
Abstract
Background:
Ankle-foot orthoses are commonly prescribed in Charcot–Marie–Tooth type 1A disease to improve quality of walking and reduce the risk of falling due to the foot drop.
Objectives:
This study aimed at assessing the effect of an anterior ankle-foot orthosis on walking economy in a group of Charcot–Marie–Tooth type 1A patients.
Study design:
Within-group comparisons.
Methods:
7 Charcot–Marie–Tooth type 1A patients (four women and three men; 37 ± 11 years; age range = 22–53 years) were asked to walk on a circuit at their self-selected speeds (‘slow’, ‘comfortable’ and ‘fast’) in two walking conditions: (1) with shoes only and (2) with Taloelast® anterior elastic ankle-foot orthoses. Speed of walking and metabolic cost of walking energy cost per unit of distance were assessed at the three self-selected speeds of walking for both walking conditions.
Results:
Speed of walking at the three self-selected speeds did not differ between shoes only and anterior elastic ankle-foot orthoses, whereas walking energy cost per unit of distance at comfortable speed was lower in patients using anterior elastic ankle-foot orthoses with respect to shoes only (2.39 ± 0.22 vs 2.70 ± 0.19 J kg−1 m−1; P < 0.05).
Conclusions:
In Charcot–Marie–Tooth type 1A patients, the use of anterior elastic ankle-foot orthoses improved walking economy by reducing the energy cost of walking per unit of distance, thus reflecting a lower level of metabolic effort and improved mechanical efficiency in comparison with shoes only.
Clinical relevance
From a practical perspective, Charcot–Marie–Tooth type 1A patients with anterior elastic ankle-foot orthoses can walk for a longer duration with a lower level of physical effort. Improvements in walking economy due to ankle-foot orthoses are likely a consequence of the reduction in steppage gait.
Keywords
Background
Charcot–Marie–Tooth (CMT) disease, also referred to as hereditary motor and sensory neuropathy (HMSN), is a genetic and progressive neuropathy affecting 10–30 per 100,000 people in the world. 1 CMT type 1A (CMT1A), which is the most frequent form of CMT type 1 (CMT1; 60%–80% of total cases 2 ), is characterized by segmental demyelination, reduction in the nerve conduction velocity of peripheral nerves and consequent axonal degeneration that impair functions of the distal part of legs and arms. 3 CMT1A patients show a decline in motor performances due to loss of muscle strength,4,5 fatigue or experienced fatigue,6,7 foot and ankle deformities and alteration of balance,1,8 pain,9,10 reduction in functional aerobic capacity 11 and, as a consequence, low levels of daily activity. 12
Patterns of walking in CMT patients have been extensively described by means of motion analysis. These studies highlighted that the main limits of CMT walking are instability of the ankle in the sagittal plane, 13 increase in plantarflexion during the initial contact, 14 higher dorsiflexion during the stance phase,14,15 loss of active push off, 13 higher knee and hip flexion, 14 the asymmetric hip movement in medio-lateral plane, 16 hip elevation14,16 and decrease in hip adduction.14,16 Thus, the altered patterns of walking result in an increased energy cost of walking, which has been assessed by measuring both the mechanical displacement of the body centre of mass 14 and oxygen consumption. 17
In CMT1A patients, the ability to walk independently is the motor skill that most positively affects the perceived quality of life, as assessed by means of questionnaires. 10 Ankle-foot orthoses (AFOs) are commonly prescribed to improve quality of walking, avoid stress on joints and muscles and reduce the risk of stumbling and falling due to the foot drop. 18 Various designs, features and materials of AFOs exist although posterior leaf spring AFOs (P-AFOs) are the most commonly used. 19 Indeed, positive effects of P-AFOs on walking performance have been demonstrated in CMT patients.19–23 Walking with P-AFOs resulted in an increase in walking speed20,22,23 and step length 19 with respect to walking with shoes only. Moreover, improvements in gait kinematic have been demonstrated, such as a reduction in hip and knee flexion in the middle phase of swing21,22 and an increase in ankle dorsiflexion during the initial heel contact. 22 In a single-case study, Bean et al. 24 demonstrated that the use of a P-AFO allowed a CMT patient to reach maximal oxygen consumption at a higher mechanical load during an incremental test on a treadmill, thus reflecting an improvement in the ratio between energy cost and mechanical load, referred to as energy efficiency.
Nevertheless, in CMT patients the compliance with AFOs is poor. 18 Ramdharry et al. 25 demonstrated that only CMT patients with a high level of walking impairment wear AFOs on a regular basis. Recent studies based on interviews revealed that CMT patients consider AFOs to be uncomfortable and anaesthetic18,26 since P-AFOs usually require patients to wear custom-made orthopaedic shoes. Therefore, a few studies recently evaluated the effect of anterior elastic AFOs (A-AFOs), which improve comfort and adaptability to ready-made shoes, on walking kinematics of CMT1A patients.19,21 The use of A-AFOs significantly increased ankle dorsiflexion, decreased hip flexion during the swing phase 21 and enhanced step length 19 compared with shoes only. To the best of the authors’ knowledge, there are no studies on the metabolic cost of walking with A-AFOs in CMT patients. The measurement of walking energy cost per unit of distance (WECd), also referred to as walking economy, is a valid indicator of walking performance. Individuals with good walking economy, from a practical perspective, walk faster and for longer with a lower level of physical effort.17,27 The purpose of this study was therefore to quantify the walking energy cost of patients with CMT1A, while wearing A-AFO in comparison with walking with shoes only. It was hypothesized that walking with A-AFO would be accompanied by a lower metabolic energy cost of walking with respect to shoes only in CMT1A patients.
Methods
Participants
Seven patients with CMT1A (four women and three men; mean age = 37.1 ± 11.2 years; mean body mass = 72.1 ± 13.4 kg) participated in this study. Volunteers with CMT1A were recruited from the Unione Italiana Lotta alla Distrofia Muscolare (UILDM) Rehabilitation Centre in Rome. The inclusion criteria were as follows: (1) history of CMT1A, (2) Barthel index > 70 28 and Tinetti score > 20 29 to ensure the ability to walk without walking assistance, (3) age between 20 and 50 years and (4) no clinical signs of heart or pulmonary disease. Selected patients had a mean Barthel index of 95.7/100 ± 3.8 (mean ± standard deviation (SD)) and a Tinetti score of 22.3/28 ± 2.6 (mean ± SD). Muscle strength around hip, knee and ankle joints was assessed according to the Medical Research Council (MRC) scale, 30 as reported in Table 1. The maximal passive dorsiflexion of the ankle joint was 95 ± 10 degrees for both limbs. With ethics committee approval of the University of Rome La Sapienza, this study was carried out in accordance with the Declaration of Helsinki and informed consent was obtained from all participants.
MRC scores (mean ± SD) of patients’ lower limb muscles.
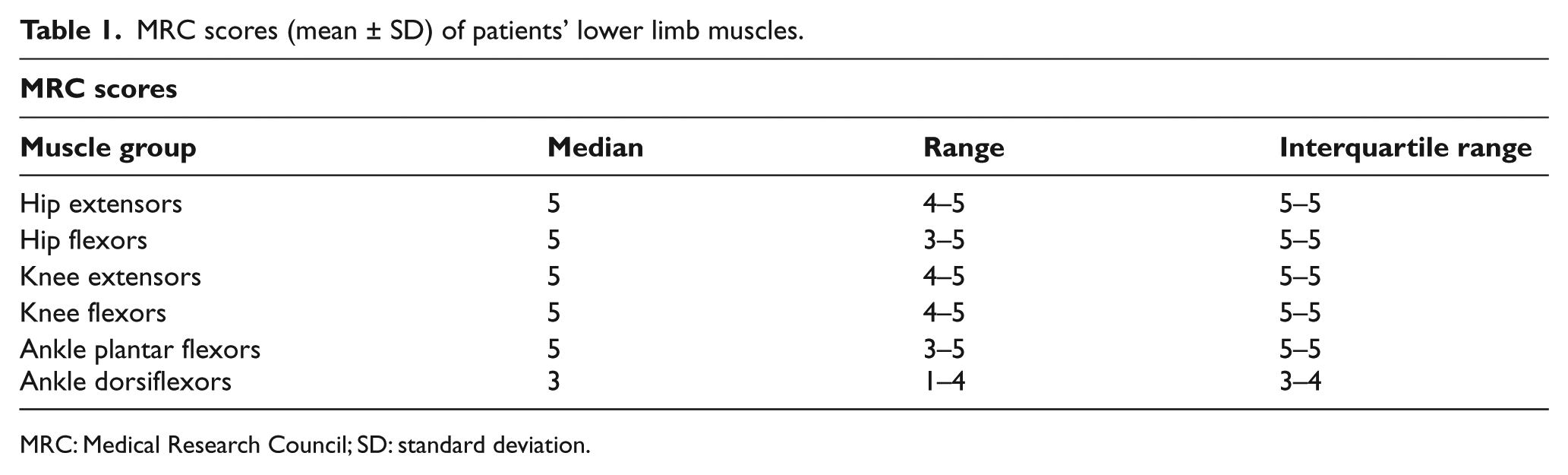
MRC: Medical Research Council; SD: standard deviation.
Instrumentation and measurements
The steady-state oxygen uptake (VO2) and carbon dioxide production (VCO2) were measured by means of a telemetric, portable system (K4b2, COSMED, Rome, Italy), of which validity, accuracy and reproducibility have been assessed during rest and exercises at various intensities. 31 VO2 was first measured during sitting for 5 min to reach a steady-state condition. Participants were then requested to walk on an oval-shaped 23-m walkway circuit (rectilinear for 5 m on each side) once wearing the A-AFO (Taloelast®, Ortopedia Mancini, Rome, Italy) and once wearing their own shoes only, in a randomized order. Taloelast consists of a polypropylene leaf positioned above the anterior part of leg, ankle and foot. The proximal part is fixed by means of a Velcro strap at the leg level and the distal part is placed underneath the shoe laces. An elastic-adjustable Velcro strap goes from the distal part to the proximal part of the polypropylene leaf (see Figure 1). The elastic strap provides a resistance to plantarflexion, which is sufficient to maintain adequate dorsiflexion of the ankle joint and allows ground clearance during the swing phase. It does not limit dorsiflexion during the stance phase. In each condition, volunteers were asked to walk at three self-selected walking speeds: slow, comfortable and fast. Instructions to the participants on the three self-selected speeds were given by associating the speeds with the activities performed during day-to-day life: comfortable speed was described as the way the participants normally walk in a relaxed mood, fast speed as the way the participants walk when they are late for an appointment and slow speed as the way they walk during relaxed window-shopping. Each condition lasted 5 min in order to reach a steady state, and 5 min were given for adequate recovery between each condition, which was verified by visually inspecting VO2 prior to beginning the next trial. The sequence of walking speeds was randomized for each participant. The data obtained during the final minute were used for further analysis.
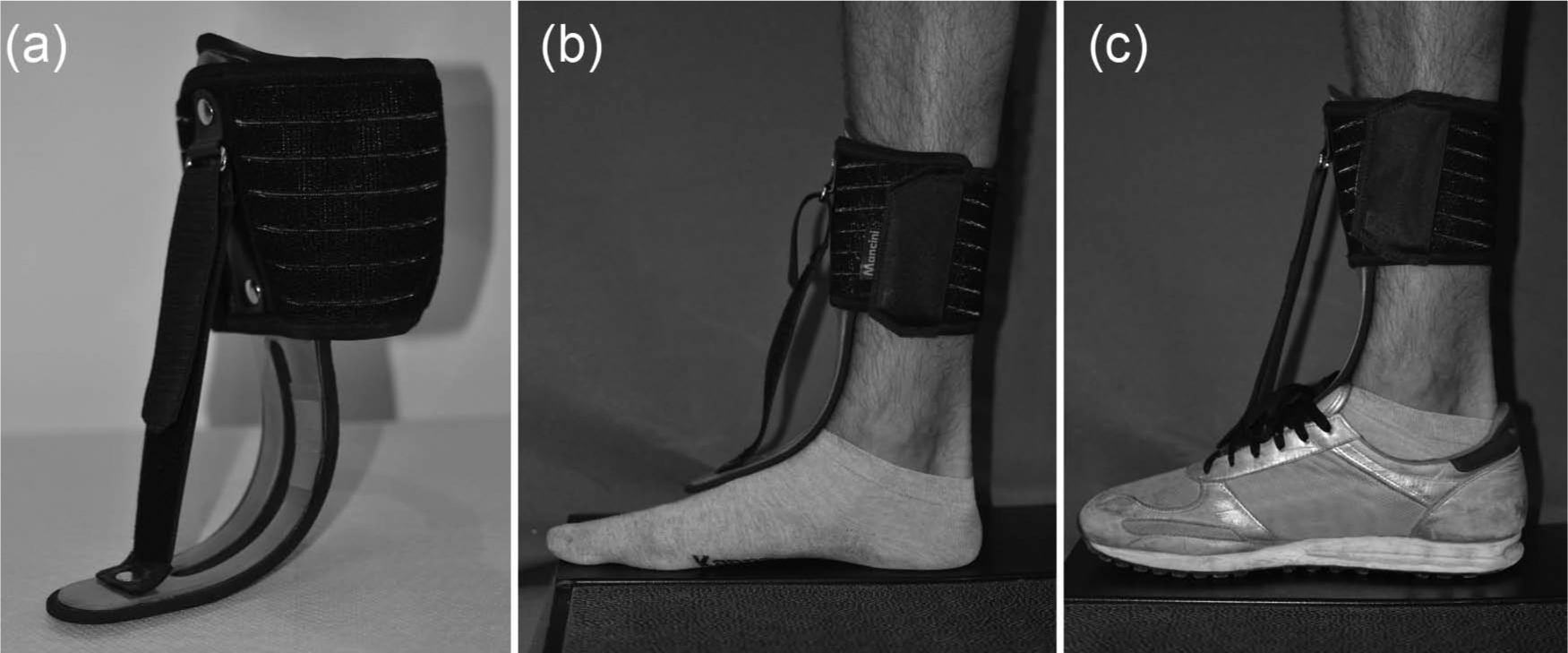
(a) Taloelast® ankle-foot orthosis, (b) Taloelast without shoes and (c) Taloelast with shoes.
Time was measured with a stop watch (Oregon Scientific, Hong Kong, China), and the total number of steps were counted by the experimenter.
Data analysis
The primary outcome measure for this study was the walking energy cost (WEC). Following Bernardi et al. 27 and Thomas et al.,32,33 the walking energy cost per unit of time (WECt) was calculated as the amount of oxygen uptake per unit of body mass and per unit of time (expressed in J kg−1 min−1). It was calculated as WECt = k (VO2), where VO2 is the energy cost (expressed in mL kg−1 min−1) and k is the energy (J) equivalent of oxygen. The respiratory gas-exchange ratio (RER) of the last minute was taken into account to adjust k. 33 The net WECd was then calculated as the net energy cost per unit of body mass and per unit of distance (expressed in J kg−1 m−1). The following formula was used: WECd = (WECt − SECt)/S, where WECt is the energy cost during walking in J kg−1 min−1, SECt is the energy cost during sitting in J kg−1 min−1 and S is walking speed in m min−1. The average walking speed was obtained by dividing the total walking distance (m) by the time taken to cover it (s). Step length, expressed in metres, was computed as the total distance walked by the individual divided by the total number of steps counted by the experimenter. Step frequency, expressed in steps s−1, was computed as average walking speed divided by step length.
Statistics
All data were normally distributed in terms of skewness and kurtosis (all values < 2). Statistical comparisons of the parameters (WECd, WECt, speed, step length, step frequency), between the two conditions (A-AFO and shoes only) at the three self-selected speed (slow, comfortable and fast) were carried out by two-way analysis of variance (ANOVA) for repeated measures, followed by Student’s t-tests with Bonferroni correction where appropriate. Statistical significance levels were set at P < 0.05.
Results
Walking speeds, step lengths and frequencies measured during the three walking trials in both conditions (shoes only and A-AFO) are presented in Table 2. The ANOVA for walking speeds, step lengths and frequencies showed a significant effect of walking trial (slow, comfortable and fast) while there was no significant effect of condition.
Walking speed, step length and frequency (mean ± SD) during slow, comfortable and fast conditions with shoes only and A-AFOs.
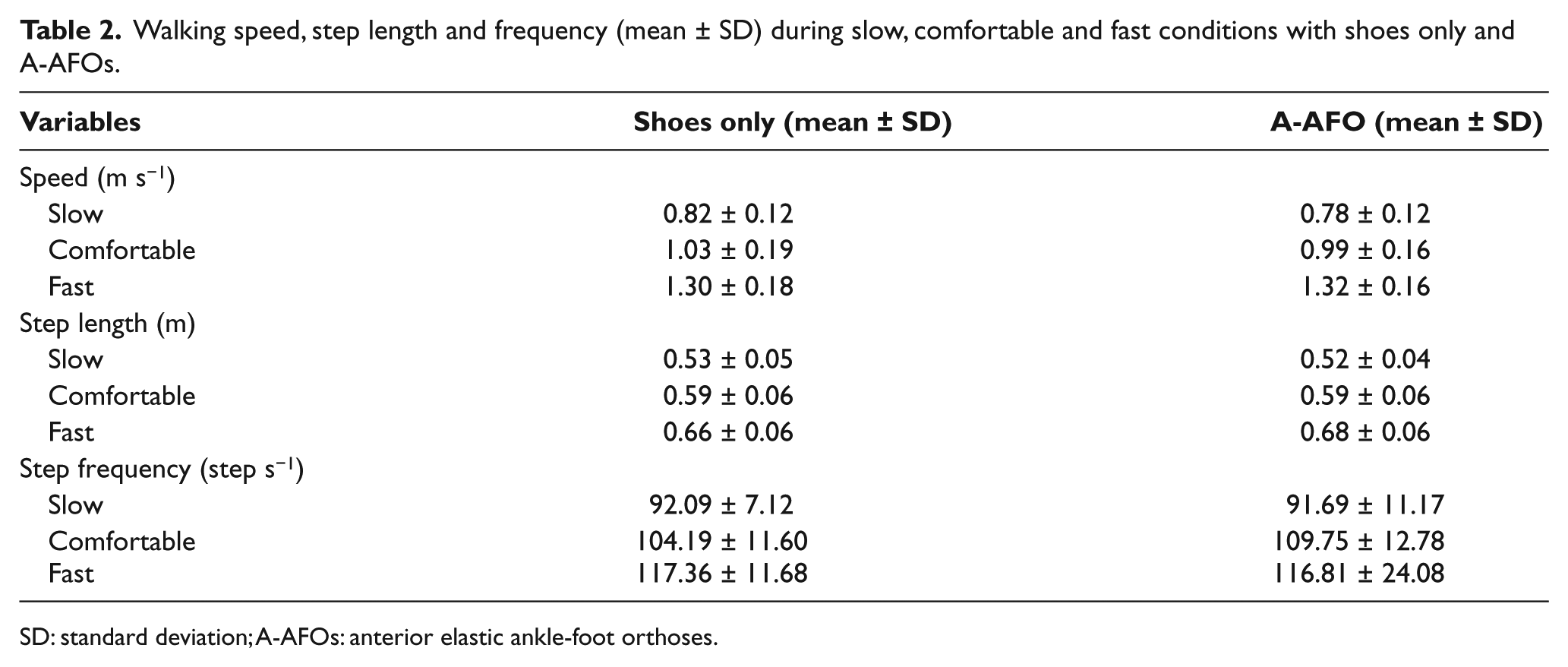
SD: standard deviation; A-AFOs: anterior elastic ankle-foot orthoses.
As shown in Figure 2, the ANOVA for WECt showed a significant effect of walking trials (P < 0.05) and a significant effect of condition (P < 0.05). The post hoc analysis showed that the WECt was lower in shoes only with respect to A-AFO at comfortable speed (P < 0.05), whereas WECt was higher in shoes only with respect to A-AFO at fast speed (P < 0.05). Similarly, the ANOVA for WECd showed significant effect of walking trials (P < 0.05) and a significant effect of condition (P < 0.05). The post hoc analysis showed that WECd (Figure 3) was lower in shoes only with respect to A-AFO at comfortable speed (P < 0.05), whereas WECt was higher in shoes only with respect to A-AFO at fast speed (P < 0.05).
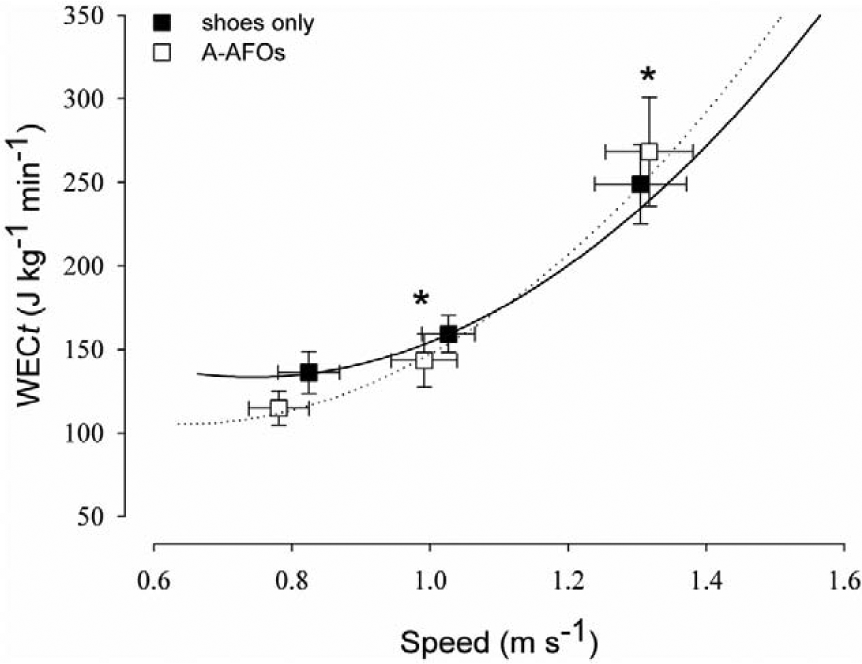
WECt (mean ± SE) as a function of self-selected walking speed (slow, comfortable and fast speeds) in patients with shoes only and A-AFO.
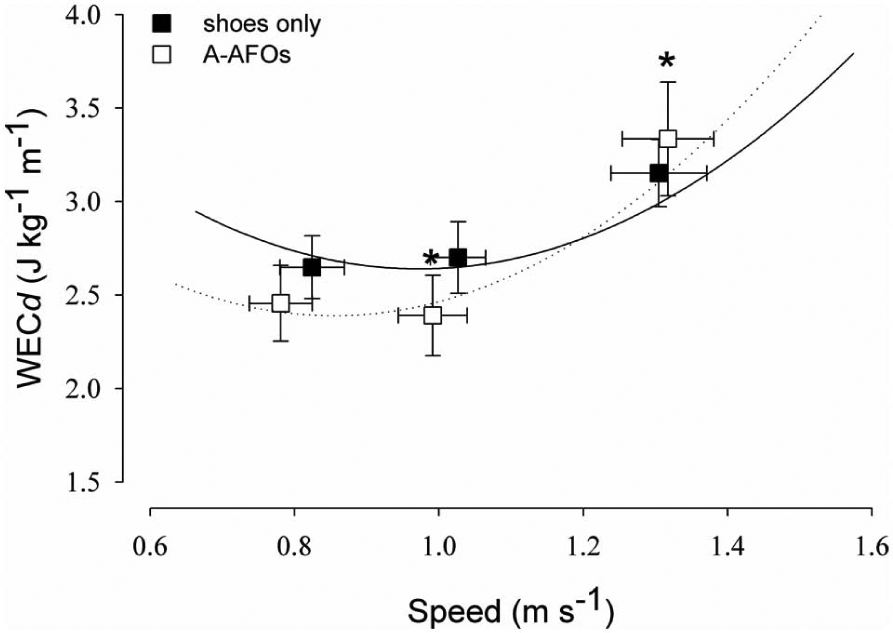
WECd (mean ± SE) as a function of self-selected walking speed (slow, comfortable and fast speeds) in patients with shoes only and A-AFO.
Discussion
The major finding of this study is that the CMT1A patients showed a lower energy cost per unit of time and per unit of distance when walking at their comfortable speed with A-AFO compared to walking with shoes only, which from a practical perspective means that they can walk for a longer duration and with a lower level of physical effort. Although, to the best of the authors’ knowledge, there are no studies on the metabolic cost of walking by using AFOs in CMT1A patients, there is evidence that AFOs improve walking economy in either hemiplegic 34 or post-polio patients, 35 which has been attributed to an improved gait efficiency by relieving patients from excessive motions or muscular overloads of the trunk and lower extremities during walking. In CMT1A patients, the higher energy cost of walking with respect to healthy individuals has been mainly ascribed to the extra-effort required to perform their peculiar steppage gait, which clinically implies increased hip and knee flexion to clear the plantarflexed ankle or drop foot. 17 Therefore, improvements in walking economy due to AFOs are likely a consequence of the reduction in steppage gait. Indeed, Ramdharry et al. 21 demonstrated through gait analysis that both A-AFOs and P-AFOs reduce hip flexion during the swing phase of gait in CMT patients, which may account for their lower metabolic energy cost. Moreover, a reduction in hip flexion with AFOs may result in an increased confidence that they will not trip, 21 which in turn would account an improved walking economy. In contrast with the results at comfortable speed, both WECt and WECd at fast speed were higher in CMT1A patients when walking with A-AFO compared to walking with shoes only. Wearing A-AFOs at fast speed may increase the degree of movement complexity 17 and oblige CMT patients to co-activate muscles around the ankle and knee joints, such as increasing walking energy cost.
The three self-selected speeds of walking did not differ in CMT1A patients when walking with A-AFO as opposed to walking with shoes only. This result is in agreement with previous studies19,21 that failed in demonstrating that CMT patients increase their walking speed by using either A-AFOs or P-AFOs. Therefore, walking energy cost per unit of distance with A-AFOs was improved independently of walking speed, indicating that the improvement was likely due to altered walking mechanics. However, an improvement in walking speed in one CMT patient using AFOs has been reported in a pilot study by Vinci et al. 22 It is likely that the patient of this pilot study had a higher level of impairment in walking than that of our group of patients and, similar to other group of patients with severe walking impairments, either hemiplegic 34 or post polio, 35 AFOs were effective also in improving walking speed.
As for walking speed, step length and step frequency did not change in CMT1A patients when walking with A-AFO with respect to walking with shoes only. Our results are consistent with the findings of Ramdharry et al., 21 although Guillebastre et al. 19 demonstrated that CMT patients enhanced step length when using both A-AFOs and P-AFOs compared to shoes only. One possible explanation of this discrepancy could be in the fact that our volunteers were not used to wearing any kind of AFOs during their daily life. Despite the brief familiarization with A-AFO, it could be that a single-day trial was not enough to change their usual locomotion pattern.
As a limitation, our preliminary results, although statistically significant, need to be confirmed by further investigations on a larger sample of patients. Second, we demonstrated that the A-AFO improves walking economy with respect to walking with shoes only, but we have not compared A-AFO with P-AFO. We cannot therefore claim that A-AFO improves walking economy more than P-AFO in CMT1A patients, although it has been reported that A-AFO has the advantage to improve comfort and adaptability to ready-made shoes.19,21 Third, comfort and patients’ perception were not assessed in this study. Longitudinal study with additional function and satisfaction measures would be required to look at any effects over time and determine efficacy.
Conclusion
In the CMT1A patients selected for this study, the use of A-AFO improved walking economy by reducing both the energy cost of walking per unit of time and per unit of distance. From a practical perspective, CMT1A patients can therefore walk for a longer duration and with a lower level of physical effort.
Footnotes
Acknowledgements
The authors would like to thank David Stewart for reviewing this article.
Declaration of conflicting interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.