
Abstract
Background:
Sitting cross-legged as an activity of daily living and its kinematics have significantly different demands on the arthroplasty of hip and knee, which can be referred in the design of joint arthroplasty.
Objectives:
The purpose of this study was to obtain the kinematics of the lower limb in Chinese people during cross-legged sitting.
Study design:
This study identified the necessary requirements for joint arthroplasty to carry out sitting cross-legged activity.
Methods:
A total of 40 healthy Chinese participants (average age = 23.8 years) performed six cross-legged sitting trials per person. Three-dimensional kinematic data of ankle, knee, and hip joints were collected; the means of the three-dimensional angles of these three joints were calculated.
Results:
At the hip, the range of motion of the flexion was 101.7°, the abduction reached 43.2°, and the range of motion of the external rotation was 36.4°. At the knee, the range of motion of the flexion was 131.9° and the range of motion of the internal rotation reached 32.4°. At the ankle, the range of motion in three planes was not great.
Conclusions:
Such motion ranges were likely to result in prosthetic dislocation. The results would provide valuable references for prosthesis design in the Chinese population.
Clinical relevance
The kinematic data of sitting cross-legged activity provided the baseline information for physicians and therapists concerned with the surgical and functional rehabilitation, and offered reference for lower limbs prosthesis designing.
Introduction
Due to the differences in cultural history and tradition, the lifestyle of Asians and Westerns differs in many different ways. Physically, there are more activities or postures involving larger range of motion (ROM) at lower limbs joints with Asians. Sitting cross-legged is such a living activity, which as a means of resting appears to have developed more extensively in Eastern cultures than in the Western countries. It is one of the most common postures in countries such as India, Japan, South Korea, and China, which have large populations. However, the commonly used joint arthroplasty techniques developed in western countries have not taken account of the persistent sitting cross-legged activity. Therefore, it is necessary to do a research on the joint arthroplasty to meet the lifestyle requirements of Chinese patients.
As the objective of the joint arthroplasty is to help patients return to an active state, so it is necessary to have the arthroplasty designed based on the normal kinematic data of the joints during sitting cross-legged in healthy population. These kinematic data would have significant effect in determining the work range of the artificial joint components of hip and knee. To the authors’ best knowledge, few studies have been conducted on the kinematics of knee, hip, and ankle joints for the critical sitting cross-legged activity. Kapoor et al. 1 conducted a survey about angular motion at the three joints on 44 Indian volunteers with a simple goniometer; however, the kinematics of knee and ankle in frontal and transverse planes were not given. Hemmerich et al. 2 collected the joint motion data on 30 healthy Indian subjects during high ROM activities of daily living, which included the sitting cross-legged activity. These two studies exhibited that the ROMs required to perform this posture were greater than that provided by most currently available joint prostheses. In addition, nobody has conducted specialized measurement and research on this activity. Many rehabilitation articles referred to this activity and considered it as a challenging activity for the patients who underwent the joint arthroplasty.3 –6 However, the sitting cross-legged activity has been referred to only as a functional rehabilitation reference of the main lower limb joints of the patients. As far as the authors have been aware, no studies specially describing the relation of sitting cross-legged and rehabilitation have been reported. Thus, it has been clear that the kinematic information about the joints in a posture of sitting cross-legged has been insufficient, not enough to support the joint prosthesis design that will meet the needs of Asian populations.
In this study, the widely used three-dimensional (3D) optical motion tracking system was used to measure the kinematics of the lower limbs during sitting cross-legged activity. On completion of the study, the ROMs of hip, knee, and ankle joints during sitting cross-legged activity collected from the healthy Chinese adults were reported. Furthermore, the continuous kinematic curves of three joints were presented to show the angular movement process from cross-legged sitting to standing up. This research identified the necessary requirements for the joint arthroplasty and clarified whether the joint arthroplasty had enough motion capability to conduct this activity without prosthetic impingement or dislocation.
Methods
A total of 40 healthy Chinese volunteer participants (male = 20 and female = 20) were recruited for this study. The recruited participants were students and staffs of a university. The average age was 23.8 years (standard deviation (SD) = 1.64 years), the average height was 168.9 cm (SD = 6.9 cm), and the average body mass was 56.1 kg (SD = 9.0 kg). These young adults were selected because the kinematic performance of cross-legged sitting by them would be better than that of elderly adults. All participants have lived in China and kept a traditional Chinese lifestyle; for instance, they preferred to sit cross-legged versus the traditional upright sitting position. They regularly sat cross-legged for resting and lunch and at times performed kneeling activity in occasions such as birthday rituals or traditional festivals. They commuted by bike (most Chinese women normally get use to sitting cross-legged activity as well as getting on and dismounting from a bike). They had no history of injury to or pain in the lower limbs, or any type of lower extremity surgery, neuromuscular disease, or balance problems. This study was approved by the ethics committee of author’s university, and all participants signed a consent form before participating in the tests.
Kinematic data were collected by the Optotrak® Certus™ 3020 active tracking system (Northern Digital Inc. Waterloo, Ontario, Canada). The 3D accuracy was 0.15 mm, and the resolution was set to 0.01 mm. In order to gain a more effective detect range, three Optotrak 3020 position sensors (nine cameras) were used. The motion data were collected at a sampling rate of 95 Hz. As the sampling rate would decrease when the number of the tracking markers increased, 95 Hz was the highest frequency that the tracking system could achieve when 48 tracking markers were used. Directly performing activity on the ground would make lower limb segments and infrared markers too close to the ground, and hence, the infrared markers were in a position too hard to be collected in cross-legged sitting posture. To resolve the problem, all participants performed the designated activity on a special test platform that was 50 cm in height.
In order to achieve high-quality results, during the test, all participants wore shorts to allow the secured attachment of the rigid tracking plates onto the skin of the body. Seven rigid optical tracking plates were used to track the 3D movement of all the seven segments, which were both left and right foot, shank, thigh, and pelvis. Each plate consisted of four noncollinear infrared markers. These rigid plates were placed on feet (bilateral instep), shanks (bilateral surface of tibia), thighs (bilateral surface of the thigh), and pelvis (over the center point between both posterior superior iliac spines) using the flexible cohesive elastic bandage (BandMax™, 3HMedical Inc., Nanjing, China). The rigid tracking plates were attached to the pelvis and fixed by the Velcro fasteners on the waist band. In order to prevent the bandage from loosening and avoid the relative displacement of the markers and skin, the rigid plates and limbs were secured by a common nonelastic medical bandage.
A local coordinate system for each lower limb segment was defined through digitized palpated bony landmarks on the lower limb segments using a digital probe, where the bony landmarks included left/right ilium anterior superior (LIAS/RIAS), left/right prominence of the greater trochanter (LGT/RGT) external surface, left/right femur lateral/medial epicondyle (LFLE/RFLE, LFME/RFME), left/right fibula apex of lateral (LFAL/RFAL) malleolus, left/right tibia apex of medial (LTAM/RTAM) malleolus, left/right dorsal aspect of first metatarsal (LFM/RFM) head, and left/right dorsal aspect of fifth metatarsal (LVM/RVM) head. The local coordinate system was then linked to the segment’s individual tracking plate by means of coordinate transformations. Once tracking markers were obstructed by the participants’ body, the trial was not used for any further analysis.
All participants were instructed to sit cross-legged on the foam cushion, and the sitting cross-legged posture was regarded as the initial rest position. The foam cushion was only used below the buttocks, and the outside of the leg and foot were in contact with the test platform. The cushion was 5-cm thick, and flattened when participants were at rest position, which means the body weight was supported by the test platform. Thus, the function of the cushion was to make participants feel comfortable to minimize the impact to the joint motion during the test. In order to acquire the maximum motion angle, the participants were asked to hold the sitting cross-legged position motionless for approximately 5 s and then change to the standing position at a natural pace. Each participant stood up in response to the researcher’s requests. While ascending, participants let the foot touch the ground first, then stood up on their legs, and finally uncrossed their legs. Participants performed the entire activity without using other devices and without the help of the research assistant. Each participant conducted at least six effective sitting cross-legged trials. Figure 1 shows the participants with the sitting cross-legged posture in the resting phase.
A photograph showing the participant sitting cross-legged in the resting phase.
The raw kinematic data were processed with Visual-3D (version 3.91.2; C-Motion Inc., Germantown, MD, USA), then filtered using a software-integrated digital filter, with a cutoff frequency of 6 Hz. The start of the sitting cross-legged trial was triggered by the movement of any one of the three joints, while the end of trial was defined as the termination of motion of all three joints. All the trials were normalized to 100%. The relative joint angles were calculated using a Cardan rotation sequence of x-y-z. The local x-, y-, and z-axes corresponded to flexion/extension, abduction/adduction, and internal/external rotation for the hip and knee joints, and dorsal/plantar flexion, eversion/inversion, and internal/external rotation for the ankle joint, respectively. The flexion of the hip and knee and the ankle dorsiflexion were positive; hip, knee, and ankle abduction were positive; and hip, knee, and ankle external rotation were positive. The kinematic results were saved in ASCII format and transferred to Excel and Graphpad version 5.00 (Prism 5 for windows).
The variations of the joint angles at hip, knee, and ankle were quantified and presented by the mean value between the sitting cross-legged and standing-up positions. The angles of all three joints in all planes were presented. Six trials were used in the computation of the mean value for each participant. These individual data were then averaged to provide the ensemble mean value. Correspondingly, the mean kinematic curves for each participant were used to create an ensemble mean curve.
Results
Three-dimensional hip, knee, and ankle joint angles of the sitting cross-legged position are presented in Table 1, where the number of participants is denoted by n. The ensemble mean joint angle curves and SDs for three joints are presented in Figure 2. For the flexion/extension motion, the SDs at the hip, knee, and ankle were smaller than those for the abduction/adduction and internal/external rotation. The ROMs of flexion in the sagittal plane were 131.9° at the knee, 101.7° at the hip, and 12.3° at the ankle; the flexion ROMs at the knee and hip joint were significantly greater than other motions in all three planes.1,2 In the frontal plane, the maximum ROM of abduction was 43.2° at the hip and the maximum ROM of adduction was 28.3° at the ankle, respectively. In the transverse plane, the maximum ROM of external rotation was 36.4° at the hip and the maximum ROM of internal rotation was 32.4° at the knee, respectively. The ROMs of hip extension, hip adduction, knee adduction, knee external rotation, and ankle external rotation were quite low.
Measured kinematic data of hip, knee, and ankle joints in sitting cross-legged (°).
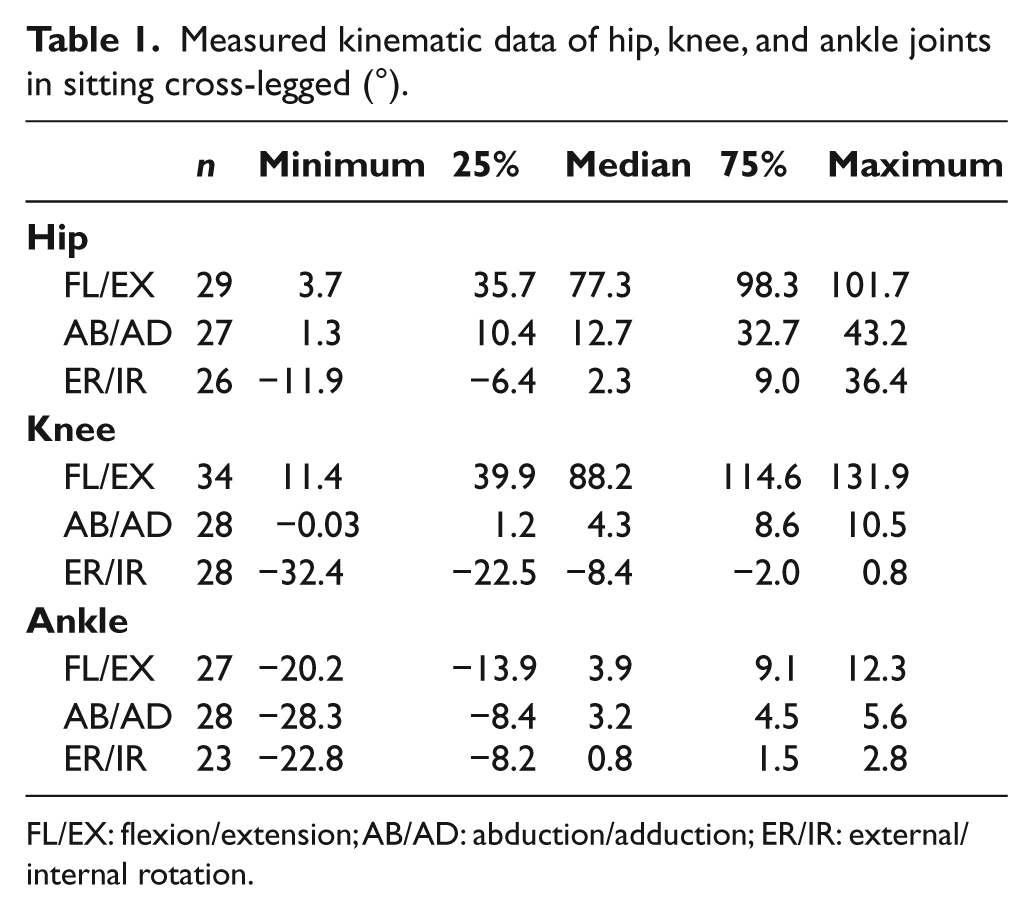
FL/EX: flexion/extension; AB/AD: abduction/adduction; ER/IR: external/internal rotation.
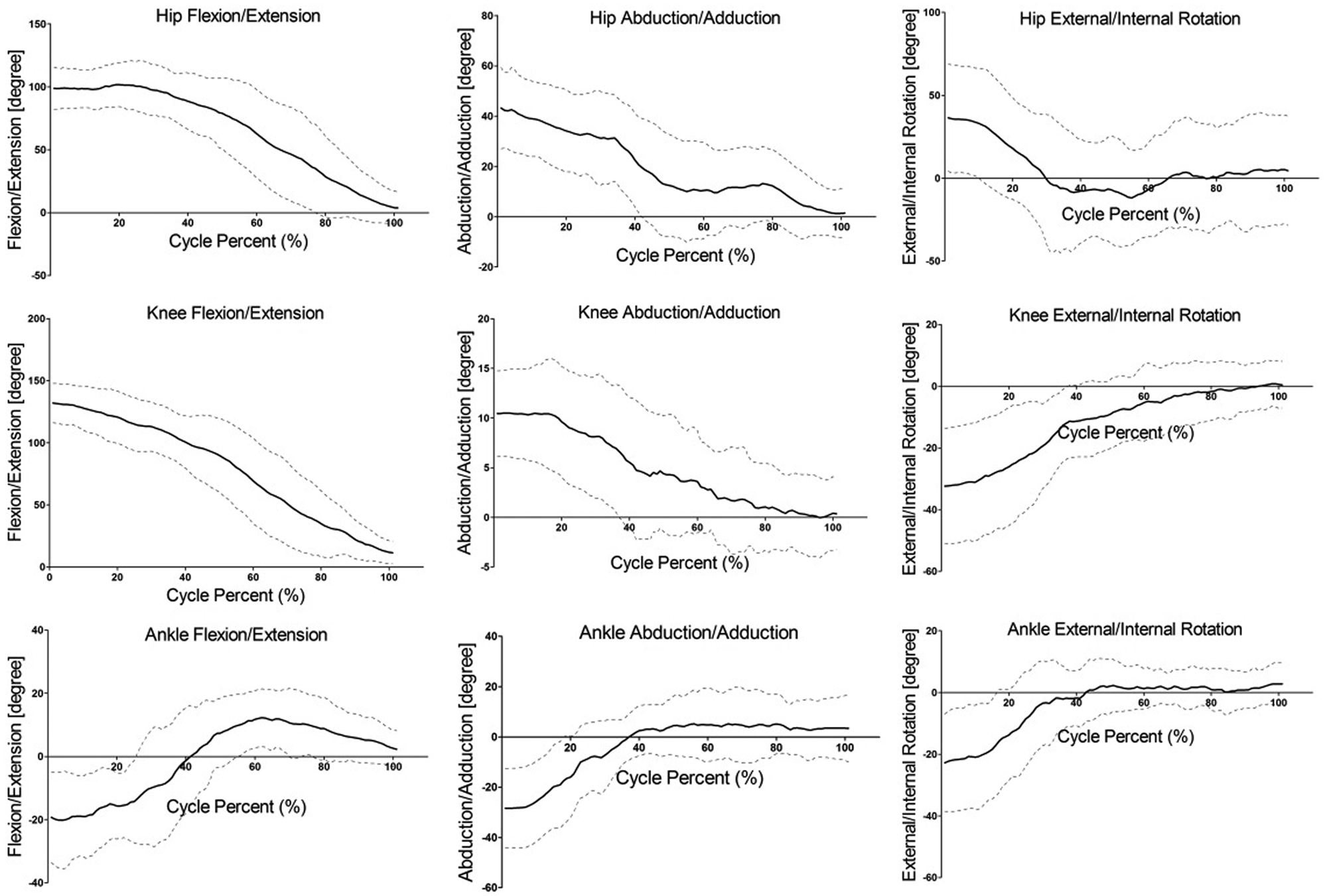
Kinematic curves and standard deviations of sitting cross-legged.
Discussion
Some oriental unique deep flexion activities have been widely used in oriental countries, such as kneeling, transplanting rice seedlings, and sitting cross-legged, whether joint arthroplasty is in support of these activities has caused more and more attention in the majority of oriental patients. Although the problem has gradually become a concern among the patients with joint abnormalities, little research has been done about these activities; therefore, it deserves special attention and penetrating research. In this study, we focused on the kinematics data of lower limbs in sitting cross-legged. In order to make sure the data were complete and correct, a large sample of young adults whose joint mobility and ROM are usually excellent was selected; hence, these measured data were more meaningful and useful for lower limbs prosthetics design and assessment for the treatment.
In this study, each participant had unlimited time to prepare before trial; each trial did not influence the earlier trial because the new trial started when the participant felt relaxed. Moreover, young participants have more vigorous body power and fine motor abilities, so consistence and reliability could be assured. Notably, sitting cross-legged was difficult for the obese, which could be attributed to the compression of the posterior soft tissues (skin, fat, muscle, and posterior capsule) between the calf and the thigh, and their excessive weight appeared to have played a role in influencing this movement during the body rising phases. Due to the excessive body weight, it was difficult to control the balance and perform the designated movement. As obese individuals would consume more energy in the body raising stage, their joints would be subject to a much higher joint force in comparison to individuals who were healthily normal. This study included four obese participants; their average body mass index (BMI) was 31.2 kg/m2, while the average BMI for nonobese participants was 20.3 kg/m2.
Sitting cross-legged puts higher kinematic demands on the hip and knee joints for the flexion motion in the sagittal plane, as the results demonstrated that the ROMs of hip and knee flexion reached 101.7° and 131.9°, respectively. Followed by the hip abduction that reached 43.2°, the hip external rotation reached 36.4°. This activity exhibited low kinematic demand on the ankle; the ROMs of the ankle extension, adduction, and internal rotation were 20.2°, 28.3°, and 22.8° respectively, and the ROMs of the ankle flexion, abduction, and external rotation motion were within 12.3°. In the ascending phase, these joint angles gradually returned to normal standing levels as the activity continued. In the resting posture, the environmental supporting (usually floor or ground) force was acting on the body through the lateral side of shank and foot and restricted them from moving, so abduction and external rotation of the ankle and knee happened in a limited scale.
For this activity, studies for hip, knee, and ankle joints in three axial planes at the same time were much less. Only two studies to date have been conducted in India to focus on sitting cross-legged. Kapoor et al. 1 had done quite comprehensive research on this posture; however, the kinematics of knee and ankle in frontal and transverse planes were not given, resulting in the absence of the corresponding kinematic curves of the sitting cross-legged activity. Their data showed that mean flexion range at the hip joint was 91° (82°–100°); mean abduction range at the hip joint was 39° (19°–57°); mean external rotation range was 49° (42°–58°); mean flexion range at the knee was 135° (126°–142°); and mean equinus range at the ankle was 29° (17°–34°). Another comparable study was done by Hemmerich et al. using a six degree-of-freedom electromagnetic tracking system on 30 healthy Indian subjects; the data as they presented it were more comprehensive. 2 Our partial data varied from their results; the discrepancies can be attributed to differences in the physical characteristics of the population groups studied or variations in the method by which the activity was performed. 2 At the knee, the Chinese subjects’ mean maximum ROM of knee flexion was 131.9°, which was very close to the mean value 135° obtained by Kapoor et al. but significantly less than the mean value of 150° obtained by Hemmerich et al. At the hip, on the contrary, the Chinese subjects’ mean maximum ROM of hip flexion of 101.7° was slightly more than the mean value of 91° obtained by Kapoor et al. and significantly more than the mean value 83.5° obtained by Hemmerich et al. This result implied that the Chinese patients who underwent total hip arthroplasty (THA) may not be able to make such a posture, but the Chinese patients who underwent total knee arthroplasty (TKA) might be comparatively safe in this posture than the Indian patients.
By comparing the data in this study with the data reported on the ROM achieved following total joint arthroplasty, the ROM of joint arthroplasty was demonstrated rather poor. The motion requirements for hip and the ranges of flexion, abduction, and external rotation were all similarly high. In the sagittal plane, the maximum ROM of hip flexion was 101.7°, but the reported mean maximum ROM of flexion achieved after THA was merely 99.8° (SD = 15.3 years) with a range of 48°–121°.7,8 Out of a total of 240 trials (6 trials × 40 participants), participants exceeded 99.8° of flexion 176 times, which also proved that the flexion value for common sitting cross-legged activity was higher than the postoperative maximum ROM of flexion of THA. The measured maximum ROM of hip abduction was 43.2° in the frontal plane, and the ROM of hip external rotation was 36.4° in the transverse plane. However, mean ROMs of abduction and external rotation achieved after THA were 25.7° ± 7.7 and 24.9° ± 8.1, 8 so these two motions would have high impingement or dislocation risk, and patients who underwent THA would be inappropriate to perform this activity. At the knee, the measured maximum ROM of knee flexion was 131.9°, which obviously exceeded the mean ROM of flexion achieved following TKA that has been reported generally.9 –11 At the same time, the knee internal rotation reached the maximum value at −32.4°, which exceeded the postoperative mean ROM of knee internal rotation that has been reported.12,13 Therefore, this study indicated that patients who have undergone joint arthroplasty, assuming the sitting cross-legged position could be a problem to the joint. It is expected that the due attention should be raised to the manufacturers of the relative artificial joints or prosthetics. It is necessary to design a joint prosthesis with a higher ROM, in addition to improving surgical techniques for joint arthroplasty. In the future, joint arthroplasty should meet joint kinematic requirements and empower patients with better physical ability. The results of this study could be used for reference to design better joint prosthetics to meet various activity needs.
The knowledge of the kinematics of cross-legged sitting is useful when designing artificial joints. It is important, however, to achieve more ROM during rehabilitation, as the participants normally do not use their possible passive ROM (protecting the joints) and the hip implants are not guaranteed to perfectly align when implanted. For these two reasons, the possible ROM for artificial joints needs to be larger than what is being reported in this study. Kinematic data of a healthy population are valuable for the postoperative rehabilitation. Hip flexion, abduction, and external rotation as well as knee flexion and internal rotation during sitting cross-legged have a certain dislocation risk for the patient who underwent total joint arthroplasty; patients and medical care personnel must give attention to this problem. Although these facts are by now well known, no quantitative data are available on the kinematics at the joints in the three axial planes required for this activity of Chinese people. Thus, these data can be used as reference in the guiding doctors to determine a reasonable rehabilitation training program and to warn patients against performing this activity too early to avoid unnecessary physical harm.
Conclusion
This study investigated the functional ROM requirements of sitting cross-legged in a healthy Chinese population with respect to joint arthroplasty. This activity demands a greater ROM in hip flexion, abduction, and external rotation as well as knee flexion and abduction. It can be found that current joint arthroplasty is not appropriate for such activity. The data of the current study provided baseline information about the Chinese population to physicians and therapists concerned with the surgical and functional rehabilitation, as well as to help engineers engaged in prosthetics design establish the criteria for lower limb prosthetics to fit Chinese populations.
Footnotes
Conflict of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This work was supported by the National Natural Science Foundation of China [grant number 30810103908]; the Science Foundation of Shanghai [grant number 09441900300]; and the State Key Fundamental Research Program of China [grant number 2011CB711000].