
Abstract
Background:
The Activity Time-Use Intervention (ATUS) is a novel occupational therapy theory informed intervention for adolescents with emerging mental health difficulties. Designed to empower 16- and 17-year-olds to reflect on their time use to achieve a healthier balance of activity within the context of their daily lives. Acceptability to healthy adolescents is explored in preparation for testing with the more vulnerable target population.
Aim:
To explore the acceptability of the ATUS intervention to healthy adolescents when delivered in a mainstream secondary school.
Method:
A pragmatic, non-randomised, mixed-method, pre- and post-, single-group, exploratory study. Analysis involved descriptive statistics and template analysis informed by Sekhon’s theoretical framework of acceptability.
Results:
The ATUS was successfully delivered to healthy students. Nineteen sub-themes were identified based on the seven constructs of Sekhon’s theoretical framework of acceptability. Feedback was positive, highlighting areas for modification. Online completion of measures ranged from 17 to 99.4% and took on average 12 minutes to complete. Change in well-being scores was most frequently observed.
Conclusion:
The ATUS is deliverable and acceptable to healthy adolescents; however, some components should be reviewed before delivering in the target population, and further work is required before feasibility testing.
Keywords
Introduction and literature review
Internationally, the prevalence of reported mental health problems among adolescents has increased (Patel et al., 2018). Minimising the impact of poor mental health or preventing it completely requires early interventions (Sawyer et al., 2012) that can address the influence of multiple inter-related personal, social and environmental factors (Mei et al., 2020; Patel et al., 2018). The role that daily activities and lifestyle factors play in causing, preventing and managing mental health problems is a research priority identified by young people, parents, teachers and professionals (McPin Foundation, 2023). Evidence suggests that the daily choices young people make in the context of their own environment, about what combination of activities to do, and for how long, are likely to affect their mental health and are therefore important (Parsonage, 2022). Indeed, evidence increasingly supports an association between young people’s engagement in daily activities and their mental health (Bowman et al., 2020). This knowledge can be used in interventions to improve mental health and mental well-being.
Conceptually, the terms ‘occupational choice’ and ‘occupational balance’ describe the theoretical and empirical exploration of ideas related to choosing daily activities, and the health impacts of chosen activity combinations on the individual (Eklund et al., 2017). Research has also suggested that enabling the development of autonomy, competence and connectedness during adolescence has positive health effects (Ryan and Decci, 2000). A scoping review of the peer-reviewed academic literature found no reported activity-focused interventions underpinned by an understanding of occupational choice and occupational balance, and which specifically target adolescent time-use in those aged 11–17 years of age to improve mental health (Parsonage-Harrison et al., 2022). The Activity Time-Use Intervention (ATUS) was developed to address this research gap and specifically targets adolescents aged 16–17 years in full-time mainstream education (Parsonage-Harrison and Dawes, 2024; Parsonage, 2022). Developed and evaluated with young people, the intervention aimed to empower adolescents to develop the competencies necessary to make autonomous occupational choices leading to a healthier balance of daily activities and improved mental health.
The Medical Research Council guidance for developing complex interventions provides a framework for the appropriate transition from intervention development to feasibility testing (Skivington et al, 2021). The 8-week ATUS intervention manual was systematically developed using the Intervention Mapping framework but had not previously been tested (Bartholomew-Eldredge et al., 2016; Parsonage-Harrison and Dawes, 2024). It is important to identify and understand any possible risks arising from the delivery of an intervention in healthy controls to ensure harm minimisation ahead of piloting with the target population. The intervention targets a highly vulnerable group, those aged 16–17 years of age, who are not yet in receipt of a clinical diagnosis or mental health services. Who may be presenting with early warning signs of an emerging mental health difficulty, or who may have been identified as ‘at risk’ of developing a mental health difficulty. Young people experiencing difficulties are frequently identified through school, on waiting lists, and are not in receipt of specialist mental health services. Therefore, it is essential to ensure the safety, acceptability and feasibility of the intervention in healthy controls before further delivery in more vulnerable populations. This study aimed to explore the acceptability and partially explore some feasibility aspects of the ATUS intervention to healthy 16- and 17-year-olds when delivered in a school environment. The study had three objectives. First, to deliver the ATUS intervention and explore its acceptability from the perspective of 16 and 17-year-olds in secondary education. Second, to identify barriers and facilitators to delivering the ATUS intervention in a school environment, and finally, to explore the acceptability and practicality of administering the planned outcome measures via an online platform.
Methodology
A pragmatic, non-randomised, mixed-method, pre- and post-, single-group, exploratory study, to explore the acceptability and some aspects of the feasibility of the ATUS intervention in a school environment with healthy participants. The purpose of which is to address uncertainties ahead of a future acceptability and feasibility pilot with adolescents who have mental health difficulties.
Study setting and study criteria
The study setting was a mainstream secondary school, situated in an inner-city location, known for significant economic deprivation and high ethnic diversity. Participant inclusion required students to be in their first year of post-GSCE education and aged between 16 and 17 years. Participants were required to understand and speak English to participate fully in the intervention. Because of the high vulnerability of the target population and the limited prior testing of this intervention with adolescents, the decision was taken to exclude students known to be experiencing active mental health difficulties or currently accessing services for any mental health difficulty.
Delivery of the intervention
The intervention was delivered according to the manual by the main author, an occupational therapist, with clinical experience of working in mental health settings and delivering interventions. As the developer, no additional training was required to deliver the intervention. The 8 group sessions, each of 50 minutes, were delivered face to face in the school library or computer room at the end of the day. The school gatekeeper was on-site. The intervention consisted of eight sessions designed to be delivered weekly. Session topics include exploring skills and developing the occupational repertoire, Balancing occupations and time, Volition and valuing occupation, Managing the situational context, Managing occupational choice, Appraising occupational choice and developing the occupational self. Each session addresses specific objectives, building towards the overall intervention outcomes to improve their balance of daily activities, to make better personal choices, and improve related occupational performance. It is theorised that achieving these objectives will result in improved mental health and well-being. Full details of the intervention’s development and session schedule are published in another paper (Parsonage-Harrison and Dawes, 2024). No personalisations were pre-planned.
Recruitment and sample size
The first author approached a school with whom a prior relationship was already established through earlier Patient Public Involvement (PPI) work. The school agreed to participate. The sample size estimate of 8–12 students was based on the maximum number for appropriate delivery of the intervention and qualitative principles of sample size. Students were recruited via an in-person presentation delivered by the first author during a year 12 assembly. The presentation detailed key study information, which was followed by the provision of an information sheet including email details of how to opt into the study. All participants gave informed consent via an online platform; parents of students were also provided with information about the project before pre-intervention self-report measures were completed. Participants were also compensated for the time taken to complete the pre- and post-assessments. Following agreement with the school, students were paid £25 for each part of the assessment completed e.g. Prequestionnaires, pre-interview etc.
Data collection and outcome measures
Three types of data were collected to explore the acceptability of participating in the intervention, the acceptability and feasibility of completing the measures, and the feasibility of delivering the intervention.
Qualitative data collection
A research assistant and pre-reg occupational therapist student conducted semi-structured interviews with participants to understand expectations (pre-intervention) and experiences (post-intervention) of participating in the intervention. Interviews were conducted online, and were audio recorded and lasted no longer than an hour. Interview Recordings were anonymised, transcribed verbatim and checked for accuracy. A topic guide is available in Supplemental Appendix 3.
After each intervention session, the facilitating occupational therapist wrote a reflective log documenting the experience of delivering the intervention, noting any deviations from the manual, attendance, perceived engagement with the task and other noteworthy observations resulting from delivering the intervention, such as concerns about student safety and reflections on completion of tasks, group interaction around tasks etc.
Self-report measures
Participants were asked via email to independently complete four self-report measures via the online platform Qualtrics prior to both the pre- and post-online interviews. The measures were replicated in a digital format closely aligned to the originals, but placed sequentially so they could be completed online as one single questionnaire. The usual instructions and guidance on how to complete the questionnaire was also retained. The research assistant provided time for participants to complete the online questionnaire at the start of the interview if required. Completion of measures was not reviewed at the time of the interviews. The measures were the Short Warwick-Edinburgh Mental well-being scale, The Strengths and Difficulties Questionnaire (SDQ s11–17), the Kidscreen-10 and the Children’s occupational self-assessment (COSA). A summary of the measures is available in Table 1.
Measures summary.
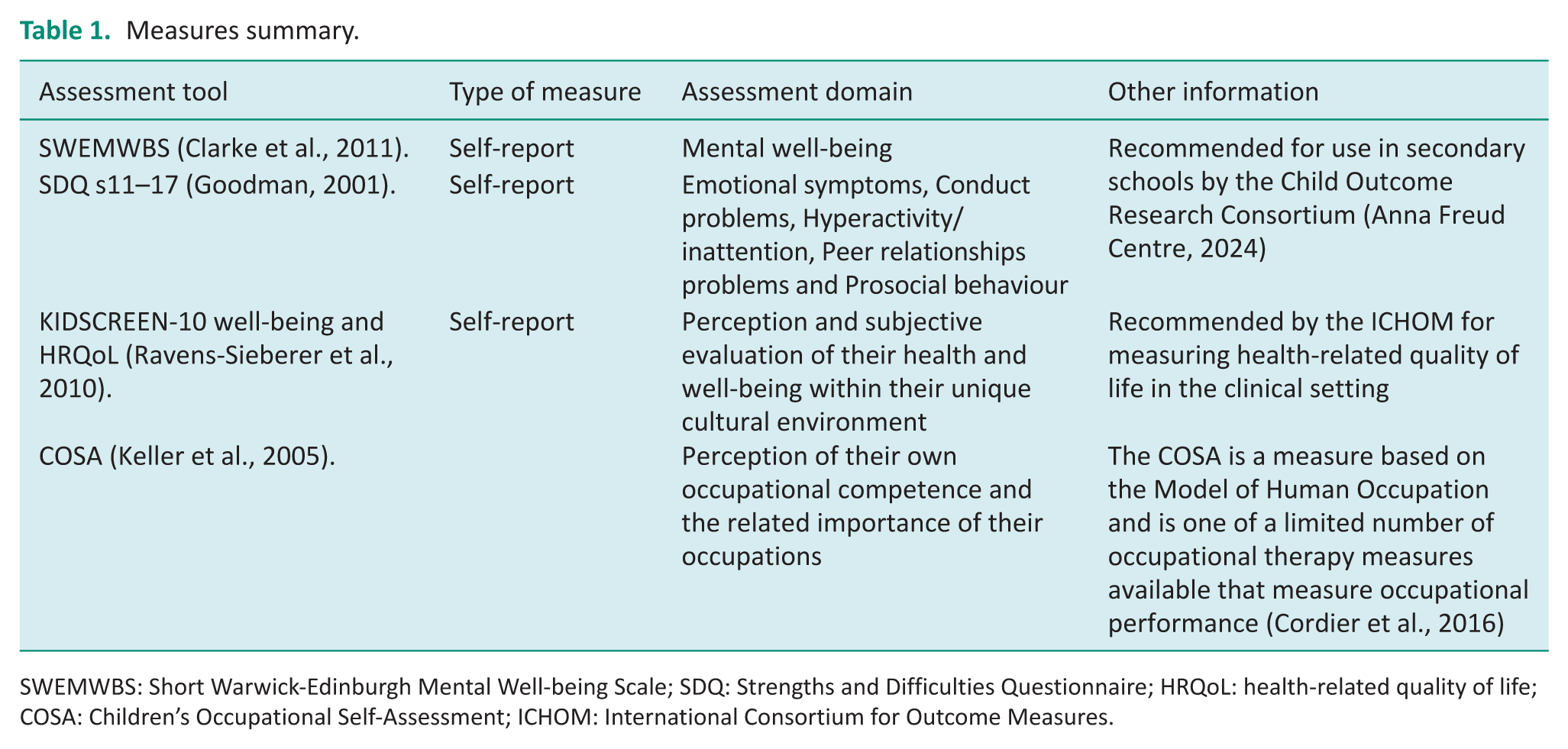
SWEMWBS: Short Warwick-Edinburgh Mental Well-being Scale; SDQ: Strengths and Difficulties Questionnaire; HRQoL: health-related quality of life; COSA: Children’s Occupational Self-Assessment; ICHOM: International Consortium for Outcome Measures.
Service user involvement
Two young people with lived experience of mental health difficulties were recruited to have oversight of the project and inform further development of the intervention. They met weekly with the occupational therapist following the delivery of the intervention. Experiences of delivering each session were discussed. Ways to improve sessions and address issues were identified and amendments to the manual were agreed.
Assessment of safety
Safety of the intervention was assessed using qualitative reports from students and therapist delivering the intervention and by the record of untoward events.
Analysis
A concurrent pragmatic mixed-method approach was used to conduct the analysis. The primary analysis focused on the qualitative data. Template Analysis was used to analyse the interview transcripts (Brooks et al., 2015). In line with template analysis, a priori template was constructed using the theoretical framework of acceptability criteria identified by Sekhon et al. (2017) following their systematic review of the literature. The criteria include affective attitude, burden, ethicality, intervention coherence and perceived effectiveness. The interview data were read for familiarity, then coded according to the a priori template. The template was modified according to the codes that arose, primarily resulting in the sub-themes. Once complete, the full text was reviewed again to ensure that all data were appropriately coded and to finalise themes and subthemes that constitute the template (Brooks et al., 2015). Researcher logbooks were also reviewed using thematic analysis principles for key ideas and information regarding the practicality of the delivery and the acceptability of the intervention. Finally, responses to self-report measures were downloaded from Qualtrics and analysed using descriptive statistics to identify the time taken to complete measures, the viability and completeness of the obtained data.
Ethics
The study was approved by Oxford Brookes University Research Ethics Committee (UREC No: 231696 on 13 September 2023). A school staff member, acting as a gatekeeper, managed all school-related project practicalities, compliance with school safety and safeguarding requirements, and General Data Protection Regulation (GDPR) rules and managing site access. Procedures were in place to manage and report untoward and risk incidents.
Results
Following the school assembly, 9 students out of approximately 70 students expressed an interest in participating. Eight consented to participate, n = 1 did not without giving a reason. All 8 (n = 5 female, n = 3 male) completed the pre-intervention assessments 3 (17.5%) were born outside of the UK, 4 (50%) identified as black or black African, 1 (12.5%) Asian, 2 (25%) White and 1 Other (12.5%).
The intervention sessions began in December 2023 and finished February 2024. The 8 sessions took place over an 11-week period due to school holidays. Sessions were held after the end of the official school day on campus, primarily on Tuesdays at 15:15. One consented student dropped out without giving a reason. Seven students started the group. Overall group attendance was 80%. Four participants attended all eight intervention sessions, n = 2 missed one session, and n = 1 missed three sessions. The reasons given for missing sessions were a dentist appointment, additional maths lessons, and a pre-existing volunteering commitment. No adverse event or untoward incidents were reported and no safety concerns were identified by those involved.
Findings from the interview
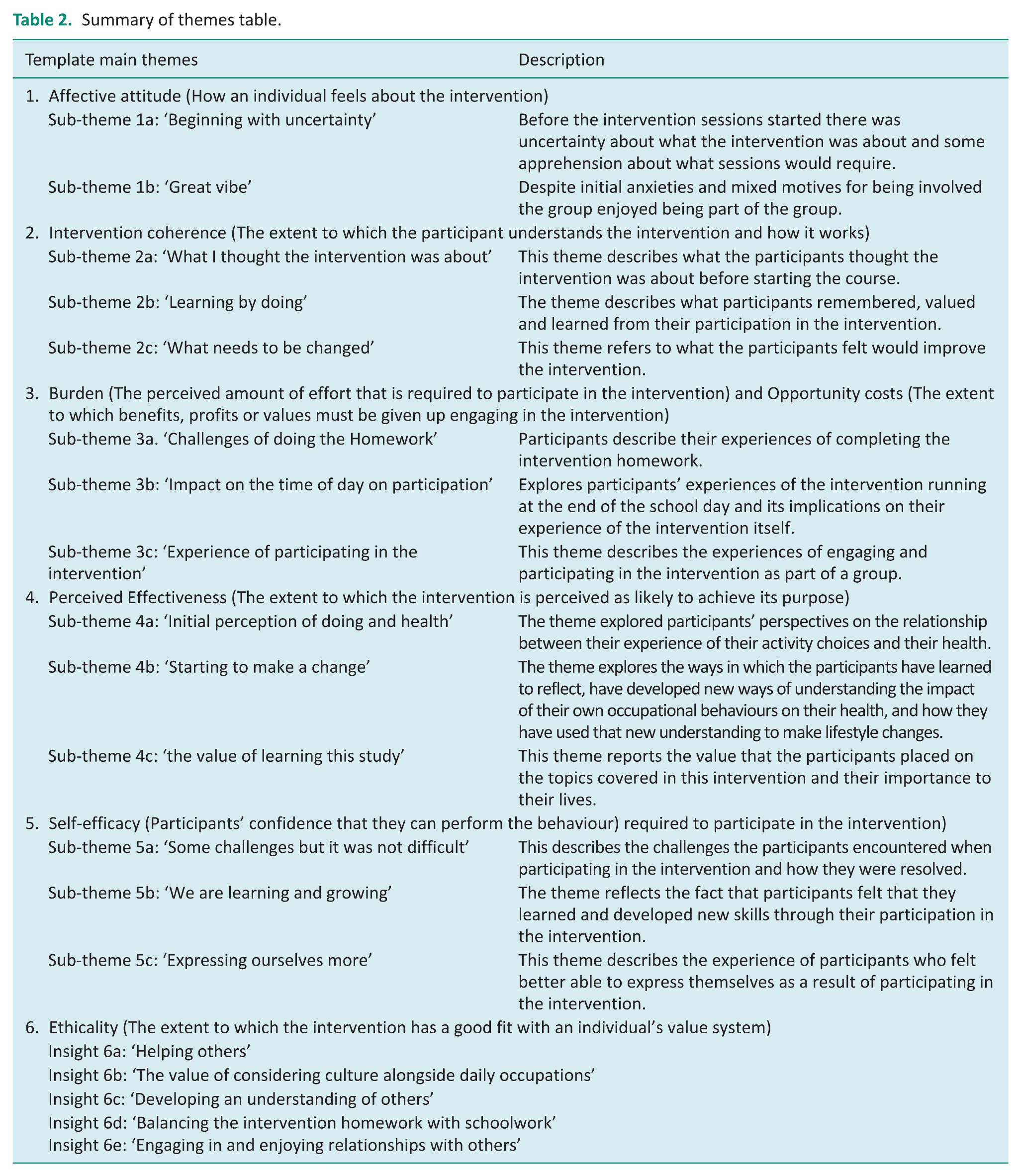
A template was created using Sekhon’s categories. Information related to burden and opportunity costs overlapped, so was combined into one category, resulting in six main themes. The text under each main theme was explored in more detail, resulting in 19 sub-themes. See Table 2, Summary of themes and Supplemental Appendix 4 for a detailed summary.
Summary of themes table.
Affective attitude
Two themes were identified that describe how participants felt about the intervention, known as Affective attitude (Sekhon et al., 2017). These themes included ‘Beginning with uncertainty’, and ‘A great vibe’.
The first sub-theme was ‘Beginning with uncertainty’, participants described their initial uncertainty and anxiety about what the intervention was and what it would entail. Despite the initial anxieties and mixed motives for being involved, the participants engaged and enjoyed the group. The second sub-theme, ‘A great vibe’, describes the factors that contribute to how it felt to be part of the group. The sub-theme ‘a great vibe’ was shaped by the intervention activities and the group environment. Activities were enjoyed and provided an opportunity to share about their occupations, helping to develop inter-participant relationships. Participants also described feeling safe and comfortable sharing.
Intervention coherence
Intervention Coherence describes the extent to which the participants understand the intervention and how it works. Before starting the course, it was evident that participants had different understandings of what the intervention was about, but by the end, they demonstrated a comprehensive understanding. The participants were largely positive about the intervention, but did highlight areas before improvement.
Sub-themes were identified: ‘What I thought the intervention was about’, ‘Learning by doing’ and ‘What needs to be changed’.
‘What I thought the intervention was about’ concerns different interpretations participants had about the intervention, despite all understanding from the school presentation and information sheet that the intervention was about adolescent’s mental health. Only one participant correctly anticipated that, through the intervention, they would consider the balance of their daily activities and their connection to mental health. ‘Learning by doing’, concerned prescribed activities that participants remembered, valued and learned from, that shaped their understanding of the intervention and what it was designed to achieve. The activities recalled and valued differed between participants. However, through engaging with the prescribed activities, they gained a more comprehensive understanding of what the intervention was designed to achieve and began to think about what they could do differently. ‘What needs to change’ Participants were mostly positive about content, sequencing and delivery, but a few struggled to understand some content before explanations were given. Three participants suggested that more time is required to complete the activities.
Burden and Opportunity costs
Burden and Opportunity costs are reported together because of an overlap in the themes and consist of three sub-themes. Burden refers to the perceived amount of effort required to participate in the intervention and opportunity costs refer to the extent to which benefits, profits or values must be given up to engage in the intervention.
‘Challenges of doing the Homework,’ while some found that the ‘homework’ (associated with the intervention) was not demanding or difficult, others highlighted the challenge of balancing this with schoolwork priorities, making it difficult to complete. ‘Impact of the time of day on participation’, and possibly ‘activities’. Opinion about the timing of the sessions varied for some; the timing was positive, as it helped to forget about school-related stress, for others, it would be preferable to occur within school time, and another was initially ambivalent but later expressed that it was a good time. ‘Experiences of participating in the intervention’. Some activities were described as a little challenging for various reasons, but overall report that they were valued and even enjoyed, influencing attendance. Participants did not report being upset by the activities or the challenge they presented.
Perceived effectiveness
Three sub-themes were identified: ‘Initial perceptions of doing and health’, ‘Starting to make a change’ and the ‘Value of learning this stuff’.
‘Initial perceptions of doing and health’ participants expressed a variety of views about how the activities they do on a day-to-day basis affect their health. Some expressed views that it did affect their health, while others did not consider there to be a connection between occupational choices and health. ‘Starting to make a change’ describes the effect of the intervention and the lifestyle changes participants made to improve their mental health. Participants described creating a space for reflecting on time use, choices to do things differently in daily activities, recognition of personal problem areas such as sleep and opportunity for personal growth. ‘Value of learning this stuff’. Participants valued the time engaged with the intervention. The content and deeper exploration of the topics covered were valued and thought to be often ignored. There was value in being genuinely asked about their activities, which students felt were not often explored at school, despite it being helpful. Participants valued learning about themselves, gaining other perspectives from peers and adults, understanding the topic in a helpful way and making changes.
Self-Efficacy
The sub-themes identified on participants’ confidence to participate in the intervention were ‘Some challenges but it was not difficult’, ‘We are learning and growing’ and ‘expressing ourselves more’.
‘Some challenges but it was not difficult’, refers to participants who, at a personal level, encountered some sense of challenge during the intervention at some point. Difficulties included understanding what was required in a task, comprehension of the topic content or terminology, unfamiliarity with personal reflection, homework and being in a group. Despite the difficulties, participants felt supported and able to overcome challenges. ‘We are learning and growing’ refers to the participants’ descriptions of how, through their participation, they have learned new things and feel that they have grown personally. While this varied between participants, examples given were gaining social skills, becoming braver, learning the importance of rest and growing personally through new learning. ‘Expressing myself’ described how some participants felt better able to express themselves because of participating in the intervention.
Ethicality
Ethicality is the extent to which the intervention has a good fit with participants’ value systems. Participants were positive about the intervention, but responses highlighted a few ethical-related conflicts. First, for some, a primary reason for participating was about helping others, rather than because of any perceived self-benefit. Yet participants went on to report the value of the intervention and how they found it personally helpful (See Self-efficacy).
The ethical insights to emerge were the ‘value of considering culture alongside daily occupations’, ‘developing understanding of others’ insight about the burden of ‘balancing the intervention homework with schoolwork’ and the fifth insight was ‘engaging in and enjoying relationships with others’. The participants’ interviews suggest that time with peers was something important and they valued the opportunity to get together as a group.
Researcher reflections
Thematic analysis of the logbooks recorded after the session highlighted the following insights about the delivery of the intervention. The insights are divided into three groups; Relationships, Practicalities and Other factors which are described below.
Relationships
Some participants knew each other, and some were friends. However, over the course of the intervention, participant relationships seemed to be strengthened and, in some cases, developed, which was something that they valued. In general, at the start of the intervention, the male participants were more confident.
Participants’ expectations of the facilitator and time constraints were felt by the therapist as a challenge in developing rapport and the usual personalisation aimed for. Giving time and space for deeper conversations related to the activity was found to be important for rapport building.
Practicalities
The main practicality issue was time. It was a challenge to complete all the planned activities in the time available and at the desired depth, which was exacerbated by an often-delayed starting waiting for participants to arrive (10–15 minutes). Challenges of delivering the intervention in a school included unplanned interruptions and internet access issues. Homework was typically not completed, and only one student returned their time diary. Mood and energy levels varied widely over the weeks of the intervention that affected engagement and motivation to participate in the group. It was not always obvious from observation if the participants were enjoying or perceiving benefit, but participants’ written feedback after each session was highly positive about the intervention.
Other factors
An interesting factor to emerge was the discussions related to occupation and cultural issues. Talking about this among this diverse group was valued, with individuals from different cultures being interested in seeing similarities in expectations.
Completion of measures
Seven participants completed the post-intervention assessments. The mean time to complete the online questionnaire pre-intervention was 155 minutes (range: 346–67,020). Post-intervention was 11 minutes and 35 seconds (range: 436–1148) to complete. Qualitative responses suggest that the participants did not find the online questionnaire difficult to understand or complete and that the time to complete was acceptable, though it appears that not all completed it at the first sitting.
Overall completion of measures, both pre- and post-intervention, was 1013 (75%) out of 1346 items. Online completion of individual measures ranged from 0% to 100%, with the COSA being the most poorly completed (See Supplemental Appendix Table 1). The combined completion of individual measures was as follows: Warwick-Edinburgh Mental Well-being Scale (WEMWBS) is 93% (Pre 100% and Post 86%), and SDQ was 92% (Pre 99.4% and Post 85%). Due to an administrative error on the Kidscreen10, only eight questions were completed. Completion of the 8 items was 94% (Pre 100% and Post 88%). The largest percentage of the missing data was the completion of the COSA. The COSA was modified between rounds to improve the clarity of the online formatting, and post-intervention completion improved to 65% despite one participant dropping out.
Outcome measures
On the WEMWBS, 3 participants 42% showed an improvement in their post-intervention mental well-being scores, and 4 (57%) reported worsening scores. Four participants (57%) reported a worsening in their post-intervention SDQ total scores, 2 (29%) showed improvement, and 1 (14%) showed no change in their scores (See Table 3).
Total scores for individual participants.
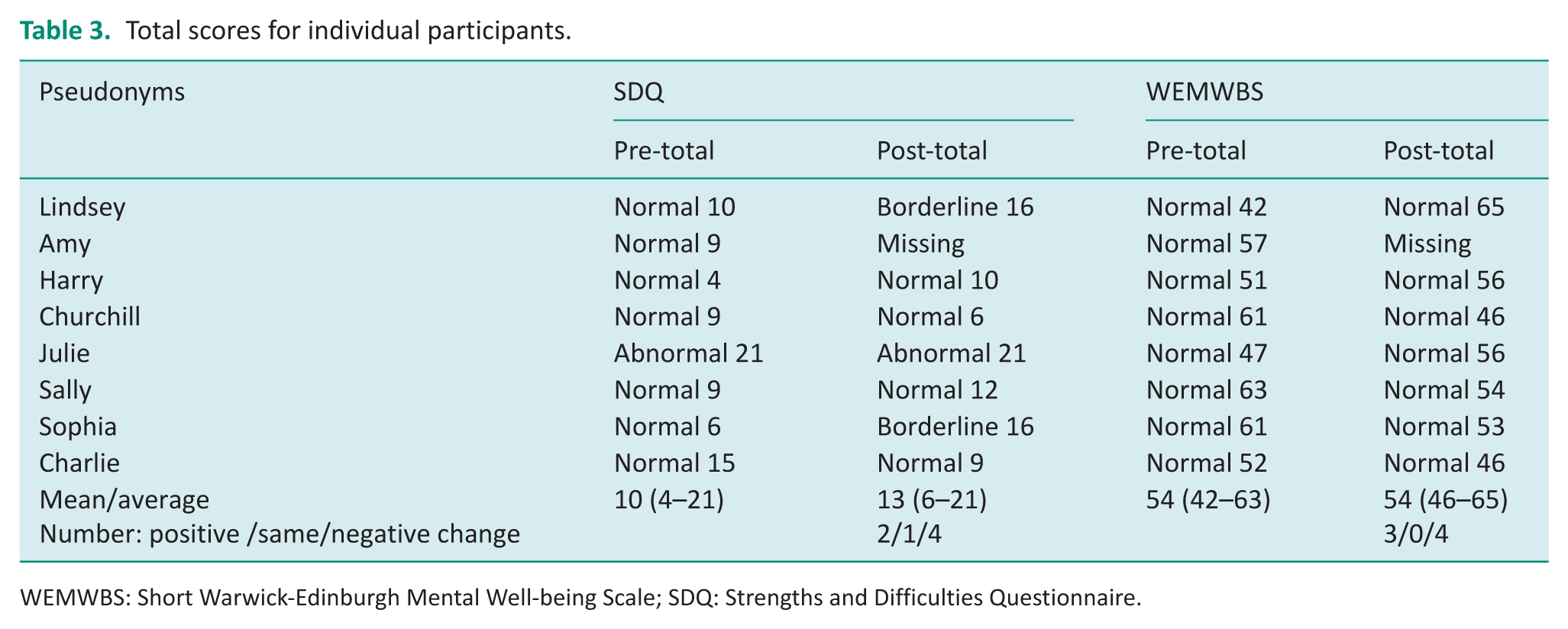
WEMWBS: Short Warwick-Edinburgh Mental Well-being Scale; SDQ: Strengths and Difficulties Questionnaire.
The Kidscreen10 suggests that on item 11, 63% of the group reported that their health was the same or better post-intervention. The individual kidscreen10 questions suggest that the same or improved scores post-intervention concerned feeling less sad (75%), feeling fit and well (50%), feeling energised (50%) (See Table 4 for details). The outcome of the COSA data was not calculated due to the amount of missing data.
Kidscreen10 item scores for individuals.
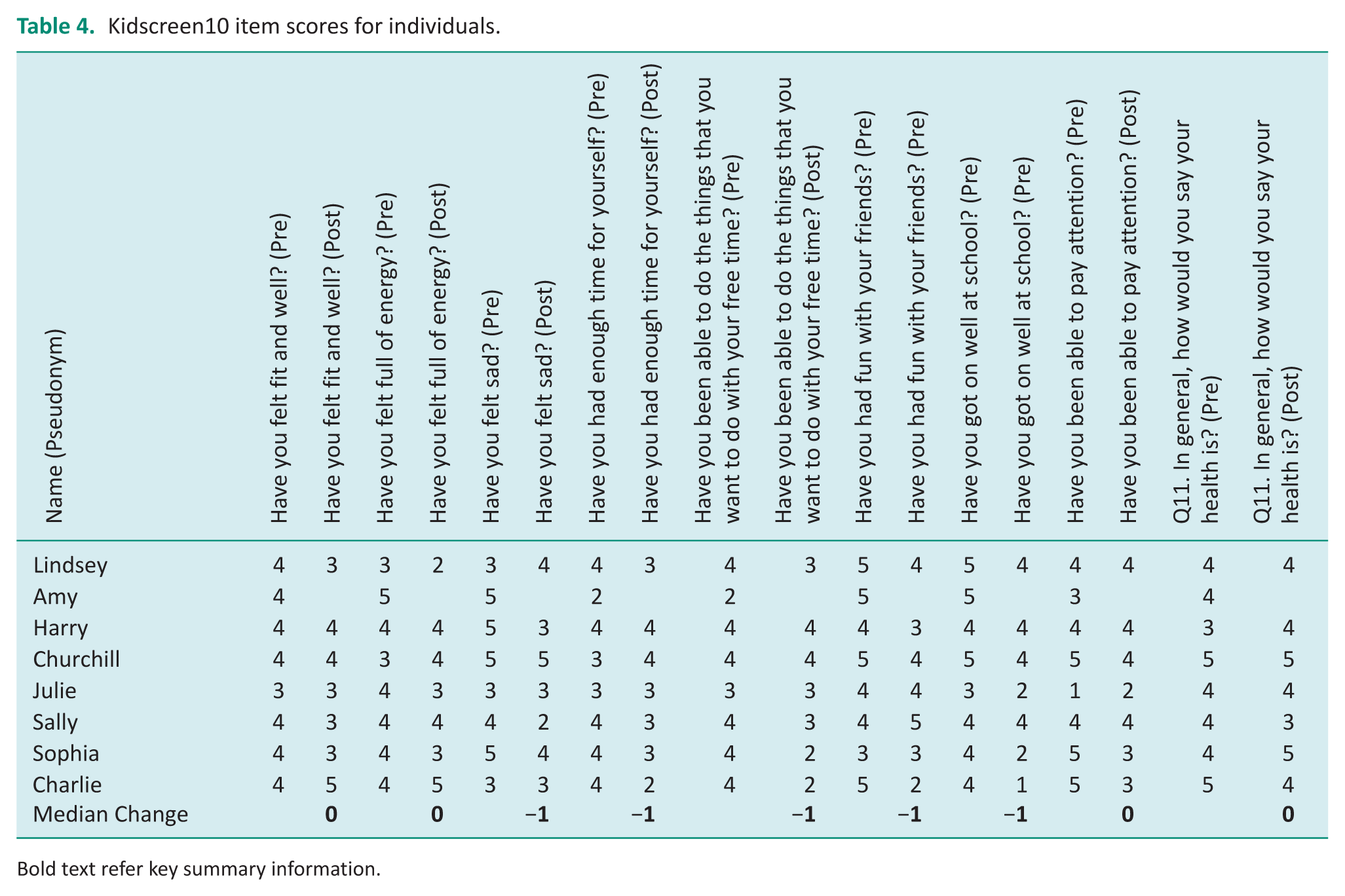
Bold text refer key summary information.
Discussion
This study has successfully described the acceptability of delivering the ATUS in a secondary school environment.
Acceptability of intervention and delivery
Overall, students felt positive about their experience, found the intervention coherent, and perceived it to be effective and valuable. The study successfully recruited participants, but the pre-intervention information could be further developed to improve clarity about the expected outcomes of participation. Although we recruited those without diagnosed mental health difficulties, six out of eight participants reported borderline or abnormal peer problem scores at baseline. Engagement with the intervention was good. Seven students were successfully recruited, and session attendance was 80%. While session attendance is not well reported in adolescent mental health intervention studies, an 80% rate is typically regarded positively (Peycheva et al, 2023). The theme: ‘a great vibe’, was identified as a factor that influenced the participant’s engagement. This included the nature of the activities, the facilitator, the group milieu, group dynamics, the food provided and the fact that friendships existed within the group. These factors and others are known to affect engagement and participation in intervention groups (Steen et al., 2022). It is important that this continues when delivering the intervention in the future. There were no reported adverse events, and no issues arose. This suggests that the acceptability and feasibility of delivering this intervention in a population with mental health difficulties could be considered subject to appropriate assessment and management of the additional associated risks of the target population.
The study has highlighted issues that should be considered ahead of future feasibility testing.
These included difficulties completing the tasks in the time available in the school setting and the variable completion of assigned activities outside of the in-class meetings. The findings suggest that participants prioritised school-based homework and other commitments over the additional tasks, suggesting these were experienced as an additional optional demand or burden that had to be prioritised. Homework is commonly incorporated into psychological interventions, but there is little empirical work around its role, compliance, quality of completion, the factors affecting completion (Kazantzis et al., 2004), or even perhaps the burden it carries. These factors should be reviewed and explored with young people to reduce the sense of burden and enhance the sense of personal benefit. The impact of wider environmental factors on participants’ mood and motivation to engage in intervention tasks varied from week to week. Further exploration of natural variation in mental health and well-being of 16- to 17-year-olds across the academic year could be considered, as it has received little research attention from an occupational perspective. Such knowledge could be used to enhance the intervention.
The delivery of the intervention sessions in the school environment was enabled through a reciprocal and supportive relationship with the school, which allocated a member of staff to oversee the school delivery. These factors have previously been highlighted as important aspects of enabling the successful implementation of an intervention within a school setting (Pearson et al., 2015). Therefore, the cost and time implications of school involvement should be considered when costing and planning to deliver the intervention in the school environment.
An unexpected finding was that the session on ‘managing the situational context’ provided an opportunity for explicit discussions about culture. The participants were from diverse backgrounds and reported that they valued the opportunity to explore differences and similarities in their cultural expectations regarding schoolwork, occupations and how their environment influences their activity choices. The ATUS provided a valued opportunity to reflect and engage in discussion about their shared values. The importance of self-reflection in developing cultural competence is acknowledged within the literature and has the potential to influence healthcare outcomes (Truong et al., 2014). Given the known ethical inequalities within the mental health service and their effect on help-seeking behaviours amongst diverse groups, the intervention manual should explicitly acknowledge and make provision for this discussion where appropriate.
Acceptability and practicality of measures
This study assessed the acceptability of three commonly recommended adolescent mental health outcome measures and one occupational therapy-specific measure. Participants reported the measures were repetitive, but not difficult, and only took on average 12 minutes to complete online. Completion of measures was acceptable, but completion of the COSA was poor even following a revision to the formatting to improve clarity the COSA. Other occupation-focused measures should be considered that more closely align with the intended outcomes of the intervention.
Participants perceived the intervention to be effective, reporting changing at least one aspect of their daily lives and articulating the value of what they had learned, but this was not necessarily reflected in individual scores on the outcome measures. The constructs measured by the Kidscreen-10, the SDQ and the WEMWBS are known to be poorly defined and have a high level of overlap, which may be problematic to both completion and measurement (Black et al., 2023).
Furthermore, it is likely that there may be some natural variation in individual participant scores arising from changes in the academic year, such as increased pressure related to exams and assignments compared with the beginning of the intervention. Indeed a recent systematic review of SDQ studies (Bergström and Baviskar, 2021) distinguished between test-retest reliability (under 31 days) and temporal reliability (over 32 days), concluding that the SDQ total score had good test-retest reliability but poor temporal reliability. The reliability of the measures past 31 days may account for the pre- and post-scores observed. Therefore, although completion of outcome measures was good, the measurement choice needs to be reviewed, considering the length of the intervention and other influencing factors identified in this study.
Strengths and limitations
The study involved a small sample of healthy adolescents; to explore the intervention acceptability prior to testing in the target population, and the results should be considered in this context. While several refinements to the intervention and study procedures were identified, the next steps towards feasibility testing should include further user involvement and acceptability testing with those who have emerging mental health difficulties or are ‘at risk’ of developing difficulties. A training programme also needs to be developed to train future facilitators, and potential feasibility issues should be considered from the teacher’s perspective. Future attention should also be given to the timing of the intervention in relation to times of increased academic pressure and the effect this might have on outcome measures. Another important consideration is the fact that the intervention is designed to encourage occupation-related behaviour change. As such, occupational change may occur more slowly given the interventions’ focus on learning, exploring and then developing one’s own personalised occupational patterns, which crosses multiple occupational domains. Following participants up over a longer period may be warranted.
Conclusions
This study aimed to explore the acceptability of the ATUS intervention. The intervention was well received by participants, was practical to deliver in the school environment from the facilitator’s perspective, and no adverse events were identified. Initial recruitment targets were not met, suggesting further refinement of the recruitment strategy to reduce anxiety about participating may be advisable. Seven participants started and completed the intervention, and session attendance was good at 80%. Some components of the intervention should be reviewed through PPI, such as homework sessions and the time to complete tasks. While online completion of measures was generally good, we recommend that the outcome measures used in this study be reviewed, and alternative measures of occupation should be explored. Following modification this study, the acceptability and full feasibility of delivering the intervention in the target population should be assessed ahead of piloting the intervention.
Key findings
Healthy adolescents found the intervention to be acceptable.
Further PPI work could help improve recruitment and intervention acceptability.
A review of outcome measures is recommended.
What this study has added
Through this study, we have begun to examine the acceptability of the ATUS intervention and highlighted further development required ahead of feasibility piloting.
Supplemental Material
sj-docx-1-bjo-10.1177_03080226261423429 – Supplemental material for The ATUS24, an activity-focused time-use intervention to improve mental health and well-being in adolescents: an acceptability study
Supplemental material, sj-docx-1-bjo-10.1177_03080226261423429 for The ATUS24, an activity-focused time-use intervention to improve mental health and well-being in adolescents: an acceptability study by Jackie Parsonage-Harrison, Tammie Esslemont, Olivia Hodges, Helen Dawes and Johnny Collett in British Journal of Occupational Therapy
Footnotes
Acknowledgements
With thanks to The Movement, Occupation and Rehabilitation sciences group, part of OxInAHR, based at Oxford Brookes University, for supporting this research and providing methodological advice. Emily Lawlor, a student occupational therapist, is conducting the interviews as part of her role emerging research placement. Louise, a young person with lived experience of mental health difficulties for providing consultancy and advice throughout this project. The secondary school that provided access and supported this project.
Research ethics
Approved by Oxford Brookes University Research Ethics Committee on 21 June 2023. UREC number: 231696
Consent
All participants provided informed consent and were required to complete an online consent form before interviews were conducted.
Patient and public involvement data
During the development, progress and reporting of the submitted research, Patient and Public Involvement in the research was included at all stages of the research.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The Elizabeth Casson Trust for funding PhD that enabled this intervention to be developed, and the fellowship that enabled the first author to plan and conduct this acceptability study. The RCOT Career Development Grant for funding the costs of undertaking the acceptability study. Helen Dawes is funded by the NIHR Exeter BRC.
Contributorship
Jackie Parsonage-Harrison was involved at all stages of the development, progress, analysis and reporting of this project.
Tammie Esslemont provided consultancy and advice on this project from the perspective of a young person with lived experience and reviewed and contributed to the writing of this paper.
Olivia Hodges was involved in the analysis of results and reviewed the paper.
Johnny Collett provided senior oversight to the project, support with statistical analysis and critically reviewed the manuscript prior to publication.
Helen Dawes initial development and review.
Supplemental material
Supplemental material for this article is available online.