
Abstract
Background and Aim: This article describes the development and testing of a new powered gait orthosis to potentially assist spinal cord injury patients to walk by producing synchronized hip and knee joint movements.
Technique: The first evaluation of the orthosis was performed without users, and was followed by evaluation of the orthosis performance using three healthy subjects to test the structure under weight-bearing conditions. The orthosis was primarily evaluated to ascertain its ability to generate appropriate hip and knee motion during walking. The walking experiments replicated the flexion and extension of both the hip and knee produced by the actuators which had previously been demonstrated during the initial computer simulations.
Discussion: The results suggest that this new orthosis could be used to assist paraplegic subjects who have adequate ranges of motion and also with weakness or reduced tone to ambulate, and may also be suitable for other subjects with impaired lower limb function (e.g. stroke, poliomyelitis, myelomeningocele and traumatic brain injury provided they do not have increased tone or movement disorders.
The new powered gait orthosis can provide walking assistance for patients with a spinal cord injury who have a good range of motion at the hip and knee and who also have weakness or reduced tone.
Background and Aim
Several limitations still exist for paraplegic patients when walking with orthoses. Such limitations include the reported high energy consumption during ambulation, high loads on the upper limb joints and the need for improvements in the kinetics and kinematics demonstrated while walking in current orthoses for this patient group.1-9 The design of new orthoses such as the advanced reciprocating gait orthosis (ARGO)3,10 the ‘walk about’ orthosis, 11 the ‘prime walk’ orthosis, 12 the hip and ankle linkage orthosis 13 and the isocentric reciprocating gait orthosis (IRGO), 14 have not solved these problems in the provision of paraplegic ambulation.
Hybrid orthoses such as those using functional electrical stimulation (FES) in conjunction with RGOs, and powered orthoses using a combination of pneumatic, hydraulic or motorized actuators with RGOs have attempted to resolve these problems.2,15 One limitation of using FES in combination with orthoses is the rapid reduction in muscle strength caused by fatigue16-19; so another approach such as the use of powered orthoses has the potential to offer more effective walking by paraplegic patients.
Powered orthoses can improve energy consumption and the cosmesis of walking for paraplegic patients.20,21 Ruthenberg et al. designed and constructed a one degree-of-freedom powered gait orthosis for walking by paraplegic patients, but this orthosis only powered the hip joints. 22 Yano et al. fabricated a weight bearing control orthosis (WBCO) which demonstrated a higher speed of walking than with other orthoses, but energy consumption was not improved.23,24 A motorized orthosis to assist walking by using direct current (DC) motors to power both the hip and knee joints was developed by Ohta et al., but it was bulky and needed high levels of power to drive the hip joint. In addition, the knee or hip actuators were only tested in isolation rather than being synchronized and tested in tandem. 15 Kang et al. designed a powered hip orthosis to assist in paraplegic walking which used pneumatic actuators applied to the hips. However, the actuators were not as powerful as electrically powered ones. 25 Finally, Audu et al. developed a novel hip orthosis for paraplegic ambulation, but it was excessively heavy and consequently reduced the speed of walking by 25% compared to normal walking in healthy subjects. 26
In view of the current limitations of current devices, and to potentially improve energy consumption, the kinetic and kinematic parameters of gait and the cosmetic appearance of walking with a powered orthoses by paraplegic patients, a prototype gait orthosis was developed which incorporated synchronized powered hip and knee joints.
Technique
Design considerations for the new orthosis
The isocentric reciprocating gait orthosis (IRGO) was developed in 1992, by Motlock, 14 by replacing the cable connecting the hip joints with a low friction rocker bar link. The IRGO produced higher walking speeds compared to other devices such as other types of RGO, the walkabout orthosis and hip-knee-ankle-foot-orthosis (HKAFO).27-29 Walking distance has also been shown to increase when compared to ambulating in a HKAFO, 27 and cadence is improved when compared to ARGOs. 29 This evidence led the development team for this project to choose the IRGO as the base structure for which electrically-actuated powered joints would be developed to add powered motion to selected lower limb joints.
The mechanical design of the hip joints in the IRGO allows flexion of one hip which causes simultaneous extension in the opposite hip. These rotations were motorized in this new design by adding powered actuators (Maxon motor, model EC powermax30, 200 W, Maxon motor manufactory, Switzerland) to the existing components of the IRGO. The actuator was connected with a planetary gearbox with a reduction ratio of 156 to the hip joint connector link (Figure 1). Figure 2 shows the pattern of hip joint movement that was achieved via the actuator.

Connection of the actuator to the hip joint connector link.
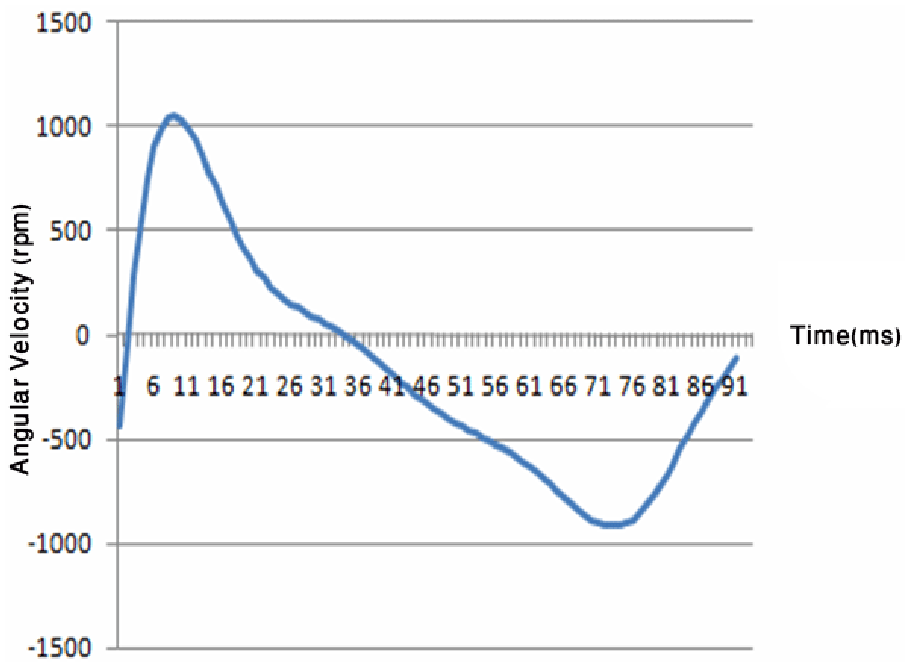
Pattern of hip joint movement using the actuator.
The mechanical knee joint of the IRGO is designed to be locked in both stance and swing phase, and only manually unlocked and locked for sitting and standing. It was therefore the intention to design a powered orthotic knee joint that would provide a more natural motion during walking. The knee joint for this new orthosis was designed to be locked in stance, but to have active flexion and extension movement during swing phase. To achieve this, a ‘Maxon Motor EC max30’ actuator, 40 W (Maxon, Switzerland) was used with a planetary gearbox with a reduction ratio of 111. The crucial part of this design was to enable a synchronizing pattern of knee joint movement with the hip joints. Figures 3 and 4 show the activated knee joint design and the knee joint movement pattern within the new orthosis respectively.

Knee joint design of new powered gait orthosis.
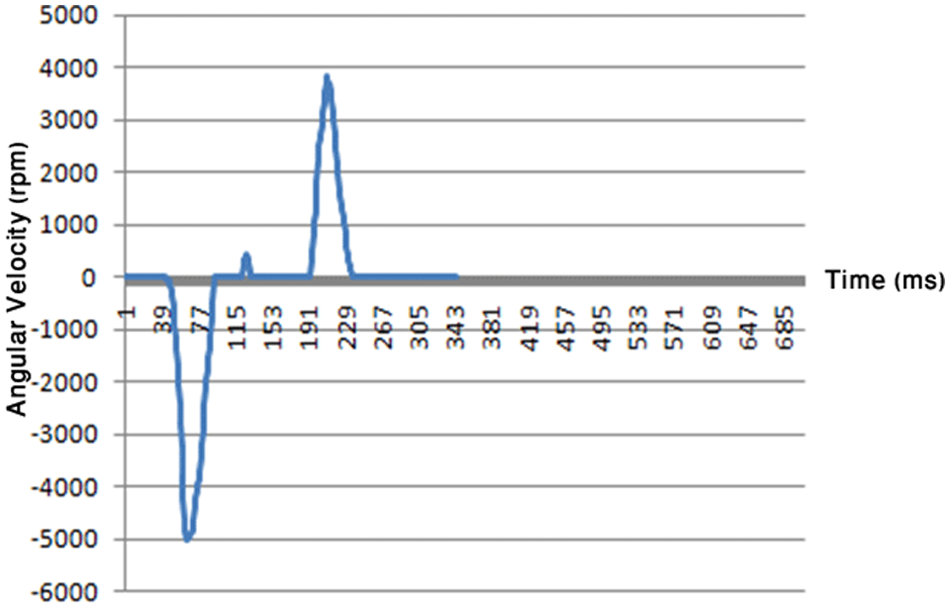
Pattern of knee joint movement using the actuator.
Figure 5 shows an overall view of the new orthosis prototype. One distinct potential advantage is its low weight (total weight 10.1 kg). One rechargeable 24 V battery (Lipo Battery, Thunder Power RC G6 Pro Lite 25C 5400 mAh 6-Cell/6S) was used in this orthosis, and was operated using a joystick during ambulation.

Prototype of new powered gait orthosis.
Functional mechanism of the new orthosis
The electronics included motors, optical encoders, motor drivers, power and a programmable controller. The electro motor and gearbox were selected in such a way to provide maximum and highest possible efficiency. The motor sequencing was based on models optimized by software specifically designed and built for this purpose. The patterns of motion in orthotic joints could then be programmed into the microcontroller to the main system. Using this approach, actuators were capable of generating appropriate movement patterns at specified intervals during the complete gait cycle.
New orthosis performance without a user in a laboratory setting
The first step in the evaluation of the orthosis was use of the new prototype orthosis in the laboratory without a user in situ. The prototype was fitted to a static plaster of Paris surrogate model of the human pelvic, trunk and lower leg and foot, which allowed an initial evaluation of the walking parameters demonstrated by the orthosis during simulations to be evaluated. This dummy model was prepared and designed based on the average adult male with 165 centimeter height and 54 kg weight, and incorporated bilateral hip and knee joints. The joints of the lumbar and pelvic areas, as well as the ankles were fixed. The hip joints were composed of a spherical joint, while each knee joint comprised of a hinged joint to provide flexion and extension movements (Figure 6). The aim of this experimental testing of the orthosis was to determine any problems with stability arising from propulsion applied by the actuators, and to resolve them. To verify the function of actuators applied to the orthotic knee and hip joints, the input pattern of motion in each actuator was compared with the simulation results. The simulation analysis showed an identical pattern to the experimental results with minimal error.

The surrogate model.
Orthosis performance with three healthy subjects in the gait laboratory
The next phase of development involved the use of the orthosis by three healthy subjects the aim being to identify and analyse the range of gait patterns which could be designed into the device. A prototype of the new orthosis was fabricated to fit three healthy volunteer subjects. The new orthosis was designed with an adjustable construction so that it could be separately worn by all three subjects. The ankle foot orthosis (AFO) portions were custom moulded for each subject individually and assembled within the frame of the orthosis for each of the subjects. They were all asked to relax their lower limb muscles as much as possible while participating in the walking trials, while using a walking aid via their upper limb musculature. It was thought prudent to utilize the three healthy individuals in this initial testing in preference to patients with a spinal cord injury (SCI) to prove the structural integrity and stability of the design prior to future testing by SCI subjects, and was thought to be a logical step from using the static clay model for safety reasons. It is, however, appreciated that during the walking trials the three volunteer subjects could not be guaranteed to not aid in the walking via applying their own muscular effort and therefore would not simulate SCI walking entirely. However, the results from the power output from the hip and knee joint actuators indicated that they did not vary from simulations; indicating that any help from the lower limb musculature of the three healthy volunteer subjects was minimal.
Fifteen reflective surface markers were applied to the lower extremity and four reflective markers were placed on the trunk. The placement positions were the greater trochanter, lateral condyle of femur, head and lateral malleolus of fibula, the second metatarsal, ASIS, calcaneus, jugular notch, spinous process of the seventh cervical vertebrae and left and right acromio clavicular joints. Lower extremity markers were placed on the uprights of the orthosis as close as possible to the considered points to minimize offset during the data capturing phase.
The marker data were captured by a Vicon digital motion capture system (Oxford Metrics, UK) using a frequency of 100 HZ and two force platforms (Kistler 9286BA, Switzerland). For all trials, each volunteer subject walked with a walking frame to simulate paraplegic patient walking. Gait analysis tests were performed in the Biomechanics Laboratory of Ergonomic department of University of Social Welfare and Rehabilitation Science, Tehran, Iran. Ethical approval was sought from the University ethics committee before the study began.
To approve the performance of actuators under weight bearing conditions, the patterns of hip and knee joint movement by the actuators on the bench were compared with the results of the dummy test condition when added to the orthosis and also when using healthy subjects (with a 61 kg mean weight) to walk with the new powered orthosis. The results showed that the hip and knee joints patterns were similar in the simulation model and experimental conditions with the healthy subjects being tested.
Hip and knee angle patterns in walking with new powered orthosis were similar in type to those of normal walking patterns. However, due to the use of the reciprocating link used in the IRGO, the maximum flexion and extension angle of hip joints was reduced compared to normal walking, along with the maximum knee joint flexion angles.
There were significant differences in step lengths (p < 0.05) and walking speeds (p < 0.05) between normal walking and walking with new orthosis. A one-way ANOVA was used to compare the means of the two parameters.
Discussion
In this study, we present a new powered orthosis with motorized actuators for the purpose of assisted walking for paraplegic patients such as those with a SCI. The new orthosis, to our knowledge, is the first powered orthosis with synchronized hip and knee joints designed and constructed for SCI patient walking. The prototype of the new orthosis was investigated with and without user involvement. The flexion and extension plots of the hip and knee joints produced by the actuators during walking experiments were the same as those demonstrated during simulation procedures.
In this study there were no significant differences when using the powered orthosis and normal walking in hip and knee joint angles except for the reduced ranges of motion. This gave the group confidence that the new orthosis could be used by certain paraplegic patients. The results, however, showed that speed of walking (28%) and step length (32%) decreased in the new orthosis in comparison to normal walking. Similar results were observed for other new orthoses designed by Audu et al. 26 and Yang et al. 30
The patterns of motions demonstrated in the hip and knee joints with the newly developed orthosis showed that it could feasibly be used for assisting in walking for those paraplegic patients with low tone and adequate ranges of motion at the hip and knee joints. The power of the electrically actuators in the new powered orthosis could also be altered according to individual’s characteristics, and could also be used with just the hip or knee activated or with synchronized hip and knee joint activation. However, the main advantage of the current developed new orthosis is synchronization of the hip and knee joint movements.
Although the motorized actuators were designed as an integral component of a new powered orthosis for SCI patients, this powered system could also potentially be used by other subjects (e.g. those with poliomyelitis, stroke and traumatic brain injury) provided they did not have increased tone or movement disorders. The key findings were that simulation and replication of hip and knee sagittal plane rotations similar to that in normal human locomotion may be feasible when adapting an IRGO with actuators at those joints and is worthy of further development. It is therefore the intention to evaluate the efficacy of the new orthosis in providing appropriate walking parameters for paraplegic patients, and a further study is therefore planned to evaluate the effect of this type of orthosis on walking by SCI patients.
Key Points
Powered orthosis could be used by spinal cord injury, poliomyelitis, stroke, and traumatic brain injury subjects.
The power of the electrically actuators in the new powered orthosis could also be altered according to individual’s characteristics, and could also be used with just the hip or knee activated or with synchronized hip and knee joint activation.
The patterns of motions demonstrated in the hip and knee joints with the newly developed orthosis showed that it could feasibly be used for assisting in walking for those paraplegic patients.
Footnotes
Acknowledgements
The authors would like to thank Reza Vahab Kashani, Ali Valizadeh and Sahar vazirzadeh for their advice and support.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.