
Abstract
Background:
Based on the literature, patients with carpal tunnel syndrome are suggested to wear a custom-made wrist orthosis immobilizing the wrist in a neutral position. Many prefabricated orthoses are available on the market, but the majority of those do not assure neutral wrist position.
Objectives:
We hypothesized that the use of orthosis affects grip strength in persons with carpal tunnel syndrome in a way that supports preference for custom-made orthoses with neutral wrist position over prefabricated orthoses.
Study design:
Experimental.
Methods:
Comparisons of grip strength for three types of grips (cylindrical, lateral, and pinch) were made across orthosis types (custom-made, prefabricated with wrist in 20° of flexion, and none) on the affected side immediately after fitting, as well as between affected side without orthosis and nonaffected side.
Results:
Orthosis type did not significantly affect grip strength (p = 0.661). Cylindrical grip was by far the strongest, followed by lateral and pinch grips (p < 0.050). The grips of the affected side were weaker than those of the nonaffected side (p = 0.002).
Conclusions:
In persons with carpal tunnel syndrome, neither prefabricated orthoses with 20° wrist extension nor custom-made wrist orthoses with neutral wrist position influenced grip strength of the affected hand. Compared to the nonaffected side, the grips of the affected side were weaker.
Clinical relevance
The findings from this study can be used to guide application of orthoses to patients with carpal tunnel syndrome.
Background
Carpal tunnel syndrome (CTS) can lead to numbness, tingling, weakness, or muscle damage in the hand and fingers. As a result of it, many people have trouble with their grip, often dropping cups and things due to muscle weakness. As it progresses, common daily activities can also be affected.
Optimal treatment for CTS should be patient-oriented and provide patients with a relief of symptoms as noninvasively, permanently, and inexpensively as possible. The treatment options for CTS are divided into two major groups: nonsurgical and surgical. 1 Nonsurgical treatment for CTS includes wrist orthosis, steroid injection, exercises, yoga, therapeutic ultrasound, activity or ergonomic modification, oral medication, and vitamins. 2
Orthosis creates immobilization of the wrist joint by external device. The orthosis usually leaves the fingers and thumb free to move, and it may be worn at nighttime and during daytime activities that cause wrist motion. 3 Some studies4,5 demonstrated short-term improvement of symptoms when comparing the use of orthoses with no treatment, but the recent systematic review 3 warns that these results should be interpreted with caution due to the high risk of selection and performance bias. The main outcome measure was the Levine et al.’s 6 self-reported questionnaire. It has 11 questions, only one of them being about hand weakness and one about grasping ability.
Two main types of orthoses can be used in patients with CTS: custom made from thermoplastic materials and prefabricated off-the-shelf orthoses. The main difference is in the wrist position, which is mainly neutral in custom-made orthoses, whereas it is in extension in off-the-shelf orthoses. Two studies7,8 indicated that orthosis with wrist in neutral position provides superior symptom relief compared to the orthosis with wrist in extension. They reported that the wrist angle that produces the lowest pressure on the median nerve in the carpal tunnel is within 2°–3° of flexion and 1°–2° of ulnar deviation of the wrist. However, the recent systematic review 3 warned that these results are also at high risk of selection bias and should therefore be interpreted with caution.
Among the five studies comparing the effectiveness of different orthoses,7,9–12 only the study by Brininger et al. 9 measured grip strength of pinch, palmar, and lateral grips. They reported that all the four groups they measured were significantly improved in tip and palmar pinches from baseline to 4-week follow-up. They compared prefabricated orthosis with wrist in 20° of extension to custom-made orthosis with wrist in neutral position, but it should be noted that the custom-made orthosis that they used also held the metacarpophalangeal joints in the neutral position.
To our knowledge, the only other study addressing the relative effects of orthosis design on grip strength in persons with CTS is the case-control study by Uğurlu et al. 13 They reported that custom-made volar thumbhole orthosis with wrist in neutral position reduced the strength of lateral, palmar, and tip-to-tip grip in persons with CTS. All other studies of effects of different orthoses on grip strength were performed either in patients with other diseases, mainly rheumatoid arthritis (RA),14–22 or in healthy persons.23,24
Based on the evidence summarized above, the rehabilitation team at our institute decided to suggest that patients with CTS wear a custom-made wrist orthosis in a neutral wrist position. Users are recommended to wear an orthosis throughout the night and also during the day if possible. But at the same time, many prefabricated orthoses are available on the market, and the majority of those do not assure a neutral position of the wrist. In clinical practice in our country, prefabricated orthoses are often selected over custom-made devices because they are cheaper. In our country, prefabricated wrist orthoses are included in the government insurance contract for the treatment of CTS. The rehabilitation team at our institute is trying to convince the professional audience in our country about the most suitable orthotic treatment of CTS. In our effort to prove that a custom-made orthosis with wrist in neutral position is a more appropriate solution than a prefabricated orthosis with wrist in 20° of flexion, we hypothesized that the use of orthosis affects grip strength in persons with CTS. We compared the effect on grip strength between two orthosis types: prefabricated wrist extension orthosis and custom-made orthosis with wrist in neutral position. We studied three different grips (cylindrical, lateral, and pinch grips). We also investigated whether the relative effect of grip type on grip strength differs between the affected and the nonaffected hands. A secondary aim was to find out whether there are general differences in grip strength between the affected hand and the nonaffected hand.
Methods
This study included persons with symptoms of CTS examined at the outpatient clinic for rehabilitation of persons with upper limb impairments at the University Rehabilitation Institute, Republic of Slovenia, from February to September 2008. The patients were included if they had been diagnosed using electromyography (EMG) as having CTS in one hand and were either candidates for orthotic treatment, according to the opinion of a medical doctor, or had rejected surgery. The patients were excluded if they were younger than 18 years or older than 80 years, had concomitant medical conditions that could influence upper limb function and health-dependent quality of life, had a history of carpal tunnel release surgery, or had undergone other types of conservative treatment. In addition, pregnant women and persons with cognitive impairments were excluded from this study.
Custom-made volar thumbhole orthoses with the wrist in neutral position were produced for each participant using a low-temperature thermoplastic material. Prefabricated elastic orthoses with the wrist in 20° of dorsal flexion were lent to the participants for the purposes of this study. Sporlastic Manu-Hit left- and right-side wrist orthoses were used in five different sizes (XS, S, M, L, and XL). The two orthosis types used are shown in Figure 1.
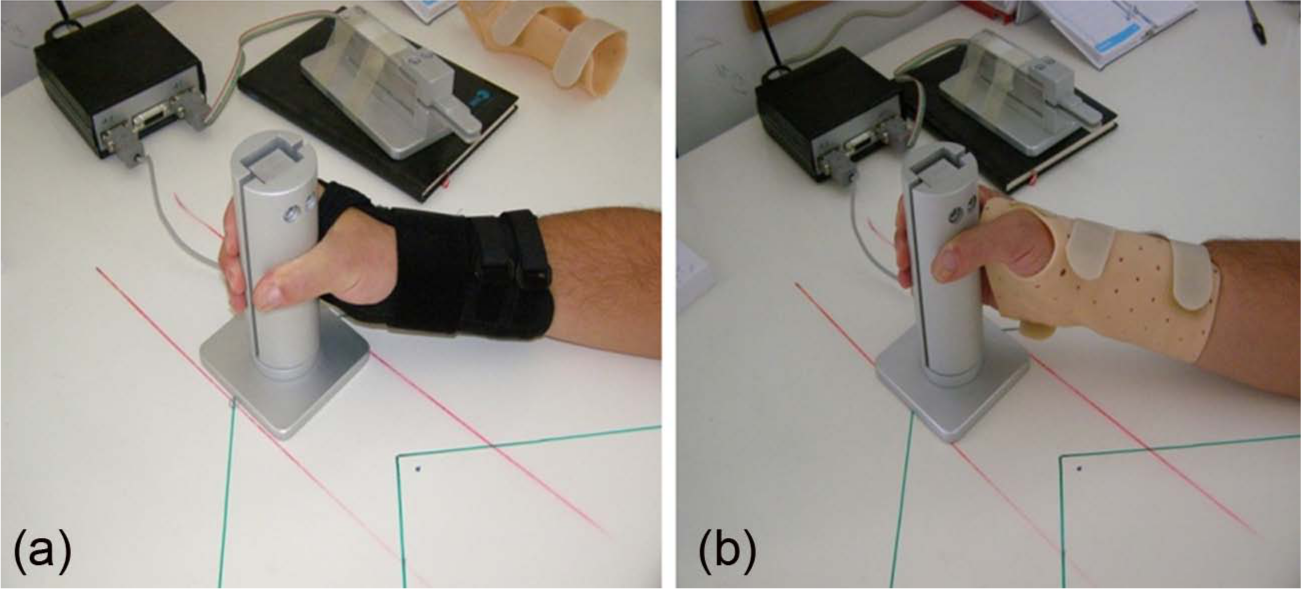
(a) Prefabricated elastic orthoses with the wrist in 20° of dorsal flexion and (b) custom-made volar thumbhole orthoses with the wrist in neutral position.
The gross strength of the cylindrical, lateral, and pinch grips was measured. It was measured in Newton (N) using a Grip Force Tracking System developed at the Laboratory for Robotics, Faculty of Electrical Engineering, University of Ljubljana. 25 This system consists of two force-measuring units of different shapes, which are connected to a personal computer for visual feedback and data acquisition.
Measurements were made with each person under all experimental conditions, that is, on the affected hand with the two types of wrist orthosis and without an orthosis and on the nonaffected hand without orthosis. Initial measurements were made with the nonaffected hand. The second measurements were made with the affected hand without orthosis in the same sequence for all three types of grips: cylindrical (first), lateral (second), and pinch (third). After a 10-minute pause, further measurements were made with the prefabricated elastic orthosis, and after another 10-minute pause, measurements were made with the custom-made orthosis. To avoid fatigue effects, only one measurement per condition was obtained. A rest period of 1 min was given between each strength measurements.
Each person was assessed while sitting upright with their feet flat on the floor. The measured hand was placed on the table at a 45° angle from the body. The elbow of the measured hand was in 90° of flexion. The wrist was maintained in a neutral position except when using the prefabricated orthosis. The forearm was positioned midway between pronation and supination for cylindrical and lateral grips. Pinch grip was measured with a pronated position of the forearm.
Descriptive statistics were calculated for all the variables, and their distributions were examined using histograms and normal q–q plots. Because all the distributions were right-skewed (as indicated by the differences between medians and means in Table 1), a square-root transformation was applied to all the variables before statistical inferences were made. This resulted in the assumptions for parametric statistical methods being met (as indicated by the symmetric box plots and nonoutliers in Figure 2, which has its vertical axis in square-root scale). The differences in strength of the three grip types of the affected hand between prefabricated orthosis, custom-made orthosis, and no orthosis were analyzed using two-way repeated-measures analysis of variance (ANOVA; with two 3-level within-subject factors), with Bonferroni-adjusted post hoc comparisons. Two-way repeated-measures ANOVA (with grip having 3 levels and hand 2 levels) with Bonferroni post hoc comparisons was also used to compare the strength of grips between the affected hand without orthosis and the nonaffected hand. Statistical significance was set at α = 0.05. IBM SPSS Statistics Version 20 (IBM Corporation, Armonk, NY, USA, 2011) was used for statistical analyses.
Descriptive statistics (for original data) and summary of statistical analyses (performed on square-root-transformed data).
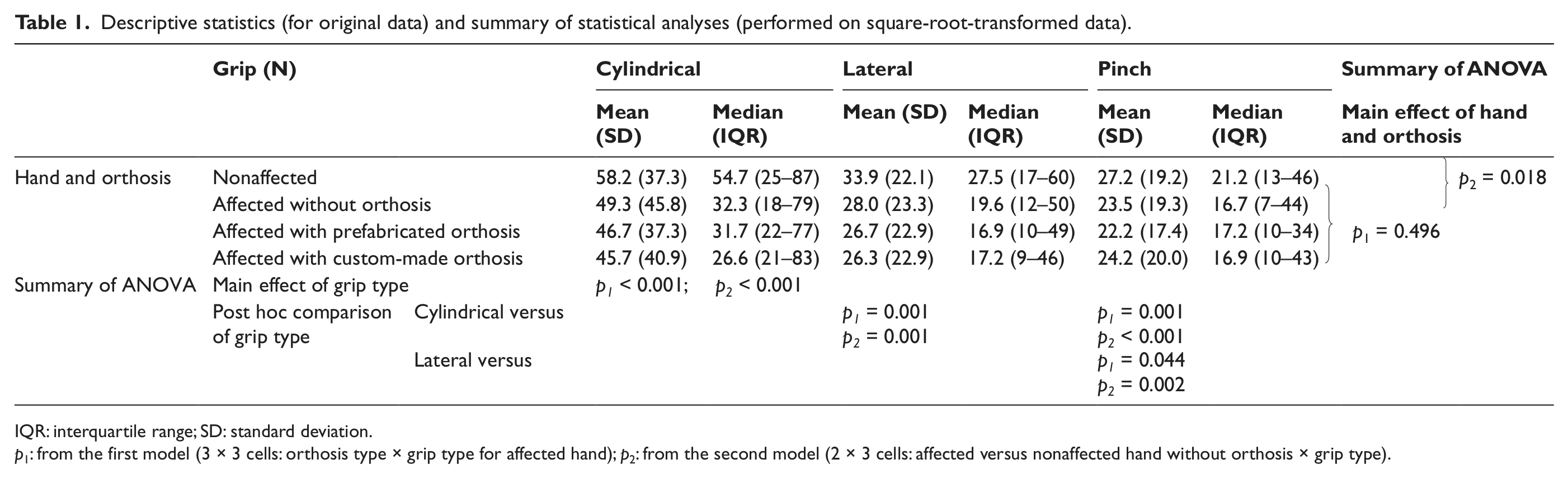
IQR: interquartile range; SD: standard deviation.
p1: from the first model (3 × 3 cells: orthosis type × grip type for affected hand); p2: from the second model (2 × 3 cells: affected versus nonaffected hand without orthosis × grip type).
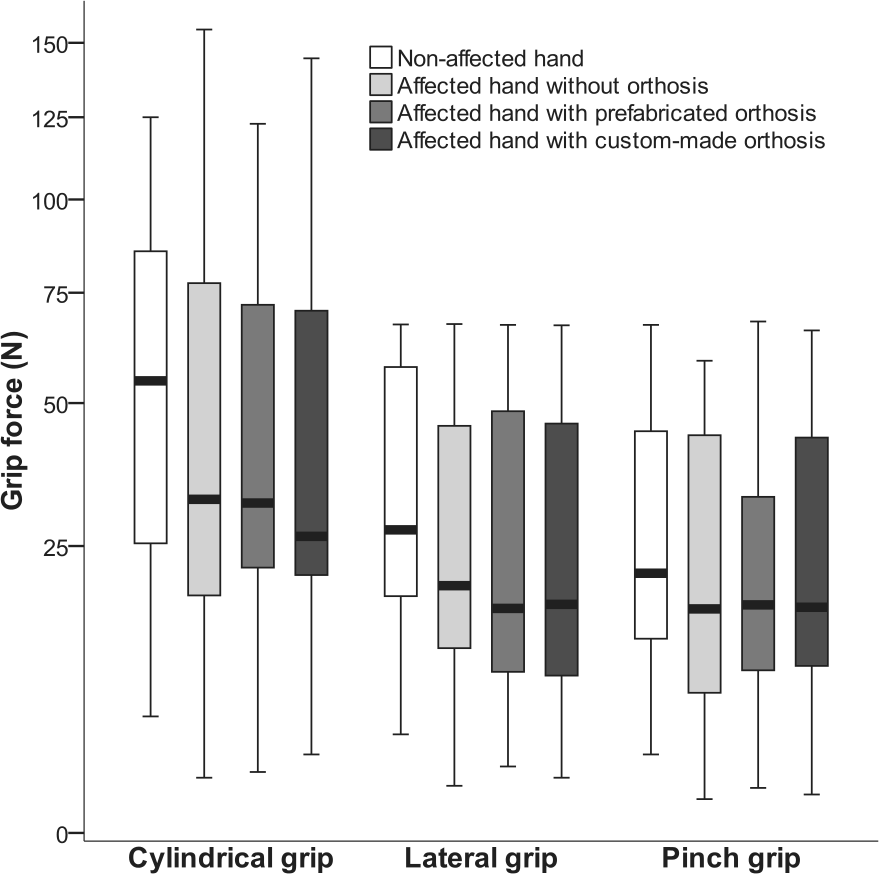
Box plots depicting all the measurements.
All the participants were introduced to the aims of this study and the procedure for the measurements and gave informed consent. Data on gender, age, affected hand, and occupation of the candidates were acquired from medical documentation. This study was approved by the local research ethics board.
Results
In total, 31 persons with symptoms of CTS were treated at the outpatient clinic for rehabilitation of persons with upper limb impairments at the University Rehabilitation Institute, Republic of Slovenia, from February to September 2008. Eight of the treated persons did not meet the inclusion criteria. In this study, 23 persons were asked to participate; 3 of them refused the request.
Hence, there were 20 participants: 18 women and 2 men. The mean age of the group was 49 years (range = 29–77 years). The most frequent occupation was unskilled worker (8 participants), followed by clerical work (6), seamstress (2), and the other occupations (mason, warehouseman, dental assistant, physiotherapist; 1).
In all the participants, the dominant hand was affected. It should be noted that one subject was recorded as having the nondominant hand affected, but she has been forced throughout her schooling to use this hand for writing and eating. She does not call it dominant, but she uses it in everyday routine as the dominant hand, so we considered her as a person with affected dominant hand.
On the affected hand, the type of orthosis (or lack thereof) did not have a significant effect on grip strength (p = 0.661), while there were significant differences between the different grips (p < 0.001). Cylindrical grip was by far the strongest, followed by lateral and pinch grips (Table 1, Figure 2). The two main effects could be unambiguously interpreted because there was no significant interaction between the two factors (p = 0.771). Compared to the nonaffected hand, the grips of the affected hand were significantly weaker (p = 0.002), which holds for each grip type because there was no significant interaction (p = 0.312).
Because the orthoses did not have a significant effect on grip, the affected hand without orthosis was used in comparison with the nonaffected hand as representing the affected hand of the participant in general, that is, whether wearing any of the tested orthoses or not. The clear decreasing order of strength from cylindrical through lateral to pinch grip was confirmed (p < 0.001 for the overall effect of grip and p ≤ 0.001 for the pairwise comparisons; Table 1).
Discussion
To first summarize the results, we found that in persons with CTS, the grip of the affected hand is weaker than the nonaffected hand and that there is no significant effect of orthoses used (whether custom-made or prefabricated) on the grip strength of the affected hand.
The main difference between the two orthosis types compared in our study was the position of the wrist. Several studies26–29 suggest that the strongest grip strengths are at 15°–30° of wrist extension and 0°–5° of ulnar deviation. On the basis of their studies, we had expected that prefabricated wrist orthosis would offer higher grip strength. However, as already noted, one study 8 presented results indicating that the wrist angle that produced the lowest pressure on the median nerve in the carpal tunnel is within 2°–3° of flexion and 1°–2° of ulnar deviation of the wrist. This raises the question of whether optimal release of the median nerve has an immediate influence on the strength of the affected hand in persons with CTS. However, we found no immediate influence of wrist position on the three measured grip strengths in persons with CTS.
The shape of the wrist orthoses is a factor that may have influenced our results. We decided to choose a custom-made volar thumbhole orthosis to be compared with a prefabricated one because we estimated that grasping and holding are less disturbed with volar rather than dorsal wrist orthoses. Volar thumbhole orthoses pass between the thumb and the second finger and cover only the proximal third of the palm. This shape offers good suspension and also better stabilization of the wrist position. But during the measurement procedure, we also noticed that with the custom-made volar thumbhole orthosis, grasping of the measurement units was more hindered than with the prefabricated one on the account of the plastic placed between the thumb and the first finger. It was most hindered when performing the cylindrical grip, followed by the lateral grip, while the least hindered was the pinch grip. Nevertheless, these differences did not seem to significantly influence our results.
Our results are not in complete agreement with those of Uğurlu et al., 13 who reported that custom-made volar thumbhole orthosis with wrist in neutral position reduces strength of lateral, palmar, and tip-to-tip grip in persons with CTS. Our results indicate that pinch grip is not reduced. In addition, four articles comparing grip strengths with prefabricated and custom-made orthoses in persons with RA14,16–18 reported on improved grip strength in persons with RA with different types of orthoses. However, one has to consider the differences in the purpose of orthotic application in the cases of RA and CTS. Orthoses for the rheumatoid hand aim to relieve pain, maintain position of function (20°–30° of wrist extension), discourage abuse of affected wrist, and assist function (pre- and postsurgically). 30 In contrast, the purpose of orthotic management in cases of CTS is immobilization of the wrist in a neutral position to minimize the pressure on the median nerve in the carpal tunnel. Furthermore, four articles and a systematic review reported that orthotic treatment in persons with RA has no effect or decreases grip strength.15,19–22 Similar results have also been obtained in studies on persons without disability23,24 and persons with chronic stroke. 31
Our results demonstrated that custom-made thermoplastic orthoses with wrist in neutral position do not have an immediate effect on grip strength for patients with CTS immediately after fitting. Custom-made orthoses with wrist in neutral position do not seem to have a better effect on the grip strength than prefabricated orthoses with wrist in 20° of wrist flexion.
Although there is no evidence that wearing an orthosis full time is better than wearing it only at night, 3 we share the opinion of Werner 32 that wearing the orthosis during the work activities that provoke symptoms may be helpful. In patients with CTS, more attention should be placed on the prevention of damaging movements of the wrist during work activities, whereby the lack of a clear effect of the orthosis on grip strength is at least not a limiting factor.
In addition to a relatively small sample size, a notable limitation of our study is that we did not repeat measurements after some time of wear. A further limitation is that we did not randomize the order of testing or repeat measurements on a second occasion to test for repeatability of the method.
Conclusion
Our results in persons with CTS indicate that neither prefabricated orthoses (with wrist position in 20° of extension) nor custom-made wrist orthoses (with wrist in neutral position) influenced grip strength of the affected hand immediately after fitting them. In the affected hand with or without an orthosis, as well as in the nonaffected hand, strength decreased from cylindrical through lateral to pinch grip. Compared to the nonaffected hand, the grips with the affected hand without orthosis were weaker.
Footnotes
Conflict of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.