsole on impaired postural stability system of these patients was too little to make a significant change. Moreover, the insignificant results of this study might be related either to the diminished sensitivity of foot mechanical receptors due to diabetic neuropathy, which makes the environmental changes less detectable, or to the interrupted transfer of sensory inputs to the central nervous system.34,38
Although no significant difference was found in this study for centre of force displacement and response latency which could demonstrate no change in balance and postural stability of patients with diabetic neuropathy while wearing rocker outsole shoes, the effect of rocker outsole on the response strength scale of these patients was significant in most of perturbations. The response strength scale of patients using rocker outsole shoe was significantly greater than that of patients using the baseline shoe in both forward and backward medium perturbations and forward large perturbations (p < 0.05). Enhanced response strength scales by the rocker outsole shoe may reveal more active force generating as a result of increasing muscular effort in order to maintain this postural balance. In other words, no alteration of postural balance while wearing rocker outsole shoe in these patients might be due to the greater strength of responses to perturbations. Another possible explanation could be related to a smaller base of support of the rocker outsole versus the baseline shoe, which may need stronger strength responses for preserving the postural stability.
Furthermore, the greater response strength scales of patients while using rocker outsole shoe may show more muscular demand as already mentioned. Recent studies on a type of rocker bottom shoes known as ‘unstable shoes’ have shown that electromyography (EMG) activity of calf muscles significantly increases in addition to improvement of venous circulation in healthy subjects.40,41 From this point of view, the rocker outsole could provide a training effect on balance and postural stability that might be advantageous in patients with diabetic neuropathy. Sousa et al. 42 demonstrated that long-term use of unstable shoes enhances the co-activation level of ankle and leg antagonist muscles, thereby enhancement of postural stability system performance. The study by Ramstrand et al. 43 showed that the unstable shoe improves dynamic stability of children with developmental disability after 4 and 8 weeks of intervention. Another study has shown an enhancement of static and dynamic stability in elderly adults wearing unstable shoes over 8 weeks. 44 However, the rocker outsole used in this study is different from the unstable shoe outsole both in the material and the geometry. Therefore, the training effect of rocker outsole shoes on balance in patients with diabetic neuropathy needs further studies considering prolonged use.
This study found that the toe-only rocker sole does not negatively affect postural stability of diabetic patients with neuropathy immediately and supports the prescription of toe-only rocker outsoles to prevent forefoot plantar ulceration. In addition to clinical importance, this study could be used as an initial investigation for future studies which may consider long-term wearing of rocker outsoles in this patient group.
For future studies, we suggest that the long-term effect of rocker outsole shoes on balance in patients with diabetic neuropathy be evaluated. Employing a control group would also be beneficial for interpreting the results, which was a limitation to this study. Another possible limitation is the height difference between the baseline and rocker outsole shoes, which was related to the aim of this study and based on the footwear used in previous researches. Further investigations are needed to determine whether height of the rocker outsole solely affects the posture of patients with diabetic neuropathy. Finally, kinetic and kinematic analyses of gait parameters in patients with diabetic neuropathy with and without rocker outsole shoes is further recommended.
Conclusion
A rocker outsole is prescribed to protect the insensate foot of patients with diabetic neuropathy from ulceration, and our results demonstrated that the rocker outsole does not negatively impact immediate postural stability in patients with diabetic neuropathy.
Footnotes
Author contribution
Study concept and design: Banafshe Ghomian, Mojtaba Kamyab, Hassan Jafari, Mohammadebrahim Khamseh and Aoife Healy. Acquisition of data: Banafshe Ghomian and Mohammadebrahim khamseh. Analysis and interpretation of data: Banafshe Ghomian, Mojtaba Kamyab and Hassan Jafari. Drafting of manuscript: Banafshe Ghomian, Mojtaba Kamyab, Hassan Jafari, Aoife Healy and Mohammadebrahim Khamseh. Critical revision of manuscript for important intellectual content: Mojtaba Kamyab, Hassan Jafari, Aoife Healy and Banafshe Ghomian. Study supervision for final approval of the version to be submitted: Banafshe Ghomian, Mojtaba Kamyab, Hassan Jafari, Aoife Healy and Mohammadebrahim Khamseh.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This work was supported by Iran University of Medical Sciences.