
Abstract
Background:
Partial body weight-supported treadmill training has been shown to be effective in gait training for patients with neurological disorders such as spinal cord injuries and stroke. Recent applications on children with cerebral palsy were reported, mostly on spastic cerebral palsy with single subject design. There is lack of evidence on the effectiveness of such training for nonspastic cerebral palsy, particularly those who are low functioning with limited intellectual capacity.
Objectives:
This study evaluated the effectiveness of partial body weight-supported treadmill training for improving gross motor skills among these clients.
Study design:
A two-period randomized crossover design with repeated measures.
Methods:
A crossover design following an A–B versus a B–A pattern was adopted. The two training periods consisted of 12-week partial body weight-supported treadmill training (Training A) and 12-week conventional gait training (Training B) with a 10-week washout in between. Ten school-age participants with nonspastic cerebral palsy and severe mental retardation were recruited. The Gross Motor Function Measure-66 was administered immediately before and after each training period.
Results:
Significant improvements in dimensions D and E of the Gross Motor Function Measure-66 and the Gross Motor Ability Estimator were obtained.
Conclusions:
Our findings revealed that the partial body weight-supported treadmill training was effective in improving gross motor skills for low-functioning children and adolescents with nonspastic cerebral palsy.
Clinical relevance
Our preliminary findings demonstrated that partial body weight-supported treadmill training was a treatment of choice for improving gross motor functioning related to standing and ambulation for low-functioning children and adolescents with nonspastic cerebral palsy and limited intellectual capacity.
Introduction
Partial body weight-supported treadmill training (PBWSTT) employs overhead suspension and harness to relieve part of body weight (BW) while walking on a treadmill machine. It allows task-specific and repetitive training 1 with postural support that promotes lower limb coordination 2 and minimizes compensatory movements. 3 With the body unweighting support, therapists can provide gait facilitation and correction in a safe environment even before the recipient has attained sufficient weight-bearing and postural control in standing. 4 It has opened gait training possibilities for people with higher degree of involvement and for people with large body size and BW.
Over the past 20 years, PBWSTT has been shown to be effective for gait training of patients with neurological disorders such as spinal cord injuries,5,6 Parkinson’s disease, 7 and stroke.1–3 Recent studies have directed interests in evaluating its effects on children with cerebral palsy (CP).4,8–14
CP is an umbrella term describing a group of permanent but nonprogressive defects or lesions of the brain that occurs during early childhood. 15 Although the condition is attributed to a nonprogressive encephalopathy, its secondary complications change over time causing activity limitations throughout the entire life span. With improved survival in CP, it has become one of the largest physical impairment groups among adults. 16
Adults with CP experienced an early decline in hysical function associated with aging and secondary complication, 17 and pre-senile walking deterioration among those who are ambulatory has been well documented.18–20 In a review of 29 published journal articles evaluating PBWSTT for individuals below 21 years of age with or at risk of motor disability, Damiano and DeJong 21 concluded that there was evidence for the efficacy of treadmill training in accelerating walking development in Down syndrome. PBWSTT serves a potential role as proactive training for adolescents at risk of early decline in ambulatory function.
Different PBWSTT protocols have been proposed for children with CP with the treadmill speed set at 0.07–1.4 m/s. The training duration ranged from 12 to 35 min per session at frequency ranged from 2 to 12 times per week for a period of 2 to 17 weeks. All these studies reported positive results, and most of them recruited children with spastic CP.4,8,9,11–13,22 In a systematic review of seven PBWSTT studies on children with CP, five were conducted exclusively on spastic CP, and the strength of evidence was found to be weak. 23
Only two studies targeted at participants with nonspastic type of CP, but the findings were inconclusive.10,14 Yu 14 reported no improvement for participants with athetoid and dystonia. In a matched-pair controlled trial, Dodd and Foley 10 demonstrated positive effects on walking speed and endurance among participants with athetoid. It has been reported that spastic CP is making up 61%–77% of all CP cases. 24 In Hong Kong, nonspastic CP constituted around 26% among the population of children with CP. 25 The aim of this study was to explore the feasibility of employing PBWSTT for improving gross motor skills among children and adolescents with nonspastic CP, in particular those at low-functioning level and with limited intellectual capacity.
A local study in Hong Kong comparing the mean Gross Motor Function Measure (GMFM) scores of children with spastic diplegia and dyskinetic CP found that the dyskinetic group scored lower than the spastic group. 26 Generally speaking, low-functioning CP encountered greater difficulty in receiving motor training. The situation is further complicated in the presence of mental retardation as their motor capacity may often be masked by their low intellectual capacity. Moreover, a number of techniques in conventional gait training are not applicable especially when they grew into adolescents with larger body size and weight. With limited interventions claiming to be targeted at low-functioning children and adolescents with nonspastic CP, PBWSTT may open a new possibility for gait training for this group of clients.
The objective of this study is to evaluate the effectiveness of PBWSTT for improving gross motor skills among children and adolescents with severe mental retardation and nonspastic type of CP. We hypothesized that PBWSTT is more effective than conventional gait training in improving gross motor functions related to standing and walking among the target population.
Methods
In this study, the classification system proposed by the Surveillance of CP in Europe was adopted. 27 To differentiate the severity of lower limb involvements, the Gross Motor Function Classification System (GMFCS) 28 was also employed. Palisano et al. 29 constructed curves, for each GMFCS level, that described the nonlinear relationship between age and gross motor function expressed in terms of the GMFM score for the CP population. 30 Palisano et al. 29 established a predicted maximal GMFM score for each GMFCS level with a correlation of −0.91. Since individuals with CP are subject to accelerated deterioration due to normal aging and secondary complications, there exists a need to assist adolescents with CP to keep their GMFM scores at the plateau levels as far as possible.
Children and adolescents aged between 6 and 17 years old with a diagnosis of nonspastic CP, including choreoathetotic, dystonic, and unclassified CP, were recruited from a special school for severe-grade mental handicaps. All of them had no previous experience of PBWSTT and did not undergo orthopedic intervention or change in medication in the past 6 months. Ethical approval (Approval Code: HSEARS20080103001) was obtained from the Human Ethics Committee, and informed consent was obtained from their parents prior to the experiment.
An electric ceiling track hoist (Likorall 242S R2R; Liko AB, Sweden) was used to partially relieve the participant’s BW. An adjustable harness (Liko MasterVest, Mod. 60, Liko AB, Sweden) was connected to the motor unit of the hoist for applying an uplifting force via the participant’s trunk and thighs without the impingement of armpits (Figure 1). The uplifting force was monitored by an electronic scale (LikoScale 350; SR Instruments, Inc., USA) to the nearest 2 N. A treadmill (JKexer, Gallant 7700M 2.0; Jih Kao Enterprise, Taiwan) was placed directly under the motor unit with its walking direction aligned with the ceiling-mounted track of the hoist. The starting speed of the treadmill was 0.36 m/s with an increment of 0.045 m/s. For the conventional gait training, strengthening of lower limb muscles, mat exercises for proximal and distal weight-bearing and weight-shifting as well as assisted standing and walking with ladder frame were given.

Experimental setup of the partial body weight-supported treadmill training.
GMFM with 88 test items categorized into five dimensions (A–E) and rated by 4-point Likert scale (0–3) is a standardized clinical assessment for measuring gross motor performance of children with CP. 30 A short version of GMFM with 66 items (GMFM-66) 31 was employed in this study. Gross Motor Ability Estimator (GMAE) that converts the ordinal scores of individual test items into a total score of interval scale 32 together with the sub-scores of dimensions D (GMFM-D) and E (GMFM-E) of GMFM was employed as the outcome parameter of this study.
A randomized two-period crossover design was adopted. Ten participants were randomly assigned into two groups (Groups I and II). Each group received 12-week PBWSTT and 12-week conventional gait trainings. A washout period of 10 weeks was put in place between the two training periods. Group I received PBWSTT during the first training period followed by conventional gait training, while Group II received conventional gait training first followed by PBWSTT. Within the training period, each participant was assessed twice, that is, the week before and after the 12-week training period (Table 1).
Experimental schedule of the crossover design with A–B and B–A patterns for Groups I and II with PBWSTT as “Training A” and conventional gait training as “Training B”.
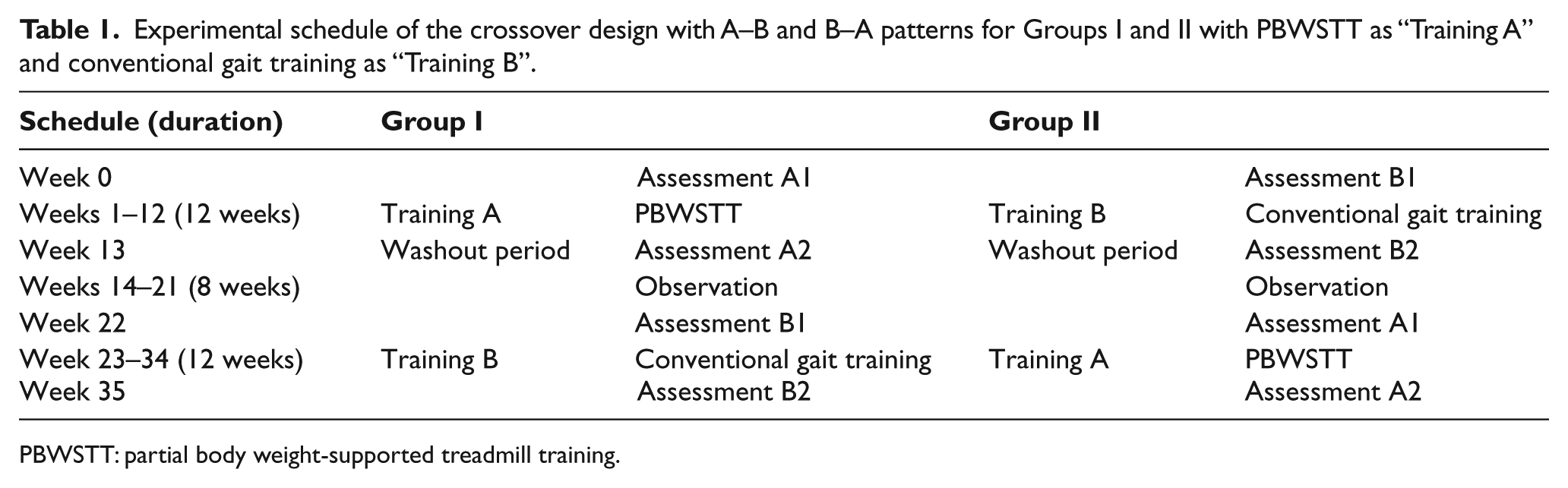
PBWSTT: partial body weight-supported treadmill training.
During the treadmill training, the initial body unweighting support was set at 30% of BW of individual participants12,33 who were requested to walk on the treadmill at 0.36 m/s for 10 min. Whenever necessary, gait modification, such as foot placing, was applied by a physiotherapist during the treadmill walking. A 5-min break was given before another 10-min walk during which the amount of body unweighting support and the treadmill speed were adjusted as the articipant tolerated. The treadmill speed was capped at 0.8 m/s during the first training session and the cap was released if no adverse effect was reported. The minimum body unweighting support at the slowest starting speed that the participants walked comfortably coupled with the maximum treadmill speed that was maintained for at least 5 min during the second 10-min treadmill walking was documented. During the PBWSTT, each participant attended the 25-min treadmill training twice per week.
The conventional gait training was administered by another physiotherapist according to individual walking capacity of the participants. Each participant received 30-min conventional gait training three times a week. A trained assistant was provided for external support to participants of GMFCS levels IV and V. Both groups received no regular gross motor training apart from the two training methods under investigation.
Results
Demographic data of the 10 participants are tabulated in Table 2. Participant 5 of Group I opted out after attending two sessions of PBWSTT due to hospitalization caused by chest infection, while participant 10 of Group II dropped out before the second training period commenced due to gastrointestinal infection. Among the eight participants who had completed the study, all except one participant were of dyskinetic type among whom six were choreoathetotic and one was dystonic. The remaining participant was unclassified (i.e. hypotonic without ataxia). Five participants were at GMFCS level IV, and the remaining three were at levels II, III, and V. With random allocation, the four participants at GMFCS level IV were assigned to Group II, while the four participants at GMFCS levels II, III, IV, and V were assigned to Group I (Table 2).
Demographic data of the 10 participants. Participant 5 of Group I and participant 10 of Group II opted out resulting in eight participants who had completed the study. Participants were classified by a combined use of the Surveillance of Cerebral Palsy in Europe classification and the GMFCS.
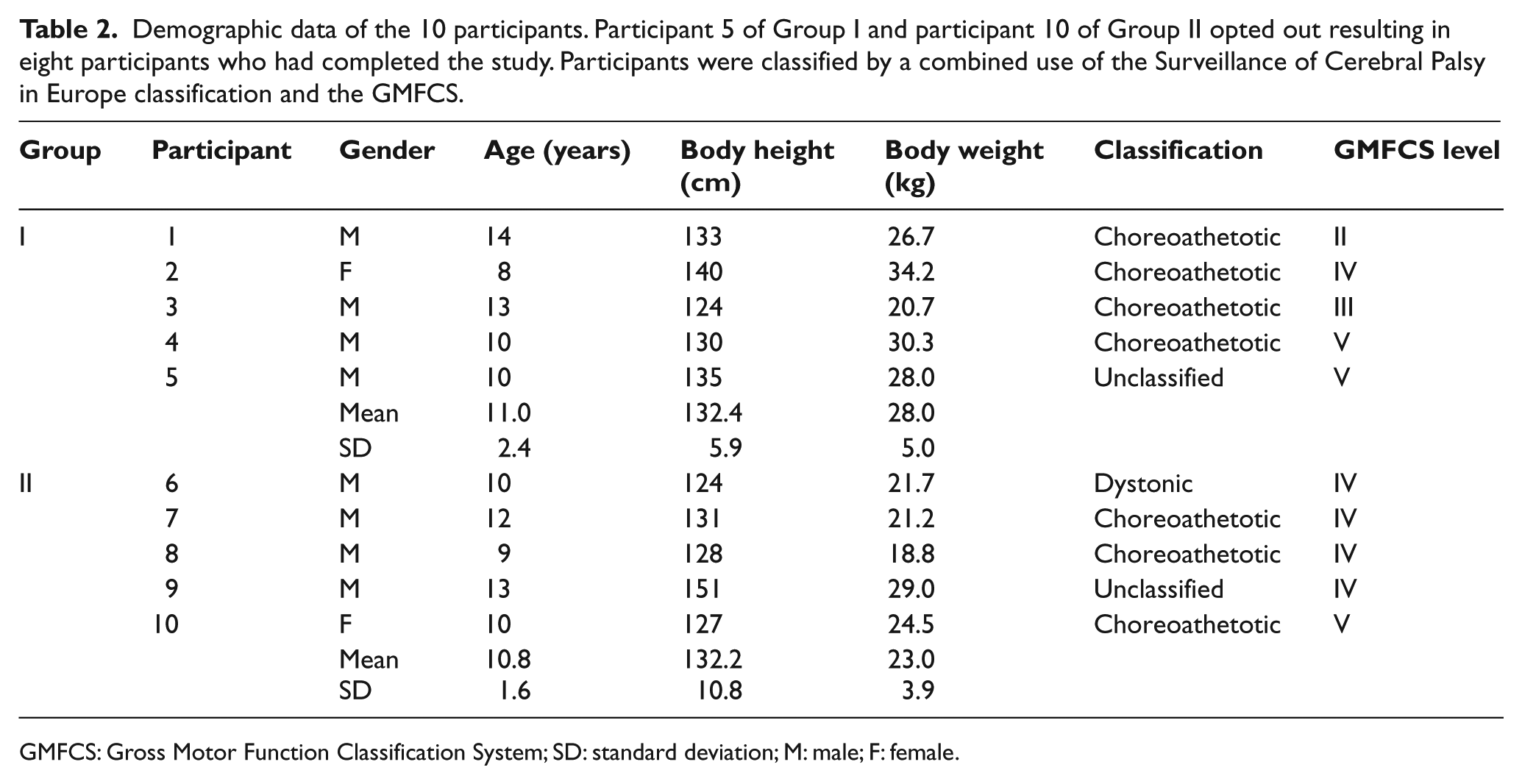
GMFCS: Gross Motor Function Classification System; SD: standard deviation; M: male; F: female.
None of the participants attended all 24 treadmill training sessions due to health and emotional problems. The number of sessions attended and the total duration of treadmill training received by each participant are tabulated in Table 3. All participants managed to reach the cap in walking speed (0.8 m/s) during the first treadmill training session. Since no adverse effect was reported after the training, the cap was released for all participants in all remaining sessions. The minimum body unweighting support, expressed in terms of the percentage of BW, and the maximum walking speed attained by each participant during the first and last sessions are also shown. Significant increase in walking speed (p < 0.05, paired t-test) with no significant difference in the amount of body unweighting support was reported (Table 3).
The total number of sessions and the total duration of the PBWSTT received by the eight participants during the PBWSTT of Groups I and II and the corresponding minimum body unweighting support (expressed in terms of percentage of body weight) and maximum walking speed attained at the first and last sessions of the PBWSTT of each group.
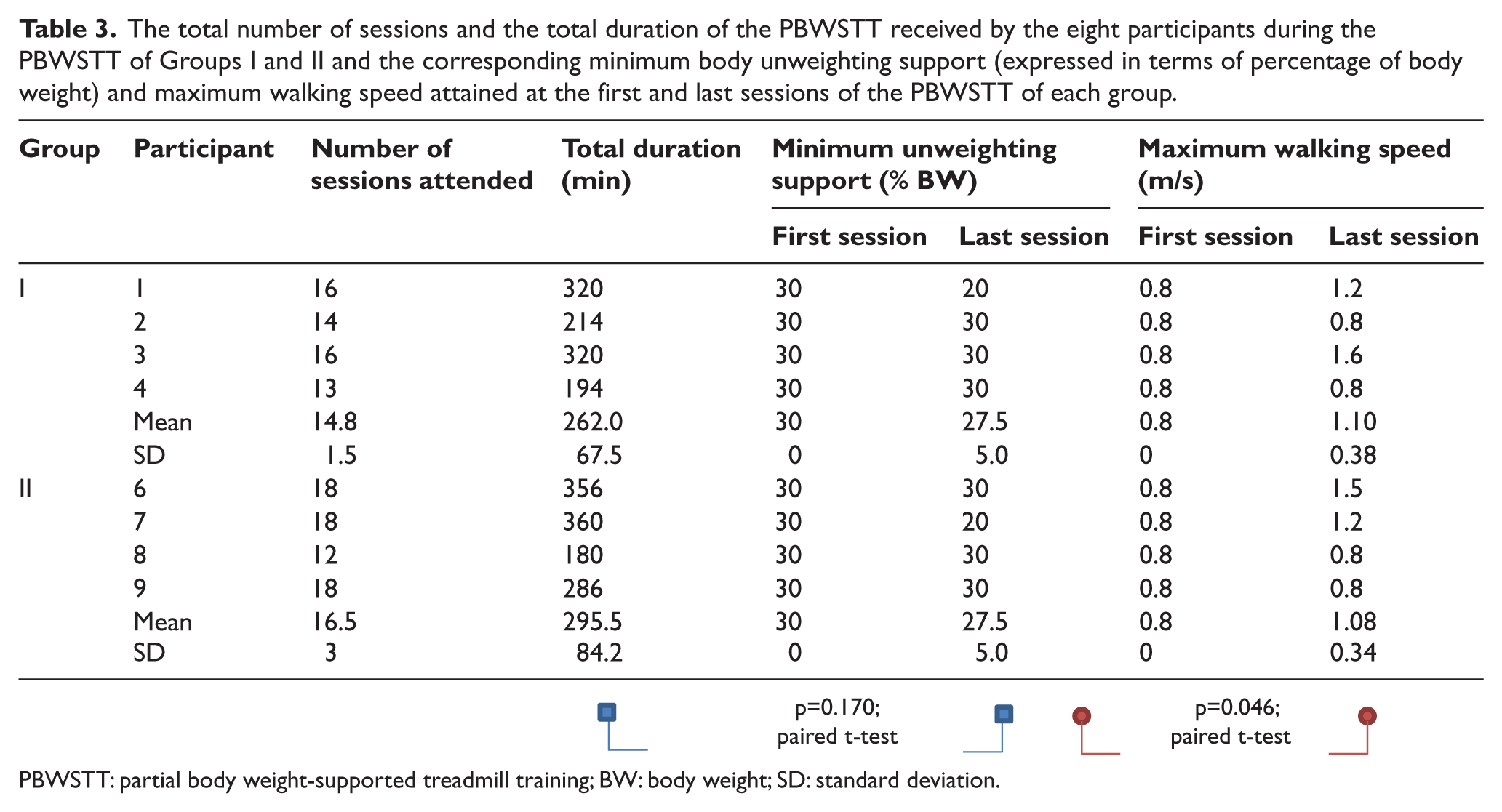
PBWSTT: partial body weight-supported treadmill training; BW: body weight; SD: standard deviation.
The percentage total scores of the GMFM-D and GMFM-E were processed with respect to their respective full scores. In the two-period crossover design, only one observation of each outcome parameter was taken from each participant in each training period. 34 Each observation was evaluated by subtracting the value obtained at Assessment 1 from that of Assessment 2. The mean values of the change as obtained from the PBWSTT were found to be consistently greater than that of the conventional gait training across the three outcome parameters (Table 4).
Comparison of changes in GMFM-D, GMFM-E, and GMAE after the 12-week training period as calculated by (A2 − A1) for the PBWSTT and by (B2 − B1) for the conventional gait training. The means of change across the three outcome parameters from the PBWSTT were consistently greater than that of the conventional gait training with significant differences between the two training at all the three outcome parameters with p < 0.05.
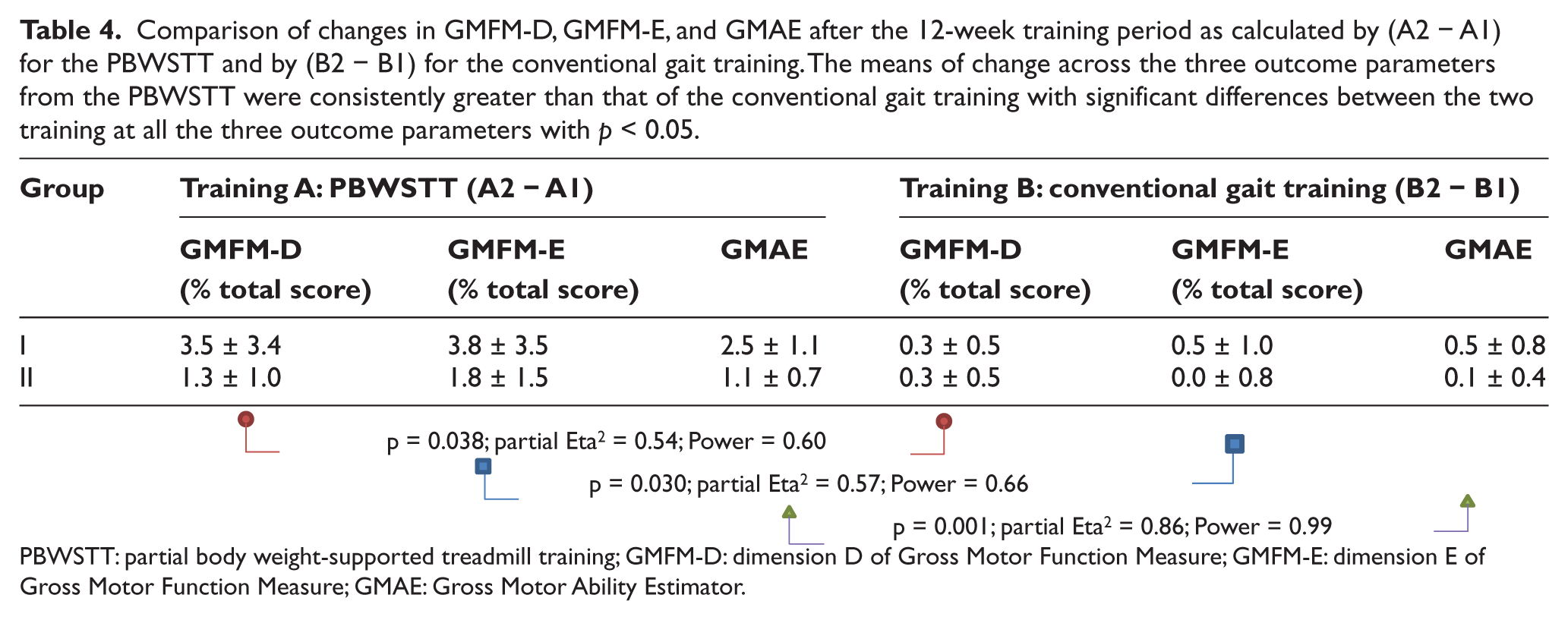
PBWSTT: partial body weight-supported treadmill training; GMFM-D: dimension D of Gross Motor Function Measure; GMFM-E: dimension E of Gross Motor Function Measure; GMAE: Gross Motor Ability Estimator.
The changes in GMFM-D and GMFM-E and the GMAE scores of the eight participants were analyzed using mixed-design analysis of variance (ANOVA) with repeated measures. The PBWSTT and the conventional gait trainings were treated as within-group “Training” factor, while Groups I and II were treated as between-group “Sequence” factor. All data were analyzed using statistical software (IBM SPSS Statistics 20; IBM, USA). Significant effects of the “Training” factor were obtained across all outcome parameters with p < 0.01 for GMAE and p < 0.05 for GMFM-D and GMFM-E (Table 4). Both the effect size and power in the GMAE score were high (partial Eta2 = 0.86, power = 0.99), while those of the GMFM-D and GMFM-E were at partial Eta2 = 0.54, power = 0.60 and at partial Eta2 = 0.57, power = 0.66, respectively.
Apart from the “Training” factor, the other two main effects within the two-period crossover design are due to “Sequence” and “Period” factors. The former refers to the sequence of the two training methods (i.e. A–B or B–A pattern), and the latter refers to the order of the two training periods (i.e. a particular training method being administered in the first or in the second training period). The “Sequence” factor was the between-group factor in the mixed-design ANOVA with repeated measures, and no significant main effect was found. The period effect (the interaction term in the mixed-design ANOVA with repeated measures) was also not significant across all the three outcome parameters.
The carryover effects were studied by examining the interactions between the “Training” and “Period” factors. Carryover effects refer to an asymmetrical transfer effects in which difference in population mean for one training method between its administration in the first and second training periods is different from the corresponding difference for the other training method. 35 In other words, the total sum of changes in the observations due to PBWSTT and conventional gait training across all participants within Group I should be the same as that of Group II. The carry- over effect can be examined from the changes of the three outcome parameters plotted as a function of the training method and the orders of the training period. By examining these plots, carryover effects were suspected (Figure 2(b)). To test for the carryover effects, the total sum of the changes in GMFM-D, GMFM-E, and GMAE scores as obtained from PBWSTT and conventional gait training in Groups I and II was calculated for individual participants. No significant differential carryover effects were found between the PBWSTT and conventional gait trainings (p = 0.303, 0.307, and 0.114 for GMFM-D, GMFM-E, and GMAE respectively, independent sample t-test) (Table 5).
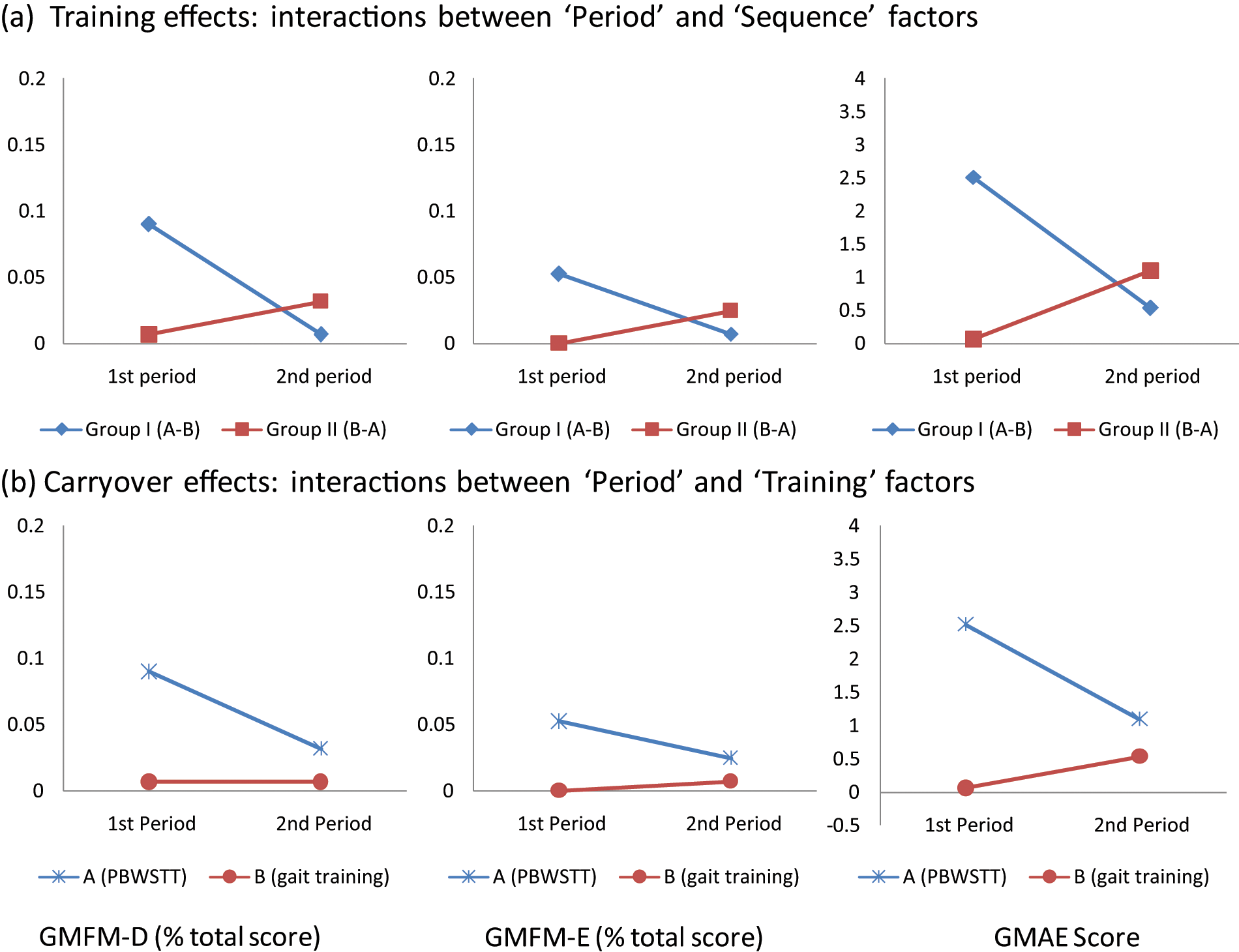
The response observations (changes in GMFM-D, GMFM-E, and GMAE) plotted (a) as a function of the “Period” (administered in the first and second training periods) and “Sequence” factors (Group I: A–B pattern; Group II: B–A pattern) for examining the main effect of the two training methods and a significant training effect was found (p < 0.01, mixed-design ANOVA with repeated measures) and (b) as a function of the “Period” and “Training” factors (Training A: PBWSTT; Training B: conventional gait training) for examining the presence of differential carryover effects of the two types of training methods under study with no significant carryover effects reported.
Changes in GMFM-D, GMFM-E, and GMAE in the partial body weight-supported treadmill training and conventional gait training and the sum of changes across participants in both trainings for Groups I and II. The mean and standard deviation of the sum of changes for each outcome parameter were also determined. The carryover effect was evaluated by examining the between-subject and within-subject variability of the sum of changes. No significant difference was reported (p = 0.303, 0.307, and 0.114 for GMFM-D, GMFM-E, and GMAE, respectively, independent sample t-test).
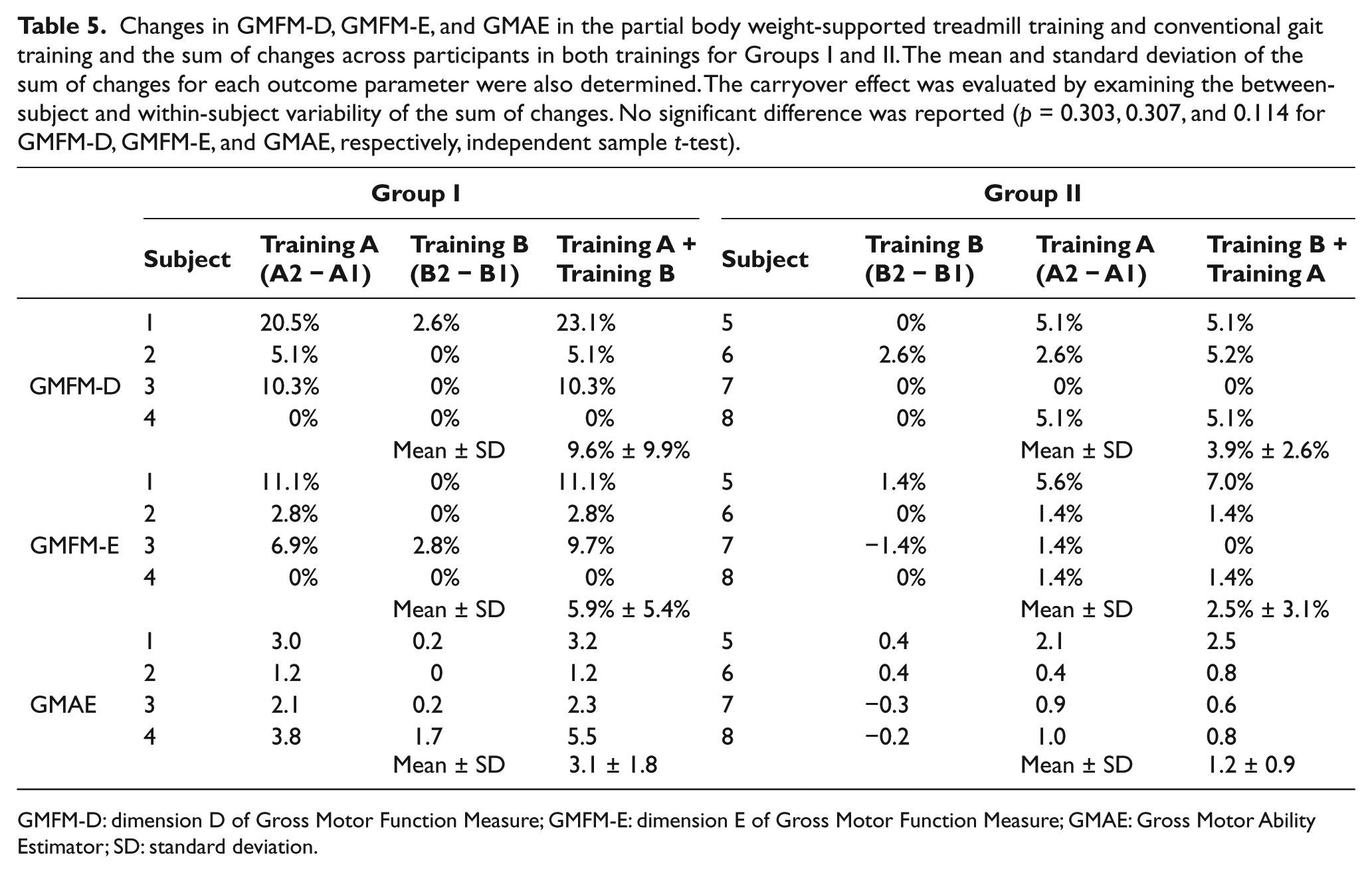
GMFM-D: dimension D of Gross Motor Function Measure; GMFM-E: dimension E of Gross Motor Function Measure; GMAE: Gross Motor Ability Estimator; SD: standard deviation.
Discussion
Physical intervention for CP has been shifted from a reactive symptom-based approach to a proactive activity-based approach over the life course.36,37 An active lifestyle is advocated to combat against the age-related functional deteriorations of CP. PBWSTT serves well as a means toward this goal particularly for low-functioning grown-up children with CP. Despite the fact that no general conclusion can yet be made regarding the efficacy of PBWSTT on children with spastic CP,21,23 the PBWSTT increases the feasibility of gait training even for those who are low functioning with severe mental retardation.
In this study, the training frequency of the PBWSTT was set at twice per week, lower than the training protocols adopted in previous studies.4,8,9,13,22 Some of these studies involved assistants,4,10,13,22 while only one physiotherapist was provided during the treadmill training sessions in this study. However, the training frequency of the conventional gait training was three times per week with a duration of 10 min longer than that of the treadmill training sessions. An assistant was provided for participants of GMFCS levels IV and V. The total number of hours of conventional gait training for individual participants was higher than that of the PBWSTT.
In a study on the correlation between GMFM-66 and functional performance, Ostensjø et al. 38 demonstrated that the GMFM-66 was a strong predictor accounting for 88% of variations in mobility among children with CP. To monitor gross motor functioning, a number of studies employed the dimensions D for standing (GMFM-D) and E for walking, running, and jumping (GMFM-E).4,8,9,13,22 Since both the dimensions D and E of GMFM are included in the GMFM-66, the total score of GMFM-66 (expressed in GMAE score) and the GMFM-D and GMFM-E sub-scores were used as outcome measures in this study.
Significant difference in outcome parameters was observed after the 12-week training period (p < 0.01) (Table 4). Despite fewer training hours and less manpower input, all the three outcome parameters of the PBWSTT were consistently at a higher level than that of the conventional gait training suggesting that the former is a treatment of choice for improving gross motor functioning in standing and walking for the targeted population group.
Compared with the two previous PBWSTT studies for children with nonspastic CP,10,14 this study involved more participants and satisfied more stringent experimental design requirements. The crossover design has the advantages of using each participant as one’s own control. It serves to increase statistical power by removing participant effect from affecting the tests for the training effects. Despite the advantages of using crossover design in this study, the possible carryover effect is still a limitation of this study. This is crucial for accommodating the heterogeneity among the participants recruited in this study. In addition, more robust and sensitive outcome parameters were used to evaluate the treatment outcomes. In contrast to the findings by Yu, 14 this study demonstrated the beneficial effects of the PBWSTT for children with nonspastic CP.
Among the three main effects (training, sequence, and period), the only significant effect was found in the “Training” factor (p < 0.01), as revealed from the interaction between the “Period” and “Sequence” factors across the three outcome parameters (Figure 2(a)). An asymmetrical transfer of the training effects between the PBWSTT and the conventional gait training was suspected (Figure 2(b)). However, the difference in population means between the treadmill training in Group I (administered in the first training period) and Group II (administered in the second training period) was not significantly different from the corresponding difference in population means for the conventional gait training.
The improved gross motor skills can be attributed to the activity nature of the treadmill training, which is specific to the ambulatory task. It provides an accommodative yet stimulating environment for the participants to experience ambulatory movements that are not possible in conventional physiotherapy. It creates opportunities for them to learn and develop adaptive skills to meet the finely tuned environmental demand through repetitive training. The partial BW support overcomes the weight-bearing challenge of an upright posture that has effectively reduced the environmental demand on postural control and body alignment.
With safety and stability guaranteed by the instrumentation, a physiotherapist can accomplish the treadmill training single-handedly even on low-functioning grown-up clients. Unlike the conventional physiotherapy, an assistant is no longer needed. The PBWSTT opens an opportunity for the targeted clients to walk for an extended period of time that cannot be experienced on level ground.
A convenient sample was recruited in this study. All participants were recruited from a special school for severe mental handicaps, and the sample was biased and might not reflect the general population of children with nonspastic CP. The small sample size, together with the dropout of two participants from each group, further compromised the results of this study. Among the eight participants who had completed the study, there were three types of nonspastic CP, including choreoathetotic, dystonic, and the unclassified type. Lack of homogeneity made the identification of significant effects difficult. This study revealed a potential, though not significant, differential carryover effects between the two trainings under investigation. A completely randomized design is recommended for future studies of the treadmill training with partial BW support for people with nonspastic CP; however, a larger sample size is required to reach a reasonable statistical power.
Conclusion
In this study, comparisons were made between the PBWSTT and the conventional gait training on gross motor skills for low-functioning nonspastic CP. To accommodate the lack of homogeneity among the targeted participants and the small sample size, a randomized two-period crossover design was adopted, and the training outcomes after the 12-week training period were evaluated. No adverse effect was reported in both training methods. Significant improvement in walking speed together with significantly higher scores in gross motor functioning related to standing and ambulation was reported in the treadmill training. However, differential carryover effects between the two training methods were suspected though not significant. To conclude, our preliminary findings revealed that the PBWSTT is a feasible and cost-effective training option for improving gross motor skills for the targeted population group. Further studies with larger sample size, higher sample homogeneity, and a completely randomized design are warranted. Future studies can also be directed at the long-term outcomes of the training and on the underlying mechanism of such improvements.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.