
Abstract
Background:
Kinetic data provide important information about the mobility performance of individuals with lower limb impairments and their assistive devices; however, there is limited understanding of this in real-life environments.
Objective:
To evaluate the effect of real-life irregular surfaces on forces and moments in knee–ankle–foot orthoses.
Methods:
In this case series study, a load cell was used to measure the forces and moments at the knee joint of knee–ankle–foot orthoses of individuals with unilateral muscle weakness as a result of poliomyelitis while walking on different ground surfaces and at different speeds.
Results:
Significantly higher shear forces and external peak knee flexion moments were found when walking on irregular surfaces. In individual cases, certain irregular ground conditions elicited large increases in peak flexion moments (>50%) when compared to walking on smooth level ground. Forces and moments were significantly higher at faster walking speeds.
Conclusions:
Higher external peak knee flexion moments during the stance phase suggest that greater demands for support and stability are placed on individuals and their assistive devices when negotiating real-life ground surfaces.
Clinical relevance
This study demonstrates that walking on irregular surfaces alters the loads placed on knee–ankle–foot orthoses and that the requirements for knee stabilization increase. This has important clinical implications on the design, prescription, and use of such devices given the structural and functional demands placed on them.
Introduction
The internal joint moments in our lower limbs generated by our muscles play a key role in human locomotion by facilitating postural support and forward progression of our body. 1 Without adequate torque generation at the three main skeletal joints, including the ankle, knee, and hip, the limbs would not only be unable to extend to propel us forward during stance but also be collapsed under the weight of the upper body.1,2 Because of their importance in human mobility, joint moments have been extensively studied in humans during steady-state level ground walking and also using paradigms representing aspects of more diverse and real-life ambulatory conditions. These include changing gait speeds; initiating, terminating and transient gait;3–6 crossing and avoiding obstacles;7,8 and negotiating stairs, slopes, and various ground surface compositions and topologies.9–11 Simulating outdoor walking environments in the lab is another approach that has been utilized to gain insight into real-life mobility; however, this is limited by the validity of the artificial conditions as well as challenges in accurately measuring kinetics.10,12 Other approaches have opted to test under real-life conditions utilizing portable instrumentation that can be worn in out-of-lab environments by the subjects to measure variables such as accelerometer-based dynamics and energy expenditure.13–16 However, although these approaches provide important information about real-life demands, they do not allow for quantification of lower limb joint kinetics. As a result, the effects of common outdoor ground surfaces on lower limb kinetics are not well established in the literature.
The study of lower limb joint kinetics is not limited to able-bodied individuals but is essential for the investigation of pathological gait patterns. Such information can be used to assist clinical assessments and diagnoses of patients and to evaluate the efficacy of interventions.2,17,18 Where muscle function is severely diminished, such as in the case of poliomyelitis and other pathologies, ambulation may only be possible with the assistance of mobility devices such as orthoses. In such cases, orthoses work by passively applying torques to resist flexion, thus stabilizing the joints in the lower limbs. In more mild cases of impairment, stabilizing the ankle joint against dorsiflexion is often adequate, but in more severe cases, additional sagittal-plane stabilization may be needed at the knee joint to prevent the knee from collapsing during stance. 19 This type of orthosis is typically termed a knee–ankle–foot orthosis (KAFO). Understanding the loads that these devices are subjected to during gait has been an important area of study aimed at improving device function and ultimately patient outcomes.20–23
To accurately measure loads in orthoses, it is necessary to directly instrument them using load transducers. 24 A small number of case series have utilized this approach to provide initial insights into the loads present in KAFOs and the factors that affect them. Andrysek et al. 24 and subsequently Bernhardt and Kaufman 21 have found that measured at the lateral knee joint of KAFOs, the largest moments and forces were present in the sagittal plane and vertical/axial direction, respectively. This corresponds to the kinetics of able-bodied gait, as well as to the primary role of KAFOs, which is to stabilize the lower limb and prevent knee flexion during stance. Specific factors affecting KAFO loading that have been investigated include patient weight, which was not shown to positively correlate with KAFO forces and moments, as one might assume. 21 The influence of orthosis setup and alignment on sagittal-plane moments has also been investigated, although primarily in the context of stance-controlled orthoses. 25 In summary, much remains to be understood about the loads imposed on KAFOs under clinically relevant and real-life conditions.
In this regard, the main aim of this investigation was to compare the loads on a KAFO knee joint in users with quadriceps weakness walking on different outdoor surfaces. In obstacle-crossing studies, greater environmental demands were shown to require greater muscular strength and to increase stance knee flexion moments. 7 Furthermore, accelerometer-based gait studies have associated more challenging ambulatory conditions with increased magnitudes of body accelerations, suggesting increased demands on the lower limbs.7,12,14 We therefore postulated that irregular ground conditions place greater demands on knee joint stabilization and that knee joint forces and moments providing support during stance would increase as a result. A secondary aim of this study was to examine the effect of walking speed. We further postulated that KAFO joint forces and moments would increase at faster walking speeds.
Methods
Participants
A convenience sample of participants was recruited from the outpatient clinic at a rehabilitation center. Participants were (1) diagnosed with poliomyelitis or post-poliomyelitis, (2) at least 18 years old, (3) using a KAFO for mobility, and (4) good functional ambulators when using their orthoses, including walking in the community (based on self-report). The research was approved by the institution’s ethics committee. All investigations were conducted in accordance with the protocol and followed ethical and humane principles of research. Informed consent was obtained from the participants. Participants were clinically assessed, and KAFOs for testing were fabricated using standard techniques and components, as previously described in more detail. 24
Instrumentation
Orthotic loads were measured using a commercially supplied 6-degrees-of-freedom load cell (MCW-6-XX 1000; Advanced Mechanical Technology, Inc., Watertown, MA, USA), which was incorporated in place of the lateral knee joint of the participants’ KAFOs, aligning one of the sensing axes of the load cell with the knee axis of the KAFO as shown in Figure 1 and described in detail previously. 24 Signals were captured and stored using CRONOS LPL-2 DIO 8-analog channel amplifier/data acquisition system with imc DEVICES 2.5 and FAMOS software programs (imc DataWorks, Madison, WI, USA). To make the system portable, it was powered by a 12-V, 10-Ah rechargeable nickel–metal hydride (NiMH) battery pack. The control and display unit comprised a remote hand-held terminal (imc DataWorks) programmed to receive inputs and display information. Operator inputs were needed to identify the condition that was being evaluated and to mark the start and end of each of these events so that walking velocity could be calculated. They were also used to mark adverse events. Displayed information included values for the relevant gait parameters being measured and whether the system was recording or in standby mode. System components, including the amplifier/data acquisition system and battery pack, were packaged into a backpack.
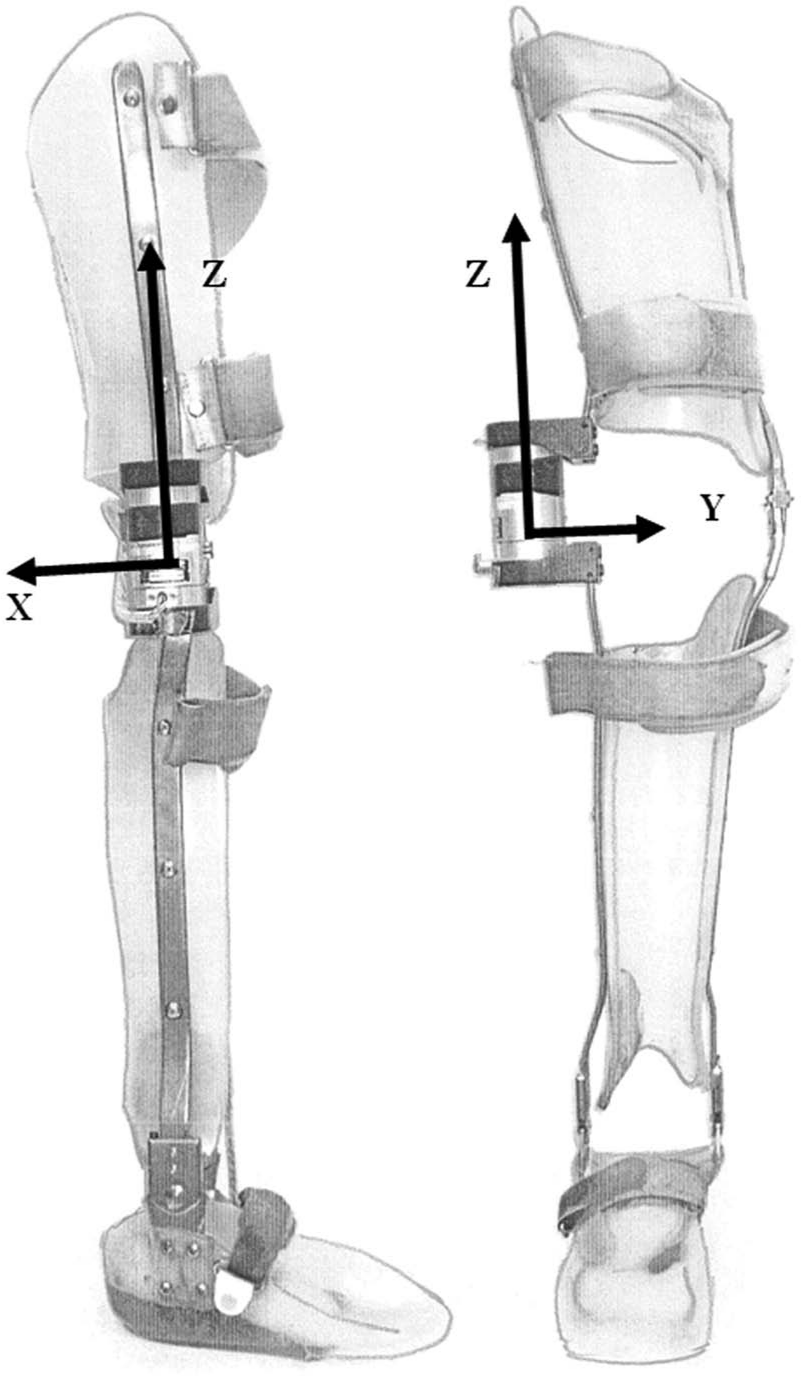
Instrumented KAFO showing load cell and coordinate system.
Protocol
An outdoor course incorporating the environmental features of interest was determined. These features were chosen partly based not only on their proximity to our facility but also on their applicability to real-life ambulation. These include mulch (MUL), gravel (GRVL), grass (GRA), rocks (ROC), and sand (SND), which were all compared to level ground (GRD) as described in Table 1.
Description of testing surfaces and test conditions.
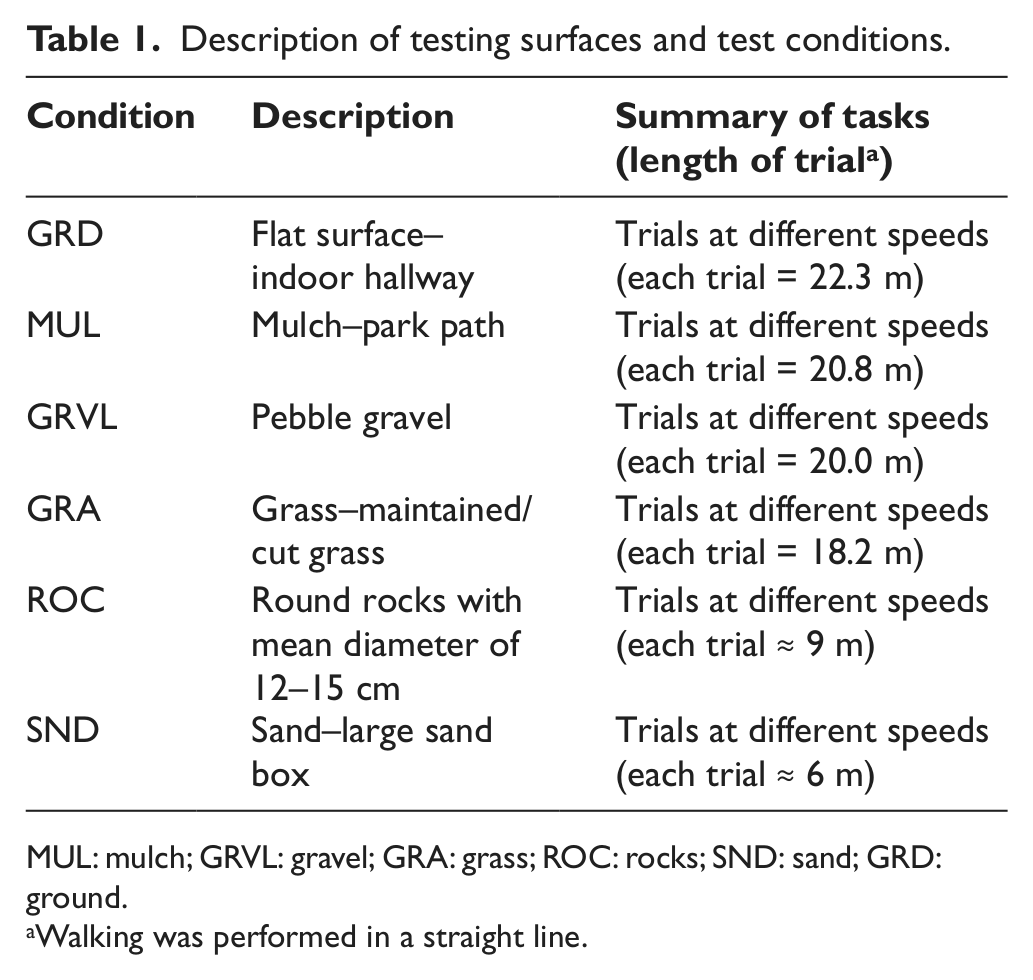
MUL: mulch; GRVL: gravel; GRA: grass; ROC: rocks; SND: sand; GRD: ground.
Walking was performed in a straight line.
The data collection for each subject was performed over a single session. While connected to a laptop, the channels of the amplifier/data acquisition system were initially balanced and zeroed. A baseline measurement was taken. The lateral orthotic knee joint was removed from the participant’s KAFO, and the load cell was attached in its place ensuring that the load cell axis was aligned with the knee joint axis. In this way, the load cell served the function of a locked lateral knee joint. The medial knee joint was kept locked during testing, which is how the participants normally used their regular KAFOs. It should be noted that by instrumenting the lateral side of the KAFO, we were able to capture a component/portion of the forces and moments, and not the overall loads passing through the lower limb. Force-sensitive resistor-based foot switches were used on the nonbraced side but were found to be unreliable on the irregular ground surfaces. Therefore, temporal data were instead based on features in the load cell measurements, namely, a sharp and well-defined increase in the axial load corresponding to the instance of heel strike.
The backpack containing the instrumentation was donned by one of the investigators. All signals were checked and the system disconnected from the laptop, to be operated by the investigator using the portable hand-held terminal device. Cables from the sensors were anchored at the participant’s belt area and extended to the backpack worn by the investigator. A 1- to 1.5-m-long tether between the subject and investigator was found to be optimal during pilot testing, providing minimal interference during gait.
Data were collected in the order specified in Table 1. The participants were instructed to first walk at their self-selected walking (SSW) speed and then at their fast walking (FW) speed. The investigator walked behind the participant to prevent pacing. A single pass was collected for each ground surface condition. Where the trial distance was long enough to allow for accurate measurement of gait velocity (i.e. >10 m), the pass was timed (Table 1).
Data analysis
For each trial, the braced limb heel strike events of the middle five strides were manually identified in FAMOS software, based on the load cell signals. Custom written MATLAB (MathWorks Inc., Natick, MA, USA) programs were used to normalize the stride times to 100% of gait cycle, generate curve ensembles, and extract relevant features of the curves including peak joint forces and moments at each of the three load cell axes. Cadence was calculated as the time between consecutive heel strikes. All forces and moments were normalized to body mass.
Single-tailed paired t-tests were used to examine differences in joint forces and moments between the combined irregular surfaces for which velocities were collected (MUL, GRVL, and GRA) and level ground surface (GRD) conditions. A single-subject analysis approach26,27 combining multiple samples from each subject was applied because of the small sample size. We adapted this technique by combining the irregular surface trials for the analysis, making it possible to determine whether differences existed between the GND condition and the irregular ground conditions. Level of significance was set at p < 0.05, and a correction applied in consideration of the two walking conditions.
Results
Three participants were included in this case series. A fourth participant was involved, but due to instrument malfunction, data for this individual were not usable. Subject 1 was a 34-year-old female weighing 84 kg, subject 2 was a 29-year-old male weighing 59 kg, and subject 3 was a 27-year-old male weighing 66 kg. Muscle weakness was unilateral for all participants with the nonaffected limb exhibiting normal muscle strength levels and function. Affected limb quadriceps strength for the three participants was 3, 1, and 1 based on the Oxford Scale where 0 represents no strength and 5 normal muscle strength. All participants had been using a KAFO for at least 2 years prior to the study, and none used additional walking aids. The KAFOs had manually locking knees. Subject 1 had an articulating ankle and subjects 2 and 3 had rigid ankles.
As seen in Figures 2 and 3 and Tables 2 and 4, overall, the results indicate that the magnitudes of forces and moments measured at the KAFO knee joint are dependent on the type of ground surface being walked on. Table 2 provides the individual subject results for each ground condition, while Table 4 provides the combined results comparing walking on even (GRD) and irregular ground surfaces (MUL, GRVL, and GRA) for the SSW and FW speeds, respectively. From Figures 2 and 3 and Table 2, large intersubject variability is evident; however, some overall trends can be inferred from these figures and also from Table 4. Specifically, walking on irregular surfaces significantly increased the peak frontal- and sagittal-plane moments (Mx and My) as well as anterior/posterior shear (Fx). However, transverse plane moments (Mz) were significantly reduced on irregular surfaces across both walking speeds. Average magnitudes of these changes ranged from 10.6% to 24.0% although individually certain irregular surface conditions elicited much larger differences (>50%) (Table 4 and Figures 2 and 3).
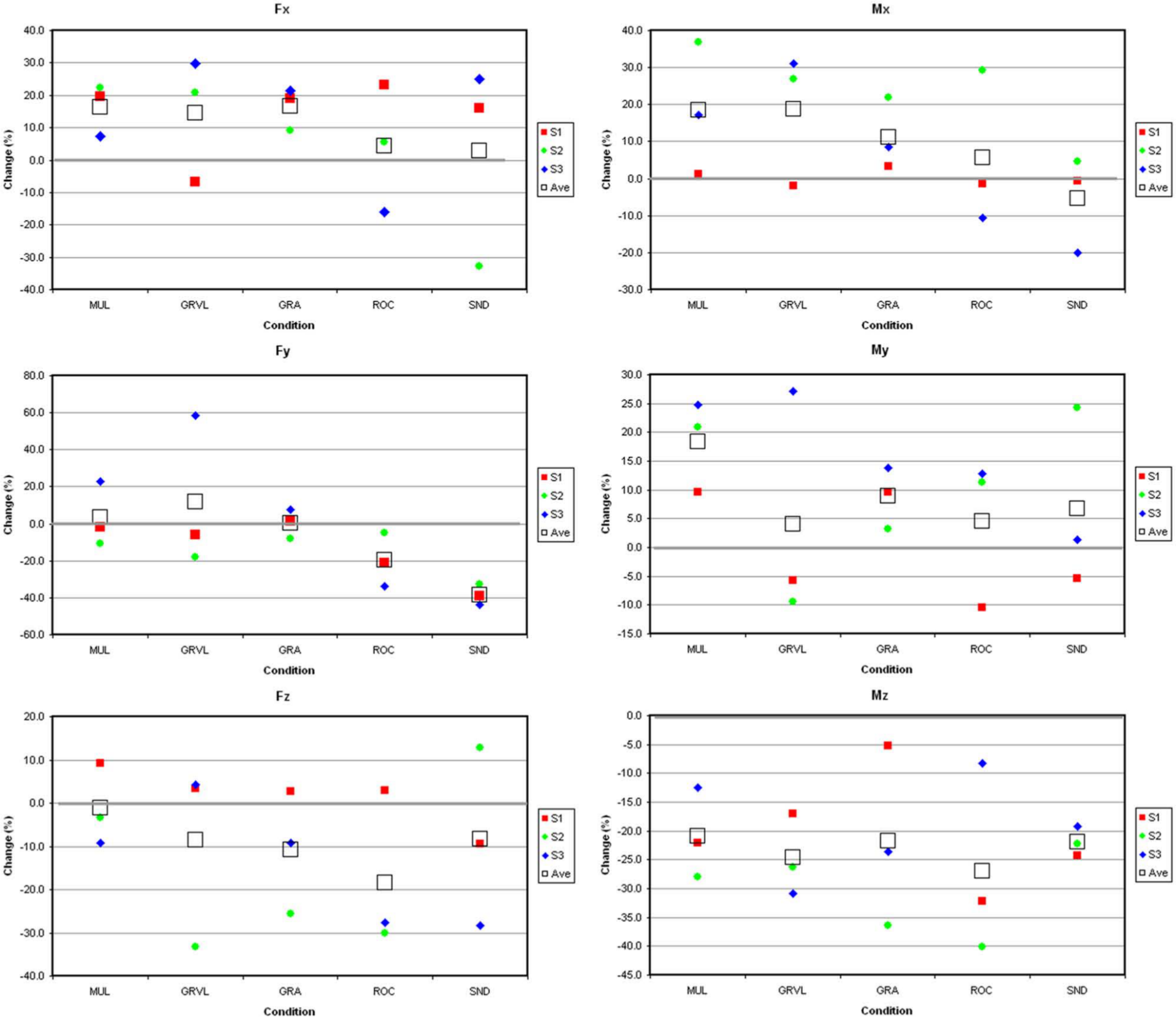
Percentage change in peak forces and moments compared to the level ground (GRD) condition for self-selected walking speed for individual subjects labeled S1–S3. Each data point is the average of five consecutive steps.
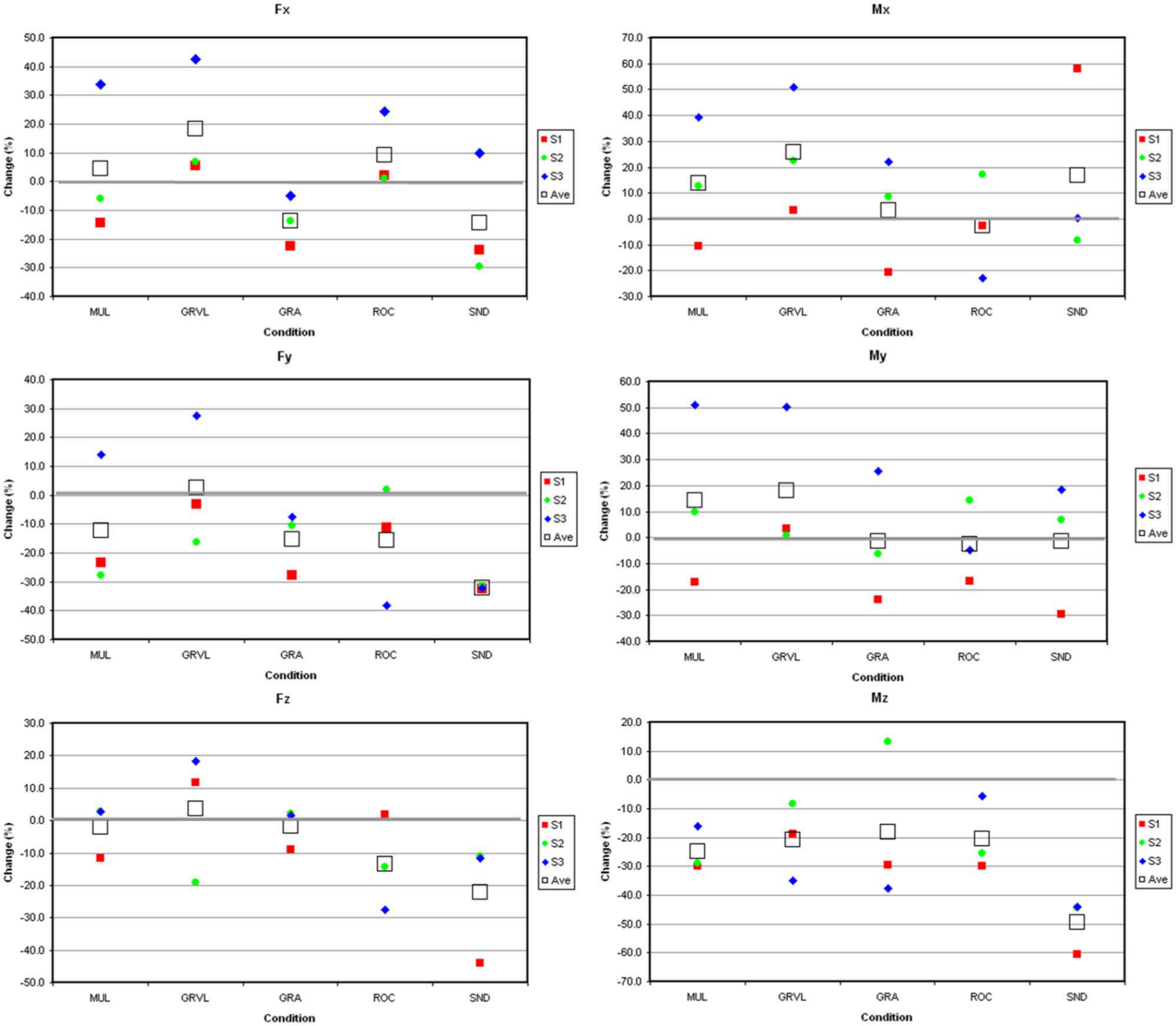
Percentage change in peak forces and moments compared to the level ground (GRD) condition for fast walking speed for individual subjects labeled S1–S3. Each data point is the average of five consecutive steps.
Individual peak forces and moments normalized to subject mass for all ground conditions.
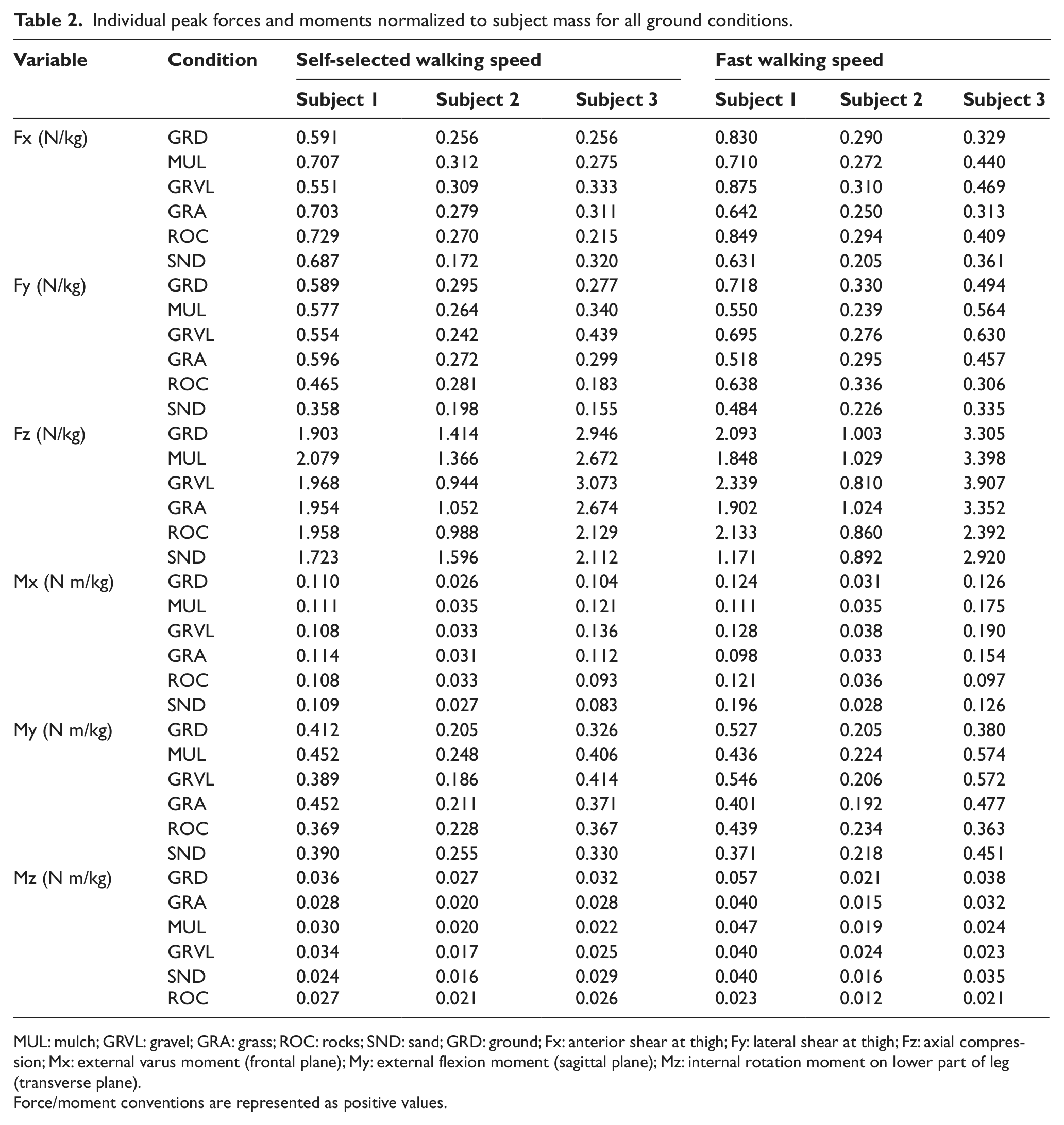
MUL: mulch; GRVL: gravel; GRA: grass; ROC: rocks; SND: sand; GRD: ground; Fx: anterior shear at thigh; Fy: lateral shear at thigh; Fz: axial compression; Mx: external varus moment (frontal plane); My: external flexion moment (sagittal plane); Mz: internal rotation moment on lower part of leg (transverse plane).
Force/moment conventions are represented as positive values.
The temporal data in Tables 3 and 4 show changes in both velocity and cadence when walking on irregular surfaces when compared to GRD, although on average these differences were no more than 5.0% (Table 4). Comparing the SSW and FW conditions (Table 5), participants had on average 31.3% higher walking speeds for MUL, GRVL, and GRA and 12.0% higher cadence across all conditions for FW compared to SSW (p < 0.000). All forces and moments increased with walking speed (FW vs SSW), with Fy, Mx, and My by 21.5%, 19.3, and 16.3%, respectively (p < 0.05).
Velocity and cadence.
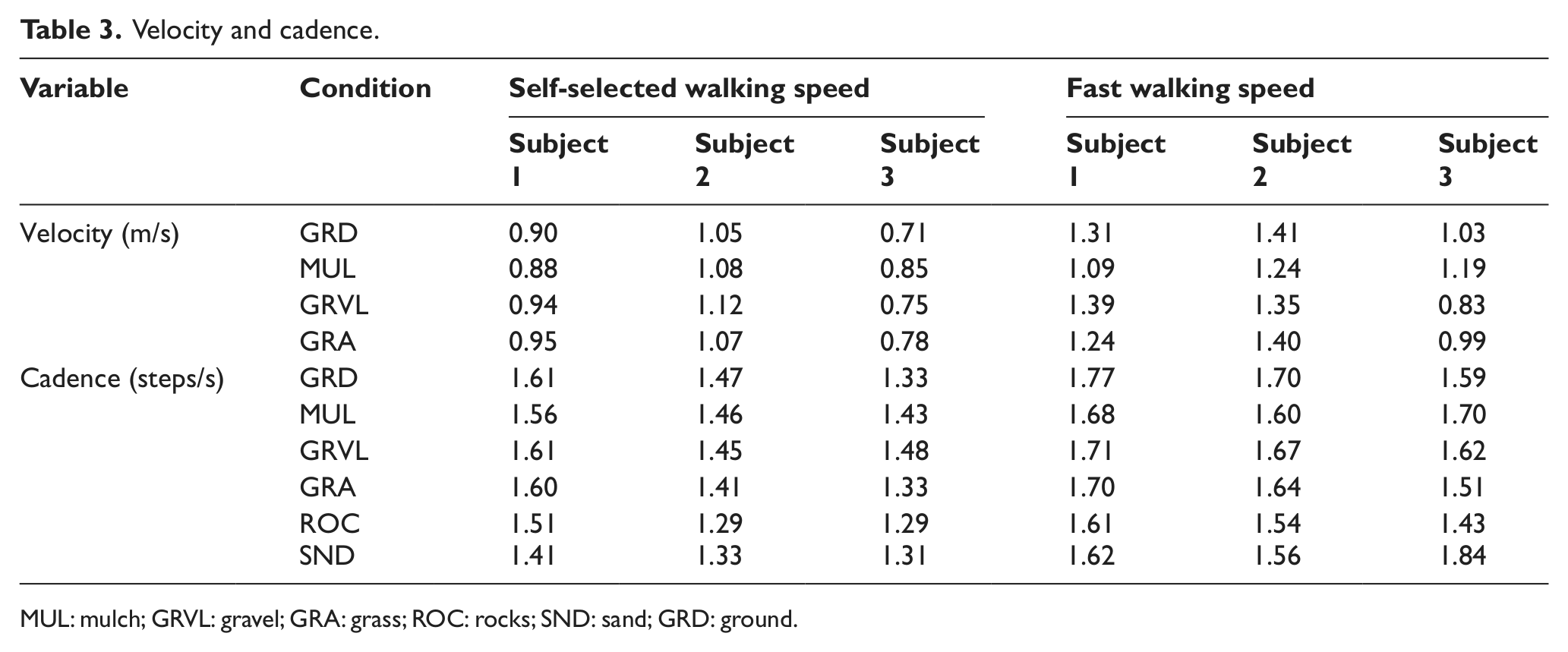
MUL: mulch; GRVL: gravel; GRA: grass; ROC: rocks; SND: sand; GRD: ground.
Comparisons of peak forces and moments normalized to subjects’ mass and spatiotemporal variables.
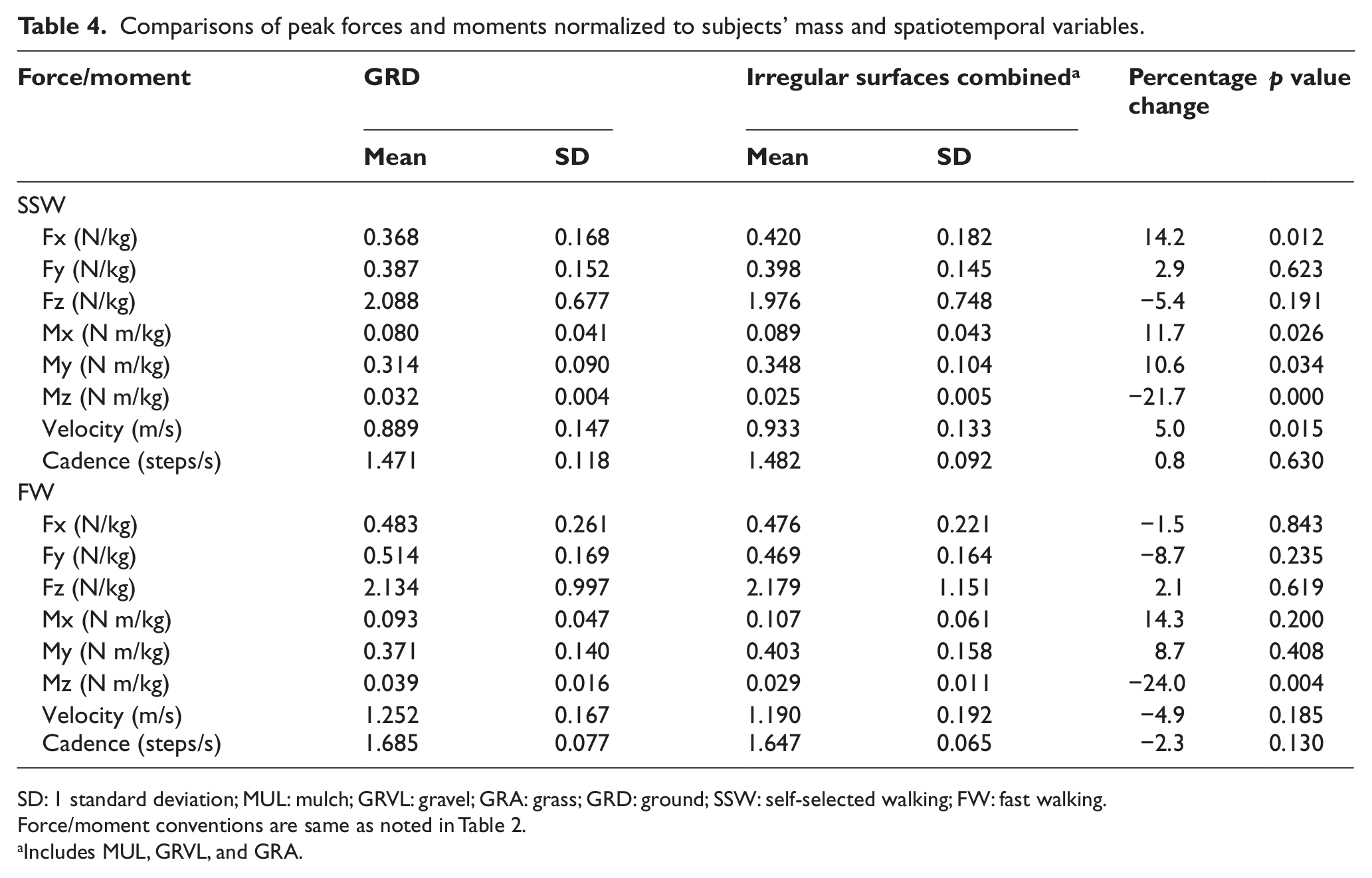
SD: 1 standard deviation; MUL: mulch; GRVL: gravel; GRA: grass; GRD: ground; SSW: self-selected walking; FW: fast walking.
Force/moment conventions are same as noted in Table 2.
Includes MUL, GRVL, and GRA.
Comparisons of variables at SSW and FW speeds for all ground surfaces.
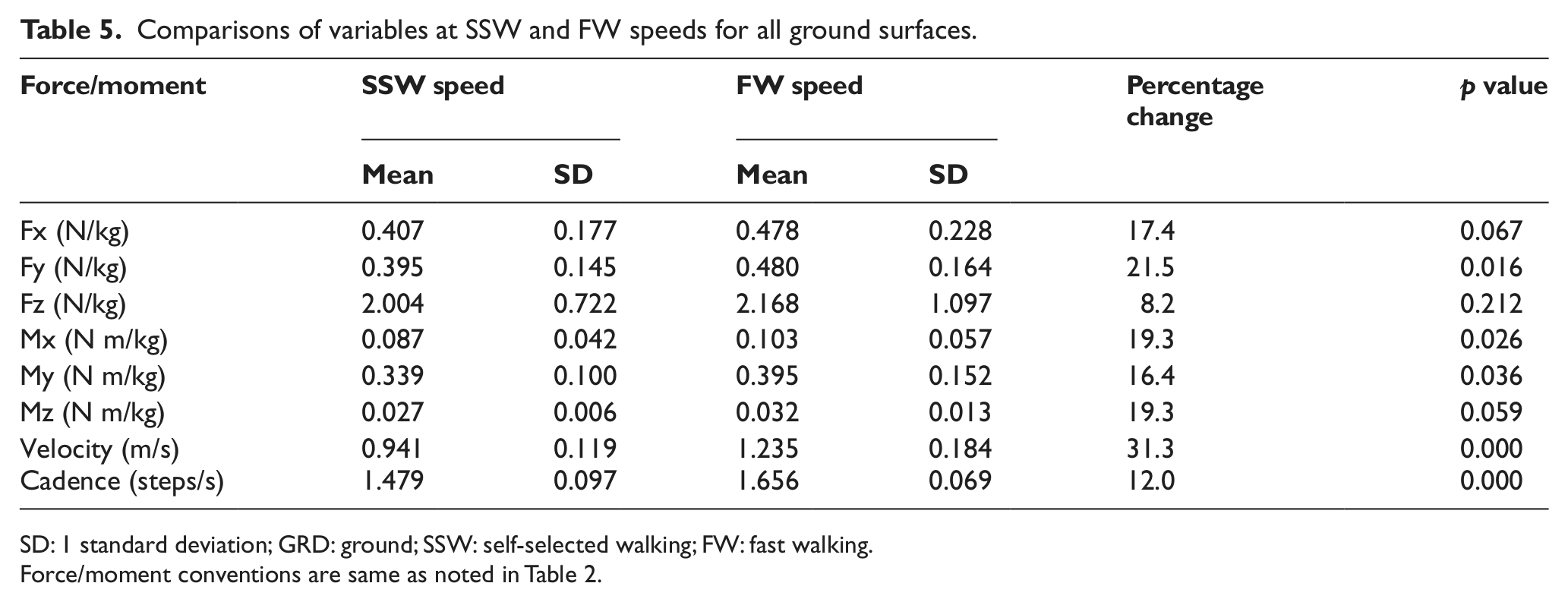
SD: 1 standard deviation; GRD: ground; SSW: self-selected walking; FW: fast walking.
Force/moment conventions are same as noted in Table 2.
Discussion
Understanding the loads imposed on orthoses is important for the design of more effective devices and the provision of improved orthotic interventions to patients.21,28 In this study, forces and moments at the lateral KAFO knee joint of three polio and post-polio patients were investigated while walking on different ground surfaces and at two walking speeds. Previous studies examining KAFO loads have been restricted to in-lab testing conditions; therefore, these findings provide new insights into important aspects of real-life mobility.
The findings suggest that irregular surfaces do alter the forces and moments that are imposed on KAFOs during gait. Supporting our expectation, higher internal peak knee flexion moments were measured during walking on irregular ground surfaces when compared to even ground. This finding is consistent with studies utilizing paradigms intended to simulate real-life mobility conditions. In one obstacle-crossing study, Chou and Draganich 7 found that the trailing limb loading response flexion moment in early stance was significantly increased by 32% on average while negotiating a 51-mm obstacle, when compared to unobstructed gait. On average, an increase in moment of 10% was found here for SSW speeds over irregular surfaces, compared to level ground. The irregularity of the surfaces that were examined, with changes in elevation acting as obstructions that needed to be cleared by the foot, likely elicited certain gait alterations to increase vertical displacement of the center of mass (COM), similar to obstacle-crossing situations. Hence, one potential cause of the increase in support knee moments is increased vertical excursions of the COM causing greater downward velocities and deceleration and hence higher loads.12,14 In KAFO gait, such vertical movement may be further exaggerated over irregular terrains because of the fact that the KAFO knee joint is typically locked in extension during the swing phase, and to achieve adequate foot clearance of the braced limb, users are required to adopt gait deviations such as vaulting whereby the ankle on the contralateral limb is additionally plantarflexed in mid stance to raise the pelvis.
Only one other study was found that measured lower limb moments over an irregular surface. Wade et al. 10 used a simulated in-lab setup to examine the effects of walking on railroad ballast. Contrary to our findings, and their own prediction, they found that the external peak flexion moments in stance phase were decreased on the ballast covered surfaces. One explanation for these differences is the significantly slower walking speeds that the able-bodied participants adopted on the ballast surfaces (being indicative of a more cautious gait) and the strong positive correlation between walking speed and magnitudes of knee moments. 5 The same effect was seen in this study; for the FW speed condition, there was on average a 31% faster velocity, 12% higher cadence, and a corresponding 16% increase in peak knee flexion moment. In this study, velocity and cadence did not generally decrease for MUL, GRVL, and GRA, but for the more challenging surfaces (ROC and SND), a slight reduction in cadence was found (Table 3). A reduction in cadence was similarly found by Paysant et al. 25 involving able-bodied participants walking on cut GRA. Menz et al. 14 also reported lower cadences on irregular surfaces for able-bodied gait. Decreasing one’s walking speed and cadence may be an effective strategy by which individuals with lower limb impairments not only limit their physiological and energy demands 13 but also decrease the demands for lower limb support moments while negotiating real-life environments.
The implications of these increased demands on lower limb support are likely at least in part responsible for the mobility limitations faced by individuals with lower limb weakness in certain real-life environments. 19 For those with compromised muscle strength in the lower limbs, the additional demands on lower limb support can make certain mobility-related outdoor activities or tasks unsafe or impossible. In cases where patients are reliant on assistive devices for additional stability, these devices will be subjected to higher mechanical loads potentially resulting in premature deterioration or failure of the device in cases where users regularly negotiate outdoor terrains. As shown in Figures 2 and 3, under certain conditions, these increases in loads can be quite substantial (≈50%). This has important clinical and technical implications on the design, prescription, and use of such mobility assistive devices since many of these devices are already designed to work at their structural limits in order to limit their weight and bulkiness and therefore increase user acceptance and satisfaction. 22
Higher knee flexion moments were accompanied by other loading changes in the KAFOs, including higher frontal-plane moments and shear force in the sagittal plane. However, in contrast to our expectations, not all the parts of the KAFO around the knee joint resulted in higher loads when walking on irregular surfaces, and in fact, torsional moments in the lateral KAFO upright were found to significantly decrease at both walking speeds. One potential explanation for this discrepancy is that while the peak knee flexion moment (My) is a direct result of externally imposed sagittal-plane loads, the other forces and moments are a product of more internalized forces that result from the indeterminate mechanical interaction of the KAFO/limb system. For example, the axial loading of the KAFO upright (Fz) is largely dependent on how much force is transferred from the limb to the KAFO, which is influenced by the setup and fit of the KAFO. 20 The forces are also influenced by the amount of load that is transferred through the medial upright; something that was not feasible to measure with this type of load cell setup as it would have interfered with the subjects’ gait. While the resulting partial data restrict a comprehensive model of the loads imposed on KAFOs, it does suggest more generally that when walking on different surfaces, the loads in the individual parts of a KAFO/limb system (i.e. limb, medial upright, lateral upright) may become redistributed, increasing in certain places and decreasing elsewhere.
A number of limitations are noted in this study. As with other published studies, 21 the small sample size and single-subject statistical analysis limit generalizability of results. Second, walking speed is an important factor affecting support moments, but it was not captured here for several of the surface conditions. Moreover, as seen in this study and more generally in non pathological human gait, 5 faster walking speeds typically result in higher support moments. Although not statistically significant, in this study, participants adopted slightly slower walking speeds on irregular surfaces, which likely reduced the moments measured and therefore the overall effect. Third, as testing conditions were not randomized, there may be some influence of the testing order of walking speeds as polio patients can be susceptible to fatigue. Additionally, consideration needs to be given to measuring additional gait variables such as joint kinematics (via goniometers) and motions of the COM (via accelerometers and/or goniometers) to make it possible to examine additional factors associated with the increase in support moments. Future work should also aim to apply a load cell to the medial knee joint of the KAFO, such that a more comprehensive model of forces and moments can ultimately be developed. Finally, a better understanding of the loads that KAFOs can withstand is needed, to establish whether these changes/increases in loads are clinically significant.
Conclusions
Our understanding of lower limb loading under real-life conditions is limited by the availability of viable measurement techniques. In this study, instrumenting the lateral KAFO knee joint of individuals with poliomyelitis provided a means for measuring lower limb knee kinetics while walking on real-life irregular surfaces. In general, irregular surfaces and faster walking speeds resulted in higher peak knee flexion moments during stance, making these conditions potentially more demanding on individuals with lower limb impairments and their assistive devices.
Footnotes
Conflict of interest
None declared.
Funding
The research was funded by the Canadian Institutes of Health Research and the Health Technology Exchange (grant no. 18 84171).