
Abstract
Background:
Different types of splints have been used as a conservative intervention to improve symptoms in patients with Carpal tunnel syndrome (CTS). Although a number of studies have been undertaken to compare different splints, information and understanding of the influence of these interventions are lacking.
Objectives:
The purpose of this study was to compare the effect of a classic thermoplastic wrist splint or a wrist splint with an additional metacarpophalangeal unit on pain, function, grip strength, and pinch strength in patients with mild-to-moderate carpal tunnel syndrome.
Study design:
Quasi experimental design.
Methods:
A total of 24 patients received conservative treatment using either the classic wrist splint or the wrist splint with the metacarpophalangeal unit for a period of 6 weeks. Primary outcome measures were pain, function, grip strength, and pinch strength. Data were collected immediately before and after using the two types of splints at baseline (0 weeks) and 6 weeks. Statistical analysis was performed using the paired t-test and an independent t-test.
Results:
Compared to baseline, both the classic thermoplastic wrist splint and the wrist splint with a metacarpophalangeal unit significantly decreased pain and increased function, pinch strength, and grip strength. Comparisons of the two types of splints for grip strength (P = 0.675) and pinch strength (P = 0.650) revealed that there were no significant differences between the two after 6 weeks of wear. However, there were significant differences in pain levels (P = 0.022) and the Disability of the Arm, Shoulder, and Hand score (P = 0.027) between the two types of splints from baseline to 6 weeks.
Conclusion:
The wrist splint with a metacarpophalangeal unit was more effective than the classic thermoplastic wrist splint in pain reduction and improvement of function.
Clinical relevance
A wrist splint with a metacarpophalangeal unit may be an appropriate conservative treatment in the rehabilitation of patients with mild-to-moderate carpal tunnel syndrome.
Keywords
Background
Carpal tunnel syndrome (CTS) is the most commonly seen entrapment neuropathy of the upper limb, 1 with a prevalence of 9.2%–15.6% in females and 6%–11.3% in males.2,3 This type of condition can occur in all age groups, but the prevalence of bilateral CTS is most frequently seen in subjects between the ages of 40 and 60 years. 4 The prevalence of CTS has been reported in the United States and the United Kingdom as being 5% and 7%–16%, respectively.5,6
Compression of the median nerve classically produces the symptoms typically presented. It also results in a reduction in the ability to perform activities of daily living (ADLs). The symptoms commonly occur at night and usually cause sleep disturbance. 7 Splinting, exercises, and ultrasound therapy are commonly used conservative approaches for the treatment of mild-to-moderate CTS.8–10 Surgery is performed in patients with severe symptoms, which is, in turn, associated with muscular atrophy and sensory loss. 11 However, wrist splinting is the most frequent conservative method used in the treatment of CTS. 12 Pain in the hand and tingling and numbness in the thumb, index finger, middle finger, and the radial side of the ring finger are commonly seen symptoms in people with CTS. 13 This can often be accompanied by an increase in pain at night and during activities which induce wrist flexion. 14 Grip strength and hand function may also be reduced. 15
Previous studies have suggested that wrist splints can produce positive effects in patients with CTS. One prospective study reported that neutral splints relieved symptoms more than cock-up splints with the wrist placed in 20° of extension. The authors also reported that symptomatic relief was observed in the first 2 weeks of using the splint, but no additional improvement was demonstrated between weeks 2 and 8 of splint use. 16 It is thought that wrist splints support the wrist in an anatomic position and prevent flexion and extension, which, in turn, can reduce pressure within the carpal tunnel.17,18
A flexed position of the metacarpophalangeal (MCP) joints causes an increased pressure in the carpal tunnel.19–23 Manente et al. 24 reported that CTS symptoms decreased and the function of patients increased when patients with CTS used a hand brace. The hand brace was made of soft material without rigid components in their study. This orthosis produced mild stretching of digits III and IV to prevent of lumbrical migration in carpal tunnel. The hand brace did not impede wrist flexion and extension. In addition, only the third and fourth digits were supported in an extended position. In a randomized controlled trial, De Angelis et al. 25 reported no significant differences between a wrist splint and hand brace when analyzing the resulting symptom severity scores.
From an anatomical perspective, the lumbrical muscle is a structure which makes up part of the carpal tunnel. Baker et al. 26 noted that a combination of wearing a cock-up splint with concurrent intensive lumbrical stretches was the most effective approach compared to a lumbrical splint or lumbrical stretch group, lumbrical splint or general stretch group, or cock-up splint or general stretch group. While this appeared to be a positive result, additional evidence on the effectiveness of a hand and wrist splint for the treatment of CTS is needed. Moreover, more effective conservative methods are required for treatment of mild-to-moderate CTS.
In a comparison of the effect of a neutrally positioned splint which covered both the wrist and MCP joints with a neutral splint covering the wrist only, and with and without exercises for the treatment of CTS, Brininger et al. 27 reported that a splint which supported the wrist and MCP joints may be more effective than a wrist splint alone in treatment of patients with long-standing CTS symptoms. The aim of this current study was, therefore, to compare the effect of a neutral wrist splint and also a wrist splint with an extended trim line to control the MCP joints on pain, function, grip strength, and pinch strength in newly diagnosed patients presenting with mild-to-moderate CTS.
Methods
A total of 24 patients (4 men and 20 women) who were referred by an orthopedic hand surgeon to the orthotics clinic participated in this study. Nerve conduction studies (NCSs) were used to diagnose CTS in the subjects, who were classified as suffering from mild, moderate, or advanced CTS according to the American Association of Electro-diagnostic Medicine guidelines. 28 However, only patients with mild or moderate CTS were invited to participate in this study. Each patient met the following criteria: being over 18 years of age; having a positive Tinel’s sign or Phalen maneuver; and having reported with nighttime pain, numbness, and tingling during the previous 12 months. In addition, patients who presented with neuropathy (e.g. due to diabetes mellitus or thyroid disease), thenar atrophy, or those having had a steroid injection into the carpal canal within the previous 3 months or a carpal tunnel release procedure were excluded from this study. Therefore, all subjects had a history of CTS. The University of Social Welfare and Rehabilitation Sciences approved this study. Written informed consent was obtained from all patients prior to participation in this study.
Interventions
Patients in this study were divided into two groups (those who wore a neutral wrist splint and those who wore a wrist splint with an extended trim line to control the MCP joints) using a randomized allocation. In this study, a neutral wrist splint was used as a control intervention. This splint was custom-made according to the dimensions of the MCP joints, wrist, and forearm regions but not molded. The wrist splint with an MCP unit was custom molded according to the patient’s hand casting in the aforementioned position. The fit of both test conditions on the hand and wrist was checked prior to testing at baseline. The splints were custom fabricated for each subject in order to position the wrist in neutral alignment (0°) according to the dimensions of their MCP joints, wrist, and forearm and a plaster cast. The wrist splint with an MCP unit incorporated was custom molded with the wrist in a neutral (0°) position and the MCP joints positioned between 0° and 10° of flexion. The distal edge of the neutral wrist splint ended proximal to the second to fifth MCP joints, so that these joints could flex freely and extend without movement limitation (Figure 1, A). In the other splint (i.e. a wrist splint with an MCP unit), the distal edge of splint ended just proximal to the proximal interphalangeal (PIP) joints, so that MCP joints were restricted, but PIP joints had unlimited movement (Figure 1, B). Both splints were checked for correct fitting prior to testing. The MCP joint of the thumb was free to move in either of the splints.
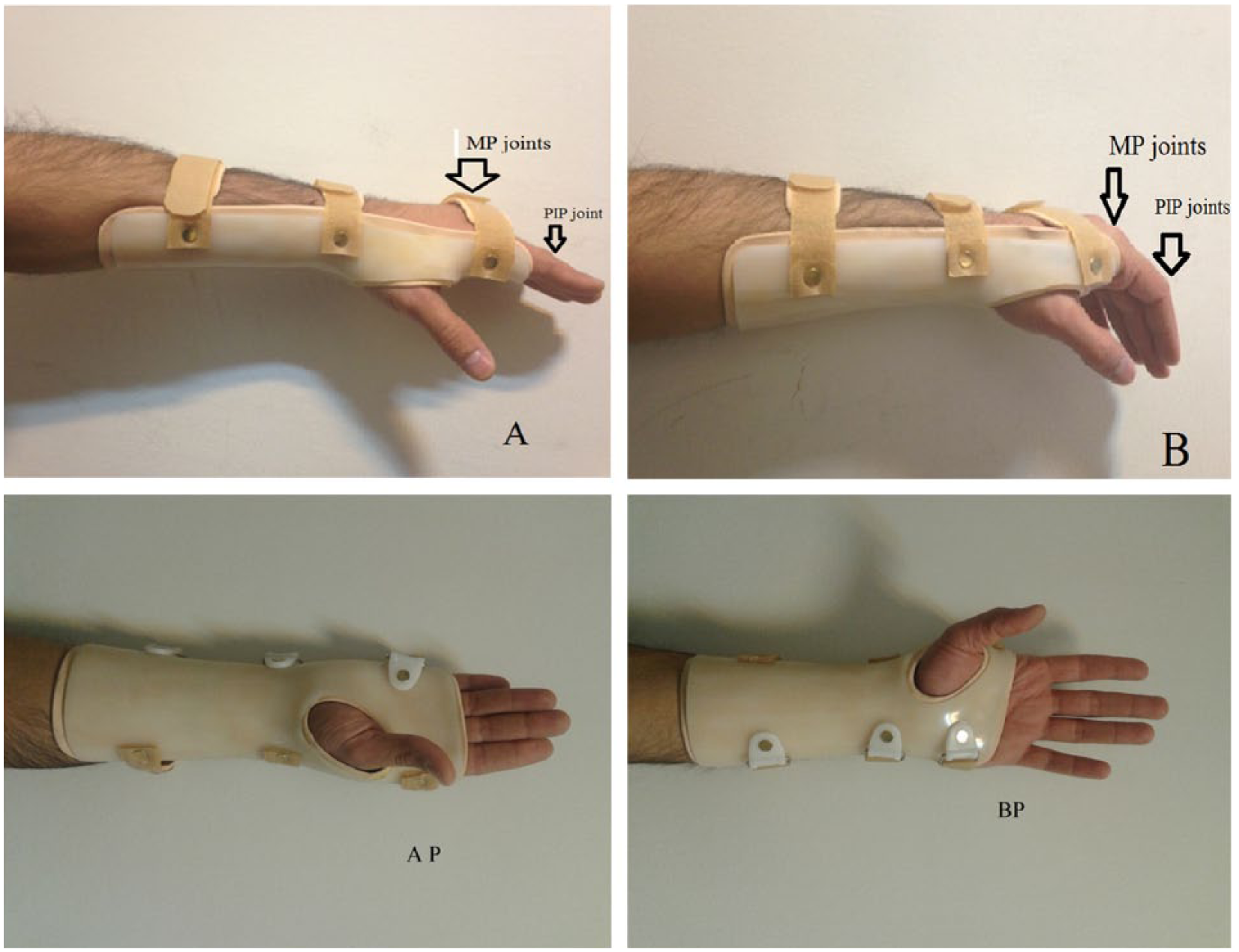
Wrist splint with an MCP unit (A and AP) and the neutral wrist splint (B and BP) used in this study.
The orthoses were fabricated for each patient using 4-mm-thick thermoplastic material (polypropylene, Tavan Sazan company, Inc., Iran). After the splint was prepared and manufactured, nonelastic Velcro© closures were added (Figure 1) to reduce relative movement between the hand and wrist and the splints. All patients were advised to report any discomfort when using the splint. The patients were asked to use the splints during the nighttime and also at daytime whenever possible for 6 weeks. Patient comfort when wearing each splint was checked on a weekly basis.
Outcome measures
A visual analog scale (VAS) was used to evaluate pain.29,30 The VAS was based on a 100-mm straight line scale (0 = no pain, 10 = the most severe pain). Patients were requested to report on the maximum pain that they had experienced for the activities over the last week at baseline and after 6 weeks of orthosis use. Patients indicated the intensity of the sensation being experienced by placing a mark on the VAS line.
The Disability of the Arm, Shoulder, and Hand (DASH) questionnaire was used to determine function.29–31 The questionnaire was completed by each patient 1 day before beginning the orthotic intervention and again after 6 weeks after orthosis use. The DASH score has 30 questions which assess function and symptoms. The following themes are included: physical function (two questions), symptoms of disease (six questions), social aspects (three questions), and two optional modules (four questions) for workers and athletes.
Grip strength and key pinch were measured using a dynamometer (model PC 5030 J1, Jamar Hydraulic Hand Dynamometer, JAMAR technology Inc, USA) and pinch gauge (model PC 7498-05, Jamar Hydraulic Pinch Gauge, JAMAR technology Inc, USA). For assessment of grip strength and pinch strength, patients were seated with the elbow flexed at 90° and with the wrist in a neutral position between pronation and supination.29–31 Pain, function, grip strength, and lateral pinch were measured at baseline and at 6 weeks in the two groups. All tests conducted were by an orthosist who was trained to administer the tests. The extent of splint use during the test period was recorded via patients self-reporting the data.
Statistical analysis
The Kolmogorov–Smirnov technique was used to determine the normal distribution of the data. To evaluate the effect of the two splints on pain, function, grip strength, and pinch strength, a paired t-test (according to the normality of the data) was used to analyze the effects and differences in the selected outcome measures between the baseline and after 6 weeks of using splints. An independent t-test was applied to determine differences in the selected outcome measures between the two splints. SPSS statistical software was used for the analysis of the data. The level of significance was set at 0.05.
Results
There were no significant differences in the age, weight, height, time of splint use, dominant hand, affected hand, duration of injury, pain, function, or grip strength between the two groups at baseline. All patients continued their contribution to the end of the study period. The characteristics of the patients who participated in this study are presented in Table 1.
Characteristics of patients who participated in this study.
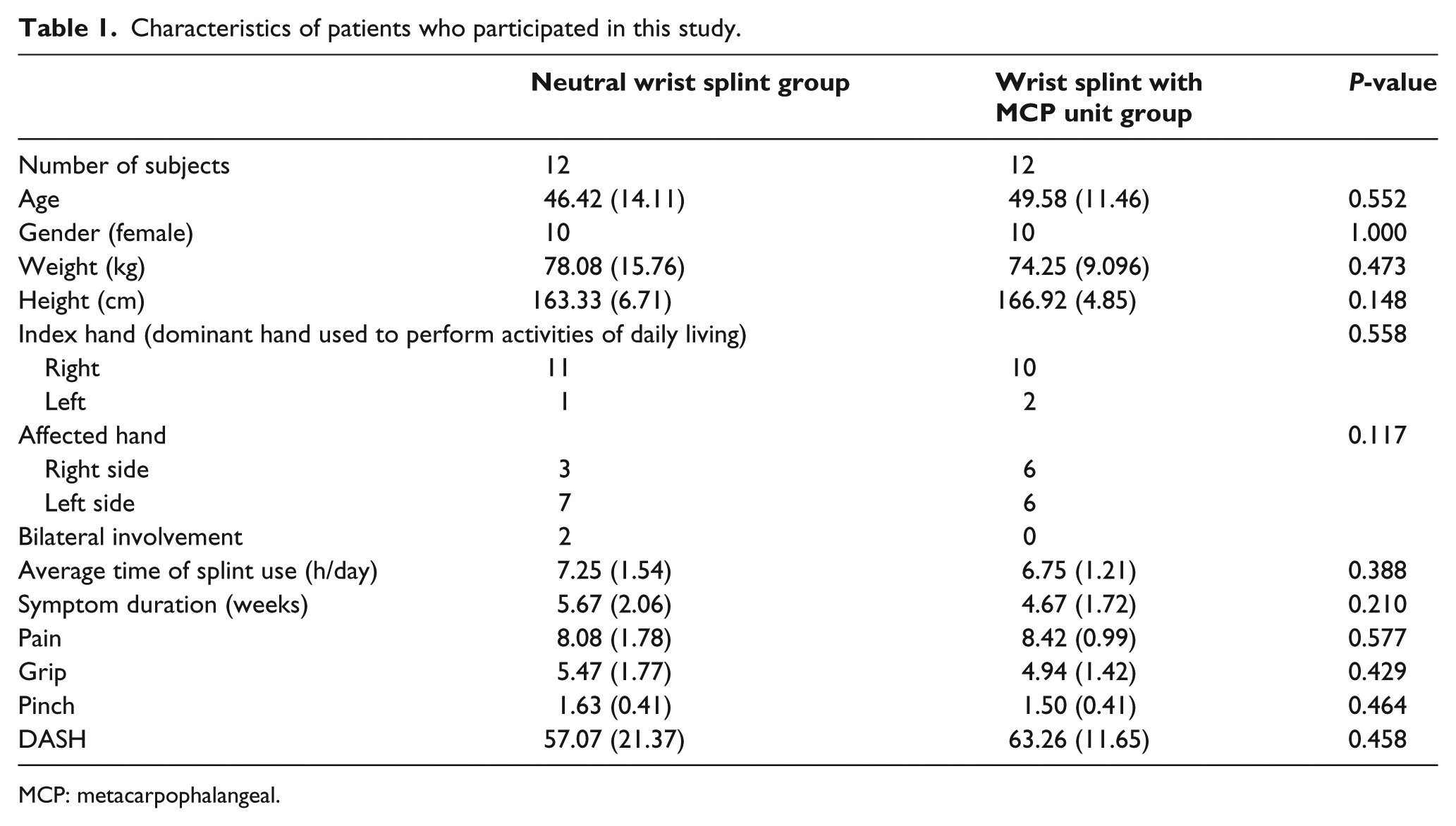
MCP: metacarpophalangeal.
Using the neutral wrist splint and wrist splint with an MCP unit significantly decreased pain (P = 0.000, 0.022, respectively) and increased pinch strength (P = 0.000, 0.000, respectively), grip strength (P = 0.040, 0.002, respectively), and function (P = 0.000, 0.000, respectively) compared to baseline at the end of the sixth week of splint use (Table 2).
Inter and intra group comparison between neutral wrist splint and wrist splint with MCP unit groups for the selected parameters after 6 weeks of use.
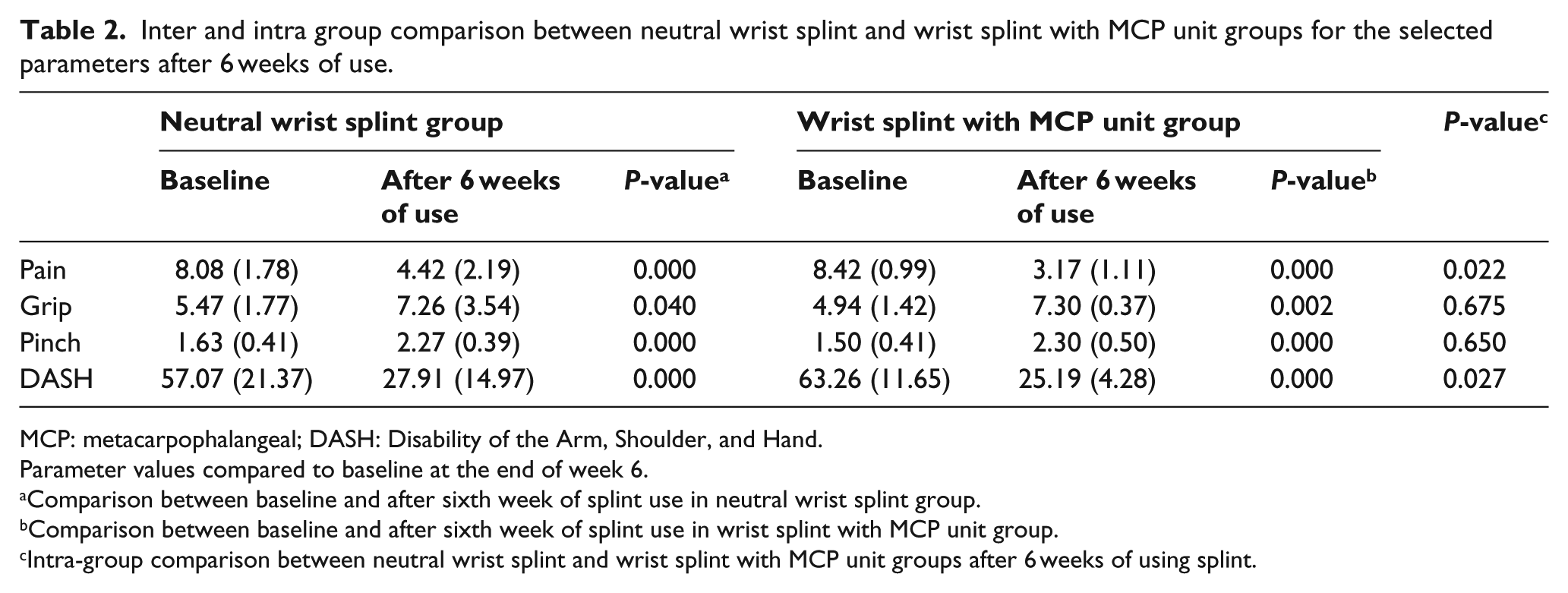
MCP: metacarpophalangeal; DASH: Disability of the Arm, Shoulder, and Hand.
Parameter values compared to baseline at the end of week 6.
Comparison between baseline and after sixth week of splint use in neutral wrist splint group.
Comparison between baseline and after sixth week of splint use in wrist splint with MCP unit group.
Intra-group comparison between neutral wrist splint and wrist splint with MCP unit groups after 6 weeks of using splint.
Comparison between splint types
When comparing the two types of splints on grip strength (P = 0.675) and pinch strength (P = 0.650), there were no significant differences between the neutral wrist splint and wrist splint with MCP unit after 6 weeks of splint use. However, there were significant differences in pain levels (P = 0.022) and DASH score (P = 0.027). The wrist splint with the MCP unit, therefore, demonstrated a better effect in decreasing pain and improvement of function (Table 2).
Discussion
Different types of splints have been used as a conservative intervention to improve symptoms in patients with CTS (8). Although a number of studies have been undertaken to compare different splints, information and understanding of the influence of these interventions are lacking. In this study, the authors used four important outcome measures to evaluate the effectiveness of a traditional splint and wrist splint with MCP unit to treat mild-to-moderate CTS. According to the prevalence of CTS, this study was matched with previous studies for patient demographics. More women than men participated in this study, and on average, the subjects were middle-aged.2,32,33 In this study, 83% of the participants were female.
The main result of this study was the improvement noted by all patients over the 6-week period with the use of the two types of splints. Both splints produced limitation of wrist joint motion, which, in turn, appeared to improve pain, function, grip strength, and pinch strength parameters after 6 weeks of splint use. These results were consistent with other studies in this field.34,35
In comparison, it was noted that for the two types of splints, there were no significant differences between grip strength and pinch strength at the end of the 6-week period, but there were significant differences between pain and DASH score. Restriction of migration of lumbrical muscles in the carpal tunnel may cause pressure relief in this tunnel and provide more pain reduction compared to a neutral wrist splint.
According to the position of the lumbrical muscles, there was a significant difference between the patient group who wore the neutral wrist and MCP extension compared to the patient group who wore the neutral wrist splint. Using the wrist splint with the MCP unit placed the MCP joint in 0°–10° of flexion. Wearing the splint in this position prevents displacement of the lumbrical muscles in the carpal tunnel and, therefore, may have decreased pressure in the carpal tunnel. This observation supports previous findings that demonstrated the flexion of MCP joints cause migration of lumbrical muscles into the carpal tunnel and provide carpal tunnel pressure.21,23
Synergistic performance of intrinsic and extrinsic muscles of the hand can provide grip power. The median nerve is proximal to the carpal tunnel, and the ulnar or radial nerve innervates these muscles. 36 The strength of the flexor pollicis longus which is innervated by the median nerve proximal to the carpal tunnel and the flexor pollicis brevis which has inconsistent innervations with variable contribution from the median and ulnar nerve can affect key pinch strength. 32 In addition, abductor pollicis brevis or opponens pollicis weakness or pain may be compensated for during key pinch by synergistic muscle action or “trick” movements.37,38
Strength in the affected hand has been shown to be reduced by as much as 10%–30% compared to normal values seen in the subjects with CTS. 32 Although wearing both types of splints improved strength in this study, 6 weeks of splint use did not return the hand to the normal mean value of strength shown in healthy participants. There was no significant difference in this variable between the two groups. Long-term follow-up of the effect of wearing a wrist splint with a lumbrical unit may provide an increase in grip strength and pinch strength. A guideline about the time required for grip strength to return to the preoperative level after carpal tunnel release has not been published. However, Gellman et al. 39 noted that grip strength may require up to 3 months postoperatively before returning.
In this article, the design of a new modified splint on the efficacy of splinting for CTS is discussed, as there is limited evidence regarding the effect of splints designed to place the wrist and MCP joints in a neutral position for patients with CTS. The aim of this study is to provide scientific evidence for the choice of the orthotic treatment for CTS patients. Our results provide further evidence of the effectiveness of a wrist splint with an extended trim line to control the second to fifth MCP joints, designed and based on an anatomic problem, decrease symptoms, and improve functional problems in patients with mild-to-moderate CTS.
Since this study followed patients for only 6 weeks, future research should focus on evaluating the effectiveness of these types of splints over a longer term to provide more information for the long-term treatment of CTS. The results of this study do not support the superiority of the wrist splint with MCP unit over neutral wrist splint in improvement of grip strength and pinch strength in treating CTS. Unfortunately, muscle testing and testing of different functional grips were not used in this study. Additional study in this field will be beneficial for measuring the impact of the splints. Future studies, with larger sample sizes and a combination of splint usage and an upper limb exercise program is required to determine the effectiveness of these splints in the treatment of CTS over a longer period of time. In addition, the use of elastic touch and close strapping was not used in this study but may have increased the circular effect of the splints in controlling motion. Modern splinting techniques, such as the use of modern low temperature directly moldable thermoplastics, should also be utilized in future studies.
Conclusion
CTS has been reported as being the most prevalently diagnosed upper-extremity dysfunction. Providing effective conservative interventions for the treatment of mild-to-moderate CTS should be given superiority. The aim of this study was to compare the effects of a neutral wrist splint and wrist splint with MCP unit, for the treatment of mild-to-moderate CTS. The results of this study provide additional evidence of the effectiveness of splinting for decreasing symptoms and improving hand performance in patients with mild-to-moderate CTS.
Both splints (a neutral wrist splint and a wrist splint with an MCP unit) reduced pain and increased function, pinch strength, and grip strength when compared to baseline and after 6 weeks. There were no statistical significant differences in grip strength and pinch strength between the two splints, but the wrist splint with MCP unit was significantly more effective than the neutral wrist splint in pain reduction and improvement of function. While further research is required, this study suggests that both splint designs are helpful in the short term for patients with CTS.
Footnotes
Author contribution
All authors contributed equally in the preparation of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.