
Abstract
Introduction
Mental health disorders and low levels of mental well-being can have a lasting effect on life satisfaction and contribution to society for children and adolescents, yet the effectiveness of occupational therapy interventions is unknown.
Methods
A mixed methods systematic review was conducted including studies with children and adolescents aged 5–16 years, who had mental health difficulties, that evaluated occupational therapy interventions and focused on participation in everyday occupations as an outcome.
Results
The nine included studies were generally very low quality. The results could not be pooled due to heterogeneity. For children with Asperger’s syndrome, the Cognitive Orientation to Daily Occupational Performance intervention had clinically significant improvements on occupational performance and social skills. For children with attention deficit hyperactivity disorder, the Ultimate Guide to Play, Language and Friendship intervention improved playfulness and the Cognitive–Functional intervention had a statistically significant improvement on occupational performance and behaviour.
Conclusion
One intervention used by occupational therapists with children with Asperger’s syndrome and two interventions used with children with attention deficit hyperactivity disorder had some evidence of effect. No evidence was identified for the effectiveness of occupational therapy interventions for children and adolescents with other common mental health conditions.
Introduction and literature review
Mental health concerns in children and adolescents, including anxiety, depression, eating disorders, bipolar disorder, post-traumatic stress disorder, psychosis, autism spectrum disorder and attention deficit hyperactivity disorder have received global attention (World Health Organisation, 2013). The reported global prevalence of mental health disorders in children and adolescents ranges from 6.7% (Erskine et al., 2017) to 13.4% (Polanczyk et al., 2015). Additionally, there are indications that as many as one in four adolescents may experience poor mental well-being, which does not meet a diagnostic threshold (NHS Digital, 2020). The impact of mental health disorders in early life is known to have a lasting impact on later adult mental health, educational attainment, criminal activity and life satisfaction (Mock and Arai, 2011). There has been a call for further resources, policies, practice and research to address mental health problems (World Health Organisation, 2013).
The breadth of disorders, wide range of interventions, influence of healthcare professionals and varied policy agenda in child and adolescent mental health has resulted in diverse research outputs and clinical practice. The scope of pharmacological interventions is limited, and while there has been a trend for ‘talking therapies’ for some young people, cognitive behavioural therapy (Van Doorn et al., 2017) and family therapy have been found to be no more effective than usual care (Cottrell et al., 2018). A recent overview of systematic reviews for interventions in adolescent mental health has reported that school-based cognitive–behavioural therapy effectively targets symptoms of depression, community-based activities have a positive effect on changing behaviour and self-esteem and internet-based interventions show promise for treating anxiety and depression (Das et al., 2016). Individual interventions were found to be too heterogeneous to conduct meta-analysis (Das et al., 2016). A similar review for mental health interventions with children has not been found, illustrating the complexity and diversity of the population, and the need to establish standardized interventions and outcomes (Das et al., 2016).
Occupational therapy is a healthcare profession that enables health and well-being through participation in everyday activities (World Federation of Occupational Therapists, 2013). A historical review of the profession identified its strong foundations in the treatment of mental illness, originating in the moral treatment movement of asylums (Hocking, 2007). Present-day occupational therapists use a range of occupational therapy interventions to enable individuals and groups of people to participate in their occupations of self-care (such as brushing teeth or eating), productivity (such as going to work or school) and leisure/play (such as swimming or soccer). Contemporary occupational therapy interventions have been described as occupation-based and/or occupation-focused (herein referred to as occupation-based/-focused) (Fisher, 2013). Occupation-based interventions engage the client in meaningful and purposeful occupations within the context of their everyday life; for example, singing or shopping. During occupation-based interventions, the participation itself is the therapeutic agent of change. Occupation-focused interventions use occupational skills training in the context of occupational performance relevant to the person’s goals; for example, the provision of adaptive equipment or the teaching of compensatory strategies during the occupation of dressing (Fisher, 2013). Interventions that focus on changing a person’s underlying body functions or structures are not occupation-based/-focused.
Three related systematic reviews have been published that considered occupational therapy in mental health with a child and/or adolescent population (Arbesman et al., 2013; Cahill et al., 2020; Read et al., 2018). The most recent one (Cahill et al., 2020) reports to update an earlier review (Arbesman et al., 2013). Both of these reviews broadly interpreted the scope of practice to include activity-based interventions whereby direct occupational therapy intervention was not provided. In addition, the reviews (Arbesman et al., 2013; Cahill et al., 2020) included studies where the population did not have a mental health illness but was considered at risk of developing a mental illness. Cahill et al. (2020) found moderate to strong evidence for yoga and sport and moderate evidence for play and arts as activities that support good mental health. In a separate review, Read et al. (2018) included interventions within the scope of occupational therapy practice, although they did not define this scope. The target population included those up to 35 years of age, and although functional outcomes were used, they were also not defined. Overall, the review by Read et al. (2018) found strong evidence for cognitive remediation to improve general functioning, moderate to strong evidence for supported employment/education to improve social and occupational outcomes and strong evidence for psychoeducation to improve general functioning, problem-solving and rehospitalisation. Each of these reviews summarized their findings using levels of evidence; Read et al. (2018) and Cahill et al. (2020) used similar systems which were different to the one used by Arbesman et al. (2013). No meta-analysis was conducted, nor summary data provided in any of these reviews. As such the findings of Read et al. (2018), Cahill et al. (2020) and Arbesman et al. (2013) suggested that a more precise review was needed that included only those studies with participants diagnosed with a mental health disorder, focussed on occupational therapy interventions, and used outcomes related to occupational participation. This shaped the overarching objective of this systematic review: to determine the effectiveness of occupational therapy interventions for children and adolescents with mental health difficulties.
Review question
The primary review question was what is the effectiveness of occupational therapy on participation in everyday occupations in children and adolescents with mental health difficulties? More specifically, the objective was to identify the evidence for the effectiveness of occupational therapy interventions that are occupation-based/occupation-focused.
Inclusion criteria
Participants
Studies were considered that included children and adolescents in the age range 5–16 years (inclusive), who had any of the mental health difficulties commonly experienced by this age group. For example, depression, self-harm, generalized anxiety disorder, post-traumatic stress disorder, attention deficit hyperactivity disorder, autism and eating disorders. Studies where participants were identified as having more than one mental health difficulty or an intellectual or physical disability in addition to a mental health difficulty were included. This age group was selected because interventions focussed on younger children are more likely to target parents, as children are less likely to be able to address the issues themselves and adolescents older than this may overlap with adult interventions and services.
Intervention(s)
Studies were considered that evaluated occupational therapy interventions, that is, interventions that were either occupation-based/-focused, which reflects contemporary professional practice (Fisher, 2013). Occupation-based interventions are characterized by the patient’s involvement in a meaningful occupation within the context of their everyday life and where the occupation itself is the therapeutic agent of change; for example, taking a shower or riding a bike. Occupation-focused interventions use occupational skills training in the context of occupational performance, for example, the use of coaching strategies during the occupation of dressing. Interventions that focus on changing a person’s underlying body structures or functions are not occupation-based/-focused and were excluded.
Comparator(s)
Studies were included that compared the intervention to any comparator, including no comparator.
Context
This review considered studies in any context where children and/or adolescents received occupational therapy. This included hospital inpatient units, outpatient clinics and community settings, such as in their own homes or at school.
Outcomes
Studies were considered that included participation in everyday occupations as an outcome as measured by standardized assessment tools or validated self-report measures.
Types of studies
This review included studies published in the English language since 1927, encompassing the time from the publication of the first occupational therapy journals. The types of studies considered were experimental and quasi-experimental study designs, including randomized controlled trials, non-randomized controlled trials, before and after studies and interrupted time-series studies. In addition, analytical observational studies including prospective and retrospective cohort studies, case–control studies and analytical cross-sectional studies were included. This review also considered descriptive observational study designs including case series, individual case reports and descriptive cross-sectional studies for inclusion. Qualitative studies were also considered, including, but not limited to, designs such as grounded theory, ethnography and phenomenology. 1 The textual component of this review included publications that describe occupational therapy interventions, such as practice reports and policies.
Methods
This review employed the Joanna Briggs Institute (Aromataris and Munn, 2020) methodology for systematic reviews. The objectives, inclusion and exclusion criteria and methods of analysis for this review were specified in advance and published in a protocol (Brooks and Bannigan, 2018).
Search strategy
A comprehensive search strategy was conducted in May 2020 to find published and unpublished studies. A three-step search strategy was used: firstly, an initial limited database search was undertaken to inform the development of the search strategy; secondly, all included databases were searched using the identified search strategy of keywords and index terms; and finally, the reference lists of included studies were searched.
Study selection
Citations of the studies identified in the search were collated and uploaded to EndNote vX7.7.1 (Clarivate Analytics, 2017) and duplicates removed. Titles and abstracts were screened by two independent reviewers against the inclusion criteria. Full texts were retrieved for all studies that met the inclusion criteria, or where there was insufficient detail in the title and abstract to determine suitability. Contact was made with study authors to obtain copies of conference posters or full-text articles that could not be accessed. The reasons for excluding studies were recorded. Any disagreements between reviewers during the review process were resolved through discussion, so a third reviewer was not required.
Assessment of methodological quality
The methodological quality of the studies selected for inclusion was independently assessed by two reviewers using the standard critical appraisal instruments in The Joanna Briggs Institute System for the Unified Management, Assessment and Review of Information (JBI SUMARI) for quasi-experimental studies, case reports and randomized controlled trials (Aromataris and Munn, 2020). Rieger et al.’s (2016) approach for the cut-off criteria for methodological quality was adopted, that is, case reports were included if they received a rating of ‘yes’ or ‘not applicable’ on questions 1 and 5. Quasi-experimental studies were included if they received a rating of ‘yes’ or ‘not applicable’ on JBI SUMARI quality appraisal questions 2, 7, 8 and 9. Randomized controlled trials were included if they received a rating of ‘yes’ or ‘not applicable’ on questions 1, 3, 10, 11 and 12. If a study received a ‘no’ or ‘unclear’ rating on any of the key criteria, the study was excluded. Discussion was used to resolve any disagreements between reviewers; a third reviewer was not required.
Data extraction
Data extraction was conducted using the recommended JBI approach (Aromataris and Munn, 2020). Data were extracted by two independent reviewers using JBI SUMARI. Details extracted from case reports included country, setting, participant characteristics and results. Details extracted from quasi-experimental studies included country, setting, participant characteristics, intervention groups, outcome measures and results. No data were deemed by the reviewers to be missing.
Data synthesis
As this was a mixed methods review of the effectiveness of interventions, a segregated approach to data analysis was planned, that is, a meta-analysis of the quantitative data and a meta-aggregation of qualitative data, followed by an aggregation of the synthesized qualitative and quantitative findings to configure the findings to generate a set of statements that represent that aggregation. Neither meta-analysis nor meta-aggregation was possible due to the limited data, so the findings as a whole are presented in a narrative summary. This was a change from the published protocol (Brooks and Bannigan, 2018) because the limited data identified meant neither meta-analysis nor meta-aggregation was meaningful.
Results
Study inclusion
Summary of critical appraisal.
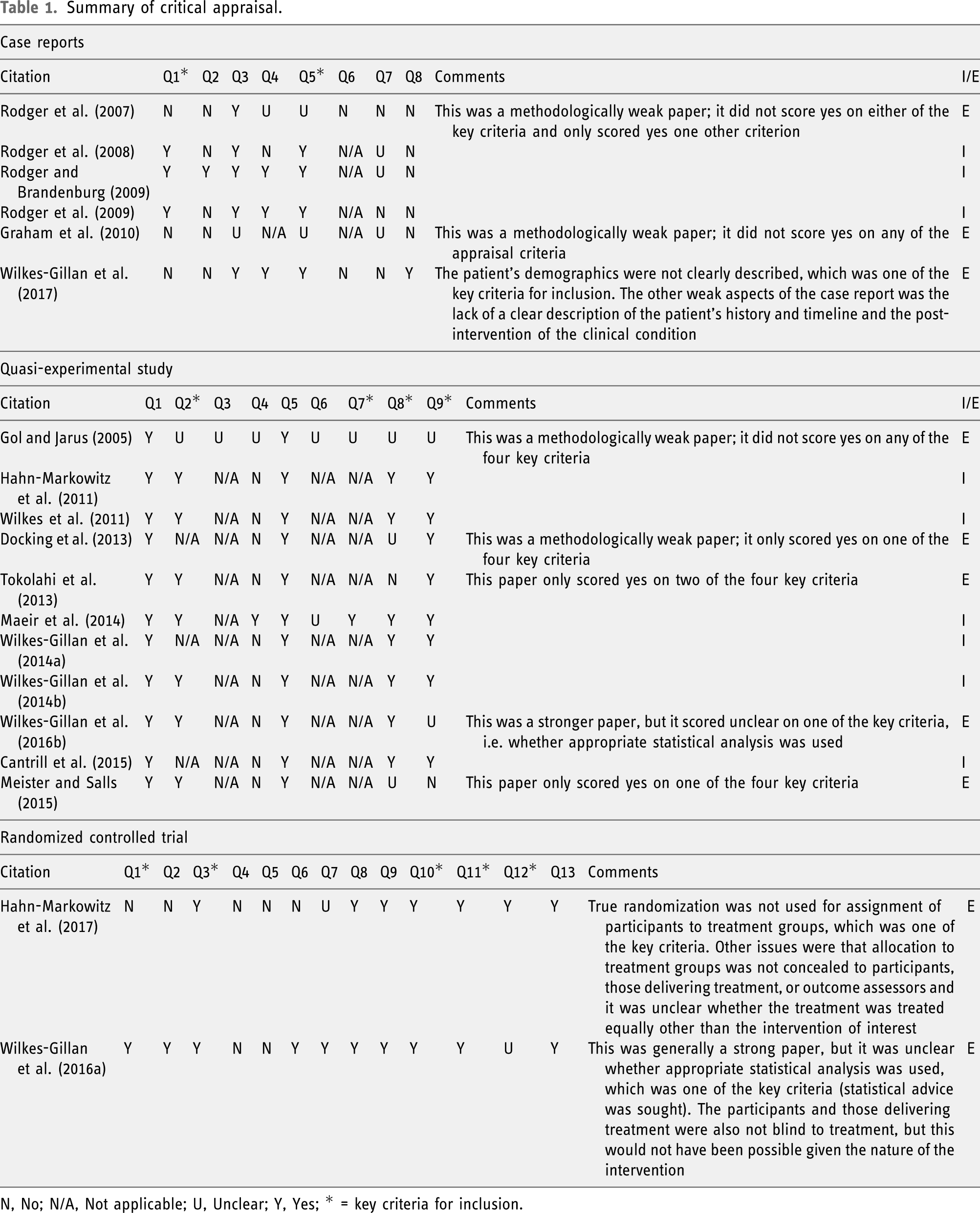
N, No; N/A, Not applicable; U, Unclear; Y, Yes; * = key criteria for inclusion.
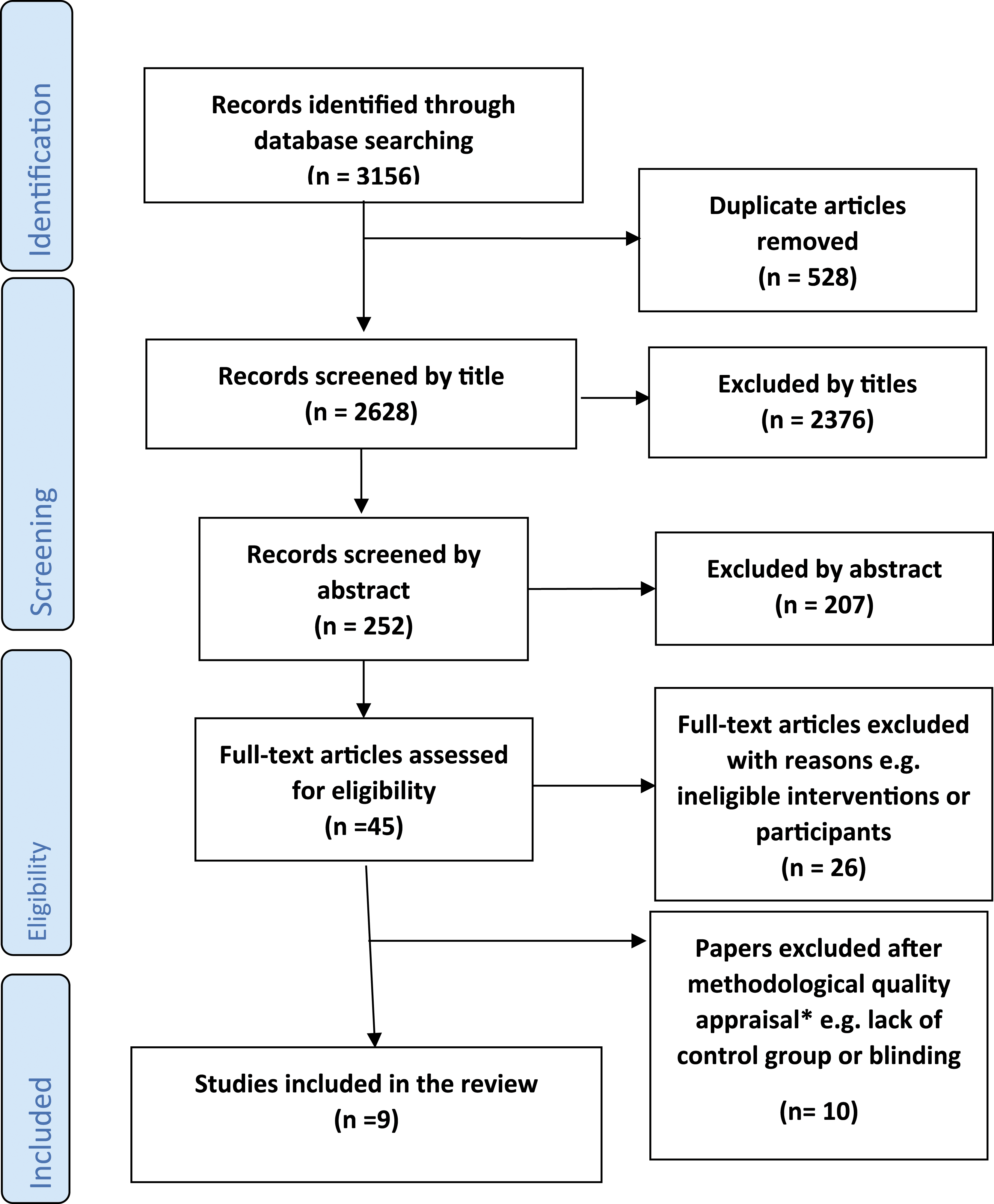
PRISMA flow chart (Moher et al., 2009) *full list available from corresponding author.
Methodological quality
The quality of the studies as a whole was very low, even though the included studies met the key criteria for inclusion. Following full-text review, 19 studies were appraised for methodological quality (12 quantitative, one qualitative, and six mixed methods, of which six were case reports, 11 quasi-experimental and two randomized controlled trials); 10 studies did not meet the predetermined key criteria relevant to their study design. There were some common reasons for exclusion; for example, case reports were usually excluded for not including sufficient patient demographic information and quasi-experimental studies were frequently excluded for not measuring outcomes in a reliable way. Both randomized controlled trials were excluded, one for not using true randomization and the other for unclear statistical analysis. Of the nine studies included in the final review, six were quantitative (Hahn-Markowitz et al., 2011; Maeir et al., 2014; Rodger and Brandenburg, 2009; Rodger et al., 2008, 2009; Wilkes et al., 2011) and three mixed methods (Cantrill et al., 2015; Wilkes-Gillan et al., 2014a; 2014b), of which three were case reports (Rodger and Brandenburg, 2009; Rodger et al., 2008, 2009) and six quasi-experimental studies (Cantrill et al., 2015; Hahn-Markowitz et al., 2011; Maeir et al., 2014; Wilkes et al., 2011; Wilkes-Gillan et al., 2014a; 2014b). Whilst the included studies all met the appraisal cut-off criteria, two case reports did not present a clear patient timeline (Rodger et al., 2008, 2009), one did not have a clear description of adverse events (Rodger et al., 2009) and none presented any takeaway lessons. The reviewers found that a rating of ‘not applicable’ was applied to the question ‘Was the post-intervention clinical condition clearly described?’ for all included case reports. Of the six quasi-experimental studies, only one had a control group (Maeir et al., 2014). Of note, the reviewers found that for all quasi-experimental studies, they needed to use the rating of ‘not applicable’ regularly for question 3 ‘Were the participants included in any comparisons receiving similar treatment/care, other than the exposure or intervention of interest?’, questions 6 ‘Was follow-up complete and if not, were differences between groups in terms of their follow-up adequately described and analysed?’ and question 7 ‘Were the outcomes of participants included in any comparisons measured in the same way?’
Characteristics of included studies
Data extraction table for included studies.
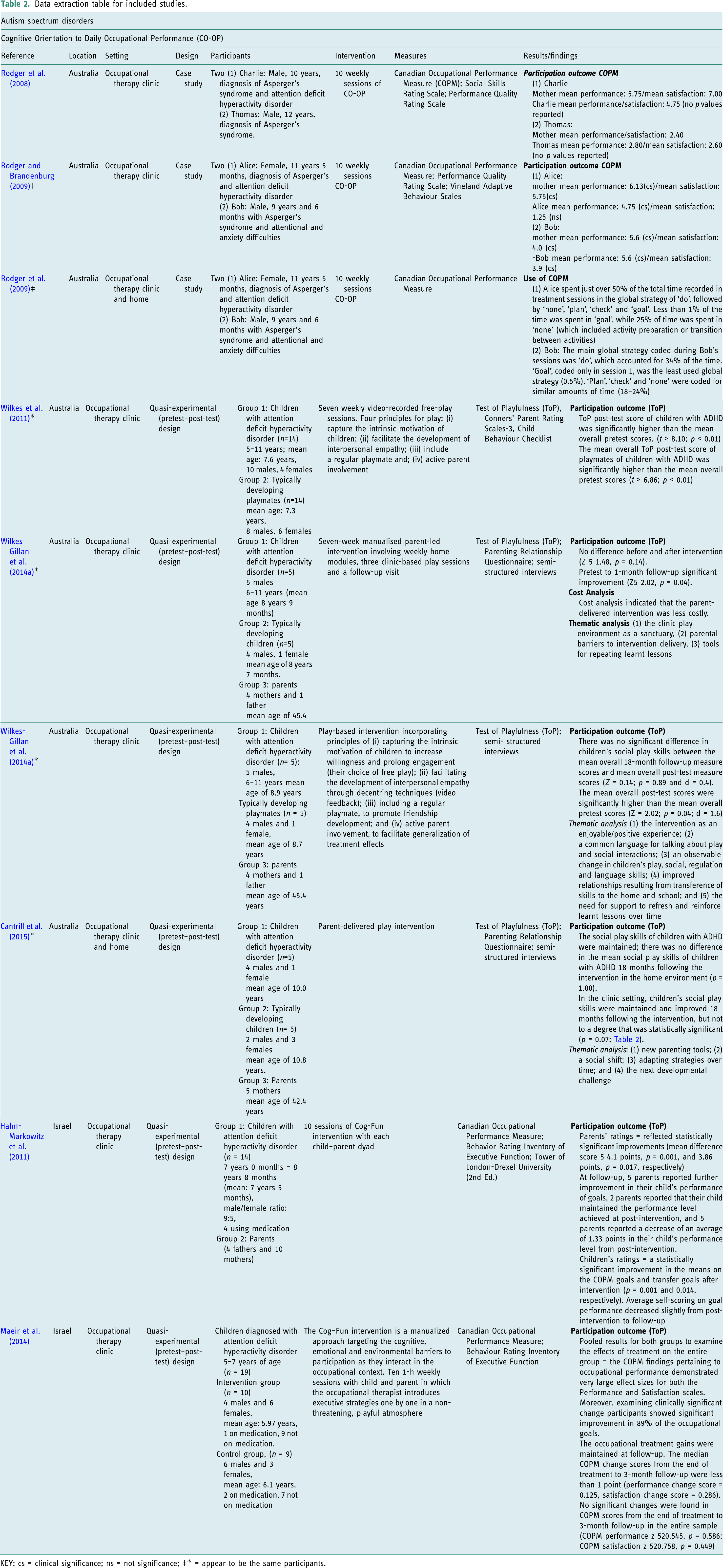
KEY: cs = clinical significance; ns = not significance; ‡* = appear to be the same participants.
Review findings
The review findings are presented in a narrative summary from the nine included studies which evaluated occupation-based/-focused occupational therapy for children and adolescents with a mental health difficulty. The level of heterogeneity in the quantitative data, that is, the case reports and quasi-experimental studies, meant it was not possible to conduct a meta-analysis. This is because these studies evaluated different types of occupational therapy interventions. Whilst some of the outcomes were measured using similar tools, the small number of participants meant pooling the results was not meaningful. The qualitative data analysis reported in three studies (Cantrill et al., 2015; Wilkes-Gillan et al., 2014a; 2014b) did not merit meta-aggregation because the small amount of data and limited reporting of methods of data collection and analysis meant this level of analysis would not have been meaningful. Therefore, to address the review question and the outcomes in the most meaningful way, the findings are presented in a narrative summary according to diagnosis, that is, Asperger’s syndrome and attention deficit hyperactivity disorder, and then occupational therapy intervention, that is, CO-OP or Cog–Fun intervention or play-based intervention (where used).
Asperger’s syndrome
There were three articles reporting an evaluation of one occupational therapy intervention: CO-OP for children and adolescents with Asperger’s syndrome (Rodger and Brandenburg, 2009; Rodger et al., 2008, 2009).
CO-OP
All three articles used a case study approach; two (Rodger and Brandenburg, 2009; Rodger et al., 2008) evaluated the intervention outcomes, and one study (Rodger et al., 2009) was a descriptive evaluation of how the intervention was used. Rodger et al. (2009) is secondary analysis of the same sample as Rodger and Brandenburg (2009). The two intervention outcome studies reported clinically significant outcomes on the Canadian Occupational Performance Measure (COPM) (Law et al., 2014) performance (p) and satisfaction (s) scores, as rated by the parent and child: The mean change rated by Alice was 4.75 (p) and 1.25 (s); mean change rated by Alice’s parent was 6.13 (p) and 5.75 (s); mean change rated by Bob was 5.6 (p) and 3.9 (s); mean change rated by Bob’s parent was 5.6 (p) and 4.0 (s) (Rodger and Brandenburg (2009). In Rodger et al. (2008) the mean change rated by Charlie was 4.75 (p) and 4.75 (s); the mean change rated by Charlie’s parent was 5.75 (p) and 7.0 (s). Mean change rated by Thomas was 2.8 (p) and 2.6 (s); mean change rated by Thomas’s parent was 2.5 (p) and 2.4 (s). In addition, both participants in both studies reported an improvement on the Performance Quality Rating Scale from pre- to post-intervention. The Performance Quality Rating Scale is an observational measure of performance quality in client-selected meaningful activities. It uses a 10-point scale for the therapist to evaluate the quality of task performance. Rodger et al. (2008) completed the Performance Quality Rating Scale with both cases, but only reported results for one case, which showed a 1-point improvement for bed making with using cutlery remaining the same. Rodger and Brandenburg (2009) reported a Performance Quality Rating Scale improvement of 3.5 points for teeth brushing and styling hair, 3 points for cutlery use, 2 points for handwriting for one participant, and 1 point for tying shoelaces, but a 0.2 decrease for handwriting for the other.
The two intervention outcomes studies (Rodger and Brandenburg, 2009; Rodger et al., 2008) both used norm-referenced outcome measures but the studies used different outcome measures. The Social Skills Rating Scale (Gresham and Elliot, 1990) used by Rodger et al. (2008) is a measure of social skills, problem behaviours and academic competence. The Social Skills Rating Scale scores were inconsistent across the child, teacher and parent ratings. The Vineland Adaptive Behavior Scale (Sparrow et al., 2005) used by Rodger and Brandenburg (2009) recorded functioning across the domains of communication, daily living, socialization and motor skills. This study reported similar changes on the Vineland Adaptive Behavior Scale for their two cases: minimal change to standard scores on socialization, moderate change for communication and considerable change for daily living skills.
The focus of one article (Rodger et al., 2009) was to explore the CO-OP intervention global and domain-specific strategies and types of guidance utilized to improve the task performance of participants with Asperger’s Syndrome. This study used independent data coding of video footage by two trained therapists, with reported excellent inter-rater agreement. The study reported that both study participants spent most (50% and 34%) of their treatment sessions in the ‘do’ global strategy and least time (1% and 0.5%) in the ‘goal’ strategy. The study concluded that the two children with Asperger’s syndrome were able to utilize cognitive strategies to effectively solve their motor performance problems. CO-OP intervention appears to have potential as an effective intervention for children with Asperger’s syndrome.
Attention deficit hyperactivity disorder
Six articles reported on two different occupational therapy interventions, the PLF intervention (Cantrill et al., 2015; Wilkes et al., 2011; Wilkes-Gillan et al., 2014a; 2014b) and the Cog–Fun intervention (Hahn-Markowitz et al., 2011; Maeir et al., 2014) for children and adolescents with attention deficit hyperactivity disorder.
Ultimate guide to PLF
Two studies (Cantrill et al., 2015; Wilkes et al., 2011) using similar pretest–post-test research design evaluated the impact of the PLF intervention for children with attention deficit hyperactivity disorder, using the same Test of Playfulness (Bundy et al., 2001) outcome measure. One of the studies (Wilkes et al., 2011) also used mixed methods and collected qualitative data. One of these studies evaluated the PLF intervention delivered by therapists, and the second study (Cantrill et al., 2015) evaluated the PLF intervention delivery by parents. Two further studies (Wilkes-Gillan et al., 2014a; 2014b) evaluated the ongoing impact of each intervention delivery method at 18 months; these studies also used a mixed methods research design, including the Test of Playfulness (Bundy et al., 2001) as an outcome and parental interview. The therapist-delivered intervention study (Wilkes et al., 2011) showed improved Test of Playfulness scores post-intervention for children with attention deficit hyperactivity disorder with a large effect size, and children maintained their Test of Playfulness scores after 18 months (Wilkes-Gillan et al., 2014b). The study findings suggested that the therapist-delivered PLF intervention was effective in developing social play skills and had long-term efficacy. The Test of Playfulness outcomes for the parent-delivered intervention study (Wilkes-Gillan et al., 2014a) showed significantly improved social play skills as measured by the Test of Playfulness post-intervention (Z = 2.02; p = 0.04) and appeared to be maintained over time (Cantrill et al., 2015). The parent-delivered intervention successfully improved play skills a month after therapy was completed (not immediately post-intervention). In the parent-delivered intervention follow-up study (Wilkes-Gillan et al., 2014a), two of the study authors were identified as the therapists delivering the intervention, providing the potential for bias. The therapists delivering the interventions were not identified in the other studies.
Qualitative findings were reported in three mixed methods articles (Cantrill et al., 2015; Wilkes et al., 2011; Wilkes-Gillan et al., 2014b). These data were collected using semi-structured interviews with parents of the children with attention deficit hyperactivity disorder. Interviews focused on the parents’ experiences of the intervention, including its benefits and challenges, though specific examples of questions were not reported. The interviews were conducted by telephone by a researcher unknown to the family, at 1 month (Wilkes et al., 2011) or 18 months (Cantrill et al., 2015; Wilkes-Gillan et al., 2014b) after the intervention. All interviews were transcribed verbatim, and all studies reported the use of interpretive thematic analysis. Overall, the qualitative findings report parents’ positive experiences of the therapist and of the interventions. Parents reported observable changes in their child’s play and that it gave them new skills to read and support their child. The home-based parent-delivered intervention (Cantrill et al., 2015) placed additional demands on family life that challenged relationships. Parents reported wanting additional support to further adapt the strategies as their child developed and in different contexts.
Cognitive–functional intervention
Two studies (Hahn-Markowitz et al., 2011; Maeir et al., 2014) using a similar pretest–post-test quantitative research design, evaluated the Cog–Fun intervention, for children with attention deficit hyperactivity disorder, using the COPM (Law et al., 2014) and the Behavior Rating Inventory of Executive Functions (Gioia et al., 2000) as outcome measures. The COPM (Law et al., 2014) showed statistically significant improvements in mean parent and child ratings in both studies, with large effect sizes (Hahn-Markowitz et al., 2011; Maeir et al., 2014). The Behavior Rating Inventory of Executive Functions parent scores in both studies showed statistically significant improvements after intervention (Hahn-Markowitz et al., 2011; Maeir et al., 2014). One study showed that Behavior Rating Inventory of Executive Functions scores were maintained at a 3-month follow-up (Hahn-Markowitz et al., 2011). The Behavior Rating Inventory of Executive Functions teacher score was only used in one study (Hahn-Markowitz et al., 2011) and also showed statistically significant improvement after intervention, with a small decline at follow-up.
Discussion and implications
This study sought to identify the effectiveness of occupational therapy interventions that are occupation-based/-focused for children and adolescents with mental health problems. Considered as a whole, the evidence for the effectiveness of occupational therapy with children and adolescents with mental health problems is extremely limited. There is no high-quality evidence for occupation-based/-focused occupational therapy interventions for children and adolescents with mental health difficulties, including anxiety, depression, eating disorders, bipolar disorder, post-traumatic stress disorder and psychosis. The available evidence is confined to small-scale studies of occupational therapy interventions for those with Asperger’s syndrome or attention deficit hyperactivity disorders. For children and adolescents aged nine to 12 years of age who have a diagnosis of Asperger’s syndrome, the CO-OP intervention appears to improve daily living tasks. For children and adolescents with attention deficit hyperactivity disorder aged five to 11 years, the picture is similar, but there is emerging evidence that the PLF intervention is effective in improving play skills, which are maintained over time. Whilst there is qualitative evidence that the PLF intervention is enjoyed by children and valued by parents, parents also reported some limitations as to the feasibility of the intervention delivery. For children with attention deficit hyperactivity disorder aged seven to 11 years, there is limited evidence that the Cog–Fun intervention appears to improve occupational performance but there are a number of limitations in the study, such as a lack of blinding, which means these findings have to be regarded with caution as they are open to bias.
Overall, the limited number of small-scale studies, with low numbers of participants and conducted in specific contexts means it is not possible to make recommendations for occupational therapists working with children and adolescents experiencing mental health disorders. The CO-OP intervention for children with Asperger’s syndrome and PLF interventions and the Cog–Fun intervention with children with attention deficit hyperactivity disorder appear to be promising interventions.
Research is needed to develop and evaluate effective occupation-based/-focused occupational therapy interventions for children and adolescents with mental health difficulties, including anxiety, depression, eating disorders, bipolar disorder, post-traumatic stress disorder and psychosis. Further research is needed to establish the effectiveness of the CO-OP intervention for children with Asperger’s syndrome and the PLF interventions and the Cog–Fun intervention with children with attention deficit hyperactivity disorder require further large scale randomized controlled trials. It is recommended that high-quality programmes of research are developed.
There were some limitations to the study. The studies included in this review varied in methodological quality, which impacted on the overall results and conclusions that could be drawn. No randomized controlled trials could be included and the remaining studies, case reports and quasi-experimental studies, were very low quality. The variety of interventions, sample size, sampling strategy and outcome measures used meant meta-analysis was not possible. The qualitative data available was limited in quantity with minimal supporting detail about method to make meta-aggregation meaningful. Equally, as only studies published in the English language were included, other important studies may have been missed.
Conclusion
This review has found no high-quality evidence for occupation-based/-focused occupational therapy interventions for children and adolescents with common mental health conditions. Limited evidence exists for occupational therapy interventions for attention deficit hyperactivity disorder and Asperger’s syndrome, but further research will be needed before there is sufficient weight to make recommendations for practice.
Key findings
1. There is limited evidence for the effectiveness of occupational therapy interventions for children and adolescents with Asperger’s syndrome or attention deficit hyperactivity disorder.
2. There is no evidence for the effectiveness of occupational therapy interventions for children and adolescents with common mental health disorders.
What the study has added
Recommendations for occupational therapists working with children and adolescents experiencing common mental health disorders are not possible due to the limited number of small-scale studies; rigorous research is indicated.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study received funding from the UKOTRF/Elizabeth Casson Trust.