
Abstract
Introduction:
Current interventions provide limited success in managing mental health in adolescents with emerging difficulties. We describe using the Intervention Mapping framework to co-develop a novel occupational therapy theory-informed intervention for adolescents with emerging mental health difficulties, addressing the need for interventions tackling activity-related determinants.
Methods:
We describe a mixed-method, multiphase, sequential study design informed by the six-step Intervention Mapping framework, to develop the Activity Time Use intervention. Involving a systematic scoping review, time-use survey, qualitative focus groups and Delphi consensus process informing the construction of an intervention logic model of the problem, the logic model of change and creation of an intervention programme.
Results:
An eight-session intervention addresses three behavioural change outcomes: improving the balance of daily activities, improving occupational choice making abilities and improving occupational performance. The programme was positively reviewed through Patient and Public Involvement (PPI) consultation against the seven aspects of acceptability (Sekhon et al., 2017). Next steps include exploring the environmental determinants affecting implementation in different intervention delivery settings and full user acceptability.
Conclusions:
This study has provided a real-world example of intervention-mapping, systematically developing an occupational therapy intervention to empower adolescents to adopt healthier time-use behaviours to improve their mental health.
Keywords
Background and rationale for study
Rising numbers of 10–24 year olds are experiencing mental health difficulties (NHS Digital, 2020), with potential adverse effects on a critical, and complex, developmental period (Bowman et al., 2020). A repeated call exists in the research literature for timely, developmentally appropriate interventions targeting the determinants that influence mental health in young people and minimising the associated developmental disruption (McGorry et al., 2013; Sawyer et al., 2012, Patton et al., 2016, Wykes et al., 2021). A position informed by the limited range of available mental health interventions for young people and sparse exploration of novel alternative approaches (McGorry et al., 2013; Patton et al., 2016; Patton and Temmerman, 2016). There is growing evidence for the positive effect of mental health interventions targeting adult populations, which are informed by occupational therapy approaches and occupational science (Kirsh et al., 2019), but there has been limited of exploration in adolescent populations (Parsonage-Harrison et al., 2022).
A strong rationale exists for developing and testing mental health interventions for adolescent populations that adopt an occupational therapy-based approach. Core to the approach is the knowledge that the daily activities in which people engage and participate affect health, but in the context of adolescence occupations are also important in shaping multiple aspects of development including: identity, roles, habits and future employment (Lobo, 1999; Taylor, 2017) with long-term health consequences (Sawyer et al., 2012). For example, neurological development and specific brain maturation in late adolescence is associated with the development of executive functioning and self-management skills and is shaped by the individuals experiences within the context of their environment (Larsen and Luna, 2018). In the context of the life course, this brain development is typically concurrent with increased levels of autonomy and freedom to make personal choices and occurs in tandem with an adolescents acquisition of the capabilities and skills required to choose and act appropriately (Holmbeck, 2002). Occupational therapy interventions, informed by a specific understanding of person, occupation and environment in the context of adolescent development can be used to support adolescents who are experiencing the early stages of mental ill health or may be at risk of developing mental health-related difficulties during the transition towards adulthood. Referred to as emerging mental health difficulties for the purpose of this article.
Occupational therapy interventions that draw on understandings of occupational balance may be particularly beneficial for this population given the potential long-term health impact of their occupational choices. The need to promote adolescent health literacy when making choices that affect health has been advocated (Patton et al., 2016). Critically, the choices adolescents make about how they use their time, such as what activities they do and when, affect their health and could shape their ability to cope, navigate and adapt to challenge (Lassi et al., 2015; Patton et al., 2016; Patton and Viner, 2007; Viner et al., 2012). Furthermore, adolescents may miss activity-related experiences or might not yet have developed the capability or skills required to meet the increasing complexity of the task demands necessary for adult societal competency. The implication is that there is the potential for a ‘miss match’ between developed skills and capabilities and the current demands of their environment which may resulting in health consequences. The ‘mismatch’ is likely to be particularly acute among those from disadvantaged backgrounds who are at risk of less activity-related opportunities and experiences (Crenna-Jennings, 2018). Consequently, the idea of developing an occupational therapy time use intervention for adolescents with emerging mental health difficulties was conceived.
Developing health-related interventions is a complex process reflecting the complexity of the human system and the complexity of the multidirectional relationships between health and the other domains of functional ability, activity, participation, environment and personal factors (Kantartzis, 2019, World Health Organization, 2001). The processes used to develop interventions is increasing important, prompting the development of best practice guidelines for complex intervention development (Bleijenberg et al., 2018). Intervention development frameworks can be helpful when developing an intervention as they provide a structure and ensure that core components are considered in the right order. The respected and widely used Medical Research Council guidance for developing complex interventions provides an overarching structure (Skivington et al., 2021), but can be enhanced by other intervention development frameworks. One literature review found 21 different approaches and created a taxonomy of intervention approaches consisting of 8 categories and 18 action points (O’Cathain et al., 2019b).
Intervention mapping (IM) was chosen to inform the systematic development of this occupational therapy theory informed intervention for young people with emerging mental health difficulties because it was identified as one of the most comprehensive of the approaches based on the developed taxonomy (O’Cathain et al., 2019b). Although the framework was originally designed to develop health promotion interventions, it has increasing been used to develop other types of intervention where a change is desired. IM was also selected because it provides a detailed, six steps strategy. The IM strategy guides the systematic collection and processing of evidence from a wide range of sources, to information the development and articulation of a logic model of change, which forms the basis of intervention development (Bartholomew-Eldredge et al., 2016). There are a few reported examples of occupational therapy theory-informed interventions developed to target mental health difficulties using IM in the peer-reviewed academic literature. Therefore, this article aims to describe the application of IM in the construction of an occupational therapy theory-informed intervention known as the Activity Time Use Intervention (ATUS24), for 16- and 17-year-olds who have emerging mental health issues.
The ATUS was systematically developed using IM, with the intention of designing an occupational therapy intervention that provides, what Hinojosa (1994) describes as a scaffold or ‘just right challenge’. The intervention aims to empower adolescents aged 16 to 17 years to develop a better understanding of activity-related determinants that affect their patterns of everyday time-use and consequently their health. While at the same time developing their skills to manage and balance the different demands on their time and create and use a personal self-help, health management strategy. The intervention is aimed at a key transition point in adolescence, when they move in to post-16 education and face increased occupational demands and increased emergence of clinical-level symptoms of mental ill-health (Kessler et al., 2005)
Aims and objectives
This article aims to describe application of the IM framework to construct an occupational therapy theory-informed intervention known as the Activity Time Use Intervention, for 16- and 17-year-olds who have emerging mental health issues.
Methodology
The MRC framework for developing complex interventions was initially used to provide an overarching methodology (Medical Research Council, 2006; Skivington et al., 2021), with the six-step IM framework used to guide the intervention development phase (Bartholomew-Eldredge et al., 2016). Consultation with young people and other stakeholders occurred at strategic points throughout the project, including pre-planning, piloting and when reviewing the intervention programme. The guidance for reporting intervention development studies in health research (GUIDE; Duncan et al., 2020) and related Template for Intervention Description and Replication Checklist (TIDieR; Hoffman et al., 2014) were used to guide the reporting in this article. Figure 1 provides a project outline summary, illustrating the IM steps against the phases of the project and the methods used in each study which formed part of the project phases. It also illustrates the projects next steps.
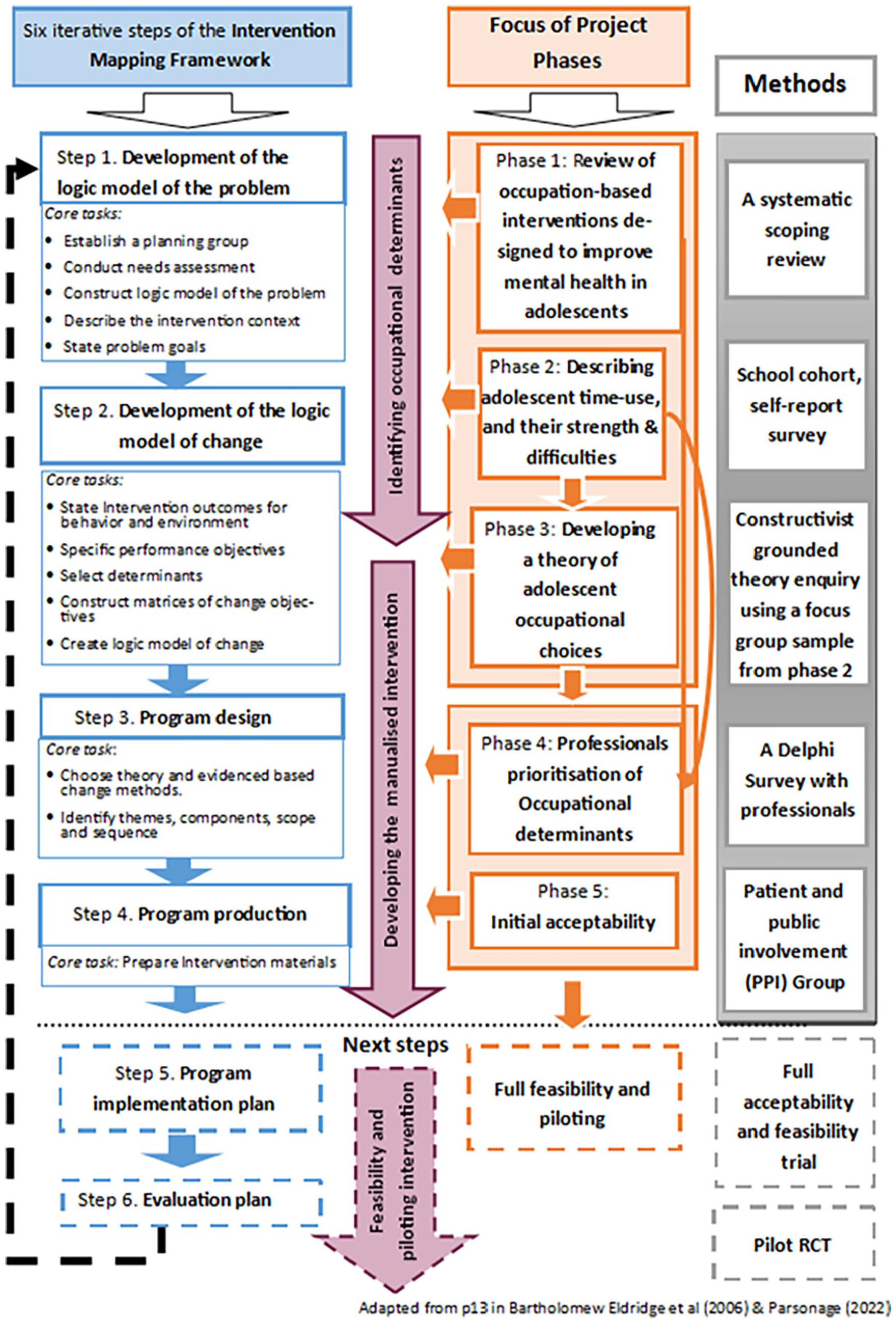
Project outline summary.
The process of using and applying IM is described in more detail below.
Applying the six-step IM framework
Step 1
Step 1 involves conducting a needs assessment that describes the context of the intervention including the population, setting and community and leading to the construction of a logic model of the problem, which intern informs the programme goals (Bartholomew-Eldredge et al., 2016). The project started with a comprehensive narrative review of the literature and a decision to focus on the health problem; occupational time-use in late adolescence affects mental health and well-being, especially for those with emerging mental illness. This mental health was identified as affecting the quality of life and future occupational functioning. This initial preparatory work was followed by a pragmatic mixed-method study, consisting of four individual sequential studies (protocol published electronically in the BMC ISRTN Registry ref-ISRCTN10573786) to illicit further information about the behavioural and environmental determinants related to the identified problem.
The four studies are as follows:
A systematic scoping review method identifying interventions reported in the academic literature that use occupation or activity to target adolescent mental health.
A time-use survey combined with the strengths and difficulties questionnaire conducted across two school sites, one urban and one semi-rural, with a year group cohort sample of 16- to 17-year-olds at the start of their post-16 education following GCSE’s.
The third study used constructivist grounded theory and involved 27 adolescents through six focus groups who volunteered to participate from the time-use cohort study. Exploring how and why 16- and 17-year olds in the first year of sixth form chose to engage in an occupation and its impact on them. The information from the first three studies informed the content of the fourth study.
The fourth study utilised a Delphi consensus method, conducted with 15 occupational therapists, clinicians and researchers in order to prioritise the occupation-related determinants identified from the earlier studies.
Ethics was sort from the Oxford Brookes University Research ethics committee. UREC Ref. 181192 and 191347.
Information generated from the first three sub-studies informed the needs assessment which stated the behavioural and environmental determinants thought to influence the health problem. The Delphi consensus study was used to prioritise which determinants were most important to tackle. The information gathered was used to create a ‘logic model of the problem’ based on the format suggested by the IM manual, a modified version of the PRECEDE model (Bartholomew-Eldredge et al., 2016). Specifically, the behaviours and environmental determinants that influence the identified health problem were organised in a flow diagram that works from right to left rather than left to right. The model starts with positioning the ‘quality of life’ domain affected being placed on the right-hand side of the flow diagram. Next, the specific health problem that the intervention intends to address is stated, followed by the behavioural and environmental determinants. Lastly, the personal determinants that affect the behaviours and environmental determinants are stated, thus, creating the logic model of the problem.
Step 2
Step 2 involves rewriting the logic model of the problem to create a logic model of change.
A logic model of change, as it is known with in intervention science, is a structure around which an intervention is developed that explains the mechanisms or logic by which an intervention is intended to bring about change. Practically, when using IM, this means that the behavioural and environmental determinants identified and described in the logic model of the problem are rewritten as intervention outcomes indicating the behaviour change intended as a result of participating in the intervention. The next action is to rewrite the personal determinants as performance objectives, which emphasising the change that is needed to achieve the behavioural and environmental outcomes of the intervention. IM states that too many performance objectives can result in an overly complex intervention consequently we included only the top three personal determinants highlighted in the Delphi survey for each of the three newly created behavioural outcomes in our logic model of change.
Next, using the literature and information gathered, a new set of personal determinants that influence the newly created performance objectives (The previous personal determinants) are identified. These newly created personal determinants are rewritten to reflect the change required to effect change in the performance objective. These specifically rewritten personal determinants become known as change objectives. The logic being that appropriately affecting change at a personal determinant level will result in the desired behaviour and environmental change described in the performance objectives and result in the specified behavioural and environmental outcomes.
The final delivery environment is not yet decided, so that at this stage in the intervention’s development a pragmatic decision was made to focus solely on behaviours, reflecting the view that tailoring interventions to the delivery environment will be required at the planning implementation stage (Mills et al., 2019).
Step 3
The third step involves three tasks: identifying appropriate behaviour change theories for each change objective; considering the parameters of the methods and selecting applications; and finally generating the intervention programme themes, components, scope and sequence (Bartholomew-Eldredge et al., 2016). Matrices are used to map each change objective, which is organised according to the nature of the type of change required, for example, does the intervention participant need to learn new knowledge, to be prompted to change their attitude, or need to develop new skills. Each change objective is then considered individually and the most relevant theories and method of delivery is selected based on which is best suited to change the individual determinant and bring about the desired change.
Step 4
The third step involves the conceptualisation of the overarching intervention programme and organisation of themes and topic content. Specifically, this involves formulating session plans, stating the order of specific prescribed intervention tasks, identifying resources required and writing or creating any materials necessary to deliver the intervention. The developed intervention then underwent PPI review.
PPI review of the ATUS intervention
A group of four young women, involved in the earlier studies as PPI consultants, were invited to discuss prospectively the acceptability of the initial programme outline and content. Conducted over zoom, the participants received an explanation of the purpose of the intervention, an overview of the intervention programme, its aims, structure and the content of each session. They were then asked to discuss and provide feedback on the acceptability of each part of the proposed intervention outline as a potential intervention for 16- and 17-year-olds. The researcher reviewed the feedback after the group, summarising and grouping the feedback according to the seven aspects of acceptability proposed by Sekhon et al. (2017) which includes affective attitude, burden, ethicality, intervention coherence, perceived effectiveness and self-efficacy of the intervention to the target population.
Results
Step 1
The results of the four sub-studies, reported as a summary here but published in detail elsewhere, inform the needs assessment described as Step 1. The review identified 74 studies of which only five appeared to be underpinned by occupational therapy theory (Parsonage-Harrison et al., 2022). A total of n134 students completed the time-use questionnaires. The results illuminated patterns of activity, SDQ scores consistent with the normative date and provided the sampling frame for the grounded theory study. The grounded theory study led to the formation of a theory of adolescent occupational choice (Parsonage et al., 2020). These first three sub-studies identified occupation-related determinants affecting adolescent mental health at an individual, interpersonal, organisational, community and societal level (Bartholomew-Eldredge et al., 2016).
Through the Delphi process, we added 30 determinants to the original 59 items identified, before prioritising the items. The occupational determinants thought most likely to affect mental health include types of activity, balance of activity, occupational identity, freedom of choice and pressure to conform. These determinants were used to create the logic model of the problem (See Figure 2).
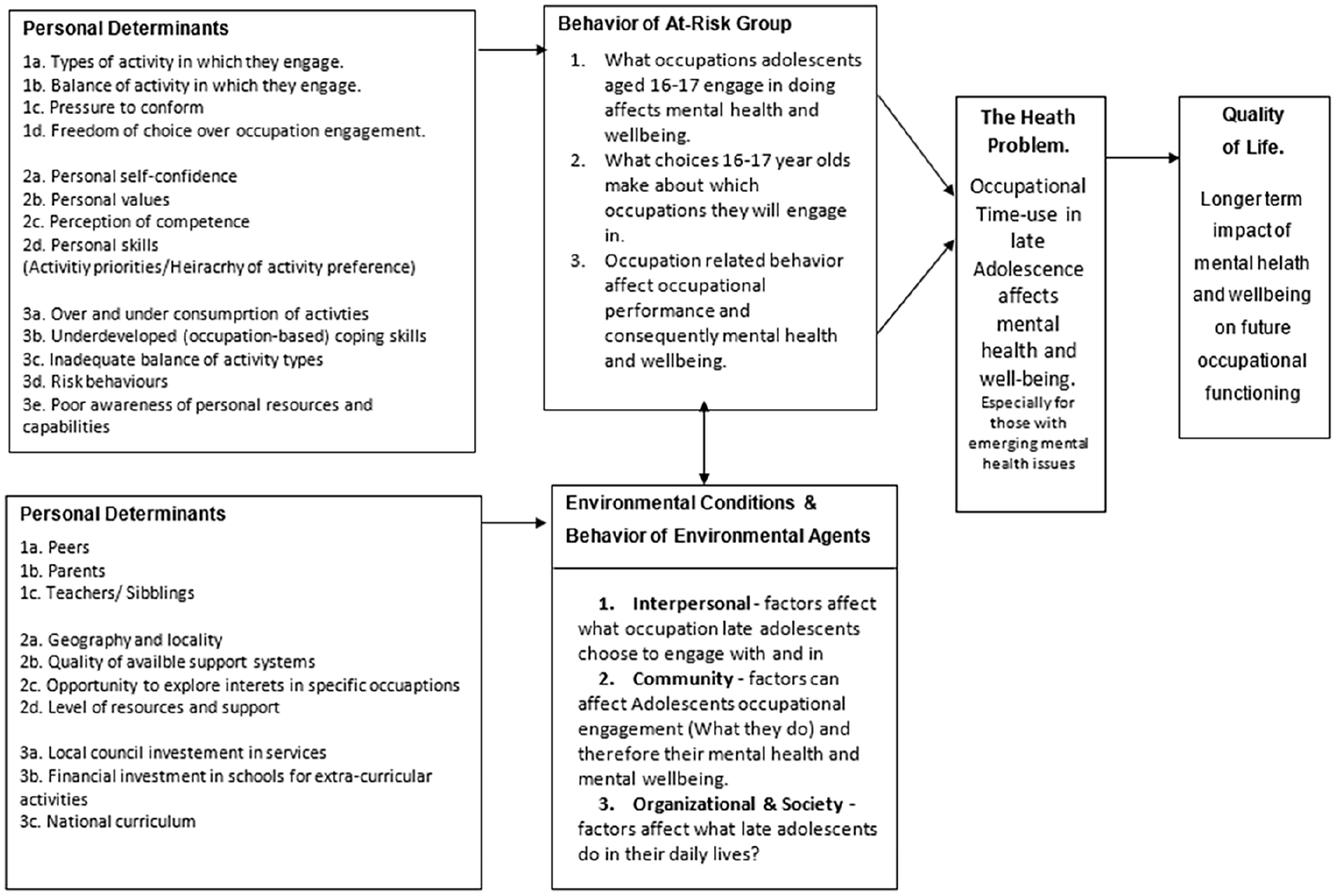
Logic model of the problem.
Step 2
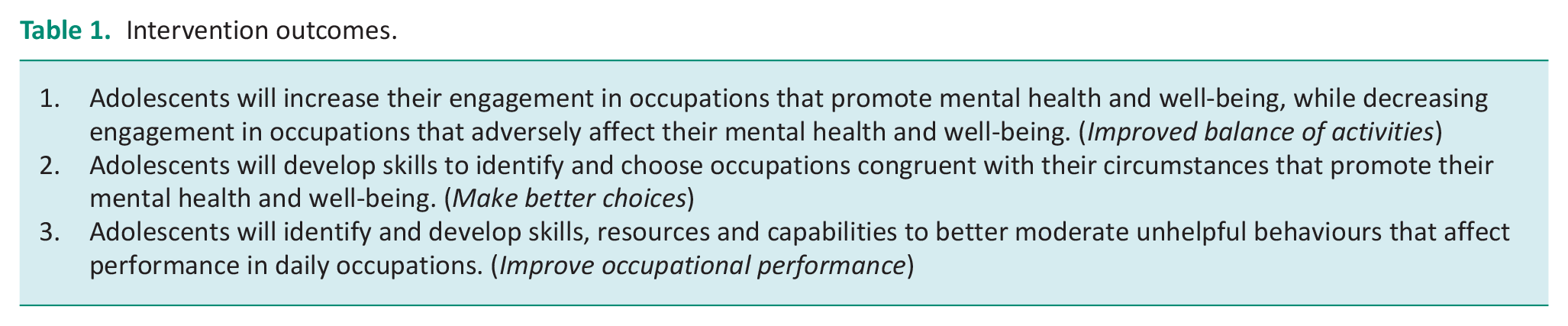
Following the IM guidance for step 2, we rewrote the identified behaviours into intervention outcomes indicating what needs to change and to improve the outcome (See Table 1). At this point in the study, it was decided to focus on the behavioural determinants and delay focus on the environmental determinants until the implementation stage. This decision was made with the project team and was guided by an understanding that this intervention may be appropriate in different contexts such as children and adolescent mental health services, schools, early intervention services and university settings. Addressing the environmental factors at the implementation stage ensures that the intervention is tailored to the services in which it will be delivered.
Intervention outcomes.
Then following the methodology as stated above led to the creation of nine performance objectives which inform the creation of the model of change (see Figure 3).
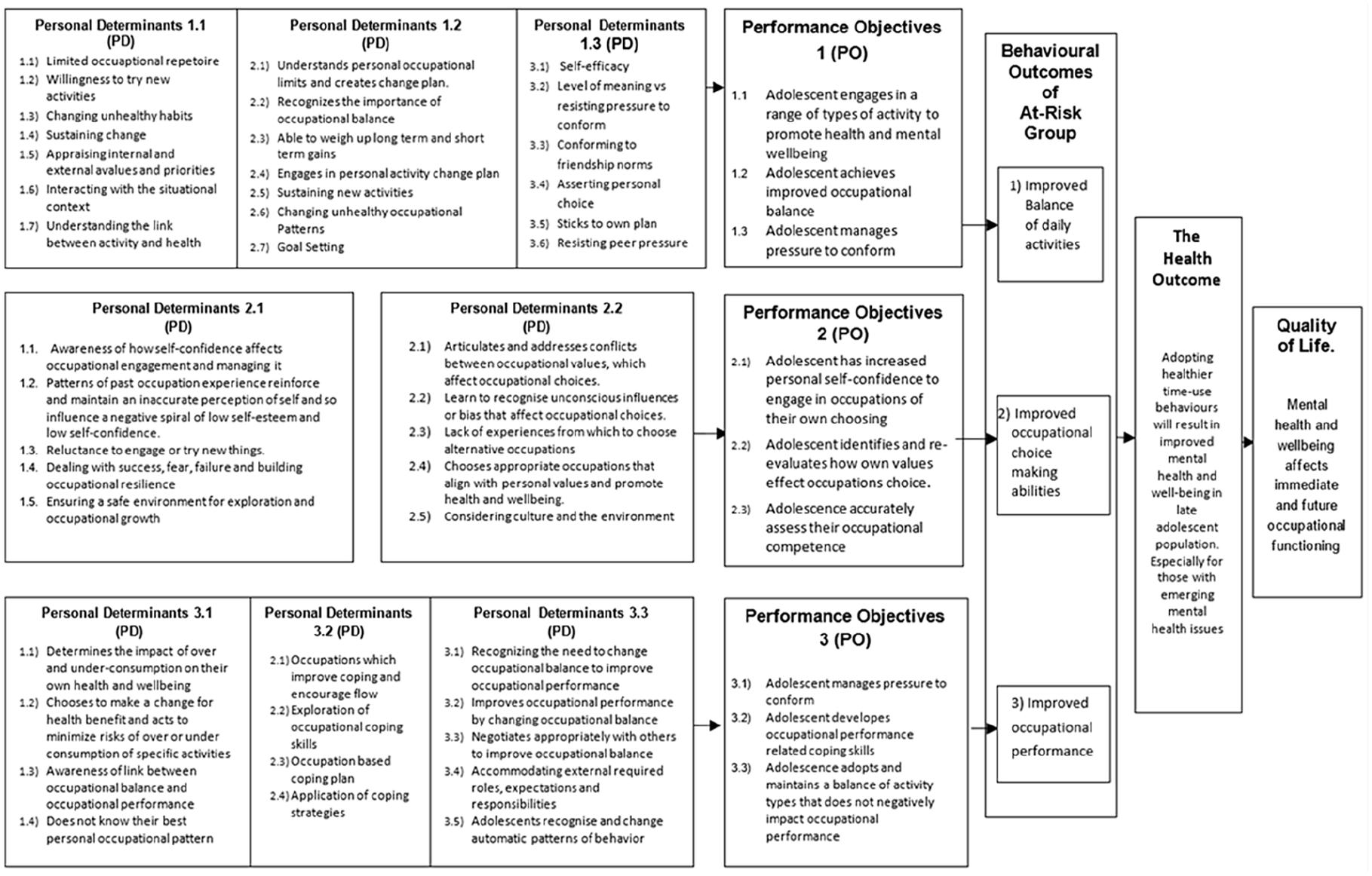
Logic model of change.
Step 3
Following an initial attempt at the prescribed step three task, the process of the task was modified to incorporate the first authors previous clinical experience of developing occupational therapy interventions. This decision followed a careful consideration of the compatibility of the IM approach with occupational therapy theories, resulting in the first authors using the occupational therapy model; The Model of Human Occupation (MOHO) developed by Gary Kielfhofner (Taylor, 2017) as an overarching framework for the intervention because it was designed to be used alongside other concepts and theories (Taylor, 2017). MOHO guides a client-centred approach to activity-related change (Taylor, 2017), is advocated for (Harrison and Forsyth, 2005) and widely used in children and adolescent mental health services (Brooks et al., 2018). The decision was not discussed with service users or other stakeholders but with the PHD project team to ensure an occupational therapy focus and theoretical compatibility between the philosophical assumption of IM and MOHO.
This adapted process involved grouping the performance objectives according to themes identified in the earlier qualitative study and considering the groupings alongside the MOHO. The themes included at this stage were making a choice, balancing occupations, values and priorities, developing skills and dealing with the situational context. Once grouped the change objectives for each performance objective were mapped to the most relevant theories and applications delivery methods identified.
Step 4
The conceptualisation of the overarching programme theme began to form during the earlier phases of the project, as patterns of time-use emerged and a theory developed around adolescent occupational choices. The subjective, complex, multi-dimensional, occupational therapy concept of ‘occupational balance’, which is related to patterns of daily occupation (Eklund et al., 2017; Wagman et al., 2015) appeared to align with the emerging determinants and change objectives and consequently was adopted as an appropriate choice for the overall programme theme.
Using experience gained in clinical practice as an occupational therapist, IM and MOHO strategies, the personal determinants outlined in the logic model of change, were organised into six themes (A detailed account of the process used is available at https://doi.org/10.24384/zkmj-mh15).
At the end of step three, six themes formed the basis of the eight-session ATUS intervention programme, with the content from two themes divided into smaller units designed to last 50 minute each. The themes sessions titles are exploring skills and developing the occupational repertoire; balancing occupations and time; volition and valuing occupation; managing the situational context; managing occupational choice and appraising occupational choice and developing the occupational self.
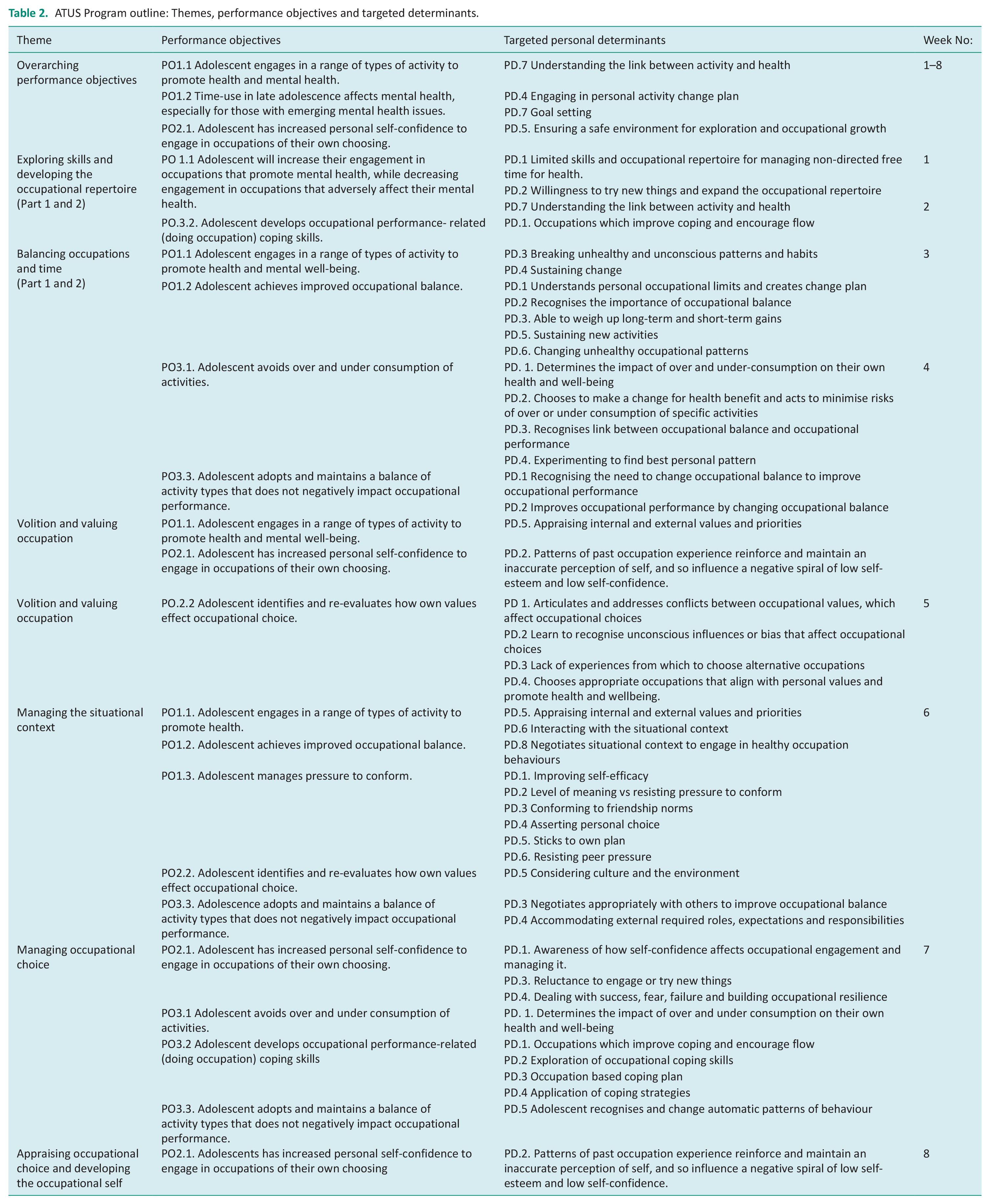
The first author designed the session plans to be delivered by a trained therapist, with each session including a warm up and introduction to topic, one or two occupation-focused tasks and a specific applied homework task. The chosen intervention strategies include validating, identifying, giving feedback, advising, structuring, negotiating, coaching, encouraging and practical support, which is all recognised in the MOHO theory and application book (Taylor, 2017). See Table 2 for an outline of the course content and structure.
ATUS Program outline: Themes, performance objectives and targeted determinants.
Outcome of PPI review of the ATUS intervention
The information collected through the PPI review was positive and constructive. There was a general consensus that the intervention not only could be helpful but also illuminated areas of the programme that could be modification to improve the acceptability of the intervention. A number of key points to address included a need: to use language that sells the intervention to young people; to ensure that the practical utility and value of the intervention is illuminated; to schedule the intervention to coincide with when young people’s need is perceived to be greatest; to consider perceived and real safety when activities involve group discussion related to personal choices; to consider using debates, quizzes and competitions as they are preferred over discussion and role play activities types in this age group; to review homework activities as the idea received mixed reviews and the general view was that apps rather than paper may aid completion of tasks.
Discussion
This article reports the systematic process used to construct a new and novel intervention programme that draws on occupational therapy theory with the aim to support adolescents’ own natural development and scaffolds time-use related skill acquisition in their first-year post-GCSE’s exams. The adolescent is encouraged to reflect on their own occupation-related needs and choices and how those choices affect their health. Each adolescent is empowered, in their own context and unique personal circumstances, to understand their current time-use patterns and adopt a healthier personalised holistic pattern of everyday time use that aligns with their own values and beliefs. Thus, potentially, influencing their own mental health and reducing the risk of mental health difficulties.
The programme development combined the MRC guidance compatible IM framework, used to develop evidenced-based interventions and the MOHO (Taylor, 2017) used as structure to ensure that the intervention was informed by occupational therapy theory. Theoretical compatibility between the MOHO and the use of multiple behaviour change theories as advocated by IM was considered achievable, given the parallels between the social ecological paradigm from which IM emerged (Wight et al., 2016) and occupational therapy conceptual foundations, which underpin MOHO. Principles in common include recognition of bi-directional relationships between the individual as a whole, in the context of their environment with corresponding health consequences (Bartholomew-Eldredge et al., 2016, Taylor, 2017). Compatibility, also extends to the IM’s pragmatic, problem-focused systems theory perspective (Bartholomew-Eldredge et al., 2016) and the MOHO’s dynamic systems perspective designed to be used alongside other interdisciplinary concepts (Taylor, 2017). At an applied level, despite language differences, both advocate that intervention development include a comprehensive assessment of the personal needs, environmental determinants, comprehensive stakeholder consultation and involvement, a conceptualisation of the needs of the group and application of theory based on the needs identified.
Despite the similarities, MOHO approach adds a unique occupation-focused perspective which illuminates principles of an individual’s occupational nature, recognises and adapts to an individual’s needs as they interact through occupation with the environments important to them, and includes an understanding of occupational dysfunction (Kielhofner, 2009). To ensure the intervention preserved the unique features of the MOHO approach, its principles were respected throughout development as advised by Taylor (2017) and which is compatible with the fact that IM uses multiple behaviour change theories, but selection is guided by each individual behaviour change goal (Bartholomew-Eldredge et al., 2016). Furthermore, the intervention programme aimed to incorporate collective and personal exploratory participation projects that are achieved and implemented through engagement in meaningful occupational opportunities that incorporate the principles of diversity, flexibility and continuity (Taylor, 2017).
Practically, this systematically developed intervention programme is a promising start to developing an intervention to address occupational determinants affecting mental health. Next steps must include a full user acceptability assessment, and an exploration of how the environmental determinants are affected by the intended implementation settings. Publishing the study outline at this stage provides research transparency and shares the knowledge gained through the initial project stages. The intervention has a potential to contribute to the variety of interventions available to tackle early and emerging mental health issues in the adolescent population. The study is of particular relevance to the emerging field of life-style psychiatry (Firth et al., 2020), which is interested in how lifestyle factors and time use affect mental health. In contrast to much of the existing lifestyle psychiatry literature, which tends to focus on specific occupations such as sleep, diet, exercise and hobbies, this study combines a recognition of interplay between the individual’s unique characteristics, their environment, and the finite nature of time in the context of occupational choice. It provides an evidence-based intervention programme designed to empower young people to make real-world occupational choices with the purpose of achieving a realistic, meaningful and healthy balance of occupations. Furthermore, this study provides an example of how behaviour-change theories and approaches, such as IM and occupational therapy theory, can be considered together to inform the development of an intervention.
Limitations and implications
The IM approach used is comprehensive, thorough and likely to produce effective results, but it is a lengthy process, and the feasibility of this intervention is not yet tested. Development of interventions using IM requires a collaborative approach between clinicians, researchers and service users. Using the IM framework, the work completed thus far, forms the basis of further work including adding the identified environmental components to the intervention, developing the programme materials and a more thorough review of the intervention plan with key stakeholders, such as parents and teachers leading to the intervention being trialled and fully evaluated. In its present state the intervention could potentially be adapted for a school population as originally intended or, potentially, other populations of young people, such as those accessing mental health services. Completing the environmental conditions assessment more specifically would facilitate the tailoring of the intervention plan to specific groups of adolescents. Although this intervention is not yet complete, the project has a tangible product that can be readily adapted to different contexts and provides scope for adaptation and exploration in different delivery contexts.
Conclusion
An occupational therapy theory-informed intervention has been systematically developed using a combination of existing and new knowledge developed over the course of the project. Next steps involve collaborative co-development of interventional materials, and feasibility testing to establish the acceptability, effectiveness and cost-effectiveness of the intervention.
Key findings
Intervention mapping can be used successfully alongside occupational therapy theory to develop interventions.
A novel occupational therapy theory-informed intervention for young people with emerging mental health difficulties has been developed.
What the study has added
This study provides an example of developing a novel occupational therapy-informed intervention using the intervention mapping framework for young people experiencing emerging mental health difficulties.
Footnotes
Acknowledgements
We acknowledge Professor Mona Eklund, who also oversaw the PHD study from which this article subsequently was developed. She chose not to be involved with this article as intervention mapping was not her area of expertise. We also acknowledge all those that supported and took part in this study.
Research ethics
The study received ethical approval from Oxford Brookes University Ethics board (UREC no. 181192 12th September 2019 and UREC. No. 191347 30th October 2019).
Consent
Written informed consent was obtained from all those that participated in the various stages of this project.
Patient public involvement data
During the development, progress and reporting of the submitted research, patient and public involvement in the research was included in the planning and progress of specific parts of the research as detailed in the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was made possible through funding provided by The Elizabeth Casson Trust. The views expressed are those of the author and do not necessarily reflect those of the Elizabeth Casson Trust. During the first authors’ PhD, Professor Helen Dawes was supported by the Elizabeth Casson Trust and the NIHR Oxford Health Biomedical Research Centre. During the preperation of this paper, Helen is funded by the Exeter Biomedical Research Centre, NIHR.
Contribution
JPH conceived and undertook all aspects of the study. HD was the study supervisor and responsible PI providing supervision and oversight of the study. JPH wrote the initial draft of the article following discussion with HD. Al authors reviewed and edited the manuscript and approved the final version.