
Abstract
Background and aim:
Mid-facial defect is one of the most disfiguring and impairing defects. A design of prosthesis that is aesthetic and stable can be precious to a patient who has lost part of his face due to surgical excision. Prosthesis can restore the patients’ self-esteem and confidence, which affects the patients and their life style. The aim of this case report is to describe a technique of mid-facial silicone prosthesis fabrication.
Technique:
To provide an aesthetic and stable facial prosthesis, the extra-oral prosthesis was fabricated using silicone material, while the intra-oral defect was restored with obturator prosthesis, and then both prostheses were connected and attached to each other using magnets.
Discussion:
This clinical report describes the rehabilitation of a large mid-facial defect with a two-piece prosthesis. The silicone facial prosthesis was made hollow and lighter by using an acrylic framework. Two acrylic channels were included within the facial prosthesis to provide the patient with clean and patent airways.
Clinical relevance
A sectional mid-facial prosthesis was made and retained in place by using magnets, which resulted in a significant improvement in the aesthetical and functional outcome without the need for plastic surgery. Silicone prostheses are reliable alternatives to surgery and should be considered in selected cases.
Surgical resection is a standard practice in cancer management process and it is well documented specially for maxillofacial cancer treatment. This surgical resection can include palatal, nasal and orbital contents, what sometimes may leave the patient with a mid-facial defect. 1
In general, mid-facial defects have an intra-oral communication. Marunick et al. 2 classified mid-facial defects into two main categories: midline defect that includes the nose and may also include the upper lip; lateral defects, which include the orbital and cheek parts. Combinations of these categories as well can be found. Acquired mid-facial defects ordinarily will be associated with a facial disfigurement and a functional impairment. These defects can be managed by surgical reconstruction or a facial prosthesis. Reconstruction of large defects remains a challenge, in spite of recent advances in surgical reconstruction methods. The necessity to restore the complex three-dimensional anatomy of the lost structures with a suitable cover, lining and support often requires multi-stage procedure and the healthy local tissue availability. However, even with all of that, the aesthetic result may leave much to be desired. The risk of recurrence and the use of radiotherapy often add further challenges to the reconstruction. 3 The surgical reconstruction has the disadvantages that the flap might fail, and the result could be poor. Furthermore, the tumour recurrence may necessitate removal of the flap. Most of the tumour recurrences will be within 36 months following initial treatment. Therefore, prosthetic rehabilitation should be the treatment of choice. Should further excision be required, replacement of the prosthesis is a relatively undemanding procedure. 4 In addition, facial prostheses can provide an appropriate alternative solution for the large mid-facial defects to restore function and aesthetics.5,6
Selection of the attachment system for this type of prostheses varies among cases. Each anatomical site has its own distinct retention requirements dictated by a variety of factors. However, the choice of attachment is not only determined by the anatomical site. The clinician must have the potential to identify the appropriate choice of attachments because every single maxillofacial defect is unique in itself and requires a different retaining design.
There are several means of retention used in the maxillofacial prostheses. Among the choices were adhesive, eyeglasses retained, magnets, implants and combinations of the previous means. The adhesive usage requires patient to apply the adhesive to the prosthesis’ periphery at each time of usage. Some patients were uncomfortable with the mucin-like appearance, and some even developed an allergic reaction to the adhesive. Those patients who do not wear eyeglasses may not prefer the option of having to wear one. As for the magnet attachment, the impact of losing its attractive force may be an issue. Although the implant is the newest option attainable, the availability of bone in the defect region needs to be considered, and the patient may also refuse any further surgery. 6 Chung et al. 7 reported that in implant supported overdenture cases, the magnetic attachment resulted in the weakest retention characteristic compared to ball, Locator and bar attachments. On the contrary, the magnet attachment permits multiple prosthesis insertion/removal paths, making it more advantageous in cases like the mid-facial defects, and the patient will be capable of putting on the prosthesis without many difficulties.
The magnet attachment is one of the most efficient means of providing facial prostheses with stability and retention quality. Usually, magnet-retained prostheses are in sections and have a magnet in each section; this application in sections is useful for a proper path of insertion/removal achievement.5,8 Several authors have reported different techniques to attach the magnets to the prostheses sections. Lemon et al. 8 described the technique for attaching the magnets to the facial prostheses by chair-side pickup using an auto-polymerizing acrylic resin. Brignoni and Dominici 5 and Patil 9 used pickup impression technique to attach the magnets to the prostheses indirectly.
This clinical report describes the rehabilitation of a challenging large mid-facial defect with a two-piece prosthesis that included an intra-oral obturator and an extra-oral facial prosthesis with the use of magnets. Two acrylic airway channels were incorporated within the facial prosthesis to make the prosthesis hollow and lighter. This design could provide the patient with clean and patent airways.
Case report
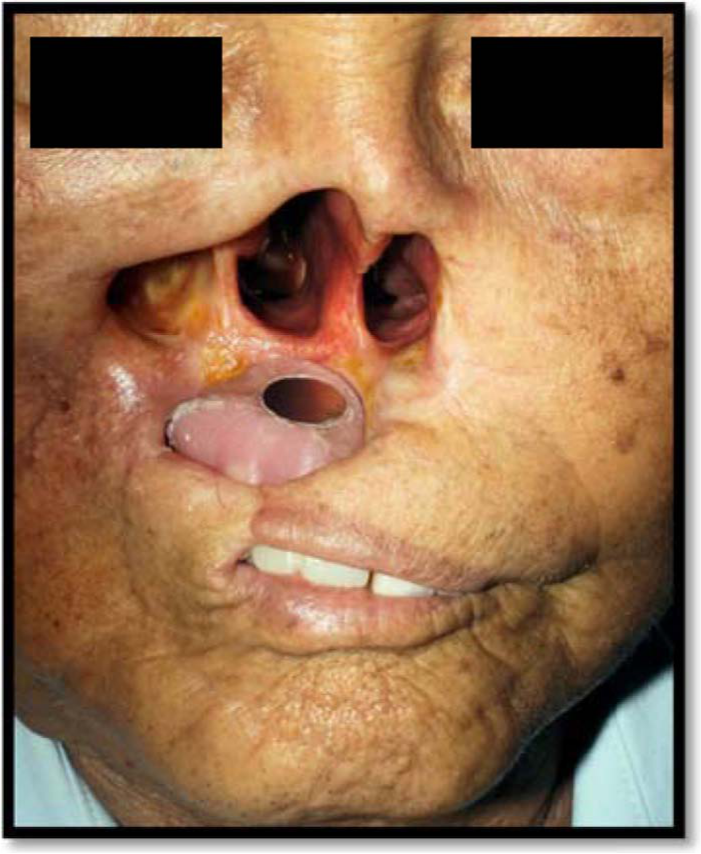
A 72-year-old man was referred to the prosthetic department for rehabilitation of his mid-facial defect. He underwent total rhinectomy with local flap reconstruction in August 2009. He was diagnosed with recurrent basoloid squamous cell carcinoma at the nasomaxillary region. The patient also underwent radiation therapy. On examination, the defect area involved complete nasal resection with right subtotal maxillectomy resulting in an orocutaneous fistula. The upper lip was stretched on the right side with a vertical scar causing a restriction in the mouth opening (maximum mouth opening was around 17 mm). The extent of the mid-facial defect, which included the maxilla, cheek and nose, presented considerable aesthetic and retention challenges when considering restoring with a mid-facial prosthesis (Figure 1). New definitive obturator and magnet-retained mid-facial (nasal and cheek) prostheses were fabricated to restore his self-esteem and confidence.

The frontal view of the mid-facial defect.
The intra-oral prosthesis construction
Prosthetic management began with a new obturator fabrication, to restore Armani class VI intra-oral defect. 10 Since the patient’s current prosthesis was broken, it was decided to fabricate new obturator prosthesis and utilize it for the extra-oral prosthesis retention purpose. However, the limited mouth opening affected the obturator prosthesis’ design and fabrication.
At the impression-taking stage, a stock tray was modified by cutting it into two halves (sectioned tray) to overcome the limited mouth opening problem. This was performed in order to take the primary impression of the maxillary arch in two separated halves (right and left).
Two (right and left) custom trays were constructed on the poured primary stone casts and used to take the secondary maxillary impression; the impressions of the right and left sides of the maxillary arch were taken separately without being assembled together intra-orally. However, the poured halves of the maxillary master cast were assembled extra-orally using the current cobalt–chromium removable partial denture (RPD) as a key; it was possible to use this new technique for this case as there was no beading line in the previous design. (Figure 2).
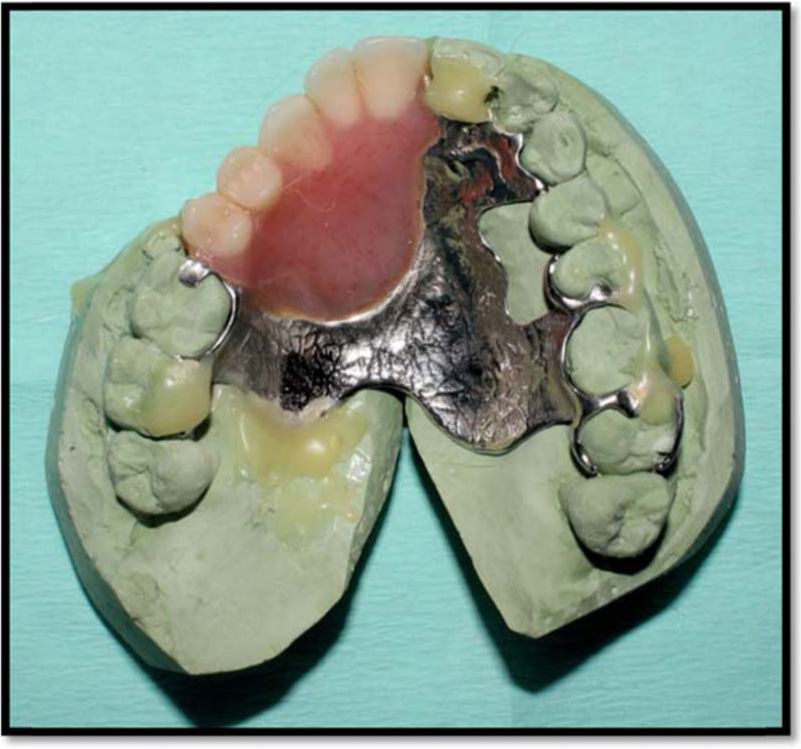
The current prosthesis was used as a key to assemble the right and left halves of the poured maxillary master cast together.
To confirm the accuracy of the maxillary master cast, an acrylic trial plate was fabricated and tried inside the patient’s mouth before constructing the new Co-Cr framework.
The extension of the Co-Cr framework design further than the first molars on the posterior side was restricted. This is because the metal framework when extended more would result in the prosthesis becoming larger and the patient would not be able to insert it inside his mouth. Then, the obturator prosthesis was fabricated in the conventional way.
The mid-facial prosthesis construction
Two magnets (one coated rare-earth magnet, one electronic magnet, Kuala Lumpur, Malaysia) with attractive force of 13.5 N were used to retain the mid-facial prosthesis’ sections attached together.
The roof part of the constructed obturator prosthesis was prepared to receive the first magnet. The magnet was secured to the obturator roof using chair-side hard relining material (KOOLINER™ Hard Denture Reline Material, GC, USA) (Figures 3 and 4).
The first magnet attached to the obturator prosthesis roof.
The obturator prosthesis in place.
Afterwards, the wax pattern for the future acrylic base framework of the facial prosthesis was made chair-side and tried on the patient’s face. Future second magnet’s room was also relieved into the wax pattern just above the previously secured magnet in the obturator prosthesis’ roof. Then this wax pattern was transformed into the acrylic base framework.
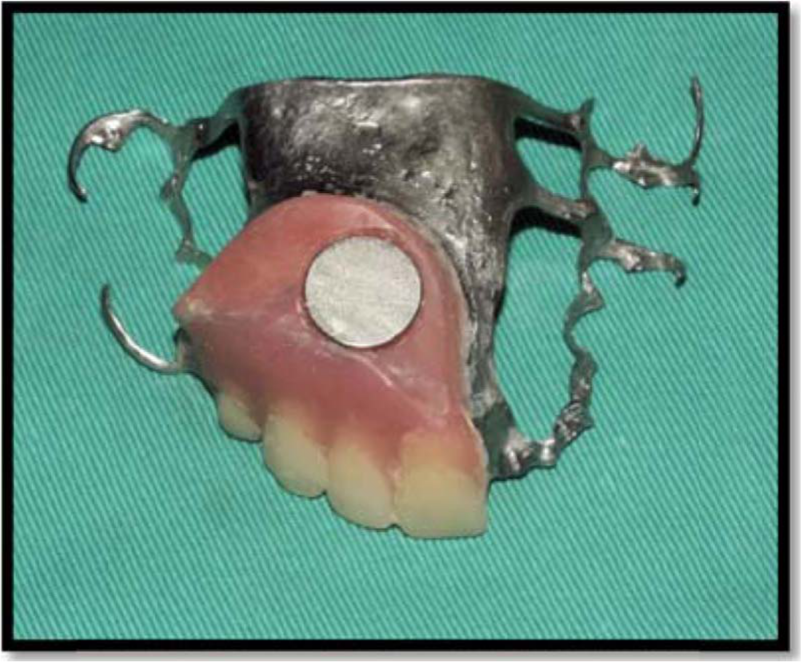
The fitting of the processed acrylic base framework was checked on the patient’s face, and the second magnet was secured into the relieved room of the acrylic framework using chair-side hard relining material (KOOLINER) (Figure 5).

The second magnet was secured in the acrylic base framework and tried on (arrow).
Using Bredent wax (Epithetic Bredent), the mid-facial pattern was sculptured on patient’s face cast, and then it was adjusted and finished chair-side. Adaptation of the pattern on the patient’s face was checked particularly at the margins. The facial wax pattern was evaluated on the patient’s face from frontal, lateral and axial views. (Figure 6)

The wax sculpture tried on patient.
The facial wax pattern was invested and dewaxed using a large flask. Subsequently, the city-colour silicone material (Multisil Epithetic, Bredent, Germany) was chosen as the body colour of the prosthesis. The silicone material was packed and polymerized at 60°C for 45 min using polymerization bath according to the manufacturer’s instructions.
A lower weight of facial prosthesis with an easily cleaned patent airway was obtained by adding two acrylic channels into the previous acrylic framework (Figure 7). However, this was performed after the acrylic framework had been picked up from the patient’s face and poured using plaster of Paris to maintain and secure the exact position of the framework to the mid-facial pattern.

Two acrylic channels added to the framework (arrows).
Attaching the silicone prosthesis to the acrylic framework
To allow bonding of the acrylic framework to the silicone material, the acrylic framework was initially painted with the primer (Multisil Primer, Bredent, Germany). Then, the finished silicone portion of the prosthesis was relined with city-colour silicone material (Multisil Epithetic, Bredent, Germany) fixed onto the acrylic base framework and left to cure overnight.
The finished mid-facial prosthesis was tried on the patient’s face for retention, adaptation, sealing and airway patency. Subsequently, the extrinsic coloration was added to finalize the colour of the prosthesis and to match the patient’s skin colour (Figures 8 and 9). The prosthesis was painted in two layers. Between the layers, it was treated with the sealing agent for epithetics. This was performed to increase the life expectancy of the prosthesis.

The final prosthesis is in place (frontal view).

The final prosthesis is in place (lateral view).
At the delivery time, the patient was asked to perform several movements like coughing and opening the mouth wide to assess the stability of the prosthesis and its margin fit to the patient’s face (Figure 10). The masticatory function was also checked by asking the patient to chew wet cotton pellets. Both the extra-oral and the intra-oral prostheses were stable, retentive and functioning properly.

The prosthesis is in place with maximum mouth opening.
Discussion
To fabricate comfortable and functional obturator prosthesis, accurate impressions of the defect area, teeth and anatomical landmarks are required. Prosthetic rehabilitation of limited mouth opening patients presents difficulties at all stages.
In this case report, the patient has a limited mouth opening (17 mm), as a result of which it was impossible to make impressions and fabricate prostheses using conventional techniques. In such cases, the sectional impression technique effectively overcame the difficulties in introducing the impression tray into the patient’s mouth and making precise impression with slight patient discomfort. 11 Several methods have been advocated to precisely relate the sectional trays intra-orally, such as the following: (1) preparing sectional tray with a stepped butt-joint, (2) preparing sectional tray with nick and notches at the handle region, (3) preparing foldable sectional tray with steel burs and acrylic blocks, (4) anterior and posterior tray sections joined by steel burs, (5) tray sectioned into three pieces to be approximated at the handle with fins, and (6) sectional tray joined by acrylic hook or lock.11–14 In this case report, new technique was advocated to assemble the poured sectional tray impressions extra-orally, which was achievable using the current cobalt–chromium RPD as a key. This technique made it possible to avoid relating the sectional tray intra-orally, thereby making the clinical visit shorter and less stressful for the patient.
Coated rare-earth magnets with an attractive force of 13.5 N were used in this case. The magnets were attached to the obturator and the extra-oral prostheses. These magnetic attachments prevent dislodgement of the obturator during breathing, masticating and coughing. However, due to rigid connection between the two sections, slight vertical movement of the facial prosthesis during mastication can still be noticed.
At 1-year review visit, the prosthesis was still retentive and in use (Figure 11). However, there was slight colour change, which was expected and can be adjusted by repainting if the patient requests. On the contrary, the intimacy between the silicone prosthesis’ edges and the skin was still acceptable. The ability of the patient to speak, swallow and to chew was also reviewed, and the patient’s comfort was confirmed.

The mid-facial prosthesis in place after 1 year in service.
Generally, the patient was satisfied and accepted the prostheses well. He was also happy that there was no more need for the face mask to cover the defect and that he got back his self-confidence.
Conclusion
The surgical reconstruction of a large mid-facial defect is a challenging procedure. Such defects can be treated satisfactorily by giving a magnet-retained extra-oral facial and intra-oral obturator prostheses. However, designing facial prostheses for such patients with complicated conditions is a significant challenge too. Unilateral mid-facial defects including the nose and the right cheek forming part of moving structures are expected to be unstable unless highly retentive elements are used.
The prosthesis in this case was designed to be removable to allow easy maintenance and cleaning of the defect area. It was also designed to be low in weight with an easily cleaned patent airway, which was achievable by adding two acrylic channels to the acrylic base framework of the extra-oral prosthesis. However, the fabrication technique should be cautiously considered according to each patient’s condition.
Footnotes
Acknowledgements
I would like to acknowledge the invaluable assistance of Professor Dr. Norsiah Binti Yunus and Associate Professor. Dr. Laith Mahmoud Abdulhadi as they were my direct supervisors for maxillofacial prosthetic cases.
Conflict of interest
The author declares that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.