
Abstract
Background:
Few reports have examined the relationship between balance ability and walking ability in people with transfemoral amputation using the Berg Balance Scale.
Objectives:
To assess the construct validity (known groups discrimination, convergent validity, and floor/ceiling effects) of Berg Balance Scale for people with transfemoral amputation.
Study design:
Cross-sectional study
Methods:
Thirty people with transfemoral amputation participated (age: 54 ± 19 years; range: 18–78 years). Outcome measures (Berg Balance Scale, Timed Up & Go test, Six-Minute Walk Test, and use of ambulatory aids) were compared between the groups requiring and not requiring ambulatory aids by the Mann–Whitney U test, Student’s t-test or Welch’s t-test. Correlations were assessed using Spearman’s rank correlation coefficients and age-corrected Spearman’s partial rank correlation coefficients.
Results:
The group using ambulatory aids had a significantly lower Berg Balance Scale score (41 ± 5 vs 52 ± 3). Berg Balance Scale score was correlated with Timed Up & Go test, use of aids, and Six-Minute Walk Test using Spearman’s rank correlation coefficients (r =−0.85, p < 0.0001; r =−0.82, p < 0.0001; r = 0.81, p < 0.0001) and age-corrected partial rank correlation coefficients (r =−0.66, p < 0.0001; r =−0.56, p = 0.0017; r = 0.57, p = 0.0012). No ceiling effect of Berg Balance Scale was observed.
Conclusions:
Balance ability in people with transfemoral amputation could be evaluated using Berg Balance Scale and is correlated with walking ability.
Clinical relevance
In clinical practice, using Berg Balance Scale for people with transfemoral amputation may adequately enable us to discriminate different groups based on walking ability from the perspective of balance ability. When walking ability is evaluated as low, the improvement of walking ability may be evaluated by Berg Balance Scale improvement during rehabilitation.
Background
Re-acquisition of walking ability for people with lower limb amputation (LLA) is crucial from the perspective of enhancing activities of daily living and quality of life. Van Velzen et al. 1 reported that there was a relationship between walking ability after LLA and physical capacity (aerobic/anaerobic capacity, muscle force, flexibility, and balance), and that balance and walking ability were the most strongly correlated among them. 1 Therefore, appropriate balance assessment should be carried out during rehabilitation programs for people with LLA to regain walking ability.
Although balance ability of people with LLA has been reported using laboratory instruments such as a force plate in research,1,2 in clinical practice, it has usually been assessed with performance-based clinical tests administered easily without expensive equipment. Performance-based clinical tests are classified into single-task outcome measures, mostly used as screening tools, and multi-task outcome measures used for detailed evaluation of balance ability. 3 Most of the studies of performance-based clinical tests in people with LLA used single-task outcome measures, including the One-Leg Standing test (OLS-t)4–7 and the Timed Up & Go test (TUG-t),8,9 and they showed the relationship between balance and walking ability. In contrast, although several studies have reported multi-task outcome measures including the Community Balance & Mobility Scale (CB&M) 10 and the Berg Balance Scale (BBS),11–16 only a few studies12,14 have reported the relationship between balance and walking ability. Pollock et al. 3 reported that multi-task outcome measures evaluate a broad range of walking balance and may better assist clinicians in identifying specific ambulatory deficits and directing treatment. Therefore, to evaluate the balance ability of lower limb amputees in a clinical setting and to plan treatment, further studies on multi-task outcome measures should be performed.
BBS was developed as a clinical measure for evaluating the balance ability of elderly individuals 17 and has been used in a variety of subjects.18–20 According to several studies of lower limb amputees, BBS has been confirmed to have excellent reliability and validity,12,13 and it has been reported to assess fall risk12,15 and predict outcomes. 16 However, these studies included a wide range of amputation levels. Unilateral and distal amputation levels were predictive of better walking ability, 21 and Burger et al. 22 reported that, for elderly people with LLA, the level of amputation had a significant effect on functional testing.
Walking ability after LLA is assessed by kinetic, kinematic, functional, and self-report measures. 1 The Six-Minute Walk Test (6MWT) is an indicator of walking ability. It has been reported that 6MWT evaluates the global and integrated responses of all systems involved during exercise, including the pulmonary and cardiovascular systems, systemic circulation, peripheral circulation, blood, neuromuscular units, and muscle metabolism. 23 Furthermore, it has been reported that 6MWT could be used as an integrated measure of mobility function 24 and was correlated with BBS. 25 In addition, it is used as the outcome measure of walking ability in people with LLA7,26 and is correlated with the OLS-t 7 and Amputee Mobility Predictor (AMP). 26 Concerning the use of ambulatory aids, use of mobility aids increases the base of support (BOS), and a mobility aid potentially allows the user to keep the center of mass (COM) within BOS limits for a greater proportion of the gait cycle. 27 Consequently, the use of an ambulatory aid can improve balance in persons with loss of stability. Therefore, people requiring ambulatory aids may have some balance deficits. Other studies reported that persons requiring ambulatory aids had lower BBS scores.12,18–20 In addition, using ambulate aids precludes the activities of daily living and social life requiring both hands, therefore it is crucial to release hands from the aids. Indeed, it is reported that use of the prosthesis indoor enabled the people with LLA to walk while carrying an object 28 and use of ambulatory aids had a negative impact on quality of life evaluated with the MOS short-form 36 (SF-36). 29 Hence, it is important to research the body functions of people with LLA from the viewpoint of the use of ambulatory aids.
Previous studies reported that people with transfemoral amputation (TFA) showed lower success rates for prosthetic rehabilitation than people with transtibial amputation (TTA), 30 and community mobility rates at 1 year following amputation were 54% for people with TTA and 29% for people with TFA. 31 However, the reasons of the lower success rates for rehabilitation among people with TFA have not been determined from the perspective of balance. Furthermore, people with TFA had significantly lower advanced score on the locomotor capabilities index (LCI) 28 and higher fall risk 28 than people with TTA. Therefore, the research focused on people with TFA is necessary. Therefore, the purpose of this study was to assess the construct validity (known groups discrimination, convergent validity, and floor/ceiling effects) of BBS for people with TFA.
Methods
Participants and context
A sample of convenience was used. Participants were recruited by physical therapists from the list of patients at Hyogo Rehabilitation Center Hospital. Fifty-six patients were approached, and all patients agreed to participate in this study. Participants with mental deterioration, severe ischemic heart disease, advanced neurological disorders, or who were considered inappropriate by the attending physician were excluded from the study. Thirty people with TFA, 18 years or older, who were hospitalized or re-hospitalized in the facility for prosthetic walking training at Hyogo Rehabilitation Center Hospital or visited as outpatients and were capable of prosthetic walking for at least 6 min met the inclusion criteria for this study. In Japan, people with LLA are allowed by the national health insurance system to be hospitalized for rehabilitation after LLA. Some of the participants were re-hospitalized to evaluate their adaptation to the prostheses. Outpatients participated at the time of their periodic medical examination. All participants were informed of the protocol and gave their written, informed consent in principle. Each participant performed BBS, TUG-t, and 6MWT. The results were analyzed and compared between the two groups classified based on the use of ambulatory aids. Older people with TFA were defined as ⩾60 years old, while younger one were <60 years old. This cross-sectional study protocol was approved by the institutional ethics review board of Hyogo Rehabilitation Center Hospital (approval number 1306).
Procedures
BBS, TUG-t, and 6MWT were assessed by 10 physical therapists for no longer than 40 min. The participants were allowed and confirmed to have enough rest between each performance test to avoid fatigue. Hospitalized participants performed BBS, TUG-t, and 6MWT at the end of prosthetic training, while re-hospitalized patients and outpatients performed them sometime within the episode of care. Whether each participant used an ambulatory aid for daily walking was confirmed by each physical therapist.
Functional evaluation of balance and walking ability
BBS
BBS assesses functional balance based on the performance of 14 items, including the sitting position and one-leg standing. 17 A participant’s performance on each task is graded using a 5-point ordinal scale ranging from 0 to 4. The total score for all tasks consists of 56. Higher scores represent good balance. In this study, tandem standing and one-leg standing were performed with both legs separately, and the lower score was recorded. Inter- and intrarater reliabilities of BBS for lower limb amputees have been shown to be excellent. 13
TUG-t
In TUG-t, 32 each participant was instructed to rise from a standard chair (seat height 43 cm), walk a short 3 m distance, turn around, walk back, and return to sit in the chair using a customary ambulatory aid if needed. The best time of two trials was recorded after the participants were confirmed to understand the method of TUG-t. Inter- and intrarater reliabilities of TUG-t for lower limb amputees have been shown to be excellent. 8
6MWT
In 6MWT, 23 participants were instructed to walk 90 m in a rectangle (30 m × 15 m) as far as possible for 6 min using a customary ambulatory aid if needed.
Statistical analysis
To identify differences between the groups with and without ambulatory aids, various statistical tests were performed. First, normality of observations for Age, TUG-t, and 6MWT was assessed based on Shapiro–Wilk test. If normality assumption was satisfied, we first conducted F-test to check equality of variance. When normality assumption was not satisfied, we applied a Mann–Whitney U-test. When equality of variance was satisfied, Student’s t-test was performed. In contrast, we applied Welch’s t-test if the equal variance assumption was violated. The scores of the BBS were compared between the groups with and without ambulatory aids by the Mann–Whitney U test because the scores of BBS was an ordinal scale. The correlations between BBS, age, TUG-t, ambulatory aids (single cane/double canes/walker, 1; no aids, 0), and 6MWT were evaluated by Spearman’s rank correlation coefficients. In addition, because the ages in this study were widely distributed from 18 to 78 years, age-corrected Spearman rank partial correlation coefficients were calculated to evaluate the correlations between BBS, TUG-t, ambulatory aids, and 6MWT, and the relationships between age, BBS, and ambulatory aids were evaluated using a scatter plot. Correlation coefficients ⩽ 0.3 were interpreted as weak, those > 0.3 to < 0.6 as moderate, and those ⩾ 0.6 as strong. 33 Floor/ceiling effects were calculated as the percentage of participants who achieved the minimum or maximum possible BBS score. Floor/ceiling effects of ⩾20% were considered significant. 33 In this study, to reduce a risk of type l error, a Bonferroni-adjusted significance level of 0.00455 was calculated by dividing the p value of 0.05 by the number of statistical analyses performed. 34 Data were analyzed using R version 3.3.0.
Results
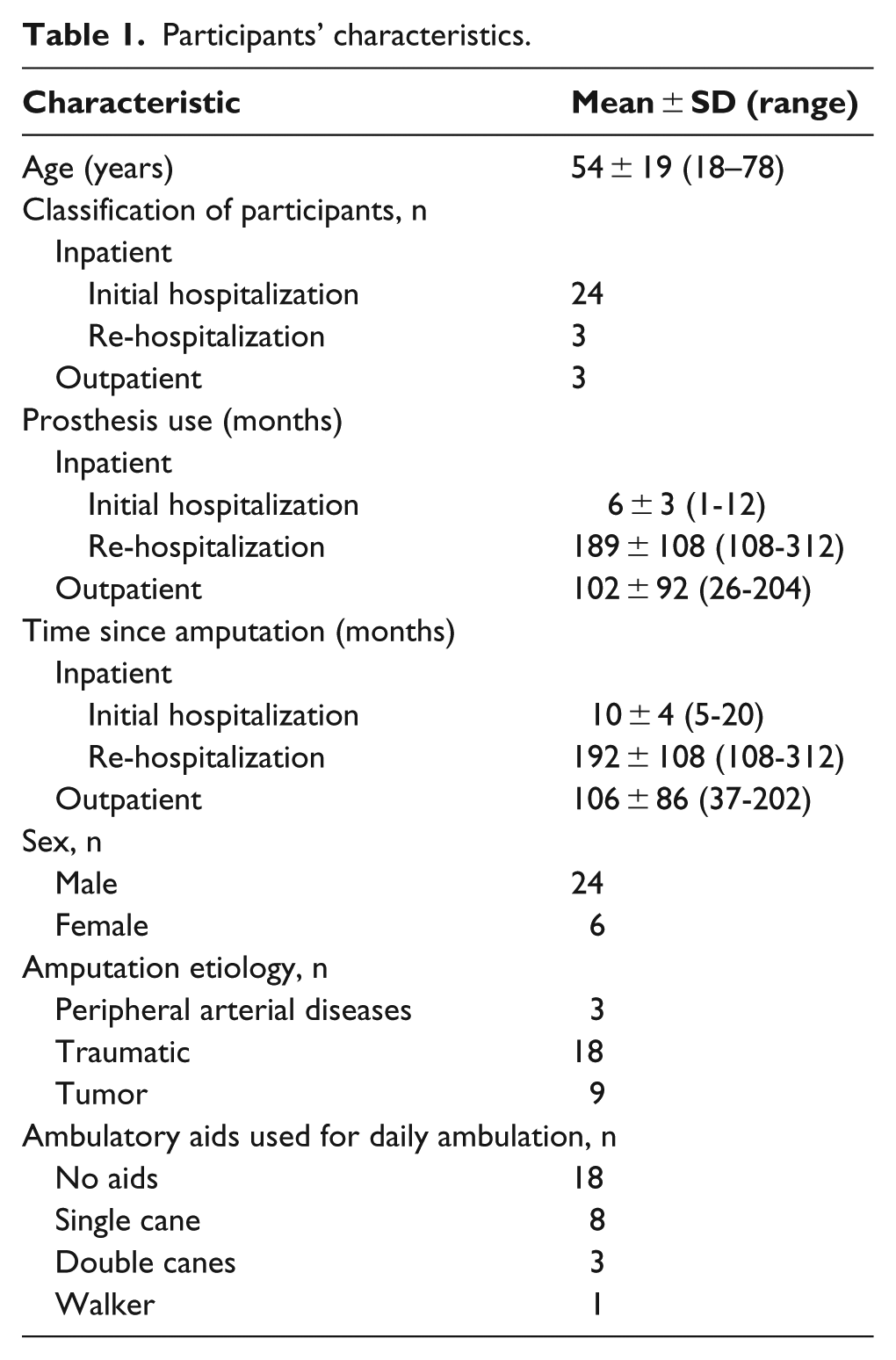
The participants’ characteristics are shown in Table 1. Twelve of 30 participants used ambulatory aids when walking. The group with ambulatory aids was significantly older (70 ± 5 vs 44 ± 18 y) and had a lower BBS score (41 ± 5 vs 52 ± 3), longer TUG-t time (23.1 ± 11.6 vs 10.3 ± 4.2 s), and shorter 6MWT distance (285 ± 90 vs 497 ± 108 m) than the group without ambulatory aids (Table 2, Figure 1). BBS score was significantly correlated with age, TUG-t, ambulatory aids, and 6MWT (r =−0.76, p < 0.0001; r =−0.85, p < .0001; r =−0.82, p < .0001; r = 0.81, p < .0001). Using age-corrected Spearman rank correlation coefficients, BBS score was significantly correlated with TUG-t, ambulatory aids, and 6MWT (r =−0.66, p < 0.0001; r =−0.56, p = 0.0017; r = 0.57, p = 0.0012) (Table 3). No ceiling effect of BBS was observed (3.3%; only one participant achieved the maximum BBS score). However, most younger participants walked without ambulatory aids and had close to perfect BBS scores. Meanwhile, most of the ⩾60-year-old participants needed ambulatory aids to walk and had low BBS scores (Figure 2).
Participants’ characteristics.
Comparison of age, BBS, TUG-t, and 6MWT by the use of ambulatory aids.
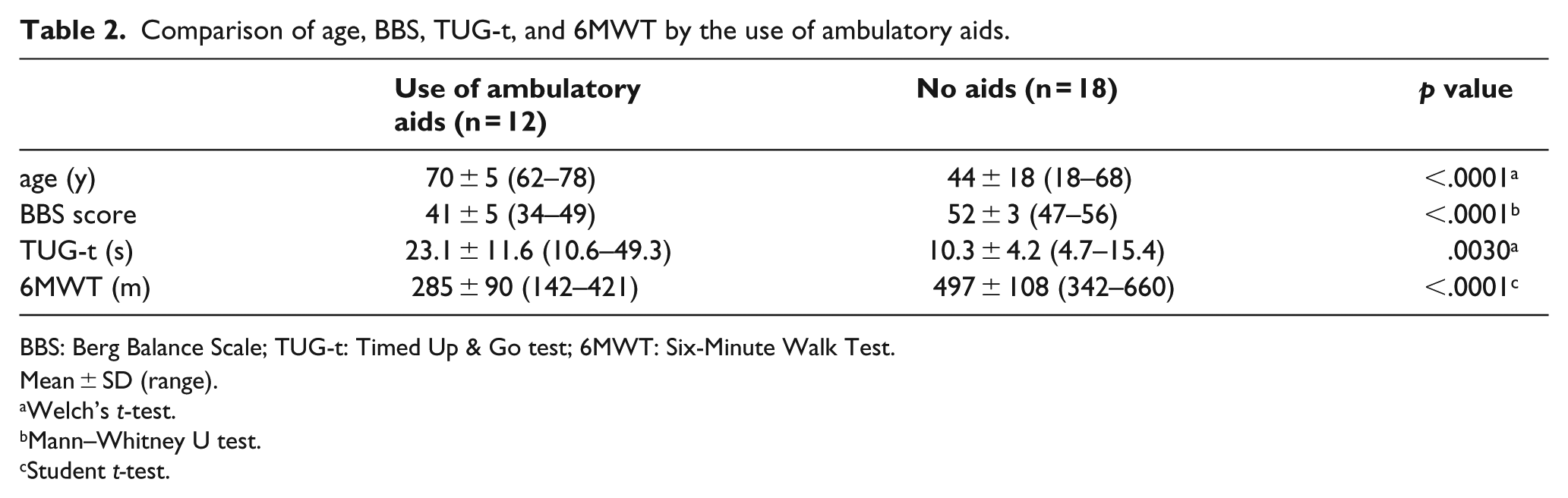
BBS: Berg Balance Scale; TUG-t: Timed Up & Go test; 6MWT: Six-Minute Walk Test.
Mean ± SD (range).
Welch’s t-test.
Mann–Whitney U test.
Student t-test.
Relationship between BBS scores and age, TUG-t, use of ambulatory aids, and 6MWT.
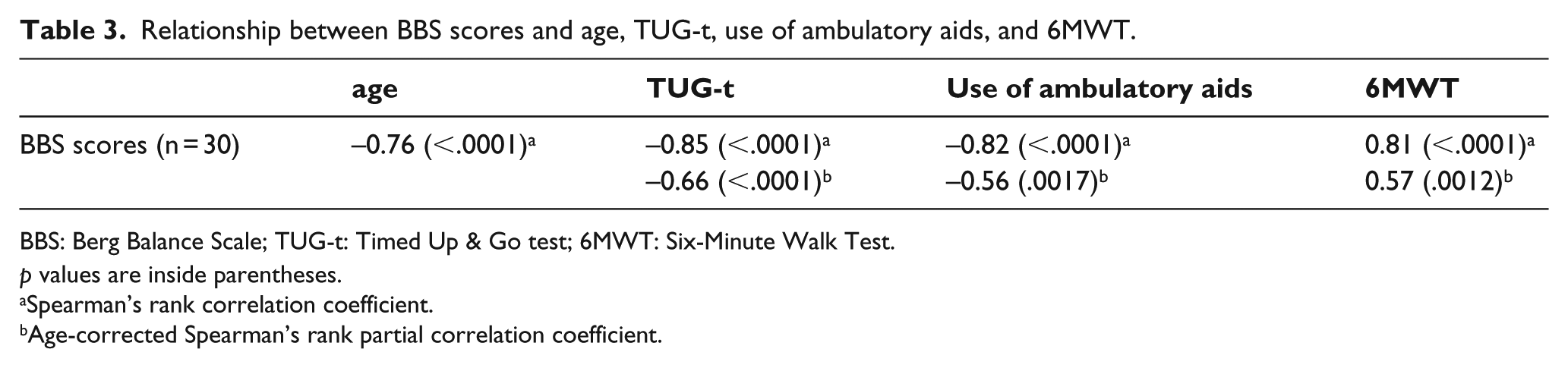
BBS: Berg Balance Scale; TUG-t: Timed Up & Go test; 6MWT: Six-Minute Walk Test.
p values are inside parentheses.
Spearman’s rank correlation coefficient.
Age-corrected Spearman’s rank partial correlation coefficient.
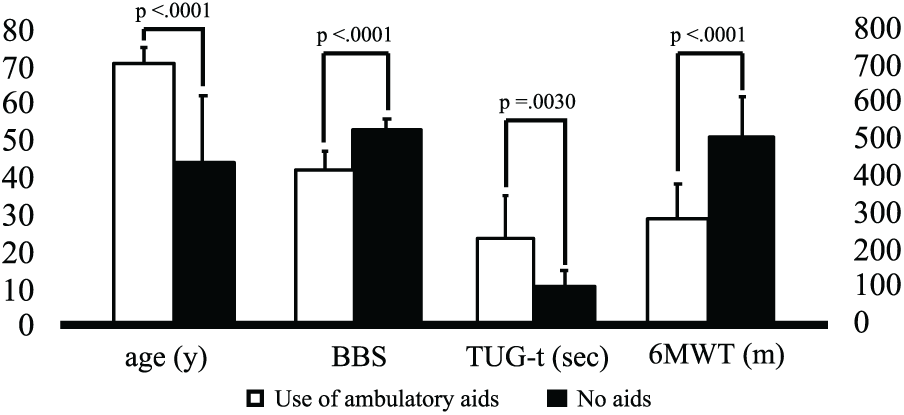
Columns of comparison of age, BBS, TUG-t, and 6MWT by the use of ambulatory aids.
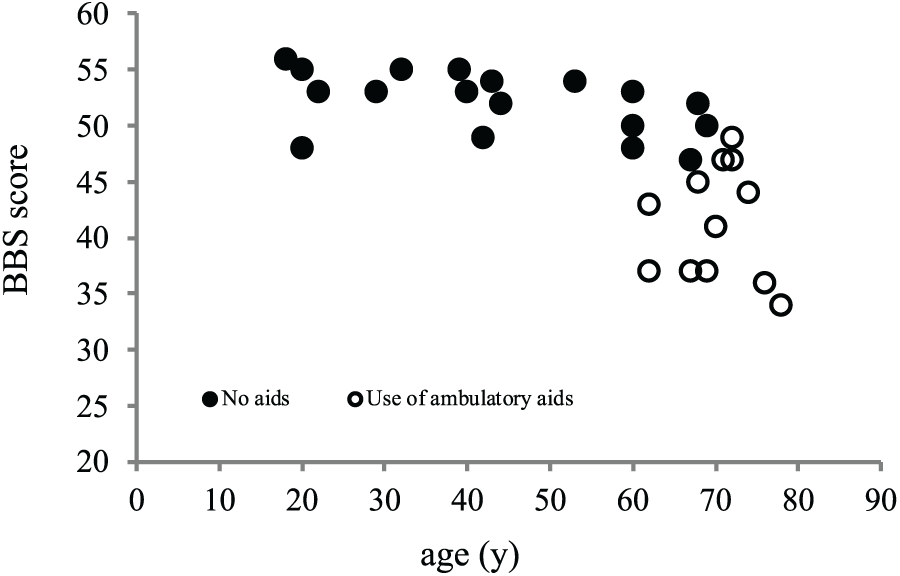
Relationship between BBS scores and age.
Discussion
In this study, the relationship between balance function and use of ambulatory aids was investigated. Previous studies reported that persons requiring ambulatory aids had lower BBS scores, including older adults (no aids:cane:walker = 47.2:39:31.1), 18 post-stroke unilateral hemiparesis patients (no aids:cane = 53.68 ± 2.18:39:72 ± 9.19), 19 and tetraplegic and paraplegic spinal cord injury patients. 20 In the present study, the group with ambulatory aids had a lower BBS score than the group without (no aids:use of ambulatory aids = 52 ± 3:41 ± 5). Major et al. 12 reported that people with LLA requiring ambulatory aids had lower BBS scores (no aids:use of ambulatory aids = 54:49); however, they did not consider the amputation level of the participants. Since amputation levels affect balance ability,2,22 it is necessary to compare similar levels of amputation. In this study, all participants were people with TFA, and BBS score was significantly correlated with the use of ambulatory aids, by both Spearman’s rank correlation coefficient and partial correlation coefficients. Balance ability in people with TFA could be evaluated using BBS and was correlated with use of ambulatory aids. In a future study, subjects’ ages should be matched to obtain a clear conclusion.
Next, the convergent validity of BBS was investigated. There were strong correlations between BBS scores and TUG-t, ambulatory aids, and 6MWT. In contrast, the age-corrected partial correlation between BBS and ambulatory aids and 6MWT, excluding TUG-t, showed a moderate correlation. The strengths of the correlations were −0.56 with ambulatory aids and 0.57 with 6MWT, which were considered moderate. 33 Therefore, the evaluation of balance ability by BBS is important, because walking ability may be improved by improving balance ability when balance ability is evaluated as low. These results are also compatible with those of previous investigations suggesting that walking ability is affected by age.1,21 Overall, the findings of the present study provide evidence for the convergent validity of BBS for functional balance and walking ability.
Furthermore, floor/ceiling effects of BBS in people with TFA were evaluated. In the study sample, 3.3% reached the BBS score ceiling, which was considered negligible. However, most of the younger people with TFA had close to perfect BBS scores and walked without ambulatory aids. Meanwhile, most of the ⩾60-year-old people with TFA had low BBS scores and needed ambulatory aids to walk. This result means that appropriate subjects should be selected when using BBS to evaluate balance ability in people with TFA. According to several investigations of people with LLA, BBS was found to have a ceiling effect.11,12 If the balance ability of active people with LLA is evaluated by BBS, decision-making regarding the assessment may be difficult, because they easily achieve close to perfect BBS scores. Knorr et al. 35 observed ceiling effects in community-dwelling patients after a stroke when BBS was administered, and they reported that the use of the CB&M may be more appropriate for ambulatory stroke survivors with mild to moderate post-stroke disability, whereas the balance and mobility of persons severely affected by stroke are more appropriately evaluated with BBS and TUG-t. In other words, there is a certain adaptation range if BBS is used, and BBS should be used for people affected by stroke with low balance ability. Similarly, there appears to be a certain adaptation range in people with TFA because Figure 2 shows that most younger people with TFA had close to perfect BBS scores. However, no ceiling effect of BBS was observed, it was not possible to reach a clear conclusion about the adaptation range of BBS. When a further study of the adaptation range of BBS is completed, the floor and ceiling effects should be evaluated after classifying participants by age and activity level.
Study limitations
This study has several limitations. First, the distribution of age in this study was wide, ranging from 18 to 78 years. Previous research indicated that older age at the time of amputation had an adverse effect on walking ability.1,5 In this study of convergent validity of BBS, the results of the partial correlation coefficients between BBS and TUG-t, ambulatory aids, and 6MWT showed lower correlations than the results of the Spearman rank correlation coefficients. When further study of the balance ability of people with TFA and ambulatory aids is carried out, age should be taken into account, such as narrowing the target to subjects ⩾60 years old. Second, this study had selection bias because the research design was cross-sectional, and the sample size was small. Therefore, additional studies taking into account sample age and sample size are necessary. Third, a convenience sample of people with TFA recruited from a single rehabilitation facility was used to assess the construct validity of BBS. Further research involving the BBS of people with TFA dwelling in the community or as a multicenter study is needed when considering the generalizability of the study results. Fourth, this study had the potential series effect (e.g. fatigue) because the order of the outcome measures was not randomized. However, the participants had enough rest between each performance test to reduce the effect. Fifth, in this study, because the statistical analysis was repeatedly performed, there is a risk of type I error. In this study, a Bonferroni-adjusted significance level calculated was 0.00455 or less. 34 Accordingly, the impact of a risk of type I error was considered to be very small in this study.
Conclusion
Balance ability in people with TFA was evaluated using BBS and was correlated with walking ability. BBS may be used as a clinical outcome measure to assess people with TFA using ambulatory aids or older people with TFA with low balance ability.
Footnotes
Author contributions
Yuji Azuma; planning of research, measurement and analysis of data, writing papers. Takaaki Chin; supervising of research. Yasushi Miura; interpretation of data, writing papers.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.