
Abstract
Background:
The aim of this pilot study was to investigate the effectiveness of serial splinting in two children with bilateral knee flexion contractures due to arthrogrypotic syndrome.
Case description and methods:
We evaluated the infants’ passive knee extension limitation and motor development levels. Serial orthotic treatment was applied to decrease bilateral knee flexion contractures in the knees of the subjects. The follow-up period was up to 1 year.
Findings and outcomes:
At the end of serial orthotic treatment, improvement in bilateral passive extension limitation (for the first case, the increase in passive range of extension was approximately 75°, for the second case it was 45°) was achieved in both cases.
Conclusion:
We believe that serial orthotic intervention is effective in patients with arthrogrypotic syndrome at the preoperative period or in patients who cannot be operated on. Further studies are needed for evaluation of effectiveness of this method.
Clinical relevance
Our pilot study aimed to investigate the effectiveness of serial orthotic treatment in knee contractures due to arthrogrypotic syndrome in two infants which showed an improvement in range of extension.
Background
Arthrogryposis is a non-progressive syndrome of multiple joint contractures that are present at birth. The etiology of the syndrome remains uncertain. 1 Although a similar form was described by Otto in 1841, the term “arthrogrypotic syndrome” was used first by Stern in 1923. The incidence of arthrogryposis is one in 5000–10,000 live births. 2
The most common cause of arthrogrypotic syndrome is lack of fetal movement. It is thought that the lack of fetal movement and formation of extra connective tissue around joints causes contractures. Contractures in arthrogryposis can be seen either on its own or as part of the syndrome as well as neurological, myopathic, and systemic disease. 3
Joint contractures in arthrogrypotic syndromes are usually symmetrical and divided into three groups. These are as follows: (1) with limb involvement only, (2) with limb involvement and other malformation or anomalies, and (3) with limb involvement and central nervous system dysfunction or mental retardation.1,3
Most common deformities in extremities are pes equinovarus, calcaneovalgus, vertical talus, flexion and ulnar deviation of the wrist. In the knee and elbow, either flexion or extension contractures can be seen.4,5 Owing to the fact that developing deformities impair the child’s motor ability, it is important to intervene in a timely manner in order to minimize these deformities. 1
Case description and methods
This study was carried out on two consecutive infants who had bilateral knee contractures due to arthrogrypotic syndrome. Other problems accompanying the diagnoses, based on the motor development levels according to Gross Motor Function Classification System (GMFCS), and demographic characteristics were recorded. Also, bilateral passive knee extension limitations were measured with universal goniometry by the same physical therapist (PT) experienced in such measurements at each session.
Case 1
The first was a 7-month-old infant with arthrogrypotic syndrome who had hand and foot deformities and various problems such as Young–Simpson syndrome, congenital hypothyroid, congenital heart disease, severe mental retardation, hypotonia, facial dysmorphism, and postnatal growth deficiency. She could control her head during supported sitting for only a few seconds. Her motor development level according to GMFCS was 5. Physical examination showed hyper mobility of upper extremity joints, bilateral pes planovalgus, and bilateral knee flexion contractures.
Case 2
Our second case was a 6-month-old infant with arthrogrypotic syndrome in addition to corpus callosum agenesis, mental motor retardation, and optic defect. In the prone position, she could turn her head bilaterally. Motor development level was 5 according to GMFCS. There was pes equinovarus on the right side and pes planovalgus on the left side; also bilateral knee flexion contractures were observed.
Assessment protocol
The universal (standard) goniometry has been used by physiotherapists to measure joint range of motion and decide limitation. The intertester and intratester reliability of the universal goniometry were found to be high, 6 and also its validity for the knee is established. 7 During measurements, the center of the fulcrum of the goniometry was placed over the lateral condyle of the femur. The proximal arm was aligned with the lateral midline of the femur, using the greater trochanter for reference. The distal arm was aligned with the midline of the fibula using the lateral malleolus and fibular head for reference and the maximum degree of extension attained was measured in degrees. 8 All measures of knee range of motion were carried out by experienced physiotherapists who were also co-authors (G.G. and S.E.). For the measurement to be precise, the infants were held in the prone position at the edge of a treatment table and supported at the hip by S.E. while G.G. passively brought the infants calves from 90° flexion to the maximum degree of extension attained and carried out the measurement as described.
GMFCS divides subgroups according to individual functional levels, thereby analyzing the child’s ability in defined age groups. According to this system, the first level includes children who walk without restrictions; second level includes children who walk without assistive devices with limitations in walking outdoors and in the community; third level includes children who walk with assistive devices with limitations in walking outdoors and in the community; fourth level includes children who have self-mobility with limitations, children are transported or use powered mobility outdoors and in the community; and in the fifth level, self-mobility is severely limited, even with the use of assistive technology. GMFCS has been shown to be a valid and reliable method in determining children’s ambulatory ability. 9
Current treatment options
In the treatment of joint contractures, physiotherapy and splinting are important as well as orthopedic surgery. 10 Despite serial casting being a common method used for hand and foot deformities, its effectiveness in the long term is controversial.4,5 In most cases, orthopedic surgery is required in the long term. However, the severity of the contracture affects the success of surgery.
Contractures in arthrogrypotic syndromes are structural contractures that include cutaneous along with subcutaneous and muscle tissue, and serial casting has been shown to be helpful.3,11
Serial casting is a method commonly used to improve contractures and maximize range of movement. 4 This intervention can be preferred especially in very young children to create tension, which can be tolerated for long periods. However, for serial casting method can also cause atrophy and shortening in the antagonist muscle. 12 Therefore, the patients should be carefully supervised. While in serial casting to remove the cast is impossible, in serial splinting you can take off the splint whenever you want for care and exercises.12,13 Although stretching of joint contractures by means of serial splinting is advocated in many textbooks, we have not come across studies explaining the application procedures in detail and giving numerical values attained by means of this application. Serial splinting is not an innovative procedure; however, its use for treating flexion contractures in the arthrogrypotic knee joint has not been investigated. Physiotherapy including exercises and activity training is also important.
The aim of this study was to present our serial splinting protocol and to investigate its effectiveness in two children with bilateral knee flexion contractures due to arthrogrypotic syndrome.
Our treatment protocol
Serial orthotic treatment was applied to infants to decrease bilateral knee flexion contractures. Although serial orthoses have been used to treat contractures and deformities, we did not come across any study in which serial orthotics was used to treat knee flexion contractures of arthrogrypotic syndromes in such young children. Before each intervention, cast measurement was taken in the maximum passive extension degree attained. After required corrections were made on the positive model, a static knee orthosis from the inguinal area to proximal of malleolar area was molded on this positive cast model by using low-density thermoplastic material that was heated in hot water at 80°C–90°C for 5–7 min (Figures 1 and 2). Orfit of 3 mm was used. This material was chosen because it is nonallergenic and easily tolerated by little children. Unlike the plaster cast, parents can take off this splint whenever they want for general care, hygiene, and exercises. The knee orthosis was renewed by taking measurements at approximately 15- to 30-day intervals. If knee extension limitation was the same following two consecutive measurements, serial orthotic treatment was terminated.

Positive cast model.

Static knee orthosis.
The infants first wore their orthoses under the supervision of the physiotherapist. After the physiotherapist was convinced that there were no problems due to compromise of circulation, instructions were given to the family about donning and doffing the orthosis and how to care for the orthosis and how to be aware of any circulation problems that could occur. The infants’ parents were advised to put on the orthosis for 15–18 h a day and to take off the orthosis when the child was active during daytime. At each control, the range of passive knee extension was measured and recorded by the same physiotherapists. The families were asked to write down how many hours the orthosis was worn each day. This study was approved by the Experimental Ethics Committee of the University of Hacettepe.
Findings and outcomes
Case 1
Serial splinting was started in the left knee. When a decrease in limitation was observed, serial splinting was also started on the other side. Increase in range of movement with serial orthotic treatment was 40° for the left knee, 35° for the right knee, and the child gained active head control in all positions and began to cruise. Change in knee extension limitation for both knees with each orthotic intervention session and average orthotic usage time is shown in Table 1. Right and left knee extension limitation alteration with time is displayed in Figure 3.
Change in knee extension limitation with orthotic intervention session and average daily orthotic usage time (case 1).
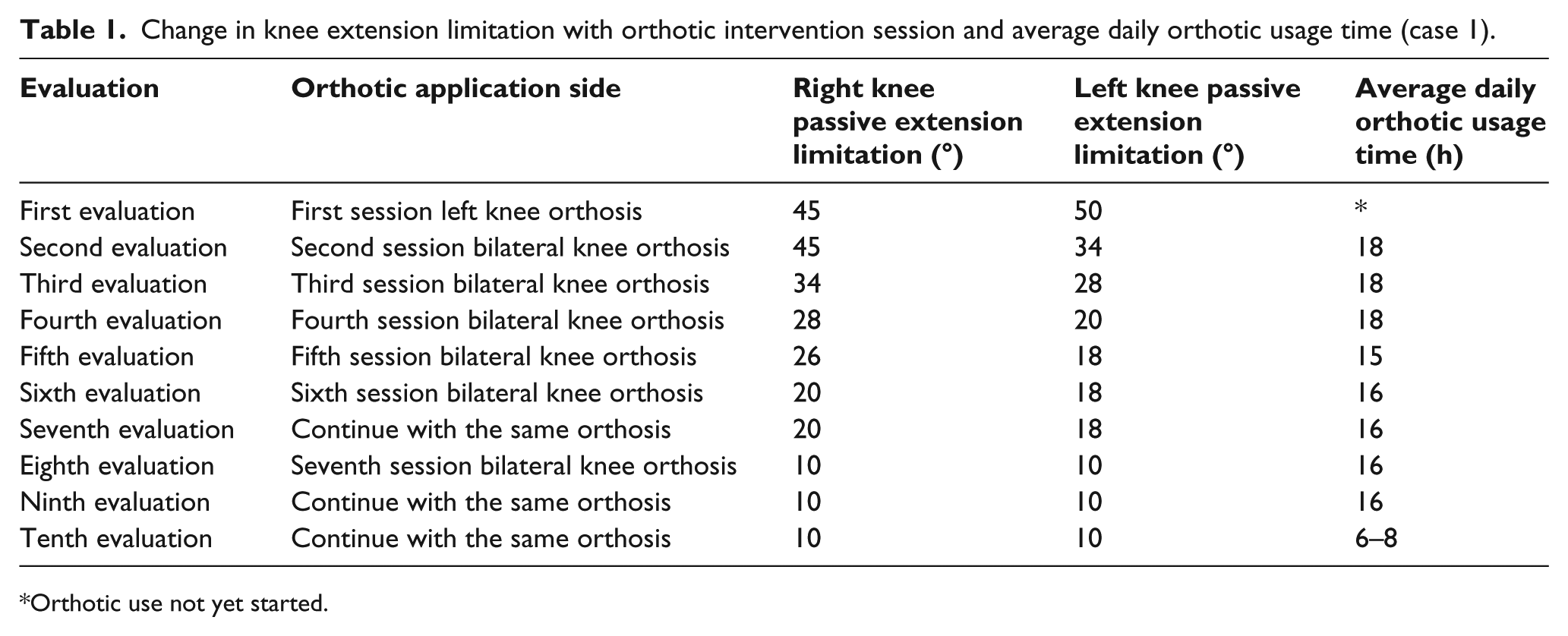
Orthotic use not yet started.
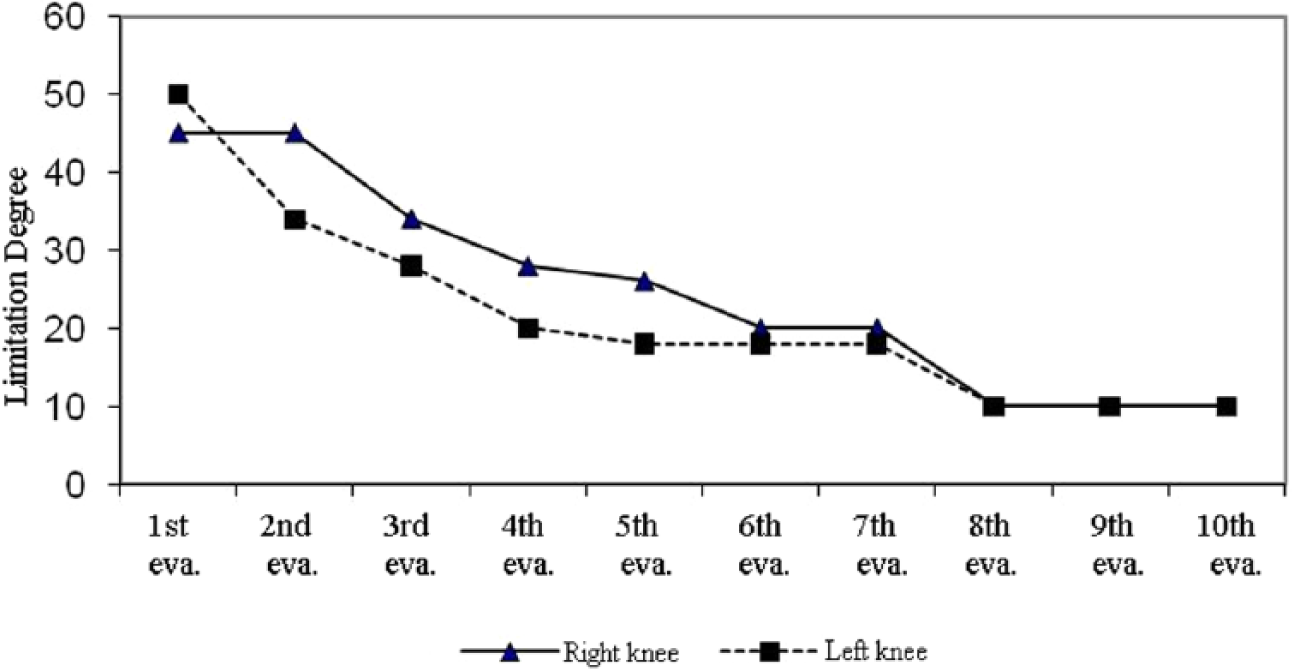
Right and left knee extension limitation alteration with time (case 1).
Case 2
Serial splinting was started with the left knee, and when a decrease in limitation was observed, serial splinting for the other side was added. The increase in range of movement with serial orthotic treatment was 25° for the left knee and 20° for the right one. Change in knee extension limitation with the orthotic intervention session and average orthotic usage time is shown in Table 2. Right and left knee extension limitation changes with time are displayed in Figure 4.
Change in knee extension limitation with orthotic intervention session and average daily orthotic usage time (case 2).
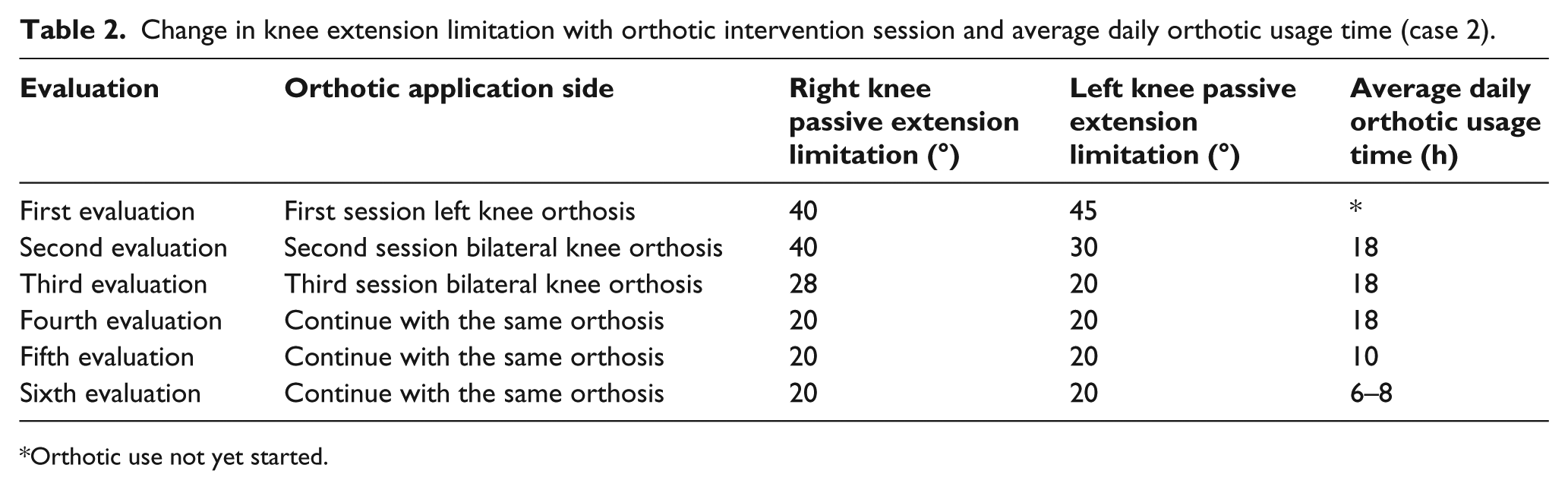
Orthotic use not yet started.
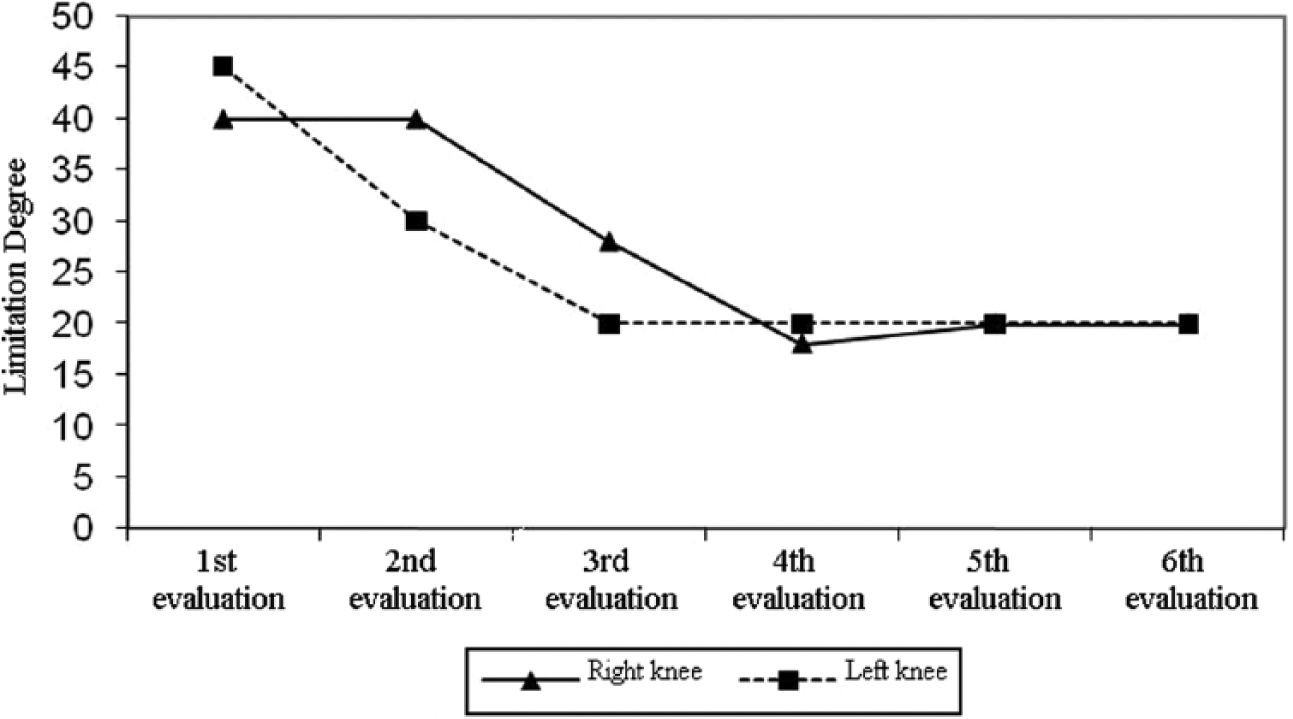
Right and left knee extension limitation alteration with time (case 2).
At the end of serial orthotic treatment, improvement in bilateral passive extension limitation was achieved in both the cases. For the first case, the increase in passive range of extension was approximately 40°, for the second case it was 25°. When knee extension limitation was the same at three consecutive measurements, the value was accepted as the maximum degree of passive extension range, and serial orthotic treatment was terminated. However, to protect the range that was attained, the parents were advised to continue using the orthosis during naptime.
Discussion
Although serial orthotic treatment is not an innovation, our study is the first study which investigates the effectiveness of serial orthotic treatment in knee contractures in two cases with arthrogrypotic syndrome.
The main goal of initial treatment in arthrogrypotic syndrome is to protect range of joint movement and to prevent contracture development during growth. 3 In the literature, the timing of surgical and conservative treatment is controversial. In case conservative management fails to treat the flexion contracture, surgery is recommended. 10 Most physicians agree that surgery should be recommended when conservative management fails to treat the contractures.10,14,15 However, some physicians believe that time should not be lost by conservative treatment and that the initial treatment should be surgical.
In conservative treatment of the lower extremity, passive stretching, serial casting,3,10 and various foot and ankle orthoses are used. 16 In the long period, surgical intervention seems to be inevitable. 10
With multiple orthopedic and rehabilitative interventions, the ability to walk and perform activities of daily living has been reported to be as high as 85%. In adult life, the majority of individuals need assistance with daily living. 3
Studies related with correction of knee flexion deformity usually compare results of surgical intervention.10,14,17 Studies that investigate the effectiveness of conservative treatment in improving knee contractures are sparse.15,17 Choice of treatment method depends on degree of deformity and level of ambulation. 18 A study showed that nonoperative treatment (including serial casting and manipulation) had good results up to 62% in extension contractures of the knee. 17 However, in another study carried out on 43 patients, a total of 78 knees with arthrogrypotic syndrome, only 6° increase was achieved in knee range of motion with nonoperative treatment. 15 In arthrogrypotic syndromes, knee joint involvement has been reported in 70%, with flexion contractures being most common, followed by extension contractures. 16 There are some studies in which the incidence of flexion contractures of the knee is as high as 90%, 10 and according to most researchers, conservative management of flexion contractures is more difficult than extension contractures.14,15,17 In a study by Hosny and Fadel 14 , all patients with arthrogryposis were treated initially by physiotherapy and splintage which was successful in all except one patient in the extended-knee group, whereas only 7 of 26 knees responded to physiotherapy and splintage in the flexed-knee group. 14 In our study, the decrease in knee flexion contracture was up to 80% in both the cases. Also, our first subject could not achieve a long sitting position before treatment; with increase in knee extension, she could sit in the long sitting position and began to cruise.
In patients with arthrogrypotic syndrome, muscles do not have enough growth potential, and bone growth will cause tightness in the muscle and consequently recurrence of the deformity.17,18 Continuation of the use of orthoses and splints even after contractures improve is required because of high recurrence rates. 10 Continuity of using orthosis is also important for surgical intervention. By using an orthosis for adequate periods and maintaining deformities at minimal degrees, less aggressive procedures can be realized. 14 In our study, the first case continued to use her orthosis 4–6 h a day for 6 months, and after 1 year, the range of motion in the knee joint was maintained. However in the second case who gave up using the orthosis, there was a recurrence in extension limitation.
Serial orthotic treatment has been reported to be costly and time consuming. 13 Yet, serial orthotic treatment is preferable to serial casting because it is possible to take off the orthosis and control the extremity, it provides active participation of the parents by allowing them to do exercises which will facilitate motor development, and it is easier to tolerate by infants and compromise of circulation is minimized.
Conclusion
Our study was the first study to investigate the effectiveness of serial orthotic treatment in knee contractures due to arthrogrypotic syndrome in two infants. With orthotic treatment, case 1 gained 75° and case 2 45° in knee range of motion. It is not possible to generalize the results; however, our results imply that serial orthotic intervention can be preferred in patients at the preoperative period or in patients who cannot be operated on. Close collaboration with the doctor who has undertaken the treatment of children with arthrogrypotic syndrome is a prerequisite of successful treatment.
Footnotes
Author contribution
All authors contributed equally in the preparation of this article.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.