
Abstract
Background:
Unstable shoes, which have recently become popular, claim to provide additional physiological and biomechanical advantages to people who wear them. Alterations in postural stability have been shown when using the shoe after training. However, the immediate effect on muscle activity when walking in unstable shoes for the first time has not been investigated.
Objective:
To evaluate muscle activity and temporal parameters of gait when wearing Masai Barefoot Technology shoes® for the first time compared to the subject’s own regular trainer shoes.
Study Design:
A pilot repeated-measures quasi control trial.
Method:
Electromyographic measurements of lower leg muscles (soleus, medial gastrocnemius, lateral gastrocnemius, tibialis anterior, peroneus longus, rectus femoris, biceps femoris and gluteus medius) were measured in 15 healthy participants using Masai Barefoot Technology shoes and trainer shoes over a 10-m walkway. Muscle activity of the third and sixth steps was used to study the difference in behaviour of the muscles under the two shoe conditions. Temporal parameters were captured with footswitches to highlight heel strike, heel lift and toe off. Paired samples t-test was completed to compare mean muscle activity for Masai Barefoot Technology and trainer shoes.
Results:
Indicated that the use of Masai Barefoot Technology shoes increased the intensity of the magnitude of muscle activity. While this increase in the activity was not significant across the subjects, there were inter-individual differences in muscle activity. This variance between the participants demonstrates that some subjects do alter muscle behaviour while wearing such shoes.
Conclusion:
A more rigorous and specific assessment is required when advising patients to purchase the Masai Barefoot Technology shoe. Not all subjects respond positively to using unstable shoes, and the point in time when muscle behaviour can change is variable.
Clinical relevance
Use of Masai Barefoot Technology shoe in patient management should be monitored closely as the individual muscle changes and the point in time when changes occur vary between subjects, and evaluation of how a subject responds is not yet clear.
Introduction
Over the past decade, a new market has opened into developing footwear that claims to provide the user with a body workout while walking in specifically designed shoe. An irregular and unstable sole is thought to change the interaction between the foot and the ground. On wearing such shoes, these changes have been hypothesised to alter muscle function and contraction, making the lower limb muscles work harder. However, it is not clear from the research carried out so far what the specific effects of wearing unstable shoes have on lower limb muscle activity and contraction timing while walking.
The unstable shoe concept was originally launched with the Masai Barefoot Technology (MBT) shoe® that has a curved outer sole in the anterior–posterior direction and a dual-density heel profile. Research, to date, has primarily focused on the trained effects of the MBT shoe over a period of time on posture and muscle activity in stance.1 –4 After a trained period of using the MBT shoe, there have been observed alterations in standing with anterior and posterior sway increasing suggesting that the shoe has an impact on stability and balance.1,5
The effect of the MBT shoe while standing on external foot muscles was investigated after a 6-week adaptation period, using an electromyographic (EMG) circumferential linear array with magnetic resonance imaging (MRI) scanning. The activity of the soleus (SOL) muscle remained unchanged when wearing the shoe, yet there was increased activity in the anterior leg compartment and peroneal muscle group, suggesting that these muscles are recruited as a method to improve stability. 6 Although this increase in muscle activity when standing in unstable shoes may be beneficial to some users, the full impact of wearing the MBT shoe while walking still remains unclear.
Improved postural stability, while walking, has been indicated in other unstable shoes such as the Reflex Control shoe. 4 This shoe was used over a 6-week intervention programme and was found to improve posture and balance when compared to the MBT shoe. Furthermore, the instability of this shoe differs to that of the MBT shoe with the mode of instability being along the longitudinal axis of the foot. Although this study introduced a dynamic component to postural stability with a moveable plate, the testing did not include gait trials, and therefore, the results should be used with caution when discussing the effects of unstable shoes on gait.
Analysis of gait in subjects who had been trained for walking in MBT shoes for a 4-week period were found to have a smaller step length and altered ankle range of motion with increased amount of dorsiflexion. 2 This altered range of motion has also been highlighted when testing MBT sandals. Subtalar and ankle sagittal plane motions increased when wearing the sandal compared to barefoot trials. 7
More recently, it has been suggested that there is a great variability between subjects when studying the effects of walking in MBT shoes with outcomes being subject dependent. 3 Again, subjects were given a period of time to become accustomed to using the shoe, and testing occurred after a training period. The changes that were observed between subjects have been linked to different strategies of compensation being employed by the individuals wearing the shoe.1,8 Different strategies have also been adopted between various subject groups. When studying the changes between female and male subjects who were trained in using the MBT shoe, it was found that female users had greater anterior–posterior excursion of centre of pressure than males and altered control around the ankle joint. 5 However, the effects while walking after a period of training in the shoe appear to be varied and subject dependent. There is limited research to indicate exactly when habituation occurs and whether those subjects who have increased muscle activity adapted immediately or over a period of time.
Previous studies have focused on the effects of the shoes after a period of training or adaptation and are unable to make specific recommendation with respect to the usefulness of the MBT shoe while walking. The immediate effect of wearing the MBT shoe has recently been investigated, yet the subjects were allowed to become habituated prior to data collection. 9 If the MBT shoe is to be considered as a rehabilitation or training device, it is not clear from previous work as to how quickly muscle habituation occurs. This is important to distinguish how to use the MBT shoe in a clinical situation as a treatment modality as impact on patient rehabilitation needs to be considered.
The aim of this study, therefore, is to identify whether the activity of eight lower limb muscles alter while walking in the MBT shoe for the first time without any habituation period. This will test the hypothesis that a change in muscle activity while wearing the MBT shoes will occur immediately. The secondary objective of this study is to evaluate temporal parameters of gait between a regular trainer shoe and an MBT shoe during walking.
Method
Design
A quasi-experimental study with two repeated measures, where each subject acted as their own control. Ethical approval was sought and given by the University Ethics Committee, and all subjects provided a written informed consent.
Inclusion criteria
Subjects were recruited from a convenience sample of healthy student population who were able to stand on one leg and rise on to the toes without falling and have no musculoskeletal injury or pathology. All subjects had not worn the MBT shoe prior to testing.
Exclusion criteria
Subjects were excluded if they were unable to stand on one leg, had used the MBT shoe previously and were currently injured or had an injury within the last 6 months.
Outcome measures
The following outcome measures were reordered: number of steps taken in each shoe condition, mean EMG activity for each muscle, percentage change in muscle activity and time at which heel strike, heel lift and toe off occurred between the control and MBT shoes.
Study protocol
In total, 20 volunteers (male, n = 12; female, n = 8) with a mean age of 26 years (standard deviation (SD) = ±5.62 years), mean height of 170 cm (SD = ±7.11 cm), mean weight of 69.8 kg (SD = ±10.5 kg) and a Foot Posture Index (version 6) range between +2 and +12 consented to partake in the project.
Subjects’ own training shoe was used as a control measure, which was weighed; the MBT shoes used in this study weighed 1.3 kg. Test leg allocation was randomly assigned with the subject choosing an envelope stating which leg was to be tested. EMG electrode placement was defined using the surface EMG for non-invasive assessment of muscles (SENIAM) guidelines. 10 Accurate placement was made with musculoskeletal ultrasound (MyLab; Esaote, Genoa, Italy) and functional muscle testing, 11 which allowed reporting of reliable and valid data. Bipolar electrodes were placed directly on to the skin that had been prepared with an alcohol wipe. The following muscles were selected for investigation based on previous studies that had investigated EMG muscle activity, and additional muscles were included, which are known to be involved in key stages of gait that had not been previously studied.
SOL
Medial gastrocnemius (MG)
Lateral gastrocnemius (LG)
Tibialis anterior (TA)
Peroneus longus (PL)
Rectus femoris (RF)
Biceps femoris (BF)
Gluteus medius (GMed)
A footswitch was used to identify heel strike, heel lift and toe off, sensors were placed on the plantar posterior aspect of the calcaneus (sensor 1), the plantar aspect of the first met head (sensor 2) and also the plantar aspect of the apex of the first digit (sensor 3). The subject then replaced the sock over the sensors. Testing commenced with the subject walking in the trainer shoes along a 10-m walkway at a self-selected pace. The subject then placed the MBT shoes on and immediately walked again along the 10-m walkway.
Data processing and analysis
The number of steps taken over the 10-m walkway was identified from the EMG data. For data analysis, two steps were analysed as a representation of activity (the third and the sixth step) for each condition. These middle steps were selected to remove the acceleration and deceleration seen at the beginning and end of the walkway. Data collected from the EMG, sampled at 2048 Hz, of the eight muscles were notch filtered and rectified prior to passing through a 10-Hz eighth-order Butterworth filter. These data along with footswitch data were processed offline in a custom-developed program in MathCAD (Version 15; PTC, Needham, MA, USA). The footswitch data were used to identify key phases of the gait cycle, heel strike, heel off and toe off. The mean and maximum values were obtained for each muscle during a full gait cycle (defined as heel strike to heel strike). The mean EMG value was then calculated as a percentage value of the maximum EMG value recorded in the analysed trials.
As data met parametric assumptions, a paired samples t-test for mean EMG activity was used to identify differences between the control shoe and the unstable MBT shoe for each muscle (significant at p > 0.05). Additionally, differences between time at which heel strike, heel off and toe off occurred were also compared using a paired samples t-test.
Results
From the 20 subjects recruited, 5 were excluded due to inconsistencies with EMG data collection and outliers, therefore n = 15 (age = 25.2 years, SD = ±5.2 years; height = 168.36 cm, SD = ±6.7 cm; weight = 66 kg, SD = ±10.6 kg; control shoe weight range between 0.3 and 0.8 kg; right: left leg measured = 10 : 5).
Steps taken
The average number of steps taken in the control shoe is 9 (SD = 0.89), and in the MBT shoe, it is 8.69 (SD = 0.87). The distribution of this change included four subjects taking more steps while wearing the MBT shoe, eight subjects taking less steps and four subjects not altering the steps taken.
Mean EMG
Mean activity between the trainer shoe and MBT shoe increased in SOL, MG, PL, RF and GMed. Activity in LG stayed the same, and overall activities of TA and BF decreased. Paired t-test, however, showed no significant differences for these recorded values (p > 0.05) (Table 1).
Mean, maximum EMG (mV) and percentage values for each muscle for each condition. Paired t-test shows significance at p value.
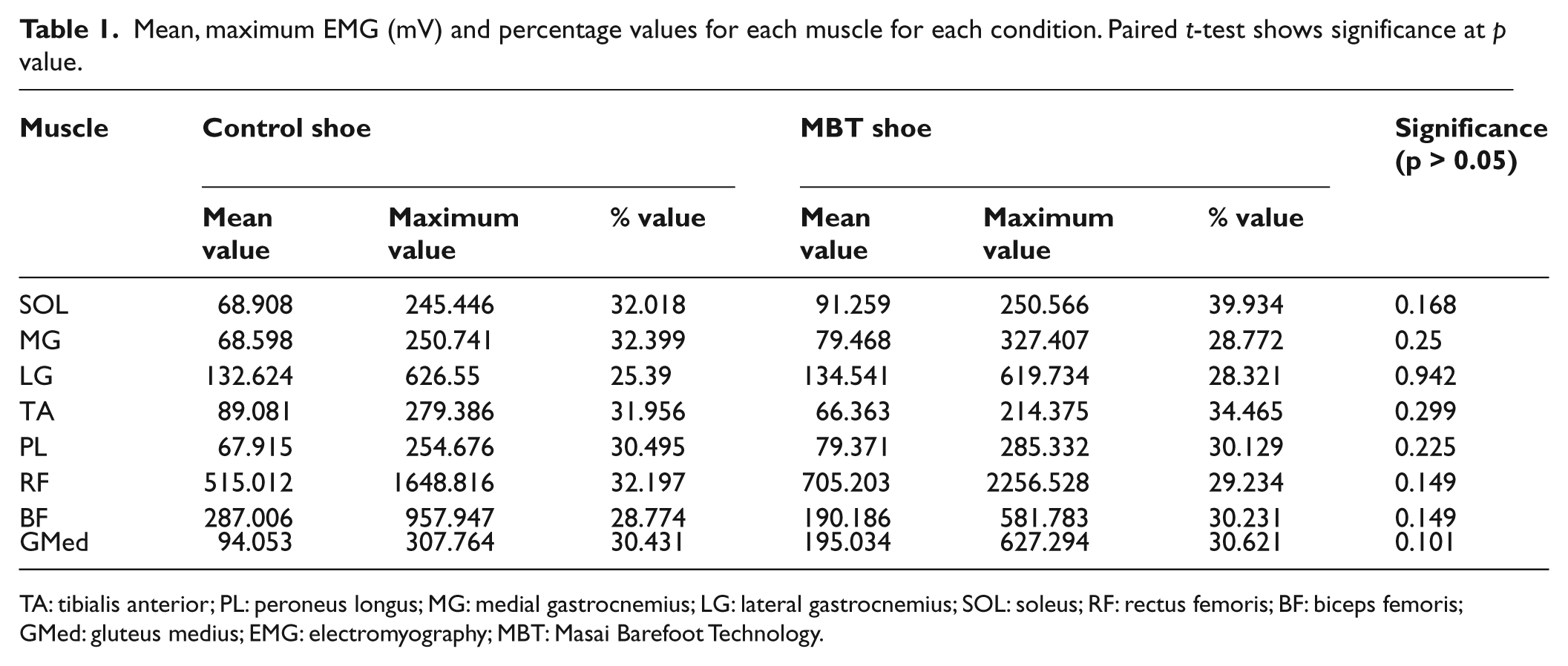
TA: tibialis anterior; PL: peroneus longus; MG: medial gastrocnemius; LG: lateral gastrocnemius; SOL: soleus; RF: rectus femoris; BF: biceps femoris; GMed: gluteus medius; EMG: electromyography; MBT: Masai Barefoot Technology.
Across all the muscles tested, there were an observed group of subjects that had no alteration in the EMG activity between the control shoe and the MBT shoe. Similarly, there was also a group of subjects that had more EMG activity while wearing the trainer shoes. Figure 1(a) to (h) shows scatter plots for the mean activity of each muscle tested for each subject (n = 15). Demonstrating an inconstant variability in responses between the trainer shoe and MBT shoe conditions. It can be seen from these graphs that some subjects had increased activity while walking in the MBT shoe and others had no change or reduced activity.
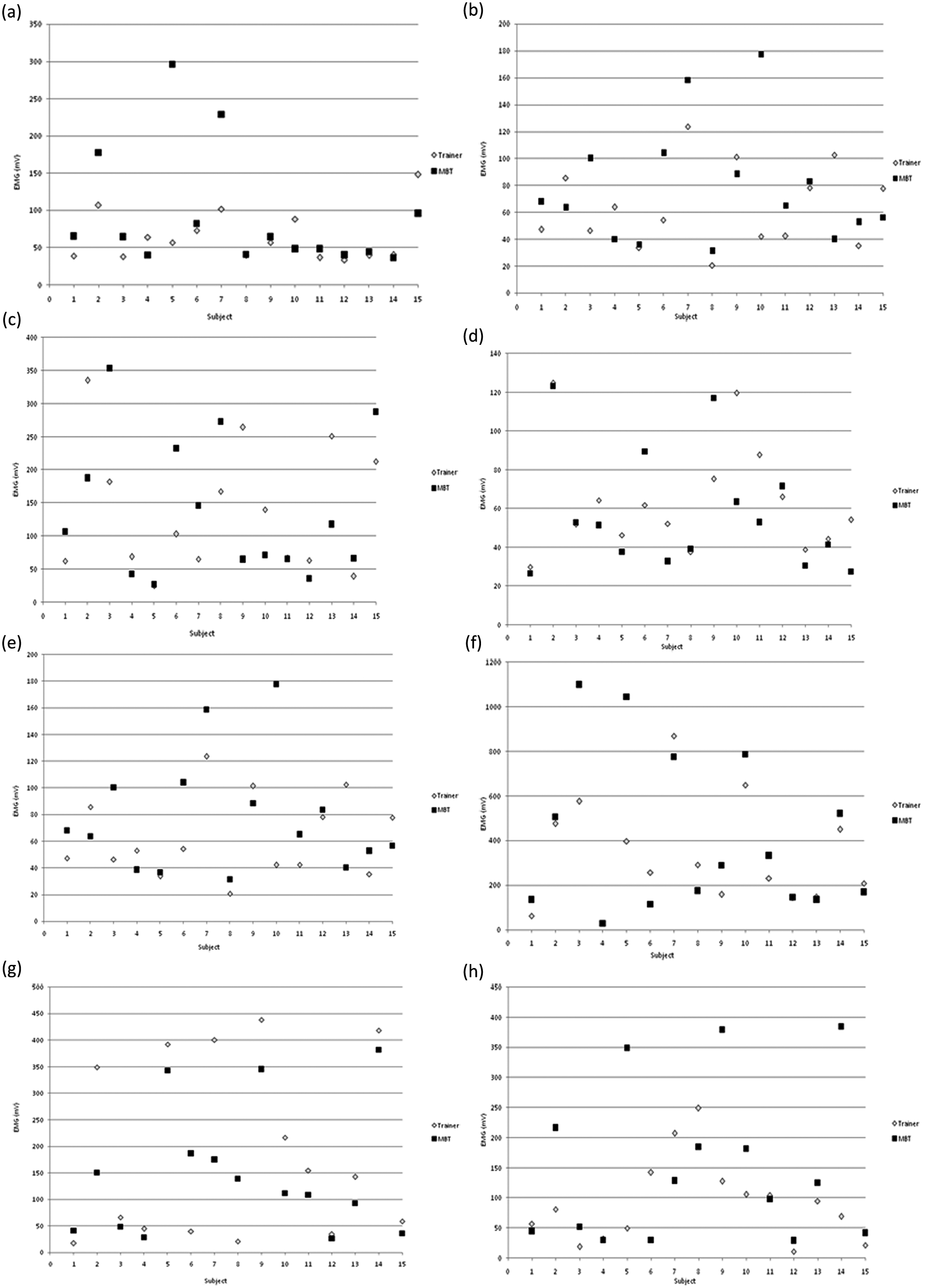
Scatter plot for the mean activity of each muscle for each subject in each shoe condition: (a) soleus, (b) medial gastrocnemius, (c) lateral gastrocnemius, (d) tibialis anterior, (e) peroneus longus, (f) rectus femoris, (g) biceps femoris and (h) gluteus medius. Triangle markers indicate the subjects own trainer shoe and the square markers indicate MBT shoes.
Percentage change
As a representation of the work done by each individual muscle, the mean muscle EMG data were calculated as a percentage of the recorded maximum value for that muscle in each shoe condition. This was compared to the mean maximum recorded for the tip toe exercise. Increase in the muscle activity when wearing MBT shoes were seen in SOL, LG, TA and BF. There was no difference in percentage change for PL and GMed and there was a decrease when wearing MBT shoe in MG and RF (Table 1).
Gait timing
Footswitch data showed no significant difference between the timing of heel strike, heel off and toe off between shoe conditions (Table 2). Again, individual patterns of footswitch data showed that 56% of subjects had the same contact time when wearing trainer and MBT shoes, 25% had lower contact in MBT shoe and 19% had higher contact time in MBT shoe. Paired t-test showed no significant difference for any of the gait timing events between the trainer and MBT shoes.
The mean time (s) at which each event (HS, HL and TO) occurred during gait cycle for each condition.
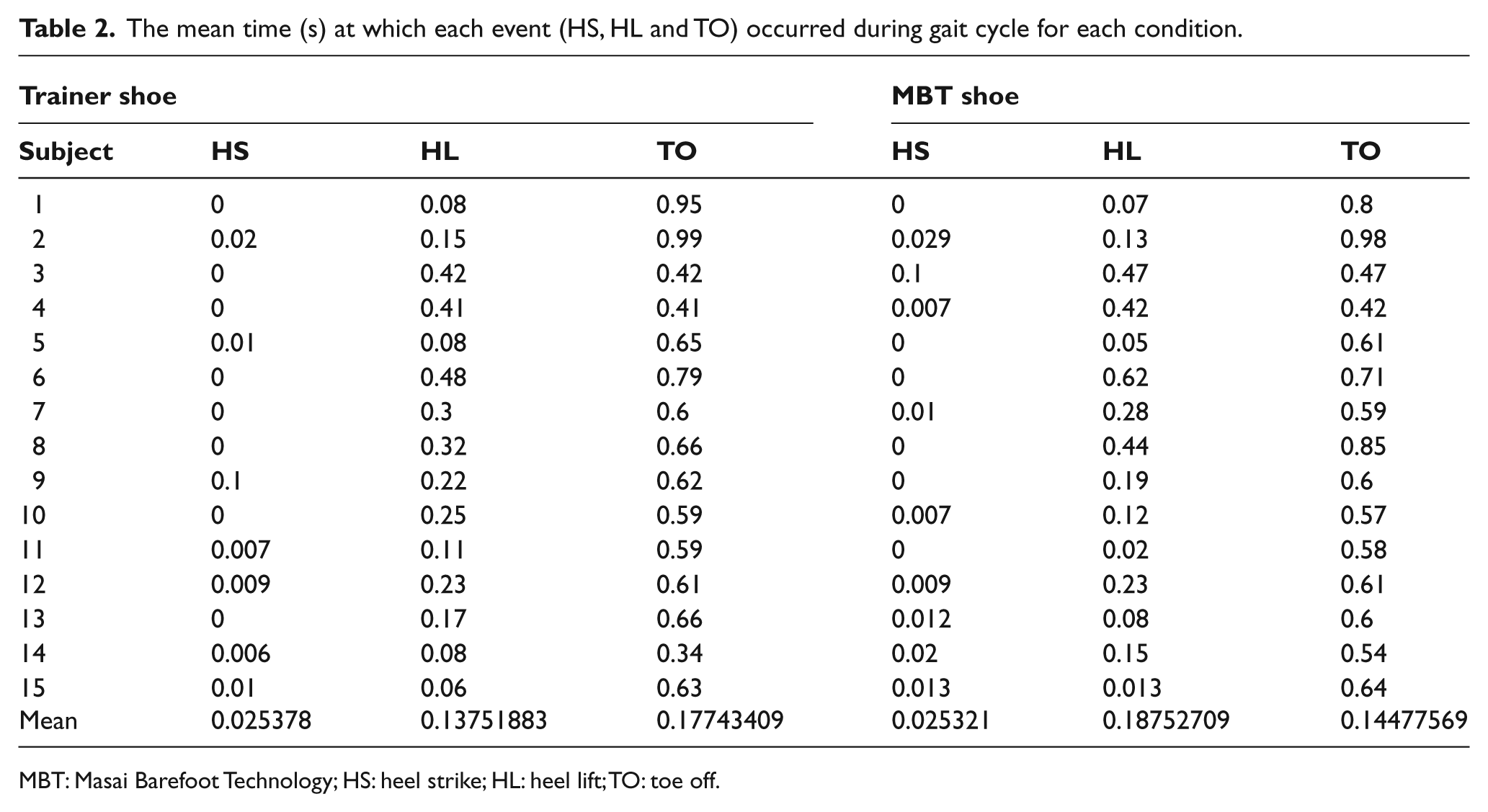
MBT: Masai Barefoot Technology; HS: heel strike; HL: heel lift; TO: toe off.
Discussion
The hypothesis tested was to identify the immediate reaction of the lower limb muscles when the subject wore the MBT shoe for the first time. Although this hypothesis was statistically not supported from the results, mean muscle activity while wearing MBT shoes showed an increase in activity, in five of the eight muscles studied (SOL, MG, PL, RF and GMed). This increased change agrees with previous work that looked at EMG data while wearing MBT shoes after a 4-week adaptation period, with observed increases in muscle activities in TA and gastrocnemius 2 and GMed, 1 suggesting that the observed changes reported after 4 weeks of training can occur immediately in some subjects.
However, it should be noted that in this study, there was a high level of variability between subjects, and there was no systematic response in EMG activity between conditions. Any changes observed were not consistent throughout the group as previously suggested. 2 Furthermore, it is not clear from the current results which factors determine whether the response from wearing the MBT shoe for the first time will increase, decrease or have no effect on muscle activity and at what point adaptation occurs when wearing the shoe. The variability in muscle EMG seems to be unpredictable as to what effect wearing the MBT shoe will have. This makes assessment of the benefit from wearing such a shoe difficult. Therefore, caution should be taken on suggesting an unstable shoe as a treatment modality, and tight monitoring of patients who use these shoes is recommended.
Subtle differences were seen within this study that may provide some suggestions for the variability seen in EMG activity. The weight of the MBT shoe was in some cases 1 kg heavier than the control trainer shoe used. The four subjects who wore the lightest control shoe did have increased EMG while wearing the MBT shoe but the pattern between these groups of subjects was not consistent to substantiate a claim that the effect of the MBT shoe is due to altered weight. Footwear changes have been noted in previous investigations as a reason for altered muscle activity. 12 Instant changes from a lightweight shoe, which the wearer has adapted to using, to a heavy shoe could induce immediate alteration in muscular activity as a response to the altered weight rather than the design of the shoe. Advancing technology to developing varying levels and grades of instability shoes that can be personalised to the subject’s needs and functions could provide differing levels of support and instability dependent on individual muscle activity giving more specific impact. This varied and staged approach will enable a choice as to the most suitable level of instability required.
Discreet changes in the number of footsteps taken, gait event timings and percentage of maximum EMG used were also noted from this study. Overall, the results for these outcomes were unremarkable and the differences between the trainer shoe and MBT shoe were negligible. A primary reason for this could be due to the design of the study where cadence and trainer shoe were not controlled. It was, however, noticed that in some of the subjects, the MBT shoe reduced the number of steps taken, and within that subgroup, the contact time from heel strike to heel lift was faster. These changes (although not directly measured in this study) would alter the stride length and speed at which the subject walked. It has been reported that wearing the MBT shoe did reduce the number of the footsteps taken, and although this change was seen in some of the subjects studied, the result was not constant across all subjects. 2 For a therapeutic intervention, a reduction in footsteps and altered stride length may be a desired outcome for management of certain conditions where the posterior group of muscles is strained, that is, hamstring injury and Achilles tendon pathology. Specific assessment and further research as to the suitability of using the unstable shoe for such an intervention would be required prior to the use of the shoe as a treatment modality.
The percentage of maximum that the mean value of muscle EMG activity worked at compared to the exercise one leg tip toe condition was not significant but indicated that each of the muscles studied demonstrated a mean EMG value of 30% for trainer shoe and 31.4% for MBT shoe. It can be argued that the MBT shoe, therefore, has little effect on the percentage of maximum work done by each of the muscles studied. Expanding this study to evaluate the prolonged changes over a time period when wearing MBT shoe would enhance the understanding of the effect that the unstable shoe has on EMG activity.
Although the results demonstrated variability between subjects, the muscle activation pattern from the MBT shoe condition was in synchrony with the normal trainer shoes suggesting that using MBT shoes do not alter the activation pattern but only alter the intensity of muscle activity when a change is observed. This outcome could be used therapeutically to implement a training effect for treatment of pathologies that are associated with underuse of a muscle. The MBT shoe could be used as a training device to be worn for a set period of time each day. Considering the unpredictable reaction seen within this group, thorough individual assessment of patient suitability would be required prior to intervention to evaluate the individual response to the use of MBT shoe. For those subjects who respond with an increase in muscle activity, the MBT shoe could then be used as a training device to improve poor muscle function. Further work is strongly recommended to investigate the therapeutic use of such shoes and the use of the MBT shoe in the management of pathologies associated to muscle fatigue, imbalance and dysfunction.
In view of the results produced from this study and other significant work on MBT shoes,3,5,9 the widespread commercial availability of MBT and other unstable shoes should be monitored more closely as the effect of the shoe on function and stability can vary so greatly between subjects. It is not known if the immediate or long-term use of unstable shoes has an impact on health. A more vigorous method of assessment as to the suitability of wearing an unstable shoe is recommended. This will require additional understanding as to the effect unstable shoes have on whole body function and adaptation with a focus on identifying factors that predict the behaviour of muscles while subjected to an unstable environment.
Conclusion
This study has shown that there is an increase in mean muscle activity in lower limb muscles, specifically SOL, MG, PL, RF and GMed, but this increase is not statistically significant and varies greatly between subjects when walking in the MBT shoe for the first time without any prior training or muscle adaptation. Although this observed increase in muscle activity in the MBT unstable shoe can occur in some individuals, the mean muscle activity can equally decrease in others. The full effect of wearing such an unstable shoe is not yet fully revealed, and further work into the long-term use and therapeutic use of unstable shoes is recommended.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.