
Abstract
Background:
Due to blocking of pronation/dorsiflexion in flexible flat foot and restriction of these movements in using the University of California Berkeley Laboratory orthosis, provided pressures in sole by the orthosis were increased. Therefore, this article describes the evaluation of modified foot orthosis with flexible structure in the management of individuals with flexible flat foot.
Case description and method:
The patient was a 21-year-old male who had symptomatic flat foot. The modified foot orthosis included movable surface and the outside structure. The modified foot orthosis was evaluated by standing foot X-ray, comfort rate, electromyography of leg muscle and vertical ground reaction force during walking.
Findings and outcomes:
The modified foot orthosis improved the foot alignment and decreased the symptoms of flat foot with more comfort. Subtalar position by sub-maximum supination had higher position than neutral in sagittal plane. It may increase the muscle activity of peroneus longus by 7% compared to barefoot, and there was a decrease of 11% ground reaction force in mid stance.
Conclusion:
The result of this single case evaluation only proposed the feasibility of this modified insole as the orthotic treatment in flexible flat foot.
Clinical relevance
The modified foot orthosis, which is mobile in the midfoot, is an orthosis for walking and standing in subjects with flexible flat foot.
Background
Flat foot is defined as the reduction of the medial longitudinal arch in the foot, heel valgus deformity, and medial talar prominence. 1 The deformity is usually asymptomatic and resolves spontaneously in the first decade of life or occasionally progresses into a painful less flexible form, which causes significant disability. Ligamentous laxity, equinus deformity of the foot, tibial torsional deformity, the presence of the accessory navicular bone, and obesity have been observed as contributing to the causation of flat foot.2,3 The prevalence of flat foot has been reported between <1% and 28% at specified age groups.4–6
The primary aims of treatment of flat feet are reduction of pain, relief of disability, and the prevention of future disability (e.g. joint damage and, in later life, a rigid fixed foot deformity). 7 Conservative management to surgical approaches has been considered in the treatment of flat foot. Surgical methods are used usually only after the failure of conservative management advice, which includes foot orthoses (shoe inserts), stretching, footwear selection and modifications, activity modifications, manipulation, serial casting, appropriate weight reduction, and anti-inflammatory medications, all reported as conservative methods in the treatment of flat foot. 8
Many orthoses have been introduced in the treatment of flexible flat foot. Corrective shoes, arch supports, and shoe inserts are examples of this type of intervention. 9 These types of orthoses as mechanical devices were introduced to support the foot near the optimal position in order to provide more effective mechanics of the foot during ambulation and develop normal growth of the foot. 10
The University of California Berkeley Laboratory (UCBL) orthosis is a maximum-control foot orthosis that is used as conservative method in the management of flexible flat foot deformity. The UCBL fully encompasses the heel with a molded heel cup, which in turn holds the heel, or hind foot, in neutral and vertical positions associated with controlling arch support. 11 Due to blocking of compensatory motions (pronation/dorsiflexion) in flexible flat foot and restriction of these movements in using a rigid UCBL-type orthosis, provided pressures in sole as well as medial and lateral borders by the orthosis increased. Therefore, the affected leg is forced to go into knee hyperextension or produces a forward trunk leaning positions that cause shortened step length and reduced speed of walking. 12 So, similar to normal walking, some flexibility of the foot is essential for better function. 13 Therefore, this article describes the fabrication of a modified UCBL in order to become a more functional insole in the management of individuals with flexible flat foot.
Case description and method
Subject
The patient was a 21 year old male, who had symptomatic flat foot of 10 foot posture index (FPI) (14). Symptoms included a sensation of discomfort such as early tiredness or difficulties during prolonged standing or walking. He was referred to the department of orthotics and prosthetics in the University of Social Welfare and Rehabilitation Sciences. The referral was for the production of an insole. The subject gave informed consent to participate in this study. Approval was obtained from the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences to undertake this study. Based on the technique, explained earlier, one pair of modified orthosis was prepared for the subject. After 1 month of daily use, the orthotic treatment was evaluated.
Intervention
To provide a negative cast, a foam impression casting technique was used. Casting was taken in a semi-weight-bearing position while the subject was seated on a chair and the foot was in contact with the ground. Hand pressure was used for positioning and keeping the foot at an uncompensated mid-stance posture, where the maximal natural arch height was captured with the subtalar joint in a maximum arch stabilizing supination (MASS) position.15,16 The NAS anterior line method was used to find subtalar neutral and the MASS positions. 17
According to the method of modification that was introduced by Colson and Berglund, 18 correction of the positive cast of the foot was performed for the modified UCBL. Plaster was removed in the posterior region of the longitudinal arch and the medial aspect of the heel inferior to the sustentaculum tali. Additional plaster removal was done beneath the anterior aspect of the talus, navicular, and the cuboid. Through this cast removal, the midtarsal joints were stabilized in the sagittal plane. An addition of plaster was made on the base of the heel for stabilization of the orthosis in the shoe and during walking.
The orthosis was based on the trim lines of the UCBL but with a flexible structure, in order to ensure flexibility in all three planes. The modified orthosis included two parts: a movable surface and an outside structure. The construction of the orthosis, regarding its corrected positive cast, was provided by lamination. To provide the modified orthosis, lamination was performed in two stages. To prepare a movable surface, in the first stage, the sole of the orthosis was prepared with carbon fiber and glass fiber hybrid reinforced plastics, including three layers of Otto Bock 616B17 carbon fiber cloth with an angle of 90° and one layer of Otto Bock 616G18 fiberglass cloth, by lamination with hard material Otto Bock 617H19 Orthocryl® Lamination Resin. Dimensions of carbon fibers are intended to be smaller as the edges and hence produce more flexibility. In the second stage, an outside shell with medial and lateral flanges similar to traditional UCBL was made by lamination. The prepared carbon sole was isolated and put on the positive cast between the laminated layers to fabricate the outside structure. Afterward, the heel post was connected to the sole and then the sole and the outside structure of the orthosis were connected together by glue. The edge of the sole in the front two-thirds of the orthosis was shortened by 2 mm to allow mobility inside the orthosis. Based on the C-shaped channel of the outside structure and the lack of arch in walls, the motion of the orthosis was observed to be more in the new design of insole. As specified, modified orthoses are designed primarily not only to allow graded flexibility in the orthosis but also to support the longitudinal arch same as the standard UCBL orthosis. The orthosis was based on the trim lines of the UCBL but with a flexible structure, to ensure flexibility in all three planes. Figure 1 shows the overall view and two parts of the modified UCBL orthosis.
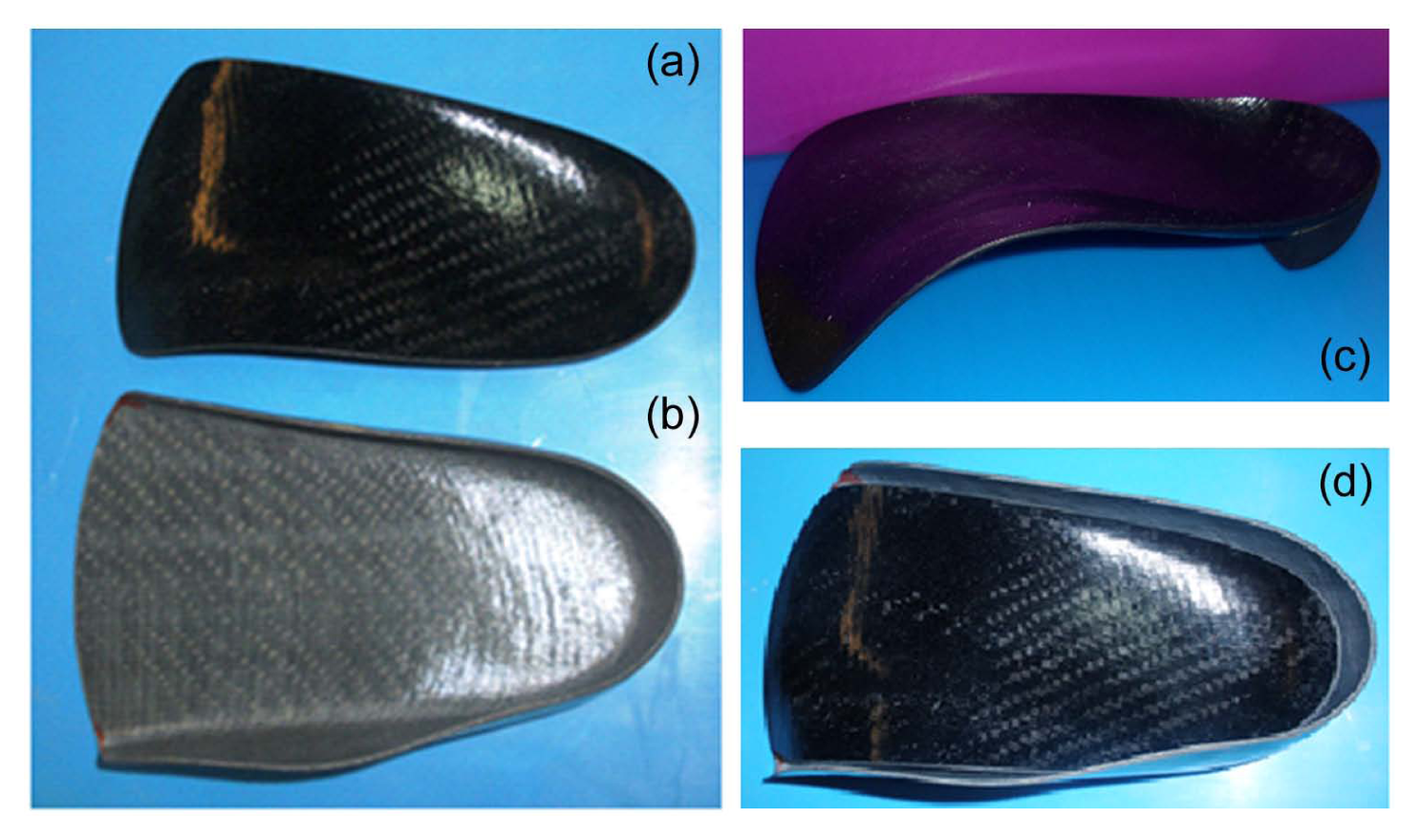
Overall view and details of modified orthosis parts: (a) inside sole, (b) outside sole, (c) lateral view of inside sole, and (d) top view of modified insole.
Evaluation approaches
The evaluated parameters were foot skeletal alignment by X-ray in weight-bearing standing posture and comfort and pain rate by visual analog scale (VAS), 19 ranging from 0 (“no comfort,” “no pain”) to 10 (“high level of comfort,” “worst pain”). A portable system with data link (Biometrics Ltd, England) and bipolar active electrodes with a fixed electrode distance of 20 mm (model SX230) was used to collect the electromyography (EMG) of the tibialis anterior, peroneus longus and medial gastrocnemius. An active electrode has a preamplifier with gain 1000, which can differentiate between a small and interference signals that would create on the skin. For tibialis anterior, the surface electrode was placed at approximately 20% of the distance between the tuberosity of tibia and the inter-malleoli line, starting from the tuberosity of the tibia. For medial gastrocnemius, the surface electrode was placed at approximately 25% of the distance from the medial side of the popliteal cavity to the calcaneal tubercle. 20 For peroneus longus, the surface electrode was placed at approximately 20% of distance from the head of the fibula to the lateral malleolus. 20 The normalized mean amplitude was analyzed for each muscle. The EMG data were normalized to 100% of maximum voluntary isometric contraction (MVIC) tests. 21 The muscle tests were performed to take the MVIC following the methods described by Soderberg et al. 22
The effect of orthosis on the ground reaction force (GRF) was evaluated with two Kistler force plates (Model 9286B; Winterthur, Switzerland) with frequency of 100 Hz. Six time trials considered to valuation of this parameter.
Findings and outcomes
From the transversal view of the foot X-ray, the talus-second metatarsal joint and the talonavicular coverage angles (TNCAs) in the lateral view, calcaneal pitch, and calcaneo-fifth metatarsal angles were measured by Agfa SE Media Viewer Version 3.7.0.0. The comparison of angles in the analysis conditions demonstrated that the modified orthosis corrected the foot alignment (Figures 2 and 3) (Table 1). The subject’s evaluation of comfort was 8 on the VAS. Due to the flexibility of the wall and the sole in this modified orthosis, there was no excessive pressure on the skin of patients using the orthosis. During prolonged standing and walking, the modified orthosis reduced pain and discomfort of the patient when compared to barefoot or shoe-only conditions.
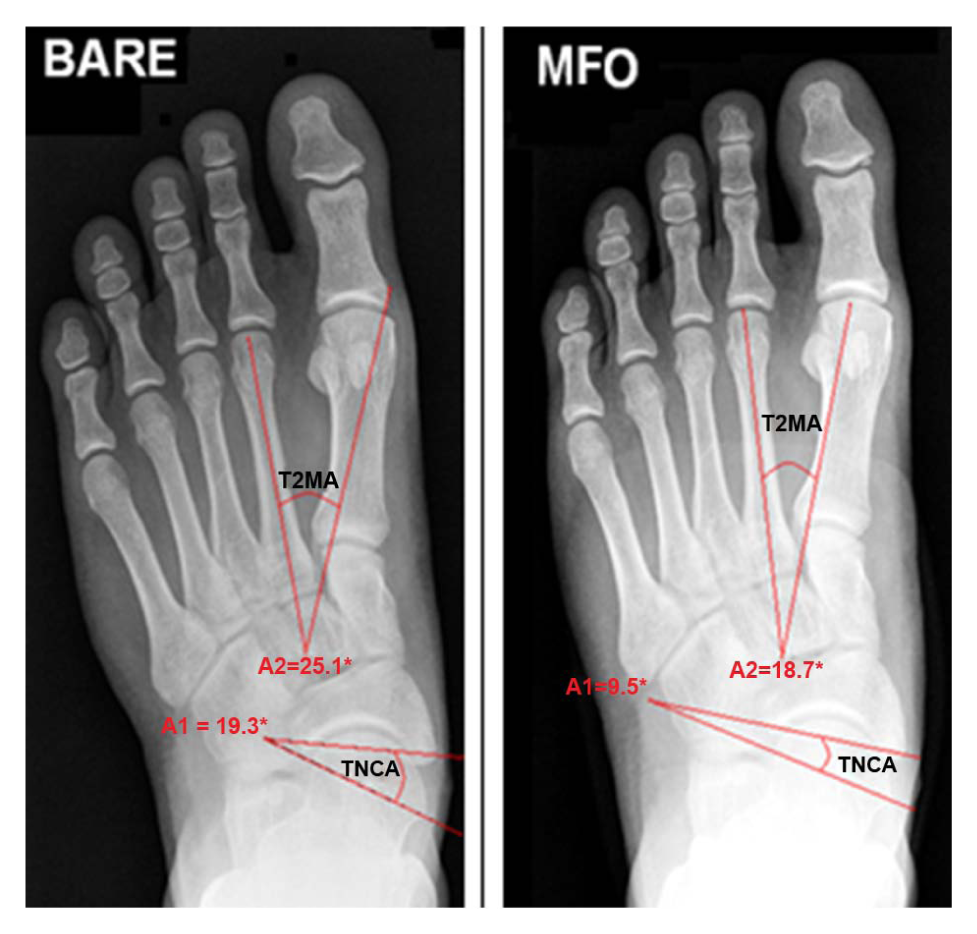
TNCA and T2MA barefoot conditions (left image) and using modified foot orthosis (right image) in tzransversal view.

CIA and C1MA foot X-ray in barefoot (top image) and using modified foot orthosis (bottom image) in medial view.
Angles of foot bones in X-ray with two conditions.
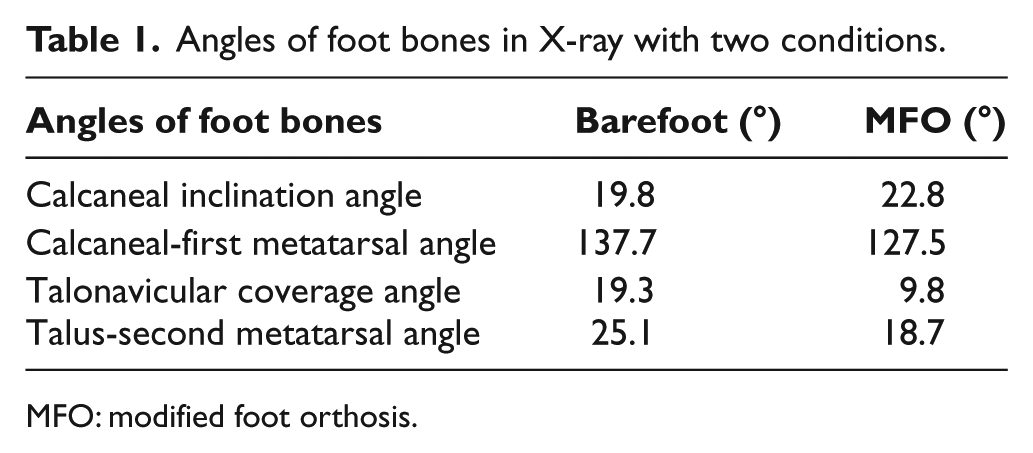
MFO: modified foot orthosis.
In stance phase, the normalized mean EMG amplitude of anterior tibialis muscle shows a 1% decrease in using the new orthosis compared to the barefoot condition. While wearing new orthosis, the activities of the peroneus longus muscle and the medial gastrocnemius muscle increased by 7% and 1%, respectively, compared to the barefoot condition. Table 2 shows means and standard deviations (M ± SD) of leg muscle amplitudes during walking based on a percentage of maximum voluntary isometric contraction (%MVIC) muscle test in three conditions with six time trials.
Mean and SD of leg muscle normalized amplitude during walking in three conditions.

MFO: modified foot orthosis; %MVIC: percentage of maximum voluntary isometric contraction; SD: standard deviation.
Evaluation of the GRF showed that vertical component of the GRF in the first peak was increased by 17% using the modified orthosis compared to barefoot condition. While wearing the orthosis, there was a 11% decrease in the minimum vertical force in the mid-stance. All conditions of walking had approximately similar GRF vertical component in the second peak during the propulsion phase. Using the modified orthosis, similar to walking with shoe conditions, improved stance time of walking compared to walking in the barefoot situation in this subject (Figure 4). Table 3 shows mean and SD of GRF vertical component during walking barefoot, shoe-only and with the modified orthosis.
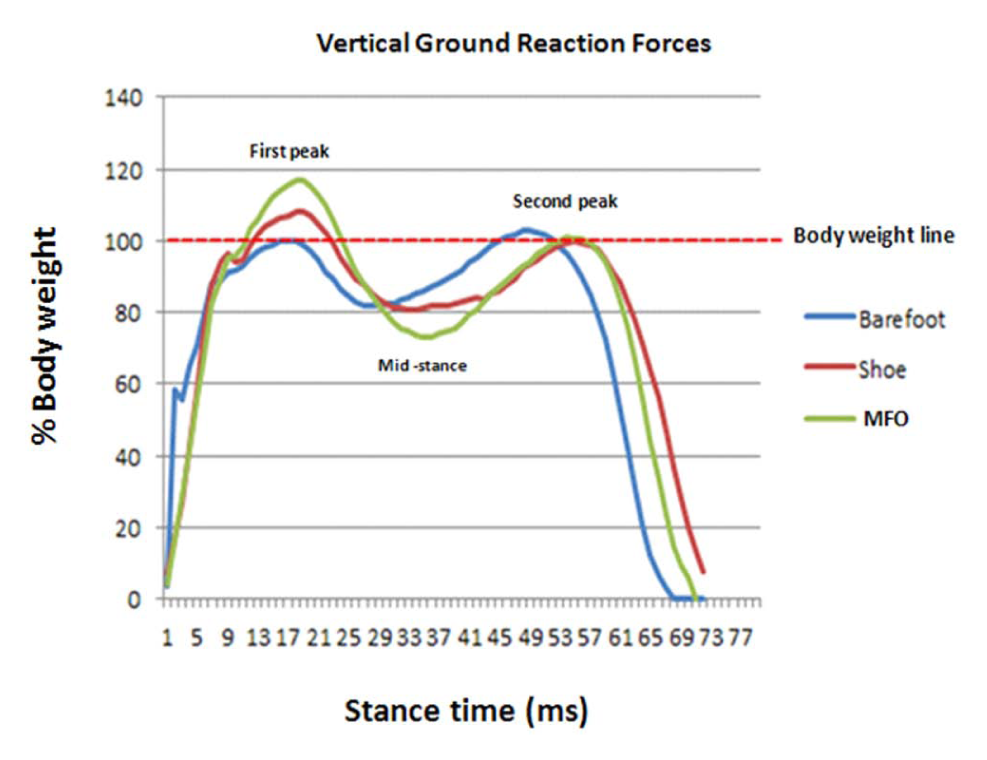
GRF vertical component during walking barefoot, shoe-only, and with orthosis.
Mean and SD of GRF vertical component during walking barefoot, shoe-only and with orthosis.

MFO: modified foot orthosis; GRF: ground reaction force; SD: standard deviation.
Discussion
The purpose of this study was the construction of modified UCBL orthosis that provided foot mobility with the orthoses, regarding the characterization identified in flexible flat foot (e.g. pain relief, supportive structure, and corrective foot alignment). Fabricated modified orthosis reduced foot pain in this study.
Movement in transverse and sagittal planes is restricted in using UCBL orthosis. Based on the flexible structure of foot, during walking and standing, we designed new orthosis that provides flexible condition in wearing it. We expected the modified orthosis to improve the foot movement in sagittal and transverse planes. Results of this study, in correction of foot position, approved our expectation in standing evaluation. Results of this study, in the control of the movement in the foot portion, were similar to the reports of previous study with custom foot orthoses used to modify pronation during standing. 23 The modified UCBL insole, in this study, reconstructed arch position, kept the foot in a position with reduced tension on the soft structures. Walls of the modified orthosis on the heel portion kept the calcaneus in the anatomical position. The movable surface of the insole, under the sustentaculum tali, restricted the motion toward a valgus position. Abduction of the forefoot was limited, by the lateral walls of the orthosis, in the midtarsal joints. The flexible flat foot was supported with normal alignment and was functional with lesser loads on soft tissue. It is expectable that the modified orthosis allows intrinsic muscles to move and prevents muscle atrophy with long period of use. This topic is interesting as further study in this field.
The measurement of GRF has been used for many years in biomechanics to quantify external forces during locomotion as GRF data are a “remote” measure of lower extremity action. 24 The GRF components consist of three force components. Maximum alternation happened in the vertical component compared to anterior–posterior and mediolateral directions. In this study, GRF vertical component in mid-stance in barefoot condition was increased in walking compared with modified orthosis, and the pattern of GRF vertical component in the first peak point was improved as normal walking. 25 In compared to previous studies, Leung et al. 26 found no significant difference in the vertical reaction force in first peak with orthotic using during walking, but Miller et al. 27 reported decreased and Sloss 28 showed increase 3%–5% of the GRF vertical component in first peak in using foot orthosis in subjects with flexible flat foot. It seems that the type of material and shape of insole affect the GRF.
During mid-stance, the GRFs produce a pronation moment at the subtalar joint so that the flat foot patient decreases the duration of the stance phase to prevent excessive pronation and subsequent discomfort which reduces downward movement of body weight during midstance. Using a modified insole improves the stance time compared to walking in the barefoot condition. It seems as if decreased GRF in the mid-stance provides a more comfortable condition in weight bearing in the flat foot subject, caused by the slow transfer of weight on the foot with the use of modified orthosis, 29 although there was no significant difference reported in previous studies in this field.27,28
Increasing the peroneus longus EMG amplitude with modified orthosis, compared with the shoe-only and barefoot during walking, may be secondarily related to the eversion and plantar flexion of the first ray. 30 This finding is consistent with previous studies, which have reported that various styles of FOs increase peroneus longus EMG amplitude during gait.30–34 In addition, there may be some functional benefits in increasing peroneus longus EMG amplitude during the stance phase, as it has been shown that people with flat-arched feet have significantly lower peroneus longus EMG amplitude. 35 EMG amplitude compared with normal-arched feet significant change was not observed in tibialis anterior activity in using modified orthosis. This finding is not similar to that from previous studies, which have reported that various styles of FOs increase tibialis anterior EMG amplitude during walking, 30 but Murley et al. 34 reported same results in using foot orthosis. The change in muscle activity of medial gastrocnemius in using modified orthosis was small and similar to previous studies in this field.31,32,34
The effect of the modified orthosis on kinematic and temporal spatial parameters of walking in subjects with flexible flat foot was not evaluated. Functional ability of orthosis and “user friendliness” of the orthosis in activity of daily living and the quality of life in these subjects were not evaluated. In this study, comparison between standard UCBL and the modified orthosis on mentioned parameters was not evaluated. Further studies in this regard will be beneficial in this field. Based on the MASS position of the foot in insole, we will expect that the muscle activity of peroneus longus will increase, and according to the flexible design of modified foot orthosis (MFO), the comfort of the patients will improve. Also, the modified orthosis has positive effect on subjects with flexible flat foot, but it has been reported that the construction of MFO is difficult and time consuming due to the required accuracy in modification. Longitudinal studies in the evaluation of this orthosis on walking parameters, lower limb muscle activity, and position of foot joints in static and dynamic conditions in large groups of flexible flat foot patients with the use of a controlled group would be required.
Limitation
The study time was relatively short and hence no long-term directives can be given; moreover, the study was performed with one subject, thus making the results achieved difficult to generalize.
Conclusion
Consequently, the results, of this single case evaluation, only proposed the feasibility of this modified UCBL orthosis as the orthotic treatment in flexible flat foot.
Key points
Flexible flat foot is a condition that the arch of the foot reduces or disappears upon standing.
The modified orthosis provided more vertical and transverse flexibility in midfoot regions, increased peroneus longus muscle activity (7%), decreased GRF (11%) in the mid-stance, and improved comfort during ambulation and alignment of foot in standing position.
The modified insole was feasible to use in improvement of subjects with flexible flat foot.
Footnotes
Acknowledgements
The authors would like to thank Dr. Mokhtar Arazpour for his advice, support, and useful comments that have greatly improved the manuscript. The authors wish to thank Dr. Arezoo Eshraghi, Angie Farrell and Mike Crossland for their language editing.
This article was a part of a PhD thesis in the Department of Orthotics and Prosthetics (O&P) in the University of Social Welfare and Rehabilitation Science. The authors would like to gratefully acknowledge the help extended by the members of the O&P Department and the contributions from the patient in all stages of this study.
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.