
Abstract
Background:
There is a paucity of evidence regarding the design of children’s footwear in relation to musculoskeletal structure.
Objectives:
The aim was to gain consensus regarding where flexibility and support should be given on a school shoe for the 6- to 10-year-olds.
Study design:
Delphi Questionnaire.
Methods:
Recruitment of 10 Allied Health Professionals yielded a consensus group. Those recruited had dedicated experience in paediatrics and foot health. Rounds of questions were delivered to investigate the basis of the opinions made by the group on the location of support and flexibility in a school shoe for the age range identified.
Results:
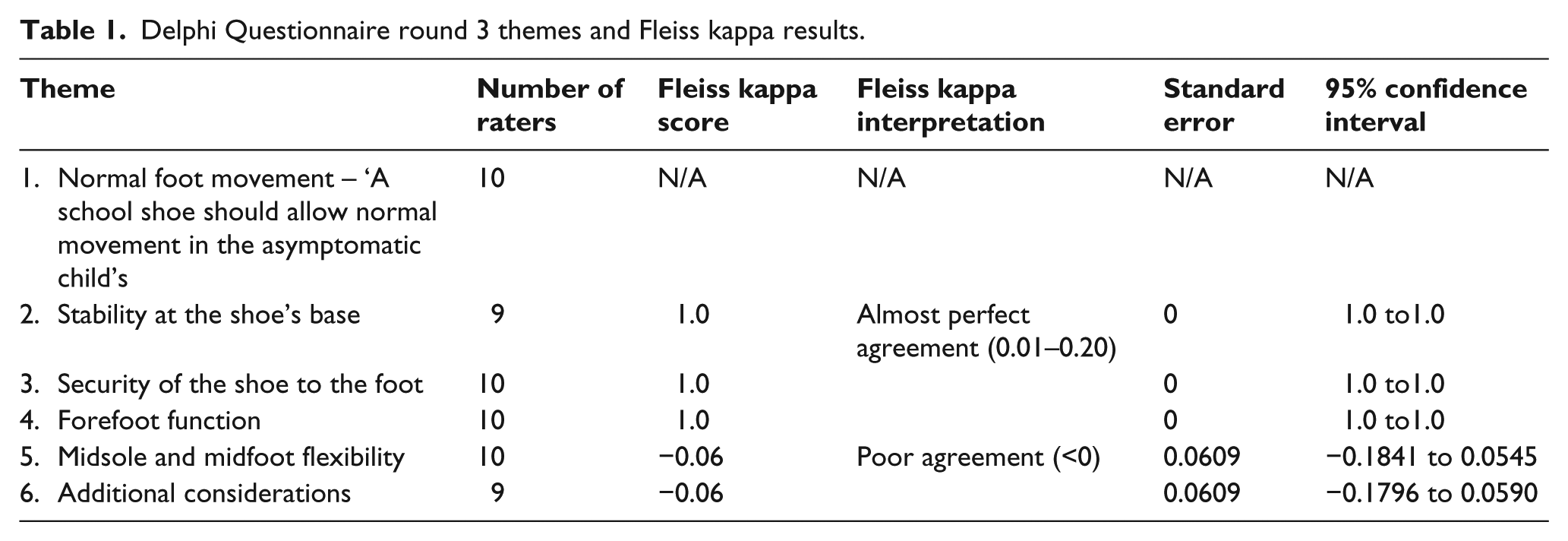
Six themes were generated. Four themes gained 100% consensus regarding footwear allowing normal foot movement, footwear allowing normal forefoot function, footwear providing a stable base and the foot being secure in the shoe. Fleiss’ kappa calculations revealed ‘poor agreement’ for the remaining two themes regarding clinical intervention and the purpose of footwear design in the midfoot in both the upper and sole of the shoe.
Conclusion:
The qualitative data generated through discussion have highlighted areas where more understanding and research are required, particularly in understanding how, in the long term, shoe design can affect the developing foot.
Clinical relevance
Children’s footwear advice is often delivered from experience and personal belief. This article questions current understanding and opinion from clinical experts in the field of paediatric footwear and highlights that there is a lack of knowledge and confidence into the effects of children’s footwear. There is a strong requirement for further empirical research to be completed on children’s footwear to allow clinicians to formulate relevant and appropriate footwear advice.
Background
Allied Health Professionals (AHPs) and parents have broad concerns regarding children’s footwear; yet there is a limited pool of research on children’s shoes to address the many questions asked. Poor fitting footwear has been attributed to painful musculoskeletal foot pathologies in children. 1 Comfortable, correctly fitted shoes have been shown to have a therapeutic benefit. 2 Wearing shoes has been found to affect the function of children’s feet, yet the effects of this are unclear.3–6 A child wearing flexible shoes so as not to impose natural foot function has consequently been an area of research interest. General research into the effects of footwear has focused on sporting and orthopaedic styles, with the populations studied being either athletes or elderly.7,8
Children’s feet are different to adults due to age-related changes. For example, children grow, skeletal proportions flux and the neural system matures.9 –11 Little is known about how external factors such as footwear influence the growth and development of the foot. It is understood that the maturing foot must independently accommodate load through its structures in stance and dynamic gait through a number of internal physiological and mechanical mechanisms. 12 The use of footwear in children has been shown to influence gait patterns by encouraging a rearfoot strike (in running), increasing walking speed and step length which consequently adjusts the kinematics at the ankle and knee.13,14
Historically, children’s footwear has been used therapeutically. This was based on the theories that applying external compressive and tensile forces had the ability to create or correct deformity. These concepts formed the basis of the corrective shoe, that is, one that could aid arch development and prevent deformity. 6 The use of footwear, however, has been linked to lower foot arches,9,10 and studies have demonstrated that arches develop regardless of corrective footwear.15,16
Footwear today is manufactured with fashion in mind, using low-cost materials and arguably compromised quality and construction; therefore, the emphasis on foot health and function is restricted.3,6,17,18 It is questionable whether footwear manufacturers, consumers and health professionals adequately collaborate to consider the other potential effects footwear could have on the developing foot and what these changes mean in the mid to long term.3,13
The research question was set with the aim to better understand opinion on footwear design in relation to the function and development of children’s feet. 14 The primary objective was to gain a consensus on where a school shoe for the 6- to 10-year-olds should provide flexibility and support using a Delphi Questionnaire (DQ) method. The expertise of AHPs such as podiatrists, physiotherapists and orthotists was selected to initiate and foster debate in this area. Secondary objectives were to gain the information that formed the basis of the opinion, identify a design criterion and identify variances of opinion between professionals.
Methods
Prior to commencing the study, appropriate ethical approval was granted via Staffordshire University’s Ethical Committee with additional approval from the National Health Service’s National Research Ethics Service (11/YH/0249) via the Integrated Research Application System.
A DQ design was chosen since this design has been shown to be an advantage in areas of little research and has also been favoured in previous studies on footwear (Table 1).19,20 This approach involves delivering rounds of questionnaires. The first questionnaire (DQ1) generates ideas and gathers information on the research question, the second (DQ2) shares information and encourages reflection and the third round (DQ3) consolidates themes and related statements to generate consensus.
Delphi Questionnaire round 3 themes and Fleiss kappa results.
The questionnaire’s focus was on ‘support’ and ‘flexibility’ which were based on the foot’s main mechanical functions: a load bearer, rigid lever and a mobile adaptor. 12 It also reflected the current research interest. 14 A school shoe was chosen to define purpose and requirements of use. 21 It was not specified by brand, style or type. With the intention to form a basis for future research, the ‘normal’ child was selected, that is, one without symptom and pathology. 22 Gender was set to consider both males and females. The age range was set according to the approximate onset of gait and arch maturation and prior to growth spurts. 22
Participants
A heterogeneous sample, confined to relevant AHPs (podiatrists, orthotists and physiotherapists), was selected as footwear opinion can polarise between professions. 17 The inclusion criteria followed the DQ recommendations of knowledge and experience in the area; capacity, willingness and time to participate and effective communication skills. Recruitment aimed to ensure external validity in the clinical community, to increase idea generation and decision quality and to reduce group error. Sample sizes are not calculated in DQs. 23
To avoid researcher bias, prospective participants were recruited indirectly by email via national paediatric interest groups, known National Health Service Managers and through recommendation. The recruitment email contained information on the research question and process, consent form and the first questionnaire. All study contact and correspondence was via email. To allow freedom of expression and avoid bias, the questionnaires were self-administered and participants were offered complete anonymity. Participants remained anonymous to each other throughout the rounds.
Analysis
The study generated a lot of qualitative data as each round offered the opportunity to debate and provide additional thoughts and information. Following idea generation in round 1, round 2 channelled discussion through closed question statements and was rated using a Likert scale. Round 3 defined six themes with associated statements directed by the high-scoring responses in round 2. This provided a fixed number of raters with nominal scale ratings to employ analysis using Fleiss’ kappa, a measure of the degree of agreement in classification. This assessed the reliability of agreement between raters for each of the themes with over one statement.24,25
Results
Two rounds of recruitment of the AHPs – podiatrists, orthotists and physiotherapists – yielded a consensus group of 12 podiatrists and 1 orthotist. Three highly experienced paediatric physiotherapists were contacted to explain they could not provide specialist opinion on footwear. Despite little representation from orthotists and physiotherapists, the study continued to avoid participant attrition.
One participant opted out on each round. The final consensus round included nine podiatrists and one orthotist, which included experience in leading a clinical paediatric service (8), lecturing in paediatrics (3) and professional qualifications of MSc (8), MPhil (1) and PhD (1). The study design prevented calculation of response rate.
Full consensus was generated in four themes, these included the following: the shoe ‘should have a stable base’, ‘have a fastening mechanism’, ‘should allow normal foot movement’ (Theme 1) and ‘footwear should allow normal forefoot function’. The latter two were qualified with the statement ‘when shod, the kinetics and kinematics are comparable to barefoot data and the activity being undertaken’. 14
Discussion
The primary aims of the research design were to generate information, ideas and discussion to facilitate consensus on the research question. The results provided enquiry and concepts for footwear design in children. Novel items were generated and developed through the iterative process of the study. Some of the information collected supported previous publications.6,14
Seminal work by Staheli 6 proposed that footwear should be well fitted, quadrangular, lightweight and flexible to allow the foot to develop naturally without harm. This standpoint initiated biomechanics research into the flexible shoe design with the understanding that natural foot function was conductive to good foot health. In Theme 1, the consensus group agreed that ‘normal movement’ was not detrimental to foot health. Normal was defined as when shod, kinetic and kinematic data were comparable to those of barefoot and the activity being undertaken. 14 Interestingly, footwear allowing normal 1st metatarsal phalangeal joint movement (Theme 4; Table 2) gained consensus in DQ2, whereas normal foot movement in general was gained later in DQ3. Discussion was limited by not discussing the tolerance of ‘normal movement’. The group acknowledged that a flexible shoe design cannot eliminate unnatural factors. It is biomechanically impossible to achieve natural gait in shoes because foot stance, postural alignment, balance, sensory stimulus and weight distribution are all influenced by shoes. It is therefore conceivable that these factors can have an effect on the development of the foot. It is also possible that these factors could enhance development in a given environment.26,27
Theme 4 – forefoot function.
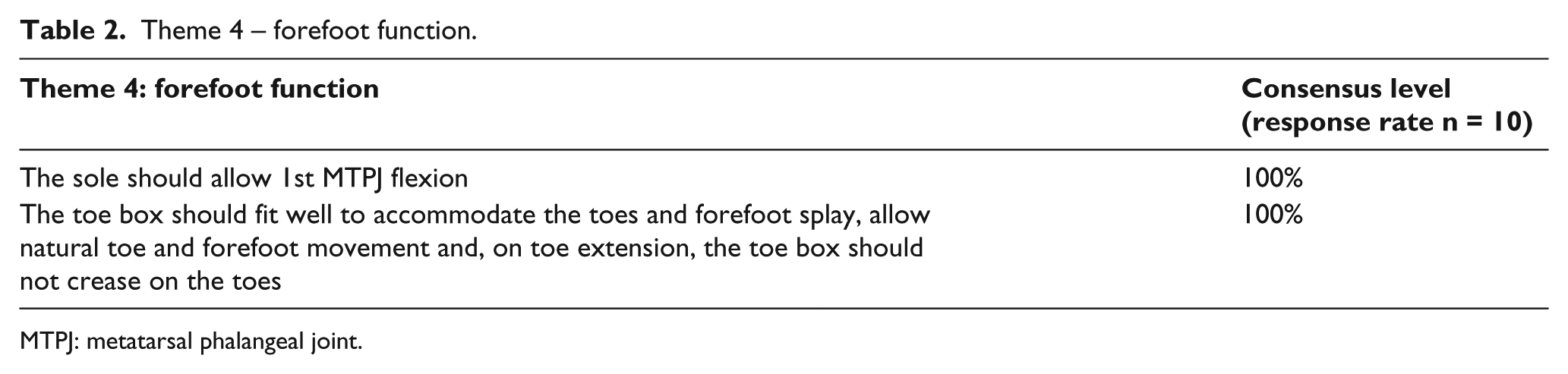
MTPJ: metatarsal phalangeal joint.
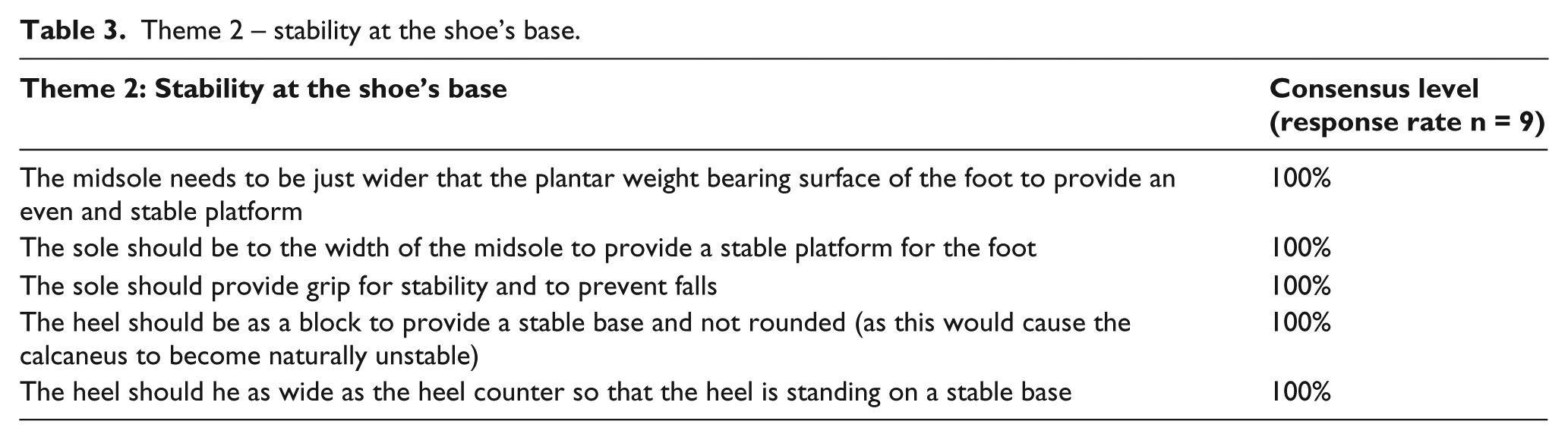
A healthy foot should distribute load independent of footwear. 12 Theme 2 (Table 3) consensus levels supported this notion through the provision of a shoe with a stable or neutral walking base, that is, the base/sole of the shoe would not interfere with natural load distribution. The group did not discuss the effects of unstable footwear.28,29 Full consensus was gained on grip of the shoe associated with stability which corresponds with the association of falls and children’s footwear 30 and sole design. 31 The group therefore agreed that the sole should provide stable support and grip for children. Discussion was limited in terms of grip design and sole material.
Theme 2 – stability at the shoe’s base.
All participants advocated for footwear. Barefoot walking at home was promoted to encourage natural walking by one participant. Similarly, discussion explored that shoes and a stable walking base would not provide sensory feedback from the variable surfaces experienced when barefoot. Paediatric research so far has concentrated on comparison of gait parameters on flat man-made surfaces versus shod condition, 14 which arguably does not reflect natural walking and mechano-sensory feedback. Similarly, discussion questioned whether shock absorption inhibited neural and bone maturation. Contoured insoles as an interface between the foot and the shoe were deliberated. The content reflected on the adult population where evidence exists for their use in perceived support and reducing foot eversion. 32 The need for correct fit and comfort was a key concern for group members when considering a generic contoured design. The impact of variable contact surfaces during gait in children is an area of little research, and further work would improve understanding.
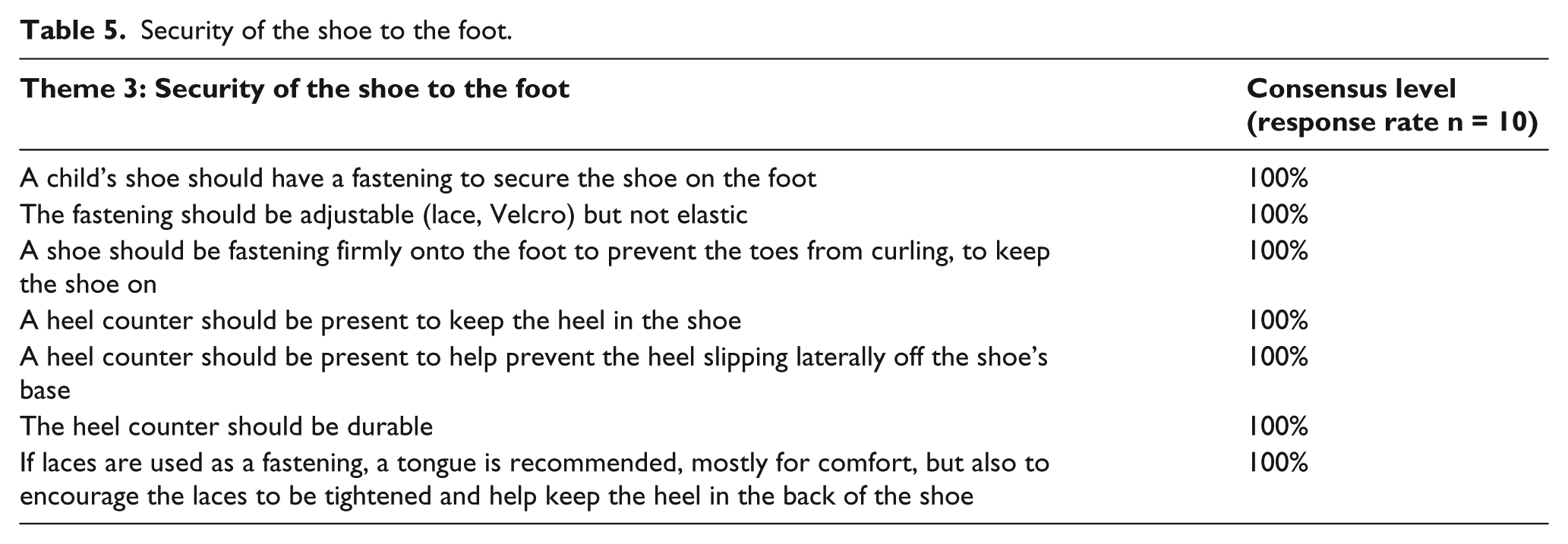
The group held the opinion of previous research that corrective footwear, heel cups and insoles do not influence children’s arch development. 15 Within Theme 5 (Table 4), the participants’ focus diverted from arch development towards midfoot function. How the shoe at midfoot should be designed with respect to foot function led to a poignant discussion within the group, despite failing to achieve consensus. This included both the upper shoe in terms of the fastening mechanism and the stiffness of the vamp, to the lower components of the midsole (in the midfoot region), shank and sole, a concept discussed by Wolf et al. 14 It was recognised by the group that the act of wearing shoes would influence foot motion but a stiffer, less flexible material would limit motion.4,33 It was queried whether stiffness was needed to protect the midfoot area, whether footwear (and even orthotics) could protect the internal structure of the foot and also whether motion control, and to what level, was safe for the developing foot. Some participants reasoned that walking on hard man-made surfaces, which imparts unnatural gait, required an alternative perspective to natural walking principles. The controversy surrounding midfoot function resulted in Theme 3’s (Table 5) statements being related only to the security of the foot to the shoe, not motion control. Research demonstrates that loose laces are associated with the foot slipping in the shoe and changes to plantar pressure and load distribution. 34 Fastened laces have the capacity to reduce pronation velocity and shock when running. 35 Children’s sport’s footwear has been found to increase power and potentially overuse pathologies at the ankle as a result of decreased power at the midfoot.4,5 Midfoot pathologies of proposed mechanical influence are a common finding in the adult population.9,36 Therapeutic footwear which is inflexible at the midfoot can be used to improve foot pain. 2
Theme 5 – midsole and midfoot flexibility.
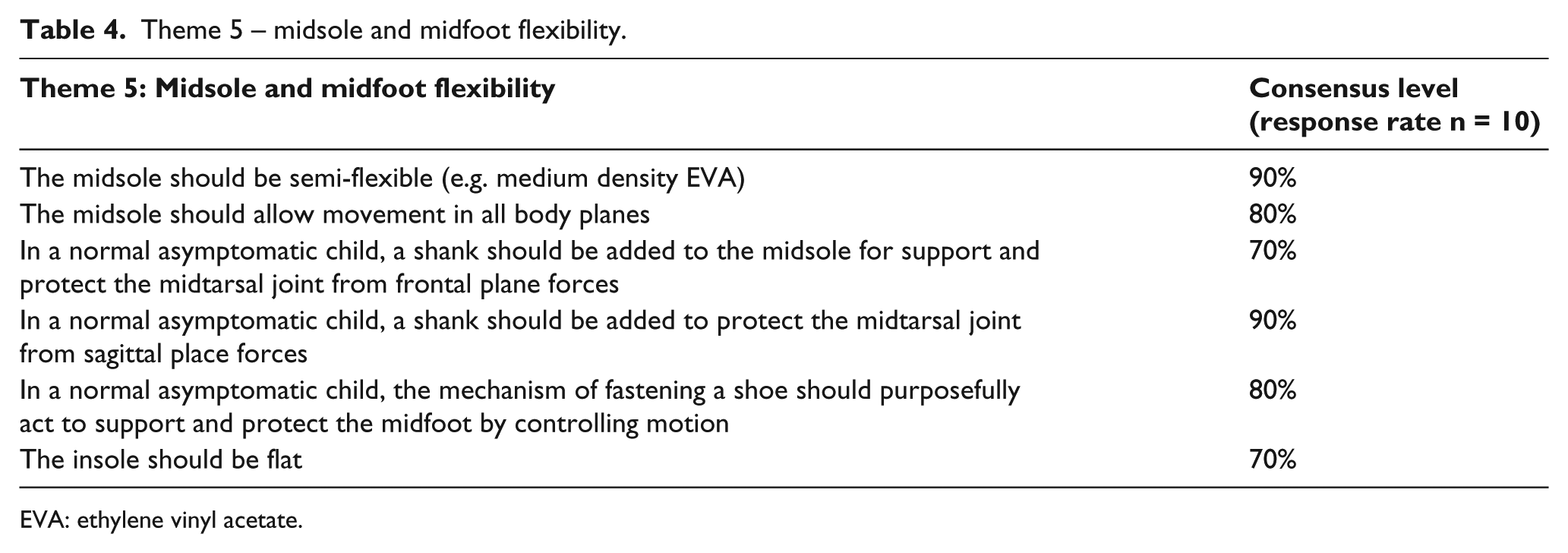
EVA: ethylene vinyl acetate.
Security of the shoe to the foot.
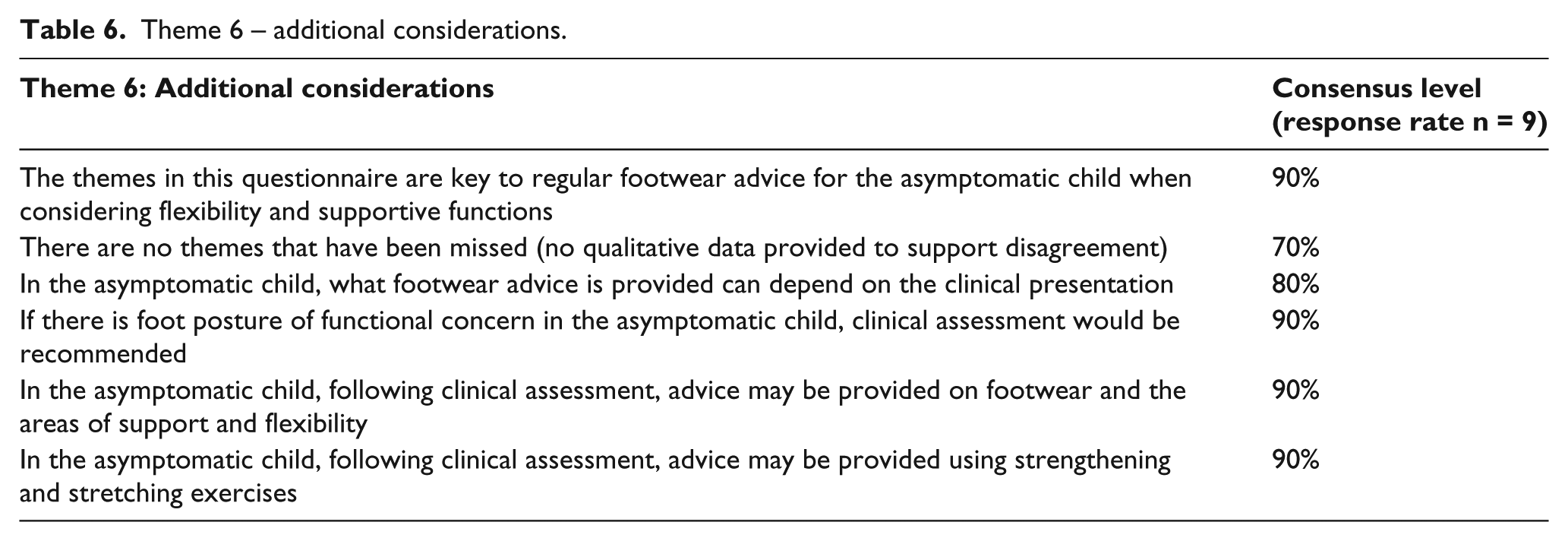
Theme 6 (Table 6) was created for clarification. The results emphasise that there was more information available to discuss. It also suggests that referral criteria and clinical interventions can vary and are dependent on the clinician. Participants’ final reasons for decisions were unclear, as closed questions were not supported with detail. Discussion was limited, which suggests fatigue and or reluctance to debate the differing practices. Participant fatigue is a shortcoming of the DQ process. 23
Theme 6 – additional considerations.
Limitations and recommendations for further work
The Delphi method cannot replace quantitative and rigorous scientific research and cannot be authoritative. 23 Not all opinions were substantiated with previous research evidence or published information in the public domain. Further research would be needed to explore and clarify the opinions presented. The indirect recruitment, small sample size and restricted group of practitioners could have inhibited the true flow and breadth of opinion, which in turn could have influenced the outcome of consensus levels. A larger sample of experts would have supported the themes and discussion further; however, extensive efforts were made in recruiting subjects, and it was felt that the smaller group recruited was a reflection of the lack of confidence to speak out about knowledge and understanding of children’s shoes. Further studies would benefit the involvement of a wider distribution of practitioners and non-clinical experts, such as material scientists, with related expertise to the research question. An increased interest in this area would provide a larger consortium for professional development.
Conclusion
Footwear has been linked to pathologies that cause pain, deformity and can alter function. How children’s footwear should be constructed in relation to the developing foot is a debated area with limited empirical research to support knowledge and understanding. The impact of footwear on children’s feet should be evaluated further with research from a broad range of disciplines to explain the effects footwear has on the developing foot in the mid to long term This research has added novel discussions to the debate on children’s shoes and has exposed the need for further studies to be completed.
Footnotes
Conflict of interest
All authors involved in this manuscript declare that they had no competing interests.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.