
Abstract
Background and aim:
Replacement of missing ear is a challenging task in which extensive array of materials and techniques have been employed. Materials such as silicones and methacrylate acrylic resins have been widely used for auricular prosthesis. This article describes a simplified procedure for fabricating resilient heat-cured acrylic resin auricular prosthesis, retained with a custom-made acrylic bar with ball attachments.
Case description and methods:
A male patient was reported with right ear loss. A modified technique was preferred to fabricate ear prosthesis with resilient heat-cured acrylic resin in which heat-cured acrylic retentive bar was incorporated.
Findings and outcomes:
Contrary to silicones, resilient heat-cured acrylic resin was more economical and compatible with acrylic retentive bar and resulted in a more long-lasting auricular prosthesis.
Conclusion:
Resilient heat-cured acrylic resin was proven to be a better alternative in terms of strength and durability.
Clinical relevance
This article presents an economical and simplified approach for the fabrication of prosthesis for a missing ear.
Background and aim
Facial tissue loss or defects can be acquired, congenital, tumoral lesions, or accidental. 1 Maxillofacial defects can be emotionally traumatizing considering the societal emphasis on physical appearance.2,3 It is not merely the functional loss resulting due to these defects, when an individual’s social behaviour is affected, it ultimately leads to serious psychological problems. The aim of maxillofacial rehabilitation should provide a suitable prosthesis for patients with facial defects so that they are rehabilitated back to the society to face and accept the challenges of life.4,5 It encourages the best possible quality of life and upholds their self-image during their traumatic psychological adjustment. 3 Among the large number of materials that have been tried out in the history of anaplastology, for example, porcelain, natural rubber, gelatin and latex, two have established themselves: methacrylates and silicones.6–8 Retention and stability are major concerns regarding comfortable use of a facial prosthesis. Medical adhesives, anatomical undercuts and mechanical devices like spectacles, hair bands, magnets and implants have been used to retain prosthesis. Since the introduction of percutaneous endosseous implants for use with bone conduction hearing aids in 1977, implants have acquired important role in the prosthetic rehabilitation of patients with craniofacial defects. 9 Implants can vastly improve the retention and stability of a facial prosthesis. Despite improvement in per capita income, financial consideration is among one of the prime barriers in seeking maxillofacial treatment in developing countries. This article describes a simplified and economical approach for fabricating implant-retained resilient acrylic auricular prosthesis.
Case description and methods
A 50-year-old male patient was referred to the Department of Prosthodontics in our institution with unilateral right-side auricular defect. Clinical examination revealed missing of all parts of the ear except tragus (Figure 1). The patient gave a history of a road traffic accident for his missing ear parts. The skin surrounding the ear defect was normal. His hearing was normal, without any intra-auricular problem as evaluated by speech recognition tests and signal-to-noise ratio by an otorhinolaryngologist. Two endosseous percutaneous 8 mm × 3.5 mm hydroxyapatite-coated cylindrical implants (Nobel Biocare Management AG, Postfach, Zurich-Flughafen, Switzerland) were placed in the mastoid area with the aid of a surgical guide. Five months later, after confirmation of osseointegration and healing of surrounding soft tissues, the second-stage of surgery was performed to accommodate 4-mm ball attachments. After the complete healing of the surgical site, an impression of the defect area was made, and a working model was produced. Earlier, a silicone auricular prosthesis (2186; Factor II Inc., Lakeside, AZ, USA) was fabricated in which a custom-made self-cure acrylic bar was made to receive the matrix part of the retentive system of implants. However, due to incompatible bonding between silicone and acrylic resin, the silicone prosthesis got torn from the junction of acrylic bar (Figure 2). To resolve this problem, we planned a resilient heat-cured acrylic (‘Super Soft’ Resilient Denture Liner; GC America Incorporation, Alsip, IL, USA) ear prosthesis in which heat-cured acrylic (Trevalon; Dentsply, York, PA, USA) retentive bar was incorporated. As these two materials were chemically bonded with each other, it provided us a successful alternative.

Auricular defect and implants with ball attachments.

Torn silicone prosthesis.
Written informed consent for participation and publication, including publication of photographs of participant, was obtained and the research was approved by Ethics committee, Research cell, King George’s Medical University, Lucknow, Uttar Pradesh.
The patient was isolated, and his hair was protected by surgical cap covering the hairline. The impression procedure was explained to the patient to make him comfortable. External auditory canal was blocked with gauze to prevent entry of impression material. Impression of the auricular defect was made using irreversible hydrocolloid (Algitex; Dental Products of India (DPI), Mumbai, India) following a modelling wax box method (Figure 3(a)). 10 Gauge pieces were used for reinforcement, and quick setting plaster of Paris (Kaldent; Kalabhai Karson Pvt Ltd, Mumbai, India) was added for backing. Impression was removed, boxed and poured in type III gypsum material (Kalstone; Kalabhai Karson Pvt Ltd, Mumbai, India) (Figure 3(b)). A custom-made heat-cured acrylic bar was fabricated on the stone model of defect over the implant abutments. A donor of similar age and build was used as an ear model. Impression of model ear was made with alginate and poured in modelling wax (Deepti Dental Products, Ratnagiri, India). The model wax pattern was adapted to the stone model over the acrylic bar and modified in such a way that the patient’s normal ear was duplicated as closely as possible. Wax pattern was verified for accurate fit and orientation in all dimensions (Figure 4). Proper placement of the auricular prosthesis is achieved by assessing its axis, level of the prosthesis and distance from orbit. It is difficult to exactly define the positioning of the axis, but it can be described as the ‘Line of Balance’ through the long dimension of the ear. An angulation of 20° from vertical position seems satisfactory. Level of the prosthesis should be assessed with the head in the anatomic vertical position. The highest part of the helix is on a line roughly with that of the eyebrow, and the lowest part of the lobule is on a line at the base of columella or slightly below that. The ideal distance of the prosthesis from the lateral orbital rim is about one ear length, or 6.5–7.5 cm. The patient’s feedback were also taken regarding any modification in pattern. Finally, it was roughened with the help of gauge piece to simulate the skin texture. The sculptured wax pattern along with acrylic bar was embedded in a three-piece mould of dental stone. After complete dewaxing of the mould, the exposed surface of the acrylic bar was roughened with carborandum stone burs. The pink-coloured acrylic resin was mixed with colouring agents to create a base colour to match the skin tone. The base colour was selected using trial-and-error method by making different custom shade tabs (Figure 5(a)). Opinions from various clinicians (e.g. prosthodontists and surgeons) and the patient’s family were solicited regarding the best colour-matched shade tab. The mould was painted with separating media, and base-coloured resilient heat-cured acrylic was packed in dough stage (Figure 5(b)). Two halves of the flasks were closed and allowed to cure in long curing cycle. After bench cooling, the completed prosthesis was retrieved carefully from the mould and cleaned. The mould of the auricular prosthesis remained intact in the flasks. Extrinsically, the prosthesis was custom-stained to match the patient’s skin tone under various light conditions (Figure 6(a) and 6(b)).The ear prosthesis was adjusted three-dimensionally (Figure 6(c)). The patient was instructed to care for the skin around the abutments and the auricular prosthesis. Proper care and maintenance of both tissue and prosthesis hygiene were emphasized. He was advised to remove the prosthesis at night, wipe the internal component with a dry soft cloth and keep it free from dirt and ear wax. A small brush and wax-removing tool for cleaning the vent was given to clear the wax. The patient was advised not to use hair oil, creams and so on with the prosthesis seated as they can clog the vent. He was advised to avoid excessive exposure to the Sun to prevent discolouration of the prosthesis. He was examined for swelling and soreness in the skin surrounding his ear after wearing the prosthesis. He came for recall till 3 years, and the result was satisfactory.
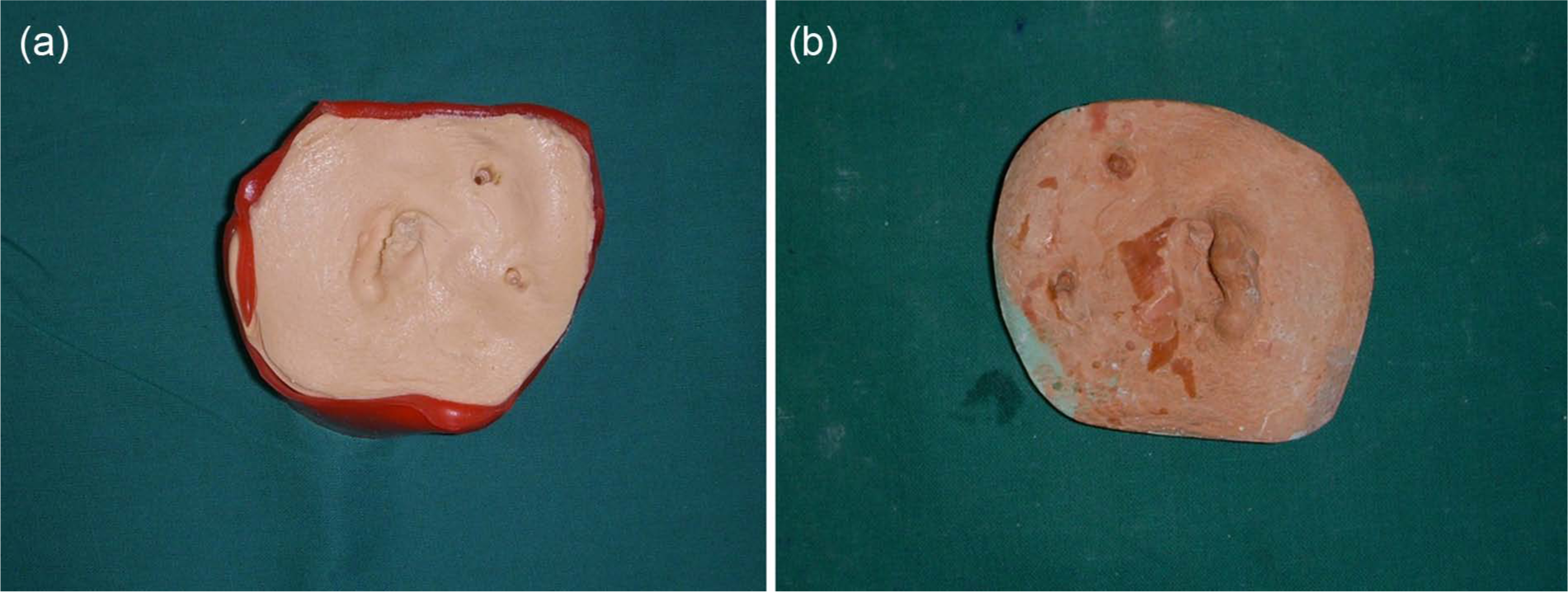
(a) Impression of auricular defect; (b) stone cast.

Wax pattern verification.
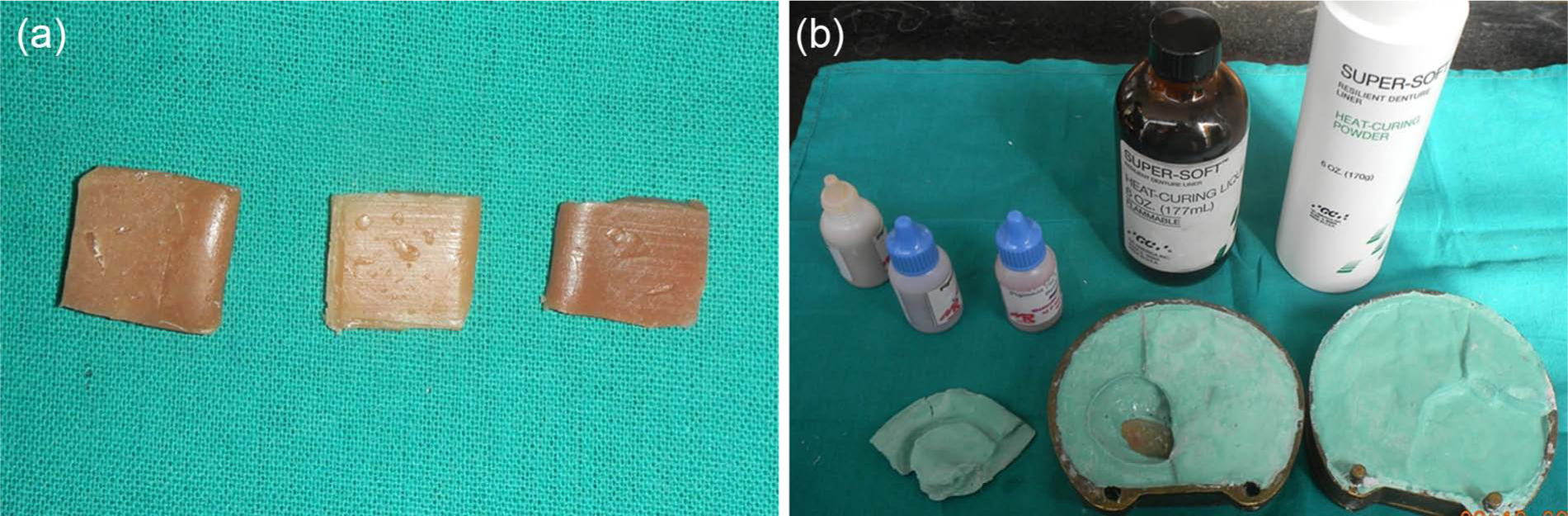
(a) Custom shade tabs; (b) processing of prosthesis.
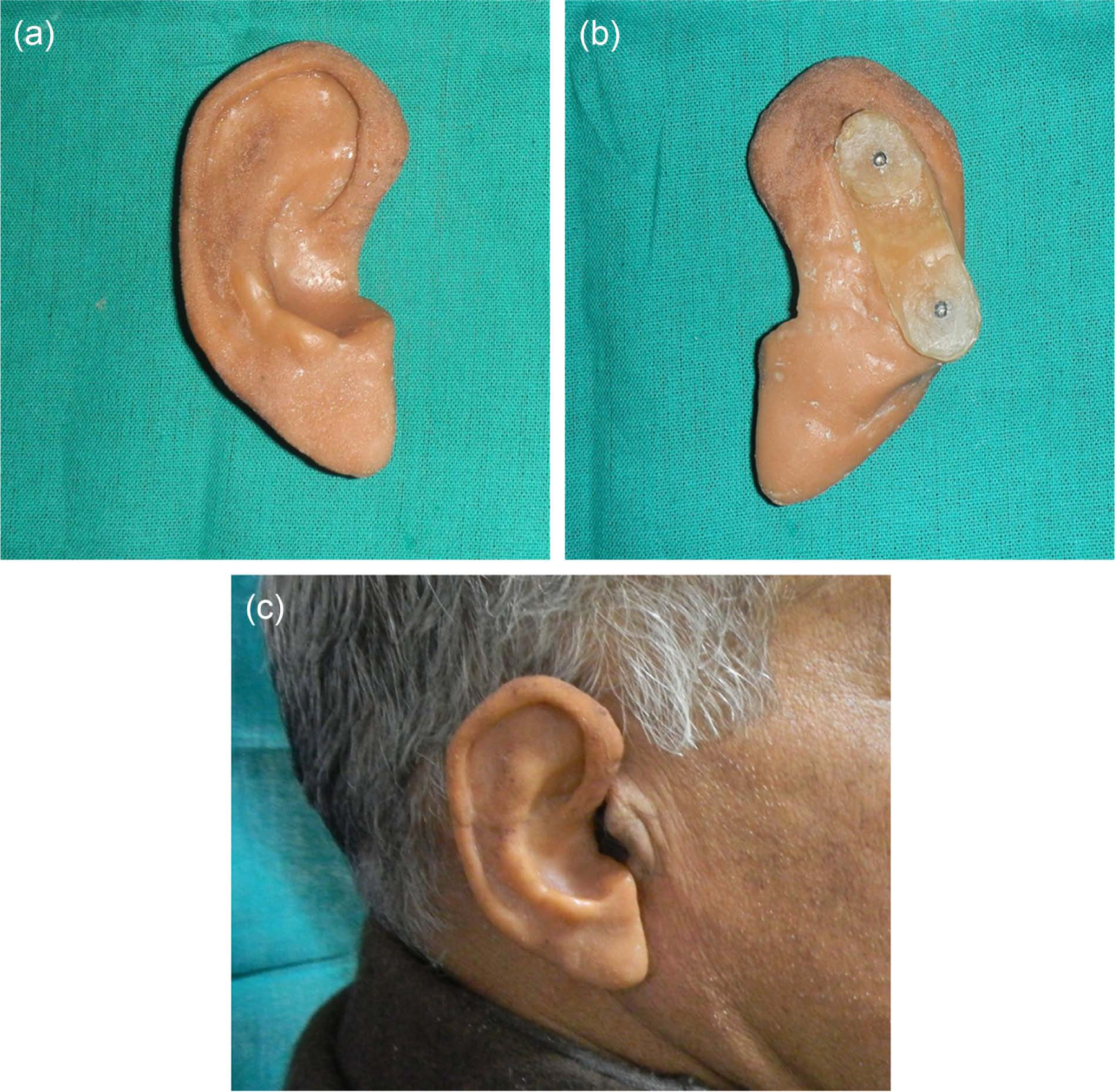
(a) Outer surface of processed and finished prosthesis; (b) inner surface with retentive bar; (c) patient with accurately fitted auricular prosthesis.
Discussion
In the present case report, we preferred resilient heat-cured acrylic resin over silicones. Auricular prostheses fabricated with resilient heat-cured acrylic resin (polymethyl methacrylate (PMMA)) have advantages of being economical, better edge strength in thin lamellar parts of prostheses, chemical bonding with acrylic bar which prevents the frequent tearing problem as in the case of silicone prostheses and easy extrinsic colouration. 11 Auricular prostheses retained by custom-made heat-cured acrylic bar with ball attachments offer improved access for hygiene, less space required behind the prosthesis, choice to use either parallel or nonparallel abutments, elimination of expensive attachment components, ease of fabrication and reduced stress on the implants due to the resiliency of the silicone around the implant. 10
Although resilient heat-cured acrylic resin is less resilient than silicone prostheses, it provided satisfactory life-like appearance. The use of resilient resin prosthesis easily allows the maxillofacial prosthodontist to modify and replace it at a relatively low cost, as observed by Shipman and Bader. 12 Drawbacks of the resilient acrylic resin are an artificial effect if highly polished, and also its inherent porosity may be responsible for organic residue accumulation and growing of microorganism, in case the prosthesis is not properly cleaned. 13 The patient should be instructed to keep the prosthesis protected from Sun as much as possible to overcome one of the limitations of its material. Plasticizers impart flexibility, but they are not bound with resin mass and therefore may be leached out. As this occurs, soft liners become progressively more rigid. Consequently, it is advantageous to use liners in which PMMA is replaced by higher methacrylates (e.g. ethyl, n-propyl and n-butyl) to make the glass transition temperature progressively lower. As a result, less plasticizer is required and the effect of leaching can be minimized. 14
Conclusion
Facial deformity can be emotionally traumatizing and can eventually affect social behaviour of an individual. Rehabilitation of an auricular defect has been a challenging task. In an attempt to provide a durable, economical and cosmetically acceptable prosthesis, a resilient heat-cured acrylic resin auricular prosthesis was made that was proven to be a better substitute for silicones. Moreover, the body is the greatest asset that a soul possesses and has every right to defend and keep it in good health.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.