
Abstract
Postoperative urinary retention necessitating catheterization after major lower limb arthroplasty surgery adds to the patients’ postoperative discomfort and increases the risk of urinary tract infection with potential risk of transient bacteraemia and seeding of infection to prosthetic joints. Preoperative evaluation of patients with lower urinary tract symptoms may help to identify at-risk patients and the International Prostate Symptoms Score (IPSS) has been used as a screening tool to quantify the severity of symptoms in males. A prospective cohort of 303 patients undergoing total hip or knee arthroplasty was evaluated using the IPSS. Patients were categorized into three symptom groups (mild, moderate and severe based on scores of 0–7, 8–18 and greater than 18, respectively) and four age groups (<50 years, 51–60 years, 61–70 years and greater than 70 years). Twenty-six patients (8.6%) developed urinary retention and were catheterized postoperatively; of these, 16 were male and 10 were female. Statistical analysis using logistic regression models showed significant association between severe IPSS scores (>18) and urinary retention requiring catheterization in both males and females with both high specificity and sensitivity in the test in predicting postoperative catheterization. Hence, this test is a valid preoperative screen in predicting postoperative catheterization.
Introduction
Postoperative urinary retention necessitating catheterization after major lower limb arthroplasty surgery is a common problem adding to the patients’ postoperative discomfort, increasing the risk of urinary tract infection, causing urinary stasis with the potential risk of transient bacteraemia resulting in the seeding of infection to prosthetic joints, delaying rehabilitation and potentially delaying discharge from hospital. 1 Various factors have been associated with urinary retention following arthroplasty with the most common being advanced age and male gender related to prostatism. This issue can be limited by identifying at-risk patients and considering catheterization in the perioperative setting. The International Prostate Symptoms Score (IPSS) is a widely accepted and used simple questionnaire to detect and quantify lower urinary tract symptoms of outflow obstruction in males.
We studied postoperative catheterization rates in patients undergoing elective total hip and knee replacements to verify the increased risk of male compared to female patients, verify that older patients have a higher risk than younger patients, investigate whether the operation type is a risk factor, and investigate the correlation between the IPSS and the incidence of requiring postoperative catheterization to assess the validity of using the IPSS as part of preassessment checklist in patients undergoing hip and knee joint replacements.
Materials and methods
Preoperative assessments and scoring of patients have been undertaken in all patients, as standard, in the first author’s institution since 2003; for this study, we analysed 303 consecutive patients admitted for total hip replacement (THR) or total knee replacement (TKR) over a 6-month period. All patients had routine preoperative assessment including urine analysis and, as per hospital protocol, patients with significant and symptomatic bacteriuria (1 × 105 ml−1) were treated preoperatively by appropriate antibiotics with surgery delayed until they were microbiologically clear of infection. At admission, all patients were asked to complete the IPSS questionnaire which contained seven questions related to urinary symptoms in the preceding month. Each question carries a score between zero and five depending on the severity of symptoms as detailed in Table 1. The total score was calculated by summation of the scores from the seven questions with a minimum score of 0 and a maximum of 35. Patients were then categorized into three symptom groups based on IPSS categories of mild, moderate and severe with scores of 0–7, 8–18 and greater than 18, respectively. They were also divided into four age groups of less than 50 years, 51–60 years, 61–70 years and greater than 70 years of age. All patients were monitored postoperatively until discharge, for voiding of urine and those who developed retention with the inability to void urine despite the sensation of bladder fullness and discomfort were catheterized per urethra under aseptic precautions and gentamicin (80 µg intramuscular) cover. The timing of development of retention was recorded. Clean catch/midstream urine sample at catheterization was sent for microbiological analysis. As per hospital protocol, the catheter was removed, at the appropriate time, after the patient successfully completed the trial of overnight clamping and sensation of bladder fullness (trial with occlusion of catheter). All catheterized patients were referred formally for further urological assessments as outpatients. The data were assessed with regard to patients’ age, sex, type of surgery, IPSS score, time when retention developed, whether they required catheterization and any complications due to catheterization.
IPSS questionnaire.

IPSS: International Prostate Symptoms Score.
Statistical analysis was undertaken in R Statistical Software Version 3.2. Exact logistic regression models were used to account for the scarcity of the data and the multiple covariates. Hence, our conclusion was based upon the estimated odds ratio of the regression models.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors. Ethical approval for the database containing patient data obtained locally through the Liverpool Research Trials Centre (refs. 1893 and 2060); early data were held on a database in Scotland requiring ethical approval through the Multi-Centre Research Ethics Committee for Scotland (ref. MREC/04/10/004), who felt this was audit data and did not require a formal review of the ethics committee.
Informed consent
The individual participants in this study gave consent for their data to be reviewed for scientific assessment.
Results
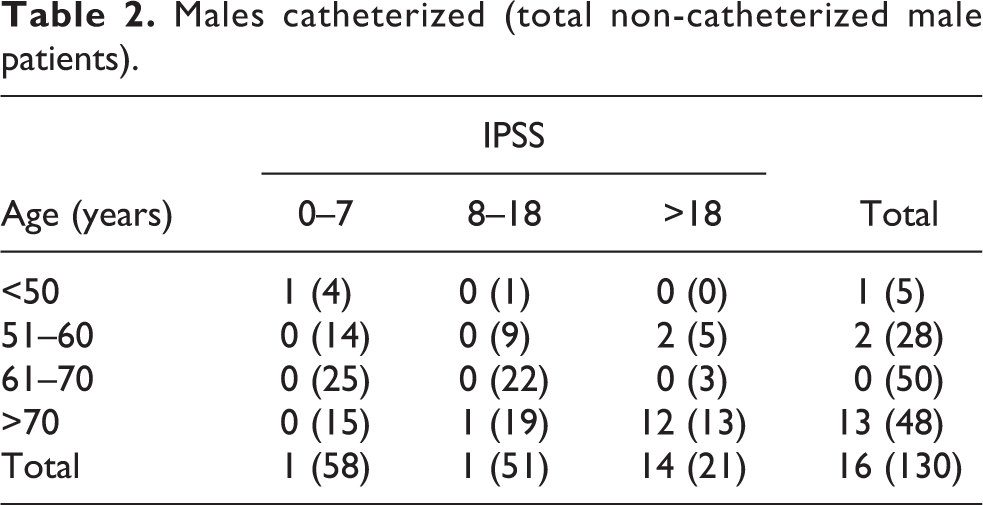
There were a total of 303 patients, of which 173 were female (92 THR and 81 TKR) and 130 were male (60 THR and 70 TKR). One female patient, having a hip replacement, was excluded due to incomplete data. A total of 26 patients developed urinary retention and were catheterized postoperatively (8.6%), of which 16 were male (12.3% of all males) and 10 were female (5.8% of all females). Twenty patients (13 male and 7 female) were catheterized within the first 24 h of operation and six patients (3 male and 3 female) needed catheterization, after initially voiding small amounts, but developing retention 24 h postoperatively. The average IPSS for males and females in non-catheterized patients were 8.4 and 9.1, respectively, whereas in catheterized patients were 21.8 and 20.0, respectively. The age distribution, IPSS categories of patients and raw data are as shown in Tables 2 and 3. Among males requiring catheterization, 14 of 16 (87.5%) had an IPSS >18 and 12 of 16 (75%) were both over 70 years and with an IPSS >18 (Table 2). Nine of 10 (90%) catheterized females had an IPSS >18 and 5 of 10 were both over 70 years and with an IPSS >18 (Table 3). There were no complications related to insertion or removal of the catheter. None of the patients needed recatheterization by the time of discharge.
Males catheterized (total non-catheterized male patients).
Females catheterized (total non-catheterized female patients).

1. Male versus female odds of requiring catheterization
In males, the odds of requiring postoperative catheterization are 2.27 times larger than in females, with a standard error of 0.96, and with a p value of 0.051 this is just outside statistical significance.
2. Odds of requiring catheterization between age groups
Table 4 presents that the odds of requiring catheterization for patients less than 50 years are not significantly different than the odds for any other age group. However, since older patients are those who are commonly perceived to be higher risk, these were recategorized into those under and over 70 years of age. When this was analysed, Table 5 presents that in patients over 70 years of age, the odds of requiring catheterization are 3.34 times larger than those under 70 years of age, which is highly significant.
Odds of requiring catheterization between age groups comparing to reference group of under 50 years.

Odds of requiring catheterization comparing between age groups greater and less than 70 years.

3. Odds of requiring catheterization between hip and knee replacements
There is no significant difference between either hip or knee replacement and the risk of catheterization, with an odds ratio of 0.616 and a p value of 0.243.
4. Odds of requiring catheterization between IPSS groups
Table 6 presents that for a patient in the severe group (IPSS > 18), the odds of requiring catheterization are 71.2 times larger than the odds for the mild group (IPSS <8), which is highly significant; however, there is no significant difference between patients in the mild and moderate groups (IPSS <8 and IPSS 8–18). Hence, these groups were recategorized into severe and non-severe groups depending on whether the IPSS was greater or less than 18.
Odds of requiring catheterization between IPSS groups comparing with reference group of ‘mild’ symptoms.

IPSS: International Prostate Symptoms Score.
Table 7 presents that for a patient in the severe group (IPSS >18), the odds of requiring catheterization are 93.1 times larger than the odds for patient in non-severe group (IPSS <18). This is highly significant, but the confidence interval is very wide due to the high concentration of catheterized patients into the severe group, with a small number of patients relative to the total number (44 in 302). Hence, if some classification error has occurred by chance, then the odds ratio could be as small as 25.8 (still large and highly significant difference between groups) or as large as 335.7.
Odds of requiring catheterization between severe and non-severe IPSS groups.

IPSS: International Prostate Symptoms Score.
5. Analysing IPSS model subgroups
A series of logistic regression models and Bayesian information criterion (BIC) were used to determine the optimum model of combination of predictors for those patients who would require postoperative catheterization. The severe and non-severe versions of the IPSS score gave the best predictor value, as they gave the lowest BIC score, with a sensitivity of 88.5% and a specificity of 92.4%. Although age was confirmed as a significant contributing factor in the univariate analysis (Table 5), its predictive value was limited in the presence of IPSS score due to low sensitivity and specificity in female patients.
6. Analysing IPSS test regards to gender specificity
The IPSS is by definition a prostatic test, but analysing the severe and non-severe versions of the IPSS gave a sensitivity and specificity in females of 90.0% (9 of 10) and 91.3% (148 of 162), respectively, and in males of 87.5% (14 of 16) and 93.8% (107 of 114), respectively; hence, the test is equally as accurate in predicting postoperative catheterization in males and females.
Discussion
While urinary retention and subsequent catheterization have a number of potential complications and adverse outcomes, the most important is the potential risk of transient bacteraemia leading to infection of prosthetic joints. 1 –3 Infection, be it from intraoperative contamination, haematogenous spread from distant foci or bacteraemia following urinary retention and subsequent catheterization, is a significant complication with increased morbidity and mortality to the patient and significant financial burden to the health care system of the society. 3 –5 The risk of infection in hip and knee arthroplasty is generally accepted to be less than 1% but rises to 6.2% in those catheterized post-urinary retention. 1,3 The requirement for postoperative catherization has a wide range in the medical literature from under 5% to over 40%. 1,6,7,8,9 Our results were in line with this wide risk range.
A number of factors have been implicated in the causation of postoperative urinary retention following lower limb arthroplasty including advanced age, male gender, opioid analgesia, previous history of lower urinary tract obstruction (benign prostatic hyperplasia) and spinal/epidural anaesthesia. 6,7,10,11,12 Among these, advanced age and male gender have been found to be the most common, which indirectly point to symptoms related to prostatism. Although there is published evidence linking deep prosthetic infection with postoperative urinary tract infection, there are currently no widely accepted guidelines relating to prediction of bladder infections and subsequent deep sepsis following total joint arthroplasty and indeed, Ritter et al. in their study showed no correlation between preoperative or perioperative urinary tract pathology and postoperative joint infections. 1,3,13,14
The IPSS was developed by American Urological Association to assess the severity of prostatism and help in evaluation of patients with bladder outlet obstruction. 15 The scoring system consists of questions which help to quantify the severity of obstructive symptoms of the bladder neck and detrusor instability. It has been widely used and found to be a useful tool in prostatic surgery as a screening tool and also to evaluate outcome after treatment. Other studies have used this scoring system to identify at-risk groups and evaluate pre- and post-surgical treatment of female patients with bladder outlet obstruction and have concluded that it is not specific for benign prostatic hypertrophy. 16 It has also been found to be useful as a ‘bothersomeness’ index but has no correlation with objective urodynamic parameters in women with bladder outlet obstruction. 17,18 Madersbacher et al. used the IPSS in their study to determine the urodynamic basis for the observation that ageing women report comparable benign prostatic hyperplasia symptom scores as age-matched men. 19 The mean IPSS was 15.7 for men and 13.0 for women (p = 0.02). The urodynamics-based comparison, however, failed to give an explanation for these similar scores. The conclusion was that other mechanisms such as changes in diurnal urine production, structural alterations of the ageing detrusor, endocrine disturbances affecting lower urinary tract function, and subtle urodynamic changes are responsible.
The use of IPSS as a preoperative evaluation tool in male patients undergoing lower limb arthroplasty in previous studies have come to similar conclusions about a strong correlation between high IPSS score and risk of postoperative urinary retention and have recommended it as a simple, quick and easy-to-use screening adjunct. 7,20 Sarasin published a prospective study in 182 male and female patients undergoing lower limb arthroplasty under spinal anaesthesia and found that although IPSS scores do show a tendency to be higher in patients requiring catheterization postoperatively, this correlation was not statistically significant. 21 The only statistically significant factors predictive of the development of urinary retention in this study were male gender and age. It was suggested that IPSS score is not useful in the accurate prediction of those patients who are likely to develop postoperative retention and, as a result, require catheterization.
This study has shown that by undertaking a comprehensive statistical analysis of the use of IPSS in predicting the requirement for postoperative catheterization, we can prove a number of widely held assumptions. Patients over 70 years of age have a significantly higher risk of postoperative catheterization than those under 70 years, as are those who have severe symptoms, defined as a score greater than 18. The latter holds equally true for both males and females with both groups having a very high sensitivity and specificity, hence confirming that the scoring system is both highly predictive and an easy tool to use in the preoperative setting. The routine practice for hip and knee arthroplasty in our, and many other, institutes is spinal/epidural anaesthesia unless there are any contraindications. The majority of the patients are controlled with patient-controlled analgesia pumps for 24 h postoperatively. All patients are screened in the preoperative assessment clinic using the IPSS questionnaire, with those scoring over 18 or being over 70 reassessed for consideration for perioperative catheterization or referral to the urologists prior to admission for arthroplasty surgery.
This study has limitations in that we have not assessed the influence of type of anaesthesia and postoperative analgesia, in particularly opioid use; however, the notion of spinal anaesthesia predisposing to urinary retention has been challenged in various studies. 8,9 This may be a basis for further studies. Previous history of urinary retention related to bladder outlet obstruction may have affected the risk of retention in our study population, but these patients would be expected to have a high IPSS score.
Hence, using this simple easy-to-use questionnaire as a preoperative screening tool seems to make a very good practical sense for identifying patients at risk of postoperative urinary retention and hence allows us to identify a group that should be considered for perioperative catheterization to minimize postoperative infection. In addition, this test is non-gender specific, hence preventing the requirement for different tests for males and females. Individual departments may consider restricting the use of the IPSS questionnaire to those over 70 years, for time and cost reasons, as this is by far the highest risk group.
Conclusion
The results have shown that the IPSS scoring system is an easy-to-use, highly sensitive and highly specific, but non-gender specific tool in the accurate prediction of postoperative catheterization in patients undergoing elective TKR and THR. Once identified, these patients could then be counselled regarding the risks of postoperative retention, need for preoperative catheterization in a sterile environment or referred for further urological assessment and management before proceeding with arthroplasty, thereby potentially preventing potential complications and improving the standard of quality of care provided.
Footnotes
Acknowledgements
The authors would like to thank Richard Jackson of the Liverpool Cancer Trials Unit at The University of Liverpool for his help with statistical advice.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors declare they had no conflicts of interest at the time the data were collected and analysed but subsequently Smith & Nephew have financed at knee fellow at The Royal Liverpool & Broadgreen University Hospitals. Mr Santini has received speaker honorarium from Smith & Nephew.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.