
Abstract
Background:
Amputations affect both the physical and the psychological aspects of an individual, causing significant impact on self-esteem. The main causes of finger amputations are work-related accidents with dangerous machinery, road traffic accidents, and animal bites, as well as systemic diseases such as diabetes. This report aims to describe a simple technique for fabrication of implant-retained finger prosthesis with a modified base of the retention system.
Case Description and Methods:
The O-Ring retention system was used with a modified hexagon-shaped base and a metallic capsule adapted to the acrylic resin to attach the prosthesis to the implant.
Findings and Outcomes:
The prosthesis was made with silicone, and after osseointegration, it was installed without complications, leading to a patient satisfied with the end result and encouraged to return to social life.
Clinical relevance
Restoring self-esteem in the patient and static and functional rehabilitation.
Background
Amputations affect the physical and psychological aspect of an individual, causing significant impact on self-esteem, often leading to depression and social isolation, as would any other deformity on the human body.1,2 Moreover, traumatic amputation of a finger seriously compromises hand function, as well as its aesthetics.3,4
The most common causes of finger amputation include work-related accidents with dangerous machinery, road traffic accidents, and animal bites, 4 as well as systemic diseases such as diabetes.
Nowadays, many finger amputations can be replanted through microsurgery. However, attempting reconstruction is not advisable in some cases due to possible lack of success. 1
Therefore, the aim of this report is to describe a simple technique for fabrication of a finger prosthesis implanted with a modified hexagon-shaped base of the retention system, which was applied in a patient who suffered a finger amputation.
Case description and methods
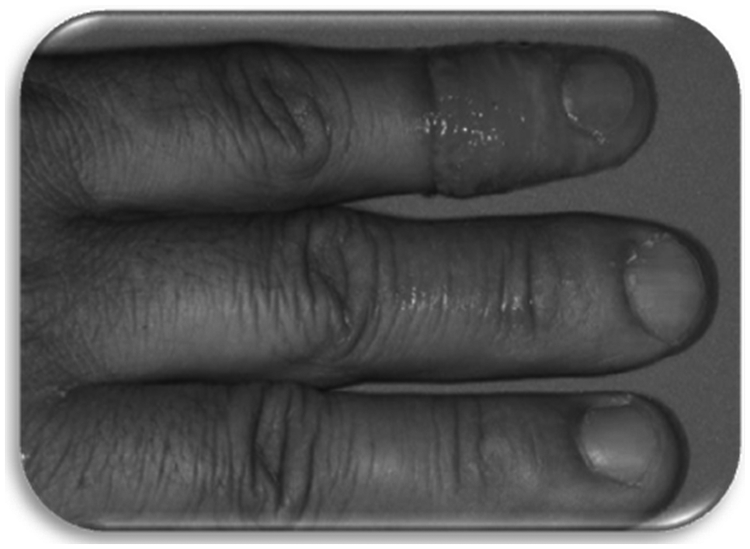
A 56-year-old male patient was admitted to the clinic after sustaining a traumatic amputation of the index finger of the right hand in an accident at work. The patient complained of decreased motor capacity and low self-esteem, which led to decreased social interaction. The patient agreed and signed with the treatment to be performed.
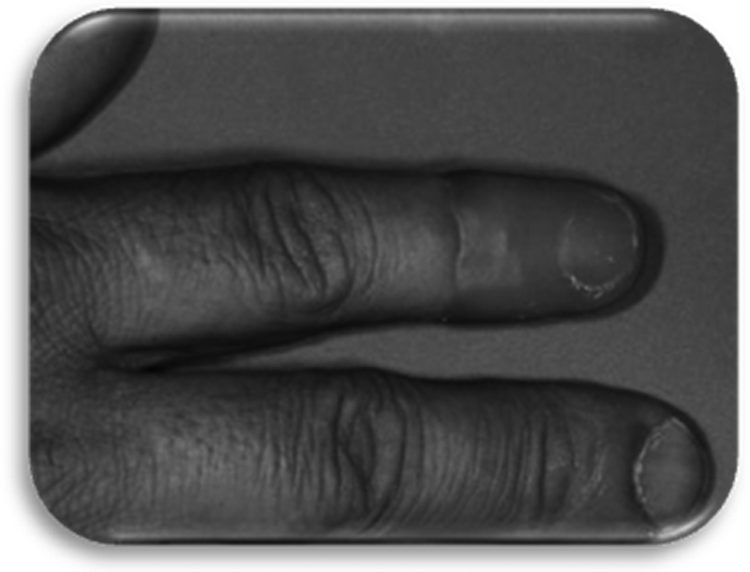
Following clinical (Figure 1) and radiographic examination of the reminiscent stump, a treatment proposal was elaborated. For insertion of the implant, its width and length were determined through radiographic evaluation. 5 An intraosseous (IO) implant measuring 3.75 mm in diameter and 10.0 mm in length (Sin, São Paulo, Brazil) was inserted into the proximal phalanx of the index finger 6 (Figures 2 and 3).
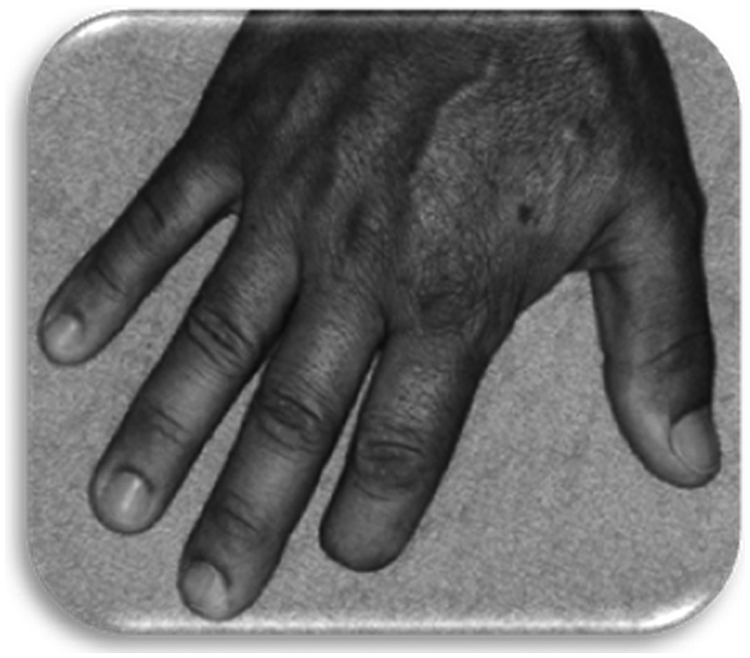
Remaining stump of the right hand.

Surgical phase.

Radiographic evaluation of the dental implant.
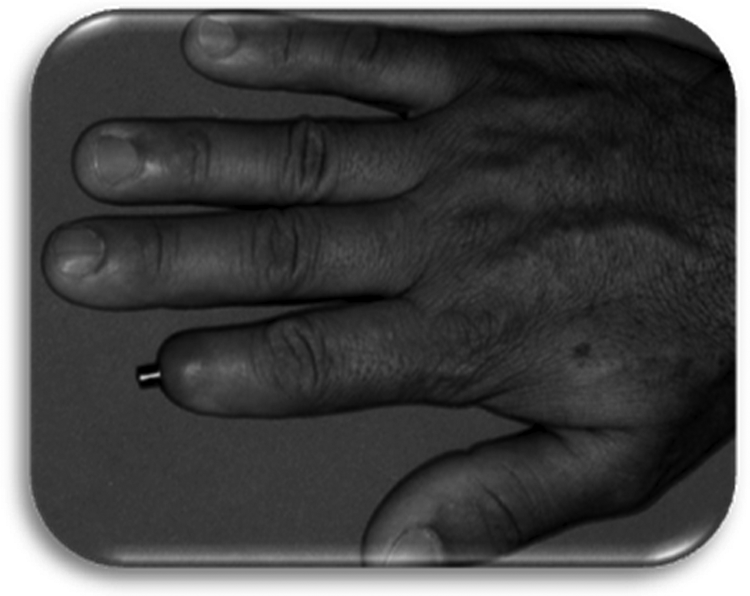
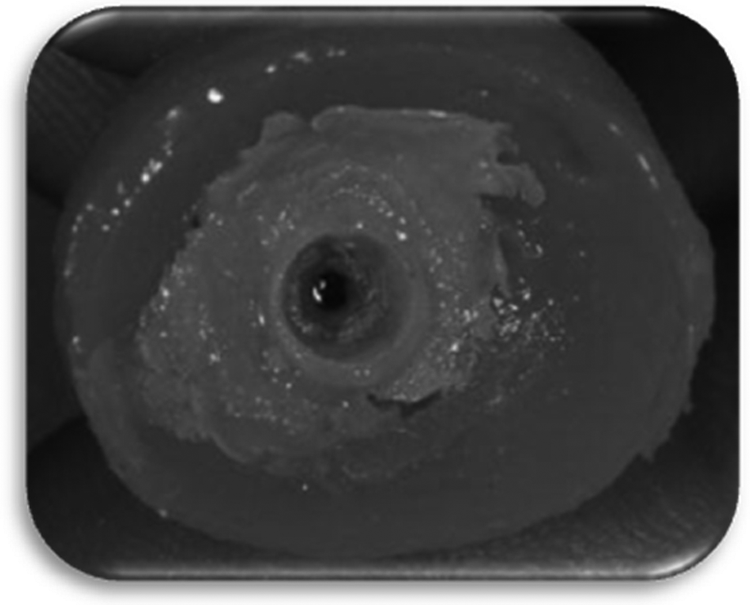
Osseointegration was achieved after 3 months, which was confirmed by radiographic evaluation (Figure 3). A ball–capsule type attachment system was adapted to the implant, denominated O-Ring. The O-Ring system suffered a modification, creating a hexagon-shaped base (Figures 4 and 5). The molding was made using Hydrogum alginate (Zhermack, Rovigo, Italy). Reproduction of the left hand (Figure 6) was taken and reproduced in wax to obtain an impression of the left index finger. From this wax mold, modifications were made to obtain an index finger for the right hand. Following this procedure, a metallic capsule was embedded into the O-Ring (Figure 7), and acrylic resin was added around it to adapt the prosthesis to the implant (Figures 8 and 9).
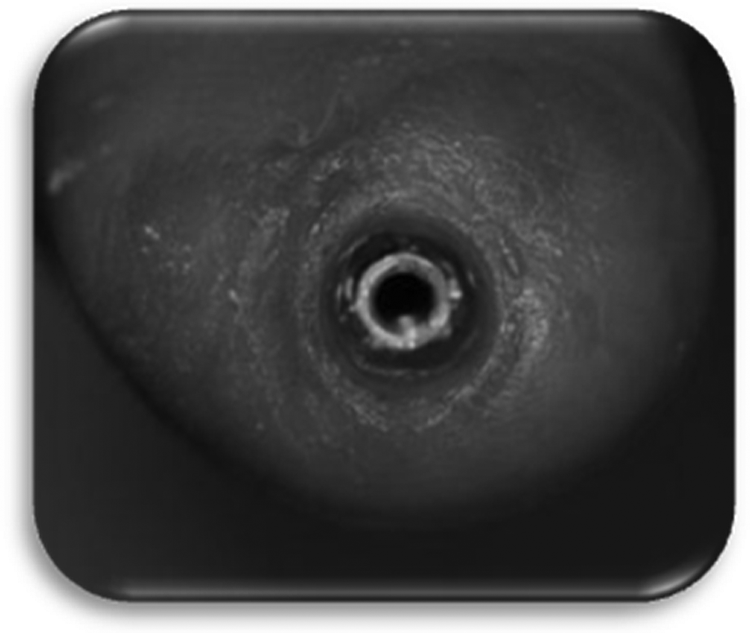
Finger implant.
Finger implant (healer).

Left hand of patient.

Restraint O-Ring.

Wax model adaptation for the resin.
Resin adapted to implant.
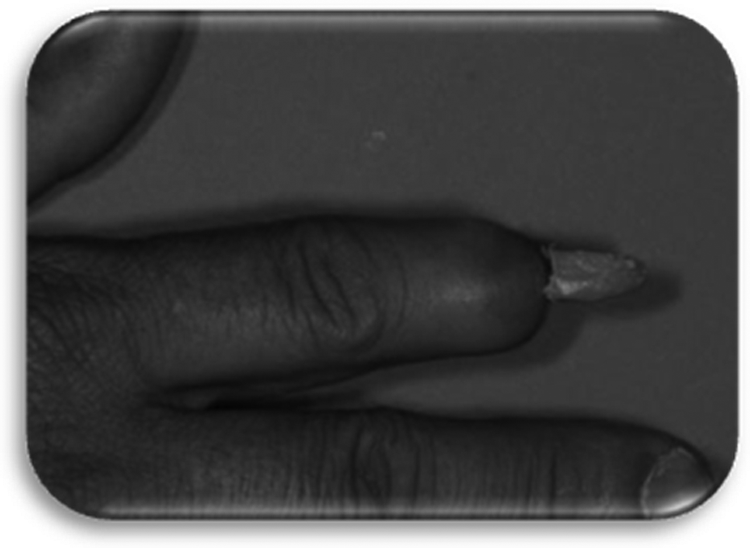
Anatomic details were verified to improve aesthetic results. A retention test between the thumb and finger was carried out (Figure 10). Following this test, retentions were made in the resin–capsule structure (Figure 11), which was enclosed in a flask with type III stone plaster and the wax pattern. Afterward, the wax was removed, and the structure was cleaned with acetone. Layers of primer (Sofreliner Prime; Tokuyama Corp., Taitou-ku, Tokyo, Japan) were applied to improve adhesion of the resin–capsule structure to the Silastic-MDX 44210 silicone (Dow Corning Corporation, Midland, MI, USA). As observed in some studies, the primer provides greater resistance to the adhesion between the silicone and the resin.7,8 The mold was filled with silicone and intrinsic colors to manufacture the prosthesis. In addition, extrinsic colors were applied to some areas of the prosthesis to correspond with complementary colors 4 (Figure 12).
Wax pattern tried on the patient.

Resin adapted to restraint (O-Ring).
Silicone-set resin–capsule.
The prosthesis was installed, and the patient was instructed about its care and maintenance. Cleaning was instructed to be carried out with a soft brush and irrigated with lukewarm water and soap.4,5,9 In order to prevent complications, postoperative care is necessary, such as maintenance of hygiene with water and soap and soft tooth brush, and medication with anti-inflammatory and antibiotic drugs. Moreover, the long-term success of the treatment with extraoral implants depends upon peri-implant maintenance, as infection and inflammation may lead to loss of the implant and failure of the prostheses. 10
Findings and outcome
After 6 months, follow-up maintenance of the retention system and skin were carried out, as well as assessment of the aesthetics and dynamic capacity (Figure 13).
Finger prosthesis installed (end result).
Discussion
Several materials and techniques were developed to be used in the process of prosthetic rehabilitation, such as resin and silicone, which present some advantages and disadvantages; nevertheless, they are still the most frequently used.3,4
The sculpture technique, or analogous finger technique, is done by molding and sculpturing the finger from another individual. Alternatively, it can be performed based on anatomical reproduction.11,12
Retention is the main determinant factor for the success of prosthetic restoration of any part of the body. It is essential for the aesthetic attribute, functionality, and comfort, thus enhancing the quality of life of the patient. 13 Acrylic resin prostheses were made and connected to the pillars using a hexagonal magnetic superstructure system. 4
In the present case, the O-Ring system was indicated due to its practicality, as it does not require the melting phase done in the laboratory, and low cost. The modified hexagon-shaped base of the retention system provided an antirotational mechanism, improving adaptation of the prosthesis to the finger, thus preventing discomfort during activities.4,5
The prosthesis was made with silicone, which contributed to an enhanced aesthetic result. It was observed that the patient could carry out his routine activities in a satisfactory manner.
Clinically, the adhesion between the resin and silicone is not completely secure. The silicone may tear or separate when removal of the prosthesis is attempted by the patient, in cases where resin adhesives are not used. 14
In implant-retained prosthesis, the most critical area concerning hygiene is around the pillars, which are projected through the skin. In this region, it is common to observe dry accumulation of debris, keratin, and epithelium, and if cleaned incorrectly, may lead to tissue inflammation.9,15
The cleaning procedures must be performed daily, preferably at night before sleep. The first step is to wet the area with a mixture of water and hydrogen peroxide, or water and neutral soap, to soften any dry debris. Subsequently, a cotton swab, brush, or a rubber point can be used to clean the area adjacent to the abutment skin and bar, taking care not to traumatize the tissue.9,16
Even though patients frequently require better reconstruction of the hand in cases of injury or amputation, prostheses only recover basic functions of the hand.
Conclusion
Maintenance and hygiene of the prosthesis certainly contributes to the longevity of the treatment. In order for this to occur, the patient must be correctly instructed and particularly motivated. Also, the role of the prosthetist is to rehabilitate, as well as to instruct. Rehabilitation of a digital loss with implant-retained prosthesis may present some motor limitation. However, employing a practical, simple, and low-cost retention system, such as the O-Ring with the modified base, may improve the quality of life and social interaction of the patient.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.