
Abstract
Background:
Evidence-based practice is commonly accepted as a means of improving patient outcomes; however, there is little understanding of the processes required to successfully implement it into prosthetic and orthotic practice.
Objectives:
To discuss factors affecting adoption of evidence-based practice and present a theoretical framework for its implementation into prosthetic and orthotic practice.
Discussion:
Numerous factors that affect adoption of evidence-based practice are discussed, ranging from individual factors to those that can be attributed to administrative and environmental issues. Specific factors are likely to be context specific and are influenced by the manner in which evidence-based practice is introduced into the working environment. It is argued that successful implementation of evidence-based practice requires consideration of numerous interrelated factors. A formal translating research into practice model is presented as a means of developing a strategic plan that considers all relevant factors and maximizes acceptance of evidence-based practice into prosthetics and orthotics clinical practice.
Conclusions:
The use of a theoretical model for implementation of evidence-based practice is likely to improve its adoption by prosthetic and orthotic clinicians.
Clinical relevance
The demand for prosthetists/orthotists to utilize evidence-based practice is increasing. Lack of strategic planning throughout the implementation phase is likely to compromise adoption of evidence-based practices by clinicians.
Background
Evidence-based practice (EBP) is commonly cited as a necessary step toward improving patient outcomes after a prosthetic or orthotic intervention.1–5 To date, articles related to EBP in prosthetics and orthotics (P&O) have focused on defining terminology, 3 reviewing the state of EBP in P&O clinical practice and on identifying factors that influence the use of EBP in P&O clinical practice.1–3,5 To date, no discussion or research has been dedicated to the practical process of introducing and sustaining EBP as part of clinicians’ everyday routine. Christensen and Andrysek 5 suggest that strategic implementation may facilitate the use of EBP but highlight that little research is available from within the field of P&O. The purpose of this article is to discuss factors that are likely to influence the adoption of EBP in P&O and to present an example of one implementation model (translating research into practice (TRIP) model) that can be used to guide both management and clinicians through a systematic process of change toward EBP.
Many examples of unsuccessful implementation of EBP are presented in the literature,6–8 and it has become apparent over the past decade that passive approaches such as traditional lectures, distribution of state of science recommendations, and clinical guidelines are often unsuccessful in changing clinical practice.9–11 In light of this, it has been suggested that strategic planning for the EBP implementation process is a major factor that can contribute to the success of its adoption by key players. 12
Much has been documented regarding barriers to implementation of EBP. The factors most commonly cited as negatively influencing adoption include access to evidence-based resources, inadequate knowledge, poor organizational support, and time constraints.13–17 In P&O, barriers to adopting EBP have been specifically identified as follows: time constraints, workload demands, limited relevant evidence, gaps in the skills and knowledge to perform EBP, demographics, and level of involvement in research.1,5
Implementation science, sometimes cited as translation science, is the scientific study of methods that promote the adoption of research into practice. 18 A number of models have been proposed to elucidate variables that may influence adoption of EBPs and to facilitate the TRIP.12,19–21 These models are typically grounded in organizational theory or adult learning and are most often multifaceted in their approach. 20 Examples include the following: Rogers’ diffusion of innovation (DOI) model,19,22,23 the decision-making framework, 24 the advancing research and clinical practice through close collaboration (ARCC) model,25,26 and the promoting action on research implementation in health services (PARIHS) model. 27 A common element within each of the implementation models is the need to address both the individual and the organization. 28
In the authors’ experience, implementation of EBP into P&O clinical practice has been rather unstructured. Facilities tend to introduce one or two specific measures to facilitate TRIP but fail to address the bigger picture and many of the other individual and organizational factors that can affect adoption of EBP. The author argues that the use of a formal model to facilitate implementation of EBP would increase the likelihood of its adoption into P&O clinical practice.
Discussion
Theoretical framework
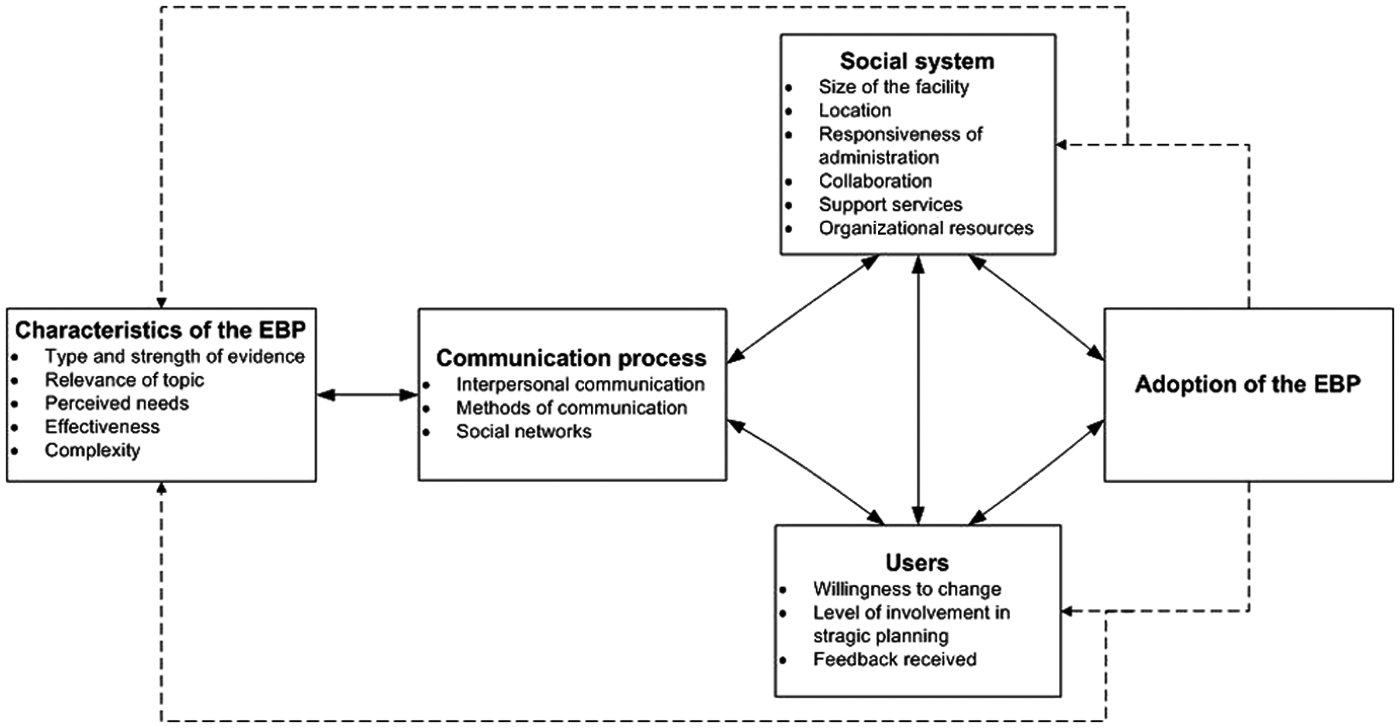
The TRIP model presented in this article was developed by Titler and Everett 22 and was based upon Rogers’ DOI model. 29 This model was selected as it has been shown to positively influence adoption of EBP when tested in other clinical environments.23,30–32 The model serves as a framework for developing strategies that promote implementation of EBP. It assumes that adoption of research is influenced by the characteristics of the EBP topic (type and strength of evidence; clinical relevance) and the manner in which it is communicated to users in a social system. Figure 1 presents an overview of the model together with specific examples of factors that are likely to affect adoption of EBP. The TRIP model is based on the premise that strategies for implementation of EBP must address all the key areas within the framework and that failure to develop an implementation strategy that includes all areas within the model will compromise adoption of EBP by the target group. Each specific area is presented in detail below; however, it must be recognized that interaction between areas also affects the rate and extent of adoption. 28
Characteristics of the EBP
The topic of an EBP and how it is perceived by potential users is an important consideration that can affect the extent to which it is adopted by users. Topics that are perceived as relatively simple, more effective, and highly relevant are more readily adopted by clinicians. 28 In order to maximize adoption of EBPs, clinicians/users should be involved in the process of assessing needs, reviewing material, and adopting EBPs to fit their current work processes and the local context. 21 When considering this in the context of P&O, this means that prosthetists/orthotists themselves must be involved from day 1 in selecting and prioritizing clinical practices that will be targeted for review. It must also be the clinician in practice who takes responsibility for evaluating the feasibility of eventual recommendations or guidelines.
The use of decision aids to simplify the decision-making process has been shown to have a positive effect on supporting EBPs if they are introduced with careful consideration of the clinical context and communication process.7,20 Examples of decision aids available within the field of P&O include decision-making algorithms 33 and clinical guidelines.34–36
Communication process
Sustainable EBP is not possible without effective channels of communication. Clinicians typically respond more positively when information is disseminated through peers and social interactions. 28 A number of strategies have proven successful in facilitating communication and increasing the likelihood of adopting EBPs. Use of opinion leaders, change champions, and educational outreach are positive examples.
Opinion leaders have been demonstrated to have positive effects on adoption of EBP.24,37,38 The role of an opinion leader is to disseminate evidence and support users in the translation of evidence into practice. As facilitators of EBP within a P&O clinic, the opinion leader should be someone from outside the facility who is considered as “educationally influential.” Opinion leaders facilitate change through a variety of social interactions ranging from informal chats and one-on-one discussions to group teaching and other forms of education.28,38
Change champions may be recruited from within the P&O facility. They should be clinicians who are committed to quality improvement and have a good working relationship with their peers. Change champions are responsible for circulating information and encouraging peers to adopt an EBP. They should communicate regularly with opinion leaders who can help to address questions and provide guidance. 28
Education outreach refers to an occasion when a trained educator visits clinicians in their own environment to conduct an education session. This technique has proven to be a factor that positively influences the adoption of EBP, especially when implemented in conjunction with opinion leaders.28,39,40
Social system
When implementing EBP, the social system refers to the organizational context within which users are operating. Social systems have been demonstrated to have an impact on adoption of EBP with interventions that have been proven successful in one organizational context found to be less effective when applied in a different context. 41 The factors that influence adoption of EBP within the social system include the location of the facility, leadership support, organizational resources, and staffing. 28 The size of the institution has also been shown to influence success in implementing EBP with larger organizations, divided into specialty units and with the capacity to devote resources to new projects more readily adopting interventions. 19
For the P&O facility wishing to implement EBPs, it is important to have strong leadership with a clear strategic vision and a willingness to devote resources to EBP. Policies, procedures, standards, clinical pathways, and documentation systems must all support the use of EBPs. Leadership is essential to promote the use of EBP, to encourage a culture of learning, and to set in place the processes to identify and apply new knowledge as it becomes available. Performance expectations should be set in place for staff, which include EBP work, and a process that includes audit and feedback should be established. For sustainability, it is essential that clinicians/users are involved in structuring workflow, so that new processes can be embedded in existing ones. 28
Users of the EBP
The success of EBP depends very much on changing the behavior of clinicians. Clinicians must be open to new ideas and willing to implement EBP. This “willingness” is intrinsically linked to the manner in which EBPs are communicated and to the level of organizational support provided. It can also be influenced by education and the way in which research is viewed by the profession. As previously discussed, this may require a cultural shift by the P&O profession. 3
Strategies that have been successfully trialed to influence acceptance of EBP at the level of the user have employed techniques that involve clinicians themselves in the strategic development and evaluation phases. This ensures that clinicians remain as active participants in the process of change rather than passive recipients of information.
Clinicians should be involved in identifying practices that shall become the focus of EBP change and in identifying practice performance indicators that will eventually be used to measure change. They should be involved in conducting performance gap assessments (PGAs), which compare baseline performance with potential performance (i.e. where are we now and where do we want to be). Audit and feedback should be ongoing and communicated regularly to clinicians. Audit in this context can refer to any summary of clinical performance over a period of time. 42 By providing feedback to clinicians on key performance indicators, clinicians are kept up-to-date, informed of their progress, and motivated to continue the process.
Examples from other health-care professions
While the TRIP model presented above has not yet been used in the context of P&O, several examples exist in which it has been used to systematically implement EBPs into a clinical environment.23,31,32 Titler et al. 23 utilized the model when developing strategies aimed at promoting EBP for management of acute hip pain in older patients with hip fracture. During the planning phase, each of the areas within the TRIP model was used to develop implementation strategies. For example, when considering “characteristics of the EBP,” the authors held focus groups to elicit feedback from potential users and introduced six quick reference guides and standardized pain rating scales in order to simplify the decision-making task. Implementation plans were similarly developed for “communication process,” “social system,” and “users.” Twelve acute care hospitals were involved in the project; all hospitals received EBP guidelines on acute pain management in the elderly, but six hospitals also received the TRIP intervention. The results indicated that the quality of acute pain care was significantly higher for patients treated at hospitals exposed to the TRIP intervention and that patients treated at these hospitals had a lower mean pain intensity rating. In a similar study, Brooks et al. 31 demonstrated that the use of the TRIP model to increase the use of evidence-based pain management led to significant cost savings.
It should be recognized, however, that not all support the use of an implementation model. Bhattacharyya et al. 43 suggest that there is a lack of empirical evidence that application of explicit theories for implementation of EBP results in behavioral change. While the TRIP model outlined in this article has been tested in numerous clinical contexts, it is yet to be tested in the P&O clinical environment. The author welcomes future studies in this area.
Conclusions
Prosthetists/orthotists are generally positive to embracing EBP into their daily routine; however, a number of barriers exist, which prevent its implementation. 1 The author believes that there is a real danger that haphazard implementation of EBP will lead to rejection by clinicians. The use of a model to facilitate implementation and maximize acceptance of EBP appears to be a beneficial means of addressing this issue, and the author strongly advises P&O facilities to consider this and develop formal plans for implementation.
Recommendations
Based upon research evidence, the following recommendations are made to facilitate adoption of EBP by prosthetists/orthotists.
Begin to implement change only when the work environment is stable (adequate staff, no planned organizational change).
Implement policy changes that support EBPs.
Have clinicians reflect upon their own practices, involve them in needs assessments and in reviewing EBPs.
Identify opinion leaders and change champions who can provide ongoing education, support, and encouragement to clinicians.
Monitor progress and provide continuous feedback to clinicians.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.