
Abstract
Background: While sparsely researched, funding structures may play an important role in use of and satisfaction with prostheses and related health services.
Objectives: The objectives of this study were to (1) quantify the direct costs of prosthesis wear, (2) explore variations in funding distribution, and (3) describe the role of affordability in prosthesis selection and wear.
Study design: An anonymous, online cross-sectional descriptive survey was administered.
Methods: Analyses were conducted of qualitative and quantitative data extracted from an international sample of 242 individuals with upper limb absence.
Results: Access to prosthesis funding was variable and fluctuated with age, level of limb absence and country of care. Of individuals who gave details on prosthetic costs, 63% (n = 69) were fully reimbursed for their prosthetic expenses, while 37% (n=40) were financially disadvantaged by the cost of components (mean [SD] US$9,574 [$9,986]) and their ongoing maintenance (US$1,936 [$3,179]). Of the 71 non-wearers in this study, 48% considered cost an influential factor in their decision not to adopt prosthesis use.
Conclusions: Prosthesis funding is neither homogeneous nor transparent and can be influential in both the selection and use of a prosthetic device.
Inequitable access to prosthesis funding is evident in industrialized nations and may lead to prosthesis abandonment and/or diminished quality of life for individuals with upper limb absences. Increased efforts are required to ensure equitable access to upper limb prosthetics and related services in line with individuals’ needs.
Introduction
Limb prostheses provide individuals with valuable options to consider when developing personal strategies to optimize quality of life and function. In accordance with Andersen’s behavioural model for healthcare utilization, 1 the decision to adopt, refuse or abandon an upper limb prosthesis depends on a mixture of predisposing factors (e.g. level of limb absence), established needs (e.g. lifestyle) and enabling resources (e.g. funding and access to healthcare services). 2 When the latter dominates the decision to use or not use a prosthesis, this may be an indication that access to the assistive device is inequitable and in need of reform. 1 While inequitable access to assistive devices is a well established problem in developing countries, 3,4 very little research has been conducted to describe individuals’ experiences in obtaining financial support in industrialized nations.
Funding policies for prosthetic technologies vary both internationally and regionally. In Canada, in-patient rehabilitation services are fully covered by the publically funded healthcare system with less comprehensive funding for out-patient services. 5 Consequently, prosthesis funding must be procured through a combination of government programmes, private insurances and charitable organizations (e.g. War Amputations of Canada). In the United States, coverage for prostheses and related services may be obtained through personal health insurance, when available, and/or through organizations such as Veterans Health Administration, Workers Compensation, Medicare, Medicaid, Vocational Rehabilitation and State Technology Assistance programmes. 6 As such, there exists a large degree of interstate variation in the provision of assistive technologies. 7 In some cases, eligibility criteria for assistive technologies are open to misinterpretation by both clinicians and/or insurers, adding to inconsistencies in coverage. 8 Culturally based differences in funding for assistive technologies have also been noted. For example, one study suggested that Hispanics in the United States are less likely to access government funding bodies for assistive technologies than non-Hispanics. 9 Australia also has several government-supported funding bodies (e.g. WorkCover, Department of Veterans’ Affairs, aids & equipment programmes and artificial limb programmes specific to each state) that can be accessed depending on eligibility criteria such as the cause of limb absence and financial need. 10 Meanwhile, the Netherlands adopts a more selective approach to prosthesis fitting and funding, based largely on level of limb absence. 11 Evidently, resources for assistive technologies and prostheses in particular are extremely heterogeneous, and accessibility may vary considerably from individual to individual depending on characteristics of the limb absence (e.g. cause, level) and personal eligibility (e.g. vocation, financial need).
Very little is known regarding the extent to which current funding schemes meet the needs of individuals with upper limb absence. A survey of clinics in the United States reported that cost was rarely a factor in prosthesis selection. 12 Conversely, in 2002, increased consumer interest in electric prostheses was documented in response to the Centers of Medicare and Medicaid Services’ decision to support reimbursements for microprocessors in the United States. 13 Interestingly, Roeschlein noted an association between users’ perceived cost of the prosthesis and its subsequent use, with better usage of devices thought to be more costly. 14
The overall goal of this study was to explore access to and extent of funding for upper limb prostheses. To this end, we will (1) quantify the direct costs of upper limb prosthesis wear, (2) explore variations in funding distribution, and (3) describe the role of affordability in prosthesis selection and wear.
Methods
The questionnaire
Description of survey items relating to the specific research goals of this study.
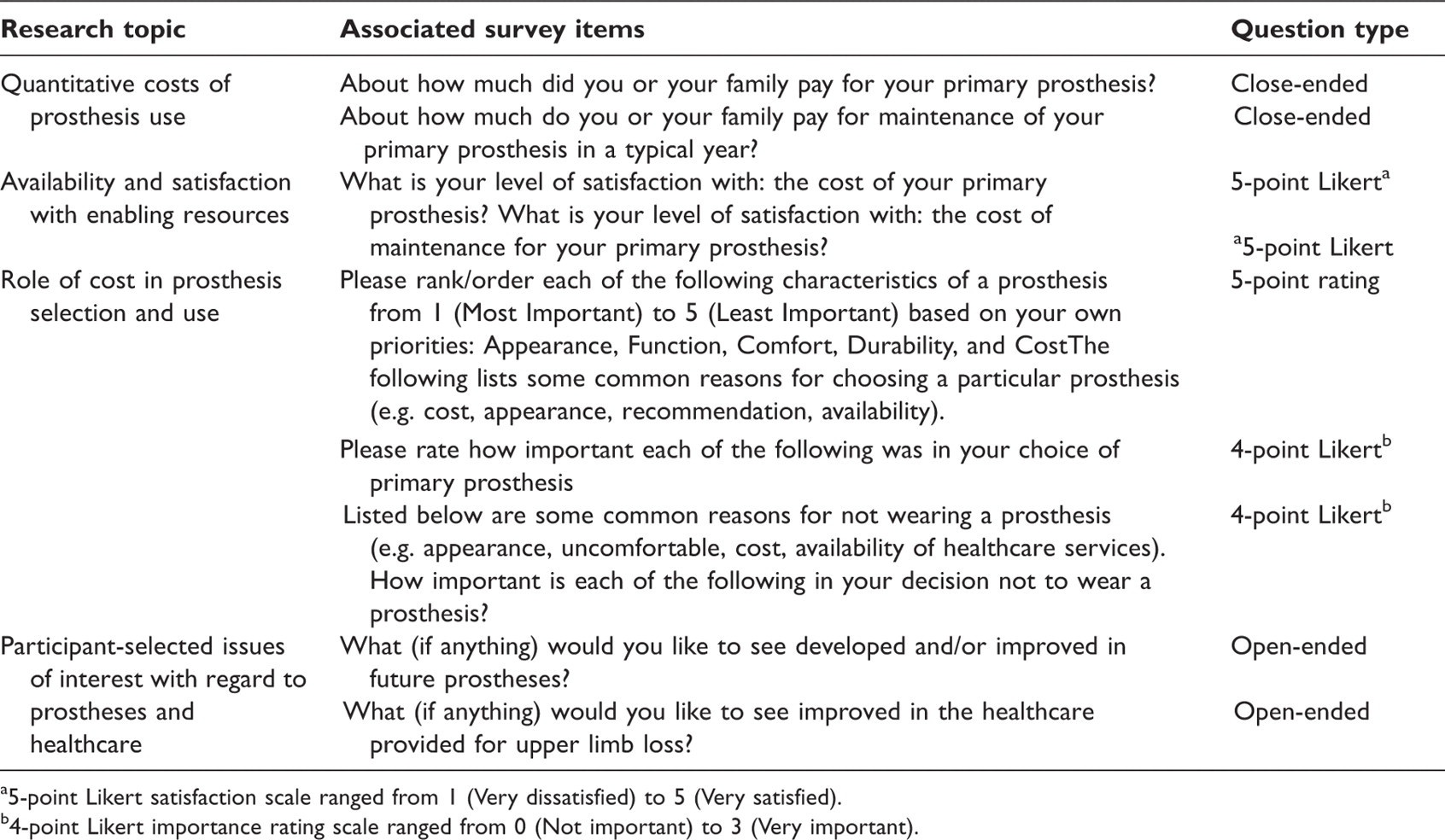
5-point Likert satisfaction scale ranged from 1 (Very dissatisfied) to 5 (Very satisfied).
4-point Likert importance rating scale ranged from 0 (Not important) to 3 (Very important).
Target population and sampling strategies
The survey was designed for individuals with different levels and origins of upper limb absence, all types of prostheses, user status and age. Children under the age of 12 years were accessed through parents/guardians. The survey was circulated through online support groups (i.e. Arm-Amp, I-CAN, Stumps R Us and UpperEx) and healthcare providers (e.g. Holland Bloorview Kids Rehabilitation Hospital, Canada; Shriners Hospital for Children, Los Angeles, USA; Sint Maartenskliniek, The Netherlands), and was also promoted on the website of Otto Bock Inc., a prominent manufacturer of upper limb prosthetics. The questionnaire was available in four languages (English, French, Spanish and Dutch) both online and on paper. The sample was self-selected.
Data analysis
Answers to open-ended questions were analysed via documented procedures of content analysis. 20 This process began with the establishment of a coding convention by which the data were systematically categorized and sorted. In this analysis, an emergent coding approach was adopted wherein categories around the issues of funding for assistive devices were not established a priori, but following two independent examinations of the data by the investigators (EB, SL). Generated codes were compared and then merged, relabelled or split, as necessary. Peer debriefing, during which key themes and interpretations of the data were discussed among the authors, helped to establish the trustworthiness of the findings. Qualitative data were organized using NVivo 8 qualitative data analysis software.
Quantitative data were analysed using SPSS 16.0 statistical software. Chi-squared analyses were applied to comparisons of categorical groups, while differences in ordinal ratings (i.e. levels of satisfaction) were evaluated using the Mann-Whitney U test (for two groups) or the Kruskal-Wallis test (for more than two groups). Frequency counts and three measures of central tendency (mean, median and mode) were used where appropriate. All costs are reported in US dollars.
Results
Summary of participant characteristics.
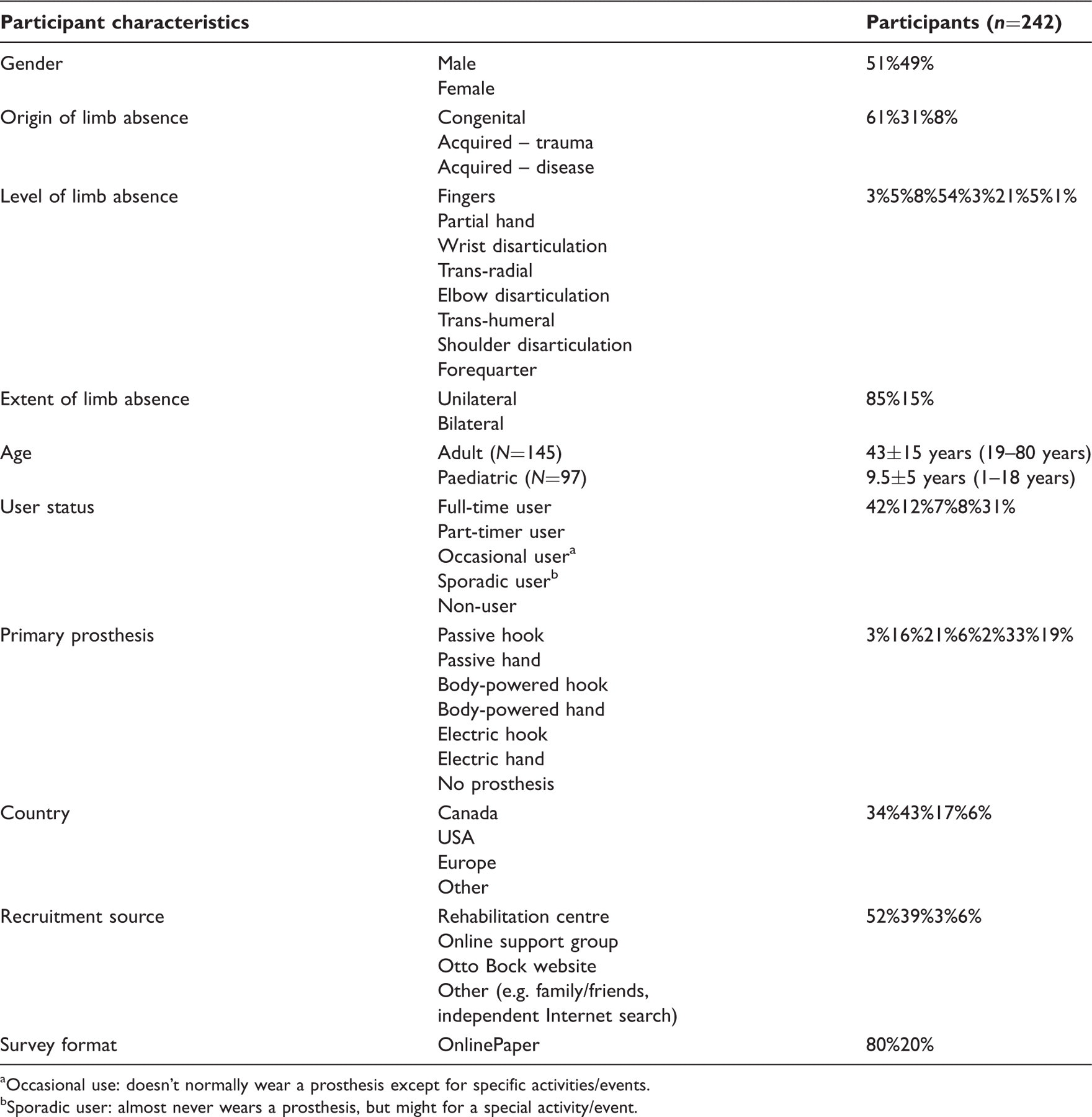
Occasional use: doesn’t normally wear a prosthesis except for specific activities/events.
Sporadic user: almost never wears a prosthesis, but might for a special activity/event.
A. Direct costs of prosthesis wear
Reported costs of prostheses by type.
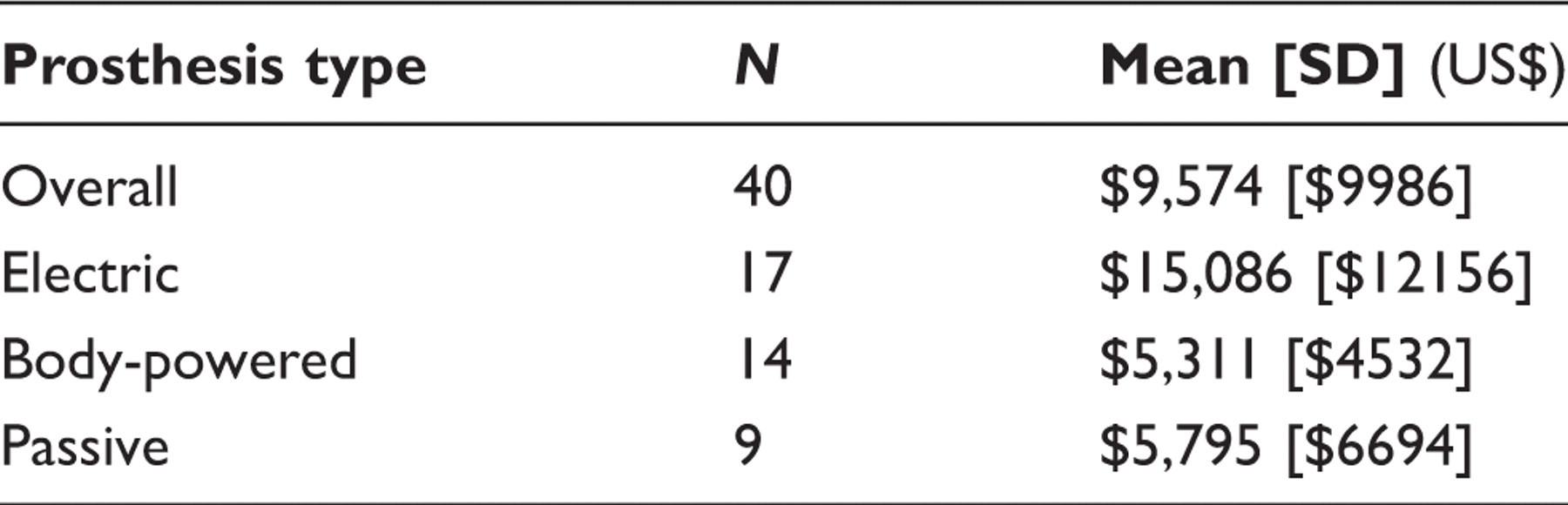
Prostheses, like any complex and well-used technology, require ongoing maintenance, which can also be expensive and burdensome to individuals if not subsidized. Of the 84 participants who completed this section, 71% (n=60) reported zero costs associated with yearly maintenance, which was either fully covered by funding agencies or not required on an annual basis (i.e. an infrequently used prosthesis might not need regular maintenance). Details pertaining to the frequency and nature of typical maintenance activities are reported elsewhere. 18 For the remaining 29% (n=24) of participants who reported on maintenance expenses, the average cost incurred per year was $1,936 [$3,179] with a range of $100 to $10,000 per year.
Not surprisingly, satisfaction with the cost of prostheses (p<0.001) and their maintenance (p=0.001) was significantly lower for individuals who did not receive full funding in comparison to those who did.
B. Variations in funding distribution
Funding was obtained through a mixture of agencies, including government healthcare and disability support (e.g. Assistive Devices Program in Canada, Medicaid in the USA, Veterans Affairs and Workers Compensation), charities (e.g. War Amps, Shriner’s Hospitals for Children) and private insurance. Many of these funding agencies cover only a percentage of prosthetic costs, which can sometimes be challenging for individuals.
‘Even with insurance the average person can't afford them (their Part). Most insurances pay 80% but the other 20% is brutal.’ [#495: male, 38 years, USA, trans-humeral, acquired-trauma, electric hook (full-time user)]
Additionally, each of these organizations may have different regulations and procedures to access funds. The aggravations of identifying and obtaining prosthesis funding were specifically elaborated on by a number of participants.
‘I know that my parents had a great deal of trouble with our healthcare providers while I was growing up and I often had to wait months for repairs and refitting because insurance was slow to permit it.’ [#618: female, 19 years, USA, trans-radial, congenital, myoelectric hand (full-time user)]
Greater standardization and timely revisions were also desired by participants to ensure that funding policies remain up to date and in line with evolving technologies.
‘Standardize the provision of prostheses so we don’t have to fight with the insurance company every time because an electric hand is “too high tech.”’[#137: male, 36 years, USA, trans-humeral, acquired-trauma, electric hook (full-time user)]
‘I would like to see healthcare providers quicker to allow for prosthetic needs and less reluctant to cover new technology and new patient needs.’ [#618: female, 19 years, USA, trans-radial, congenital, myoelectric hand (full-time user)]
When comparing the demographic attributes of individuals who received full funding to those who did not, a number of interesting differences emerged. Firstly, 33% (n=4) of individuals with low level limb absence (i.e. wrist and distal) received full financial support as compared to 58% (n=19) of individuals with high-level limb absence (i.e. elbow and proximal) and 73% (n=45) of individuals with trans-radial limb absence. These differences were statistically significant (p=0.024). Additionally, it was noted that funding may not be equally distributed across ages: 89% (n=32) of children as compared to 50% (n=36) of adults received full funding for prosthetic devices (p<0.001). Evidently, access to funding may change substantially throughout a person’s lifetime.
‘I’m fortunate that I’ve had health care coverage through my work, but retiring at age 54 because of the strain and pain of my real arm forced me to pay a considerable amount of money out of my own pocket. One reason why I pay for extra care is the tremendous cost of new and repairs to my prosthesis. Although now I don’t wear it too much so I don’t need to replace it often. The ADP program [Assistive Devices Program] has helped me considerably because my health care benefits does not cover the whole cost. When I’m 65 my extra health plan stops. I probably won’t be able to afford the amount not covered by ADP. People need help in paying for the expense of prosthesis if they can’t afford it.’ [#543: 60 years, female, Canada, elbow level, acquired-trauma, passive hand (occasional user)]
The extent of funding varied internationally in adult but not child populations. Of the adults who participated in this survey, 66% of the 29 Canadians and 33% of the 33 Americans were fully reimbursed for their prosthetic costs (p=0.021). There were no statistically significant differences between the two groups in terms of gender, level or type (uni- or bilateral) of limb absence and occupation status. However, the American sample had a greater proportion of amputations (p=0.012). The observed trend persisted when comparing only individuals with acquired limb absence from these two countries (p=0.02).
C. Role of affordability in prosthesis selection and wear
Prosthesis selection
Among the 187 participants who reported on factors influencing the selection of their prosthesis, 47% (n=88) reported cost to be influential in their decision. Of those who considered cost a factor, 30% (n=20) were fully funded as compared to 74% (n=28) who were not fully funded (p<0.001). Funding policies specific to different agencies and rehabilitation hospitals often dictated prosthesis selection. In explaining why a specific prosthesis was chosen, participants noted the following:
‘Voc Rehab [Vocational Rehabilitation] said I had to get it if they are paying for it.’ [#127: female, 40 years, USA, elbow, acquired-trauma, body-powered hook (non-user)]
‘The myo’s [myoelectric prostheses] are exceptionally expensive and not covered by insurance. I have now been in the process of getting another prosthesis for 3 years; and it seems as though it will never be a possibility.’ [#837: female, 25 years, USA, trans-radial, congenital, myoelectric hand (full-time user)]
Evidently, prostheses are sometimes selected based on affordability as opposed to personal goals or needs. Policies restricting the types of prostheses that are funded may limit choices for some individuals. For example, passive devices, considered by some funding agencies to be for cosmetic purposes only, are sometimes not supported despite functional and psychosocial advantages reported by users.
‘Coverage, it is NOT cosmetic, I can not tie shoelaces or prepare supper if I do not have one.’ [#212: female, 42 years, Canada, trans-radial, congenital, myoelectric hand (full-time user)]
‘I wear my cosmetic prosthesis all the time because I have more confidence with it on. I never go out without it – it’s psychologically VERY important to me. If I didn’t have it on, unfortunately you get stares and people treat you differently. Therefore to avoid that, I wear it all the time’ [#233: female, 36 years, Canada, trans-humeral, congenital, passive hand (full-time user)]
Individuals who must choose a single prosthesis sometimes struggle with the tradeoffs that ensue.
‘I moved from myoelectric to passive – I HATED to lose the function, however it was most inconvenient to have to charge battery every night (particularly if you went anywhere). Plus, I wanted to be able to wear one that looked real and I could swim with.’ [#559: female, 48 years, Canada, trans-radial, congenital, passive hand (full-time user)]
In contrast, the opportunity to avoid these sacrifices by obtaining multiple devices is much appreciated.
‘I did everything possible with my myoelectric – that arms like my best friend. haha. and I still do I’m just glad I’m able to have one and of course my passive arm so I can look chic.’ [#182: female, 26 years, Canada, partial hand, congenital, myoelectric hand (full-time user)]
Of the 109 participants who reported information on their prosthetic funding, 42% owned multiple devices, most commonly passive hands (32%, n=35) and activity-specific devices (24%, n=26). Of the participants with access to multiple devices, 49% (n=34) had full financial support compared to 28% (n=11) without (p=0.027).
Prosthesis wear
Of the 71 non-wearers in this study, 48% considered cost an influential factor in the decision not to adopt prosthesis use. Self-reported quality of life was significantly higher for individuals whose decision not to wear a prosthesis was independent of financial cost (p=0.005).
The financial support available for routine repairs and maintenance can be as important in facilitating continued use of the device as in its initial provision.
‘Insurance paid for initial pros. [prosthesis], but the deductible is so high that I can’t afford replacement or repairs.’ [#602, male, 61 years, USA, trans-radial, acquired-trauma, body-powered hook (part-time user)]
Of the 149 participants who reported reasons for non-wear, 34% cited ‘fear of damage’ as a factor in the decision to wear or not wear a prosthesis on any particular day. For individuals who rely heavily on their prosthesis for daily functioning (e.g. those with bilateral limb absence or individuals such as farmers who require the prosthesis to sustain their livelihood), fear of damage, prosthesis failure and delays in repairs can significantly hamper activities and participation. The ability to obtain multiple prostheses to ensure functional continuity in case of unexpected breakdowns is desired.
‘more understand[ing] from insurance companies. realizing the ongoing required maintenance... and the associated cost. the importance of backup – spare parts – for a bi-lat [bilateral] amputee.’ [#95: male, 60 years, USA, trans-radial/wrist (bilateral), acquired-trauma, myoelectric hand (full-time user)]
Lastly, a single prosthesis cannot be expected to last forever. Mechanical breakdowns and/or changes in body shape and size may necessitate its replacement. Growing children require frequent re-fittings and typically require a new device every two years. 21 Poor or delayed fittings can lead to discomfort and abandonment of the device.
‘What made me stop wearing my prosthesis was that my arm would get stuck in it. Moreover, it would leave itchy imprints in my skin after a full day at school. This was because I was still growing, but turned me off to wearing it.’ [#225: male, 22 years, USA, trans-radial, congenital, myoelectric hand (non-user)]
As an individual ages, their personal needs may also change (i.e. the functional needs of a child may be very different from those of a middle-aged adult or a retired individual). As such, it is important to ‘recognize that one single prosthesis purchase is NOT a lifetime solution.’ [#108: male, 62 years, USA, trans-humeral, acquired-trauma, body-powered hook (full-time user)]
Discussion
Key findings
A. Direct costs of prosthesis wear
The analyses presented in this paper suggest that, even in industrialized nations, the resources enabling procurement and maintenance of upper limb prosthetics in line with user needs are not equitably accessible. While many individuals receive excellent support, others are limited in their ability to optimally and expediently procure and maintain a suitable prosthesis. Direct costs of prosthesis wear can be substantial for these individuals, and range from hundreds to thousands of dollars per year.
B. Variations in prosthesis funding
Access to financial support varies from individual to individual and depends on a mixture of factors. Individuals of older age, or with higher or lower levels of limb absence, may have greater difficulty accessing the funds required to support their prosthetic needs. From the qualitative data presented, it is evident that access to enabling resources is impeded by the convoluted policies dictating their management and distribution. Individuals are often challenged to prove their need for the device, which can be difficult, particularly when assessing psychosocial value added. These findings are in line with previous studies of lower limb prostheses 22 and of assistive technologies in general. 23,24
C. Role of affordability in prosthesis selection and wear
Inequitable access to enabling resources for prosthetic management can have serious functional, emotional and physical implications that lower quality of life. For individuals who do choose to wear a prosthesis on a regular basis, the level of need associated with the device is generally extremely high. 19 Although prosthesis use is certainly not the optimal solution for everyone, there are a number of potential dangers to non-use, particularly when it is driven by insufficient access to enabling resources, as opposed to lack of functional need. Most notably, constant use of the contralateral limb over time may lead to injuries and secondary health concerns 2 which are in themselves associated with high medical costs. Mechanisms by which poor access to enabling resources may drive prosthesis abandonment include:
Future directions
Research and development of technologies, outcome measures and policies is needed to further improve access to enabling resources for upper limb prosthetics. These strategies are described below.
A. Technology development
Initiatives to reduce the costs of high quality prosthetic limbs are paramount. The price of prostheses and their maintenance could be reduced by use of high-strength, low-cost injection moulded plastics to construct prosthetic components (e.g. Touch Bionics iLimb 25 or the LCKnee 26 ), modular designs to facilitate repairs and enable interchangeable multi-purpose terminal devices, 25,27,28 and rapid prototyping along with CAD/CAM (computer-aided design and manufacturing) to improve efficiency and repeatability of prosthetic services such as size matching and fitting. 29,30 Video-conferencing could facilitate access to non-local experts for more efficient centralized manufacturing and servicing. Expanding market opportunities and thereby increasing production volumes may also lead to decreased costs. Potential areas for technology transfer include virtual reality and haptic environments for training simulations, handling of hazardous materials and autonomous laboratories, to name a few.
B. Measurement of outcomes
Prostheses range in price from a few hundred dollars for a non-cosmetic passive device to tens of thousands of dollars for a sophisticated myoelectric hand. As a result, the healthcare system is understandably under pressure to empirically justify prescription of premium prostheses in terms of functional outcomes and quality of life. Mitka 31 suggests that improvements in funding coverage must be compelled by substantiative evidence supporting the health benefits gained through prosthesis use. Continued efforts directed towards evidence-based evaluation of prosthetic practices and outcomes will provide the springboard for policy change. Continued development and use of standardized outcome measures to assess function and quality of life may enable greater focus on multi-centred, collaborative efforts for evaluation of practice and generation of a strong evidence base.
In evaluating outcomes, it is also important to give some thought to the questions of importance to ask. For example, perhaps the true question of interest regarding enabling resources is whether those individuals denied prosthetic options, or inconvenienced by challenges accessing required resources, reach an equal quality of life and level of function as those readily provided with these enabling resources. Preliminary evidence presented in this study suggests that quality of life is negatively impacted when cost and availability of resources influence health choices: in this case, the decision to accept or reject a prosthesis. Further research is needed in this regard, particularly among low socioeconomic populations.
C. Policy development
There is an absence of clear, consistent and central accountability mechanisms, which are vital in advancing the agenda for inclusive and more integrated services. 32,33 Indeed, the breadth and scope of funding programmes ‘can be a major barrier to accessing assistive devices’. 23 Yet very little research has been conducted on the gaps in health services and policy that may be influencing access to assistive devices. Using a disability lens on government policies, programmes and legislation could shed light on existing gaps and inequalities and assist in breaking down current barriers. 24,33,34
Merits and limitations
Methodologically, the most interesting attributes of this study are (1) the diversity of participants recruited from both community- and hospital-based centres, (2) the mixture of quantitative and qualitative data used to describe the funding experiences of this population, and (3) the large quantity of qualitative data examined (over 25,600 words from 175 participants, of which about 10% was related to prosthetic costs and funding). As such, this study presents a unique explorative and descriptive portrayal of the funding experiences of individuals with upper limb absence. While several studies have qualitatively explored the experiences of individuals with primarily lower limb absence, 22 ,35–39 relatively few have focused on the upper limb, 40 and none, to the authors’ knowledge, on funding issues. In line with the strengths of qualitative research, 41 this paper is intended to present data that is responsive to stakeholders’ needs and interests and to provide depth and richness to our understanding of individual experiences. The addition of quantitative data lends precision to the narratives. Mixed methodology studies, such as this, may lead to a more comprehensive understanding necessary to inform theory and practice. The benefits of mixed-method research are expounded in an excellent review by Johnson and Onwuegbuzie. 41
Several limitations to this study were accepted in order to obtain a broad overview of a diverse, international sample of individuals with upper limb absence. It is important to view the results in the context of these limitations:
It is difficult to ascertain the accuracy of the quantitative data collected with respect to prosthetic costs and maintenance. While the reported costs seem reasonable, there is the potential for recall bias. As such, the numbers presented should be regarded as estimates that would require further verification from manufacturers, healthcare providers and funders. The survey was widely distributed online in order to access individuals who may no longer be affiliated with a rehabilitation centre through web-based community resources. Although electronic surveys are likely equivalent to conventional media (i.e. telephone, mail) with regards to test–retest reliability and internal consistency,
42,43
some sampling limitations are evident. A number of strategies were adopted to mitigate these limitations, including IP address tracking, data consistency analyses and promotion through local collaborators. It is important to note that the sample population was self-selected, as is often the case in consumer-based surveys, making it difficult to assess the extent to which the opinions expressed are reflective of the population as a whole. To quantify possible sampling biases, we compared the demographic distribution of this study’s electronic respondents from the United States (n=92) to that of a large-scale epidemiologic study (n=2477) also conducted in the United States in 1996.
44
No statistically significant differences were observed with respect to age, prevalence of trans-radial limb absence or origin of limb absence. Further, the prevalence of electric hands and body-powered hooks was not statistically different. In this study, 51% of participants were male, as compared to 63% in the Atkins el al. study (p=0.02).
44
However, previous research has found no association between gender and Internet access.
45
As of 2005, 68% of adult Canadians had access to the Internet for personal use.
46
In 2003, 60% of adults in the USA reported Internet access.
47
It is possible that Internet-based surveys may exclude low-income individuals, and hence that the funding inequalities emerging in this study may be under-represented. Persons with disabilities have also been found to be less likely to use the Internet than the general population,
48
which may also have led to under-reporting of access inequalities in this study.
Conclusions
Prosthesis funding is neither homogeneous nor transparent and can be influential in both the selection and use of a prosthetic device. Targeted strategies are needed (e.g. through technology development, outcomes measurement and policy change) to ensure that individuals with upper limb absence are provided equitable access to the enabling resources needed to reach and sustain an optimal quality of life. Ensuring equal access to enabling resources and assistive technologies is essential to promote function, activities and participation for quality of life and well-being.
Footnotes
Funding
This work was supported in part by Holland Bloorview Kids Foundation, the Natural Sciences and Engineering Research Council of Canada and the Canada Research Chairs Program.