
Abstract
Background and aim:
Facial defects (from neoplasms, trauma, etc.) can be functionally and emotionally devastating. A non-invasive treatment for these defects is the application of external prostheses. Conventionally, these prostheses are fabricated by an anaplastologist through a manual procedure, which is an expensive and time-consuming approach. Current advances in computational and engineering tools report an improvement in design and manufacturing of silicone prostheses. This demand motivated this study that aims to develop a methodology for fabricating customized nasal prostheses.
Technique:
In this study, an 80-year-old woman with a total defect of the nose is considered as case-study. The proposed methodology entails six tasks: (a) data acquisition, (b) three-dimensional reconstruction, (c) prosthesis design, (d) moulds fabrication, (e) prosthesis manufacturing and (f) final fittings.
Discussion:
The presented approach showed encouraging outcomes since it saves time, reduces costs and allows the achievement of prosthesis with the minimum contact and discomfort to the patient, disclosing excellent aesthetic and functional results.
Clinical relevance
Custom-made nasal prostheses with minimum contact and discomfort for the patient can be achieved using an engineering approach based on digital technologies and additive manufacturing that is cost-effective and less time-consuming than the manual procedure.
Background and aim
Facial defects resulting from neoplasms, burns, congenital malformations, trauma or other diseases, particularly when involving partial or total loss of an external organ, can be functionally and emotionally devastating. Although tissue reconstruction is currently provided by modern surgery with grafts or flaps, it might not always be applicable due to several constrains related to advanced age, medical conditions or excessive treatment costs involved. In such cases, defects can be restored with external prosthesis. The detail level achieved on such prosthesis is determinant for the re-establishment of patient confidence.1–7
There are two main approaches to fabricate these external prosthetics: the conventional method and the digital method. 4 Fabrication of conventional prosthesis is based on the uptake of the failing part shape directly from the patient’s body. Plaster and ordinary hand tools are used by an anaplastologist to obtain a prosthesis whose shape fits the patient satisfactorily.5,6,8 This is a time-consuming and unpredictable process, because it is highly dependent on the skill level of the technician. Moreover, this method is particularly stressing for the patient as he or she should be kept immobilized in order to minimize distortion.8,9 In order to overcome such limitations, the digital method was introduced, which relies on advanced methods of reverse engineering.
The digital method has fewer process steps than the conventional method but requires access to several technologies. In a broad sense, the digital method entails three main steps, namely, data acquisition, computer-aided design (CAD) and additive manufacturing (AM)-based technologies. In the last two decades, several authors have attempted to apply the digital method in the design and manufacturing of facial prostheses. However, the increase in the number of patients and the cost constraints request a further investigation of this approach in order to increase the efficiency, reduce the delivery times and costs and improve the quality of the final product.5–12 This demand motivates the present study. Therefore, a full engineering-based approach for producing custom-made nasal prosthesis is outlined.
The main contribution of this study is the completeness of the description of the proposed methodology. Indeed, the fabrication of custom-made nasal prosthesis entails several key points, which are widely discussed, such as the retention system, the aesthetic features, the patient comfort and the costs and time demands. Furthermore, the proposed approach is wide-ranging, which means that with a few adjustments, it can be applied to fabricate silicone prostheses of other soft-tissues structures (e.g. ears).
Technique
An 80-year-old woman with a total defect of the nose is considered as case-study. The patient had been submitted to a total rhinectomy for treatment of an advanced squamous cell carcinoma involving the full thickness of the nose. Also, she was admitted to adjuvant radiotherapy and is free of disease at 3 years follow-up. The medical team does not recommend surgical reconstruction due to patient’s advanced age and technical complexity (at least 3 surgeries with bone transfer from the skull or rib).
The nasal defect was evaluated to identify possible restorative limitations regarding retention and aesthetics. Several alternatives of prosthetic rehabilitation were discussed with the patient. The fabrication of a silicone nasal prosthesis was planned, and the expectations of this treatment were explained to the patient. 9
Regarding the retention system, a non-invasive solution was recommended by the medical team. With the patient being an eyeglasses user, a substructure combining her eyeglasses and the nasal prosthesis was projected. This system takes advantage from the nose cavity for prosthesis retention and the eyeglasses for support and placement.
An engineering-based approach for design and fabrication of a customized nasal prosthesis is presented throughout this study. Figure 1 depicts some steps of the proposed methodology, which includes the following six main tasks:
Data acquisition;
3D reconstruction;
Prosthesis design;
Moulds fabrication;
Prosthesis manufacturing;
Final fittings.
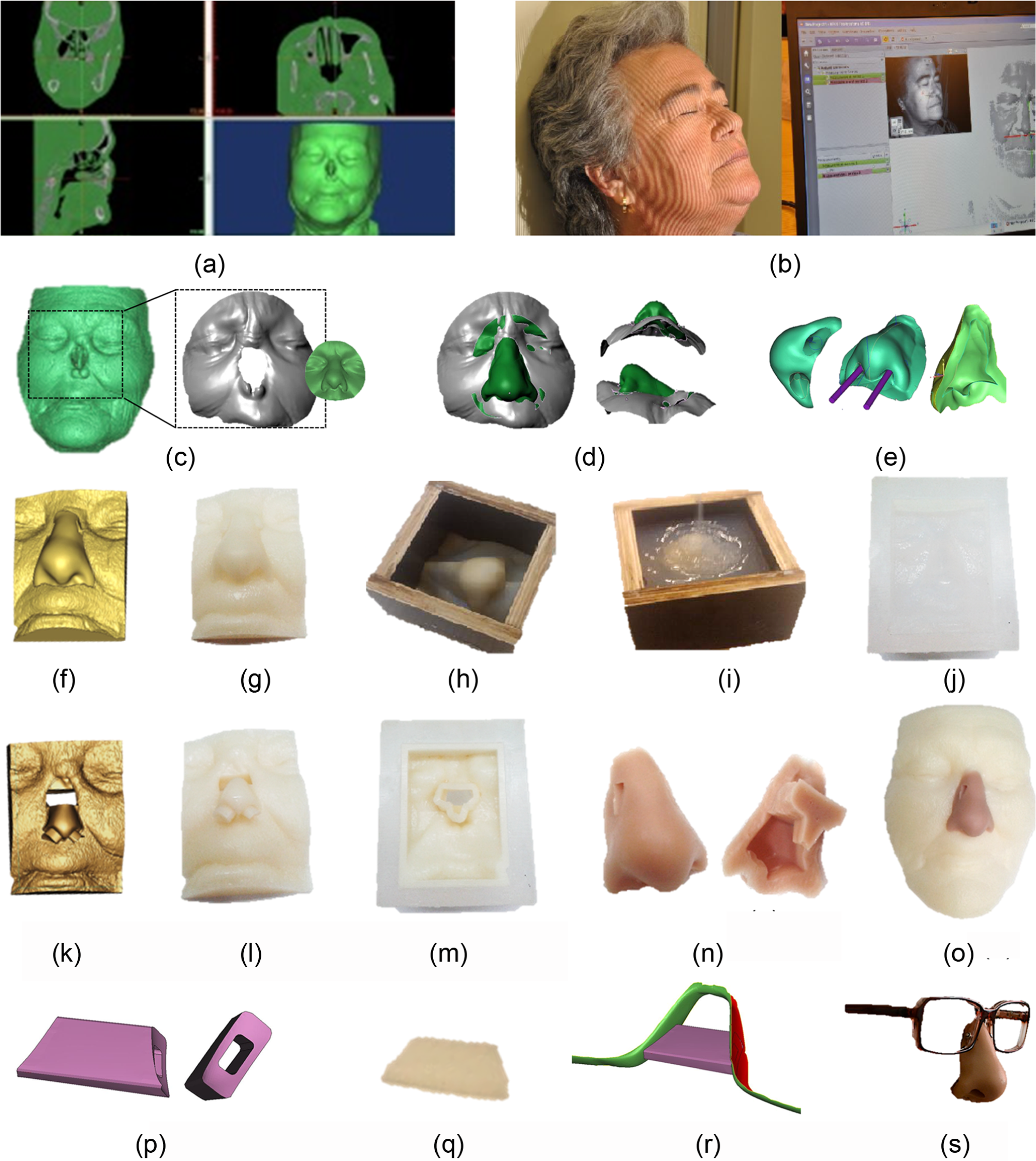
Nasal prosthesis’s design and manufacturing steps: (a) 3D reconstruction of patient’s face by CT images, (b) direct face scanning to create a digital nose database, (c) selection and alignment of virtual nose model, (d) surface fitting and trimming of the virtual prosthesis model, (e) smoothing and cutting operations to create functional nostrils on the prosthesis, (f) virtual model of outer mould, (g) plastic model of outer mould, (h) wood box, (i) silicone casting inside the wood box, (j) silicone mould, (k) virtual model of inner mould, (l) plastic model of inner mould, (m) plastic model of inner mould inside the silicone mould, (n) silicone nose prosthesis, (o) silicone nose prosthesis on the prototyped plastic model of the patient’s face, (p) CAD model of the substructure, (q) plastic model of the substructure, (r) CAD assembly of the substructure with the eyeglasses and (s) silicone nose prosthesis with the eyeglasses.
For sake of prosthesis’s endurance and hygiene, it is recommended to the patient to have a second prosthesis, which can be fabricated by repeating the last two tasks (steps 5 and 6).
It is noteworthy that, to perform this study, ethical approval was granted from the local ethics committee of the author’s institute, and informed consent was obtained from the patient.
Data acquisition and 3D reconstruction
Computed tomography (CT) scans (SOMATOM Sensation Cardiac 64, SIEMENS AG, Forchheim) were acquired for clinical purposes. Thus, the resultant set of DICOM images, which comprises a total of 176 slices with 1 mm of increment (i.e. axial thickness) and a pixel size of 0.283 mm, is utilized in this project. MIMICS 16.0 (Materialise, Leuven) is used for image segmentation and, therefore, for virtual reconstruction of patient’s face (Figure 1(a)). The output of this task is a STL file of a three-dimensional (3D) model of the patient’s face. It is important to mention that if imagiologic data are not available in the patient’s clinical records, an optical-based method should be used for data acquisition of patient’s face, because it is a less novice and less expensive technique.
For the reconstruction step, in cases of single and/or asymmetric organs such as the nose, the natural shape of a suitable donor must be used. There are several typologies of noses, such as the Roman, the Greek, the Cogitative and so on.11,12 Thus, a digital database of nose models was constructed. The nose models were acquired by direct face scanning of some individuals (Figure 1(b)) using a structured light scanner (ATOS III Triple Scan, GOM mbH, Braunschweig). This reverse engineering system has two high-resolution cameras (8,000,000 pixels), and it allows for exporting the 3D models in STL format. Prior to the direct face scanning, the individuals were made up to minimize the optical distortion features of the skin surface such as reflection, transparency and brightness. A prototype of patient’s face is built by SL-stereolithography (Viper™ SLA® System, 3D Systems® Corporation, Rock Hill, SC). Within this study, a distance of 0.05 mm between layers was adopted in each SL-stereolithography operation. All plastic models are submitted to a postprocessing treatment, which includes a three-step cleaning procedure, two steps of 2 h in water and one of 5 min in alcohol, and then a cure of the plastic model into a ultraviolet (UV) chamber. From time to time, the samples are sanded to remove layer steps and to smooth out contours.
Prosthesis design
From the digital database, a nose model was chosen, taking into account the patient’s defect (Figure 1(c)) and previous photographs. Afterwards, using in 3-matic 8.0 (Materialise), the modelling task is carried out. This software allows the manipulation of the digital nose model (move, rotate, align, etc.) until the best-fit between the patient’s face and the nose model is achieved. The design process entails several modelling operations: (a) alignment of the nose with patient’s face (Figure 1(c)), (b) adjustment of the nose to the patient’s face in terms of shape and adhesion to the skin surface (Figure 1(d)) and (c) surface fitting, trimming and smoothing (Figure 1(d) and (e)).
Moulds fabrication and prosthesis manufacturing
The design process of the moulds (outer and inner moulds) was performed in 3-matic software (Figure 1(f) and (k)). During the design process of the inner mould (core), two cylinders were placed inside the nose nostrils in order to produce a functional prosthesis (Figure 1(e)). Also, a small cut was carried out at the rhinion region aimed at providing a support for the prosthesis assembly inside the nose cavity (Figure 1(e)).
The moulds and prosthesis are manufactured using a standard procedure of silicone processing that entails the following steps:
SL-stereolithography of the outer and the inner moulds (Figure 1(g) and (l));
Constructing of the wood box (Figure 1(h));
Placing of the prototyped model of the outer mould in a central position and covering the casting surfaces with release agent (Figure 1(h));
Casting the silicone (silicone rubber VTX 950), curing and subsequent removal of the prototyped model (Figure 1(i) and (j)).
Prosthetic silicone vacuum casting and insertion of the prototyped model of the inner mould (Figure 1(m)). The prosthetic silicone (Dragon skin®, Smooth-On) colour is matched to the patient’s skin;
Curing and subsequent removal of the prototyped model of the inner mould (core) to obtain the silicone nasal prosthesis (Figure 1(n)).
Final fittings
Figure 2 illustrates the patient with the prosthesis, which has a substructure as retention system that links the prosthesis to patient’s eyeglasses (Figure 1(r) and (s)). This substructure was designed in 3-matic software (Figure 1(p)) and fabricated by SL-stereolithography (Figure 1(q)). To be ready for delivering, the prosthesis is submitted to an extrinsic colouring in order to get a more realistic appearance.
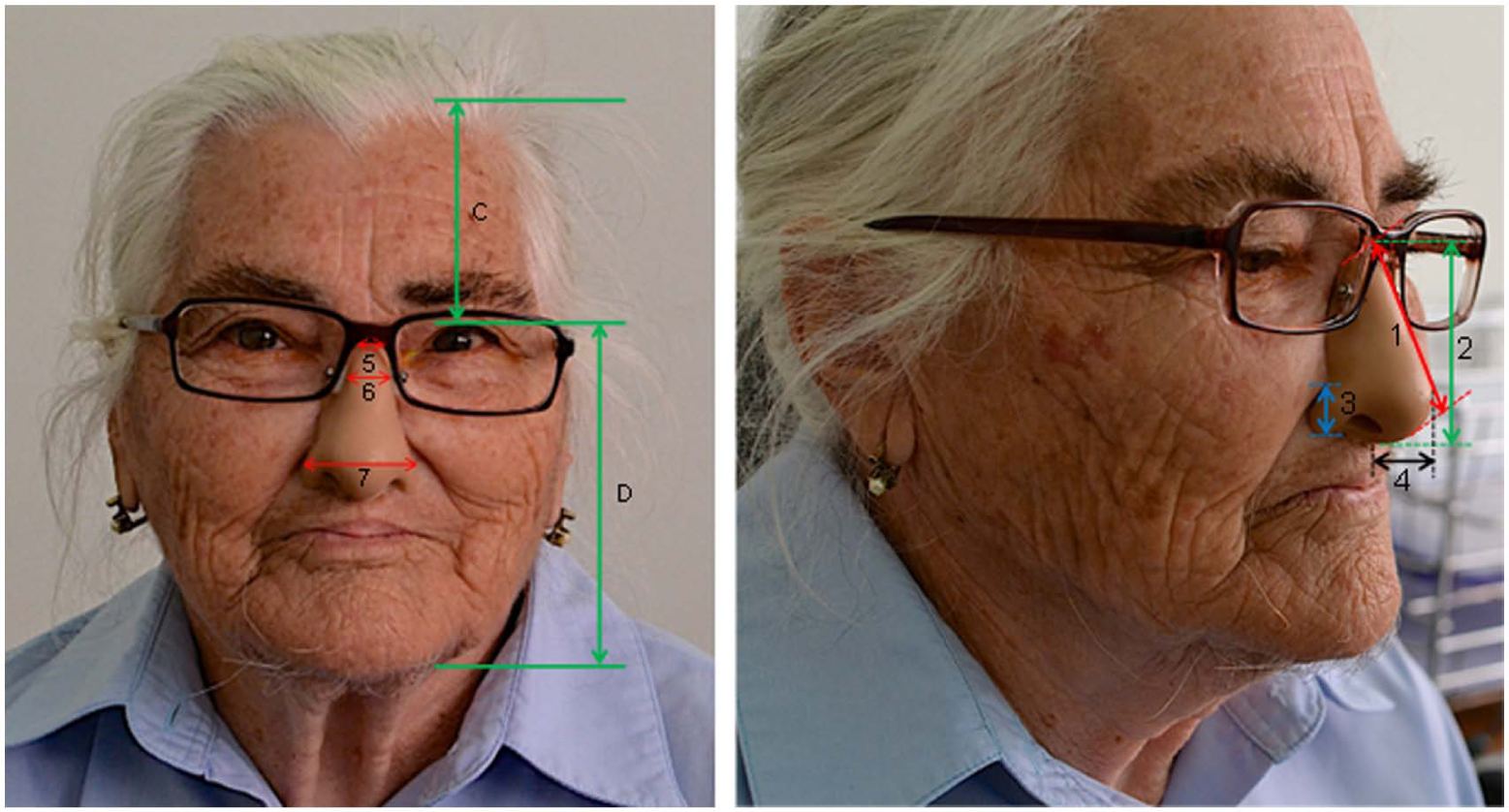
Patient with the prosthesis before extrinsic colouring (with patient’s permission).
Discussion
The proposed methodology was validated experimentally with the assembly of the prosthesis on the prototype of patient’s face (Figure 1(o)) and later in vivo by means of the prosthesis application on patient (Figure 2). For sake of discussion, three parameters were analysed, namely, the retention system, the aesthetics outcomes and the time demands and costs.
Retention system
The preliminary retention system test (on prototype of patient’s face) demonstrated sufficient retention strength, appropriate fitting (by the internal silicone support) and easy placement (and replacement). The material properties are also good for cleaning. Within this first evaluation, the retention system was considered to be ready for the in vivo test.
The results of retention system tested on the patient confirm the preliminary results. The anatomical shape of the retention system fits well on nose cavity that permits a correct placement of the prosthesis, leaving no open margins in the contact region. The eyeglasses, combined with the prototyped substructure, provide support and promote the vertical placement. As a consequence, the patient did not have to use skin adhesives to retain the prosthesis, which are uncomfortable and costly.
Aesthetic outcomes
The aesthetics outcomes include several characteristics such as fitting (shape and proportion), accuracy (position and alignment), colour and resolution (reproduction of folds, wrinkles and/or textures).
In terms of fitting, the marginal integrity of the prosthesis against the patient’s face surface reveals satisfactory results, that is, the prosthesis boundary matches with face’s prototype. To assess the degree of fit, the evaluation protocol proposed by Sun et al. 6 was adopted, which entails distance measurements and a nasal–facial proportion test (see Figure 2). The obtained results are listed in Table 1. The distance measurements and nasal–facial proportion test confirm the good fit of the nasal prosthesis.
Distance measurements and nasal–facial proportion measurement.
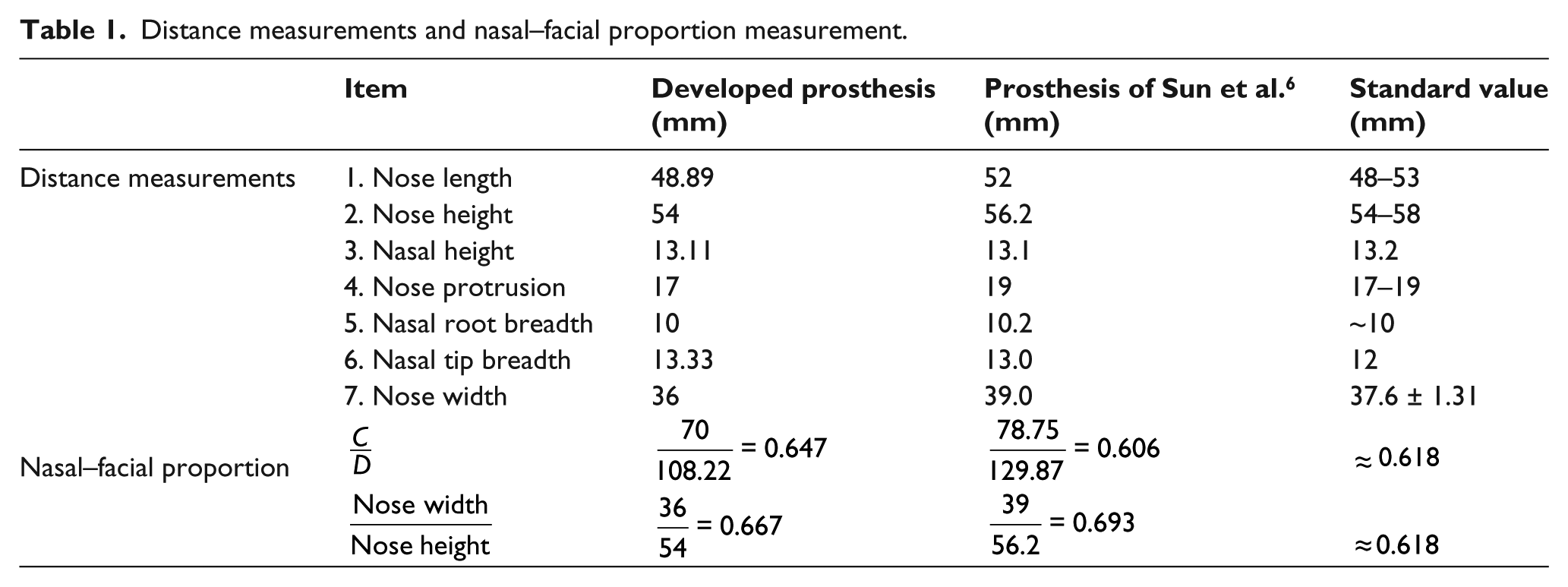
The accuracy of soft-tissue prosthesis is essentially a subjective visual assessment. The prosthesis should be convincing in restoring the appearance of the patient. In this case, it is assumed that the prosthesis has the correct size, position and anatomical shape, capable of restoring the fault limb. The agreement between the standard values and the distance and nasal–facial proportion measurements (Table 1) also support this conclusion.
The nasal prosthesis presents a skin colour similar to the patient’s skin tone. However, it is not able to reproduce the specificity of some facial features as delicate skin folds, wrinkles, texture, among others. An extrinsic colouring may give a valuable help on this matter, therefore further work needs to be done.
Time demands and costs
Table 2 lists the minutes required to perform each task and also the costs associated with it. In comparison to recent studies, that indicate delivery times of 19 h 11 and 27 h, 20 min, 12 the presented approach demonstrated to be remarkable as it offers competitive delivery times (21 h, 39 min). Regarding costs, the proposed methodology leads to cost savings in contrast to the manual procedure, which has a total cost of approximately €651 per prosthesis. 12
Costs and time demands.
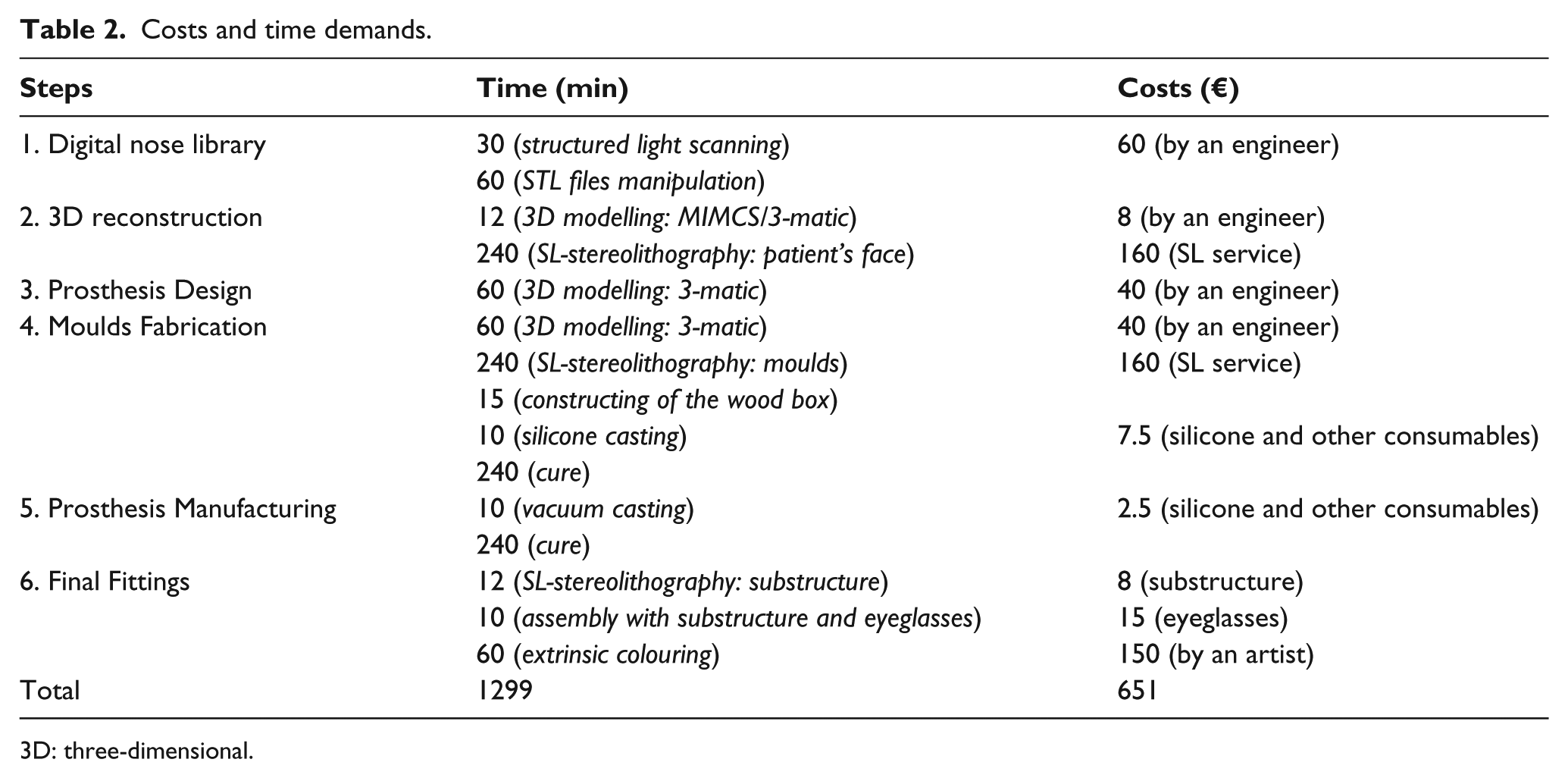
3D: three-dimensional.
Patient satisfaction
According to patient’s report, she is very satisfied with the prosthesis in several aspects: aesthetic, local attachment, cleanliness and usage. The patient mentioned that the nasal prosthesis brought significant improvements to her quality of life and enhancements to her social life, where no one looks anymore at her as a aberration or with any discrimination. To conclude, the patient expressed her gratitude, and confessed that she never thought that having an ordinary appearance again could make her so happy. Now, her grandchildren no more fear her and enjoy being with her.
Key points
The proposed methodology revealed encouraging results in comparison with the conventional method (manual procedure by an anaplastologist) since it saves time, reduces costs, and at the same time allows the attainment of prosthesis with the minimum contact and discomfort for the patient, disclosing excellent results in terms of aesthetic and function.
The adopted retention system presents an anatomical shape that fits well on nose cavity allowing the correct placement of the prosthesis without any open margins around the contact region. The vertical placement of the prosthesis is ensured by the eyeglasses.
Studies on methods for improving the surface resolution of the nasal prosthesis are pointed out as upcoming developments. Manual sculpting of plastic molds could be a solution to achieve silicone prostheses with customized skin features, such as folds, wrinkles and textures. Nonetheless, alternative techniques with some level of automation are preferable.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Conflict of interest
None declared.
Funding
The project SAESCTN-PII&DT/1/2011 was co-financed by Programa Operacional Regional do Norte (ON.2 – O Novo Norte), under Quadro de Referência Estratégico Nacional (QREN), through Fundo Europeu de Desenvolvimento Regional (FEDER).