
Abstract
Objective
The aim of this systematic review was to investigate the efficacy of sensory discrimination training (SDT) on sensorimotor performance in individuals with a neurological condition affecting the central nervous system.
Methods
MEDLINE, CINAHL, EMBASE, AMED, CENTRAL, PsychINFO, Scopus, OT Seeker, PEDro, ETHOS, Web of Science and OpenGrey were systematically searched for appropriate randomised controlled trials (RCTs). Included studies were assessed for risk of bias, and the quality of the evidence was rated using the GRADE approach. The protocol was registered on PROSPERO (CRD42017055237).
Results
Six RCTs met the inclusion/exclusion criteria. All studies used manual tactile discrimination to retrain somatosensation. Somatosensory effect sizes (0.12–0.92) and motor function effect sizes (0.12–10.39) ranged from trivial to large with narrative analysis revealing some between-group difference in favour of the intervention group. However, the total sample size (n = 220) was relatively small, and the quality of the included studies was low.
Conclusions
SDT may have potential to be an efficacious treatment option for improving sensorimotor performance in individuals with neurological disease. However, at present there is limited evidence on which to base any firm clinical recommendations.
Keywords
Background
Altered or lost somatosensation (tactile and proprioception) is common in individuals who have a central nervous system condition including stroke (Kessner et al., 2019); Parkinson’s disease (PD) (Gorst et al., 2019); multiple sclerosis (MS) (Jamali et al., 2017) and focal dystonia (Konczak and Abbruzzese, 2013). Since somatosensation guides movement and minimises the risk of injury, a loss of somatosensation has a significant impact on sensorimotor function including that of the upper limb, balance and mobility and subsequently participation and independence in activities of daily living (ADL) (Carey et al., 2018). This represents a significant economic challenge from a health and social care point of view, especially due to the progressive and long-term nature of these conditions (Rabert et al., 2012). Since the primary purpose of occupational therapy is to support people in meaningful and purposeful occupation, including participation in ADL, this topic is a specific area of concern for the profession (Wæhrens, 2015).
Cutaneous receptors within the skin on the hands and feet transmit signals to the primary somatosensory cortex (S1), from which the brain processes if a stimulus is present and where it is located, a process paramount for effective upper and lower limb sensation and movement. S1 is organised as a map containing primary representations of specific locations on the skin. These representations are plastic, and neurons can alter and take on a different representation of a bodily location in the presence of neurological damage or disease (Brooks and Medina, 2017).
Sensory discrimination training (SDT), often referred to as somatosensory retraining, involves tasks of somatosensory recognition and discrimination that focus on the development and relearning of sensory motor performance through the promotion of S1 neuroplasticity. SDT has been shown to have potentially positive outcomes in a number of neurological conditions including phantom limb pain (Flor et al., 2001), stroke (Carey et al., 2011), PD (Elangovan et al., 2018), focal dystonia (Byl et al., 2003) and MS (Kalron et al., 2013).
Four systematic reviews have investigated the efficacy of SDT for people following stroke (Chia et al., 2019; Schabrun and Hillier, 2009; Serrada et al., 2019; Turville et al., 2019). They found some evidence towards its effectiveness for improving somatosensory function in the lower and upper limbs but ultimately conclude that this is limited due to poor-quality study designs, inadequately powered with inconsistencies in outcome measurement tools. All four studies highlight the need for further research with rigorous methods, specifically randomised controlled trials (RCTs). No systematic reviews have investigated the efficacy of SDT in the wider population of individuals with a neurological condition. Such a systematic review would help to guide future research and clinical practice in this field. Therefore, the aim of this systematic review was to investigate the efficacy of SDT on sensorimotor performance in individuals with a neurological condition affecting the central nervous system.
Methods
Procedure
The Cochrane Handbook for systematic reviews (Higgins and Green, 2011; Higgins et al., 2020a, 2020b) was used to guide this review, and it is reported in keeping with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2009). The protocol has been registered on PROSPERO (CRD42017055237) (National Institute for Health Research, 2018). The Population, Intervention, Comparison, Outcome and Study (PICOS) framework was used to structure the systematic literature search and develop inclusion/exclusion criteria (Thomas et al., 2020).
Participants
Studies that included adult men and women aged ≥18 years with a diagnosed central neurological condition defined as any long-term condition ‘with a pathological process directly affecting the central nervous system (post-traumatic, degenerative, ischaemic or neoplastic), such as MS, spinal cord injury, cerebrovascular diseases, PD (Coggrave et al., 2014) and dystonia’. Acute conditions or those that only affect the peripheral nervous system were excluded.
Intervention
Due to the lack of a standardised definition for SDT, for the purpose of this review, SDT was operationally defined as having three components (1) the delivery of an external stimulus (e.g. mechanical or electrical) to an individual, which requires (2) a judgement by the individual about a characteristic of that stimulus (e.g. localisation or discrimination of texture) and (3) immediate feedback on whether or not the judgement is correct/incorrect. The feedback is usually provided by a trainer/therapist. The intervention requires the active participation of the individual with the stimulus, rather than simply the passive receipt of the stimulation. SDT that involved the delivery of visual, auditory or olfactory stimuli were excluded. Single session and multiple session interventions were included. Studies where SDT was delivered in combination with other interventions were included if SDT was the sole difference in treatment received between groups.
Control
No treatment (true control), usual care (e.g. standard physiotherapy or occupational therapy) or placebo (e.g. pure passive sensory stimulation with no active involvement from the participant) control groups were all acceptable.
Outcomes
The primary outcome of interest was sensorimotor performance such as measures of local motor or sensory impairments including but not limited to two-point discrimination, postural sway, balance, graphesthesia, texture discrimination, joint position sense and tactile object recognition.
Secondary outcome measures did not form part of the eligibility criteria but included measures that evaluated any aspect of health and well-being.
Study design
Only RCTs were included in order to reduce bias and maximise the quality of the evidence (Higgins et al., 2011; McKenzie et al., 2020; Nolan and Bradley, 2008). This included randomised parallel-group controlled trials where the primary outcome was the difference between SDT and the non-SDT control phase. Non-randomised controlled trials were excluded to reduce the risk of bias in this review. The age of the studies was not limited. Studies written in any language and published in any country were eligible for inclusion.
Search strategy
In accordance with the Cochrane Collaboration process (Higgins and Green, 2011), the search strategy was designed with support from a specialist librarian. Large generic databases and subject-specific databases were used to ensure a comprehensive literature search (Bettany-Saltikov, 2010; Dickersin et al., 1994; Lefebvre et al., 2011). The following electronic databases were searched applying no language or date restrictions: the Cochrane Central Register of Controlled Trials (CENTRAL), CINAHL, Allied and Complementary Medicine Database (AMED), MEDLINE, EMBASE, Web of Science (science and social science citation index), Scopus, PEDro, PsycINFO, OT Seeker, ETHOS and OpenGrey. Additionally, the reference lists of key studies were hand searched (Dickersin et al., 1994).
Review question based on the PICOS model and relevant search terms.
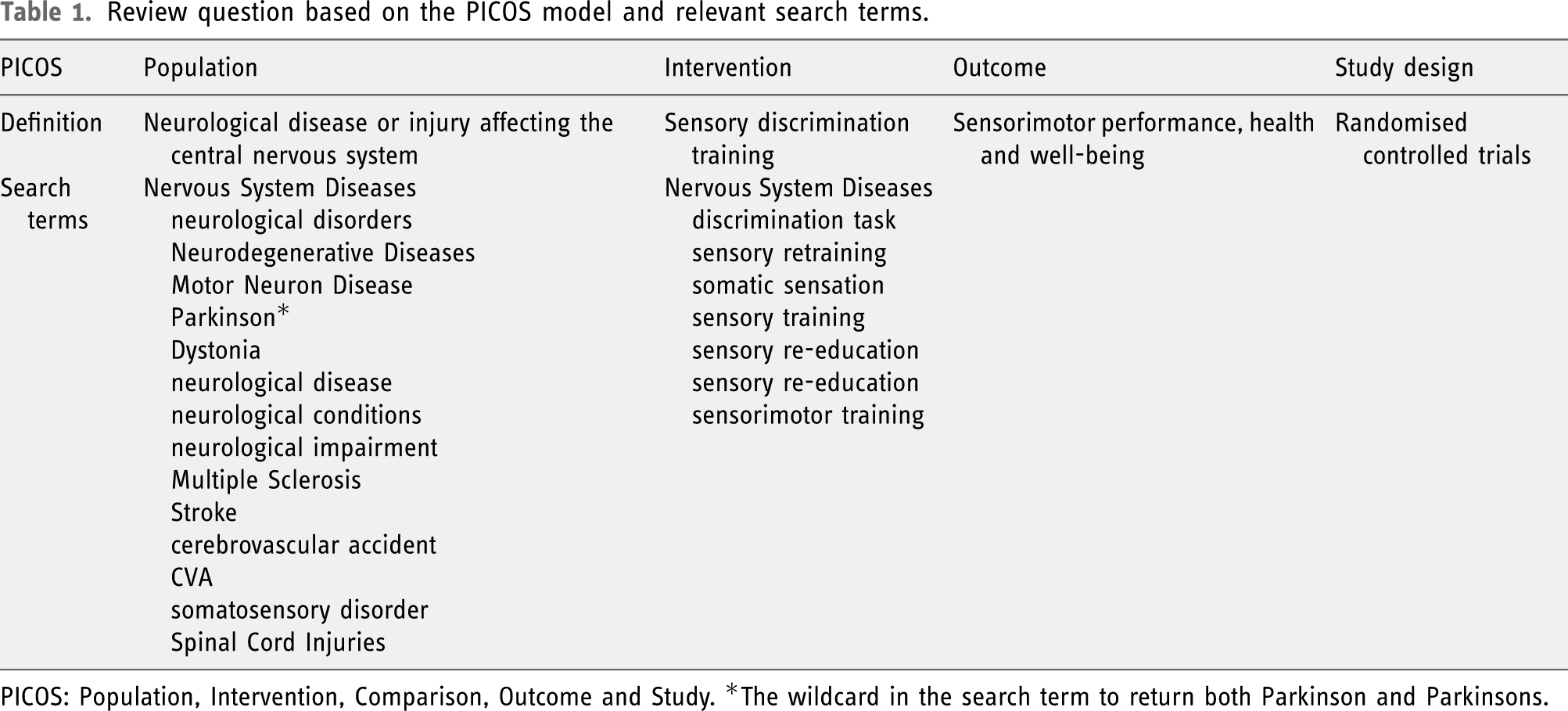
PICOS: Population, Intervention, Comparison, Outcome and Study. *The wildcard in the search term to return both Parkinson and Parkinsons.
Methodological quality assessment
Quality assessment was undertaken independently by two reviewers (ST and CR) using the Cochrane collaboration’s risk of bias tool which is a domain-based evaluation of potential biases in RCTs in which seven risk of bias questions are marked for a low, high or unclear risk of bias (Higgins et al., 2011). Where there was insufficient information for appraisal of bias, attempts were made to contact the original authors for further information using the contact details provided within the articles; however, this was unsuccessful on each occasion.
Data collection process
At least two review authors (ST, JK and MAJ) independently extracted data from the included studies using an adapted version (created by ST for topic specificity) of the Cochrane Collaboration’s (Higgins et al., 2011) tool for data extraction and included data relating to study eligibility, methodological characteristics of included studies, participant characteristics, intervention group characteristics, outcome characteristics, risk of bias assessment, data analysis and key study conclusions. Results were compared between review authors, and disagreement was resolved by discussion.
Data analysis and synthesis
Due to the degree of heterogeneity among the studies, a narrative synthesis was used as traditional meta-analysis was not considered appropriate (Bettany-Saltikov, 2010; Deeks et al., 2011). However, where possible, the effect size (ES) was calculated for each of the outcomes within each included study, to support the narrative synthesis and provide useful statistical information on results. This is advised by the Cochrane Handbook when studies assessing the same outcome measure it in different ways (McKenzie and Brennan, 2020). In this review, the included studies used various different outcome measurement tools to assess the primary outcome of sensorimotor performance. This method of calculating the ES enabled standardisation of the outcome results of the studies to a uniform scale, to facilitate quantifying the estimate of the effect and help interpret the clinical relevance of the mean treatment effect of the specific intervention in each individual study. The ES expresses the magnitude of the intervention effect in each study relative to the between-participant variability in outcome measurement tools. The ES was calculated by dividing the difference in mean outcome post-intervention between the two groups by the pooled baseline SD, with ESs of 0.2, 0.5 and 0.8 considered to be small, medium and large, respectively (Cohen, 2013). As advised in the Cochrane Handbook (Higgins et al., 2020a) two authors (ST and CR) assessed the quality of evidence through the use of the GRADE approach (Ryan and Hill, 2016; Schünemann et al., 2020) considering five domains: risk of bias, inconsistency, indirectness, imprecision and publication bias. An overall judgement was made across studies.
Results
Summary of included studies.
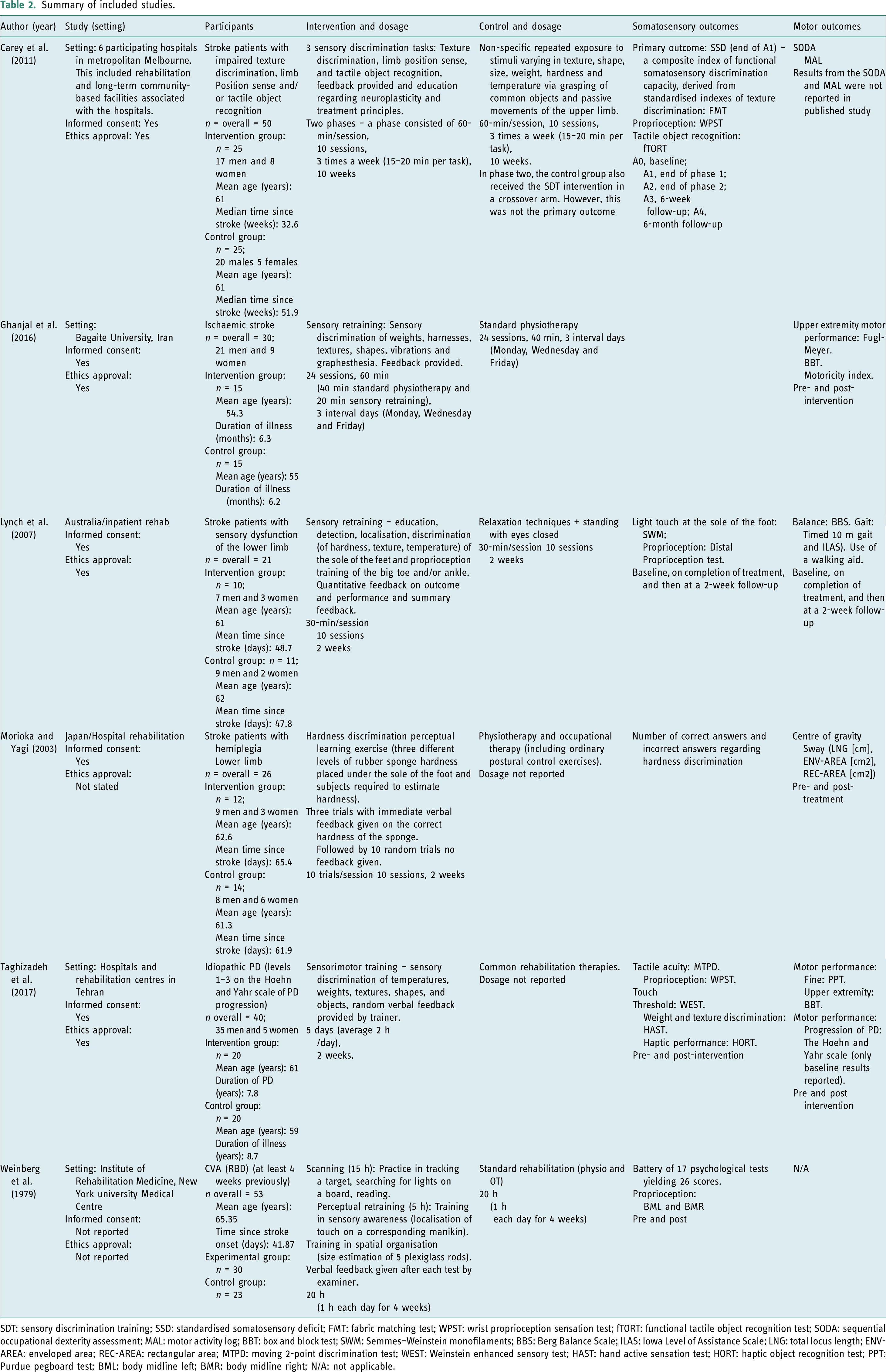
SDT: sensory discrimination training; SSD: standardised somatosensory deficit; FMT: fabric matching test; WPST: wrist proprioception sensation test; fTORT: functional tactile object recognition test; SODA: sequential occupational dexterity assessment; MAL: motor activity log; BBT: box and block test; SWM: Semmes–Weinstein monofilaments; BBS: Berg Balance Scale; ILAS: Iowa Level of Assistance Scale; LNG: total locus length; ENV-AREA: enveloped area; REC-AREA: rectangular area; MTPD: moving 2-point discrimination test; WEST: Weinstein enhanced sensory test; HAST: hand active sensation test; HORT: haptic object recognition test; PPT: Purdue pegboard test; BML: body midline left; BMR: body midline right; N/A: not applicable.
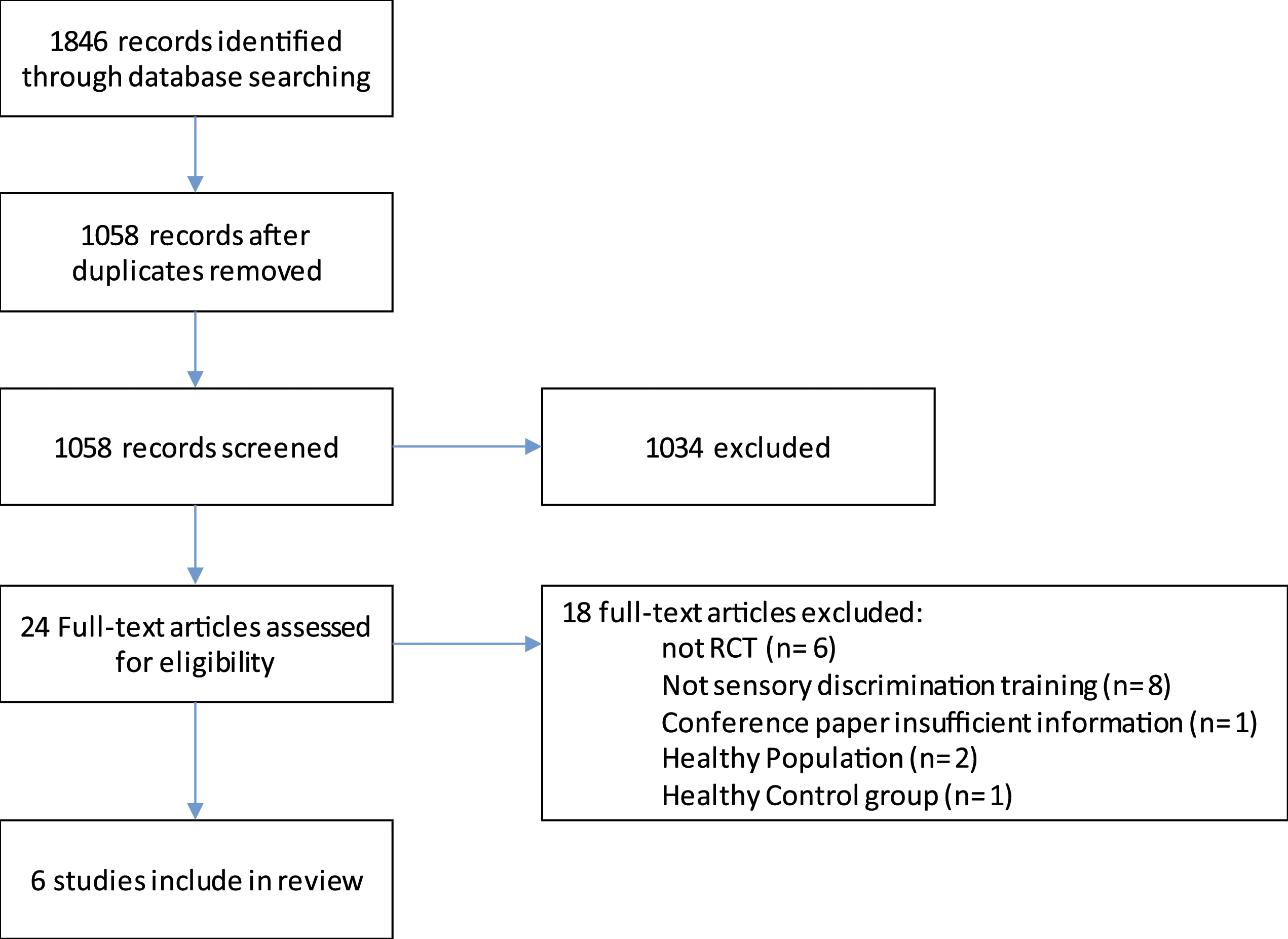
PRISMA flow chart.
Characteristics of included studies
A total of 220 adults with a neurological condition and subsequent sensorimotor deficit (40 with PD and 180 who had experienced a stroke) participated in the six included studies. In five of the studies, the gender ratio was reported, and these studies had a higher male to female ratio. The mean age of the participants ranged from 55 to 65 years. Five studies investigated SDT for people following a stroke (Carey et al., 2011; Ghanjal et al., 2016; Lynch et al., 2007; Morioka and Yagi, 2003; Weinberg et al., 1979) and one for people with PD (Taghizadeh et al., 2017). Time since stroke ranged from 6.8 weeks (Lynch et al., 2007) to 51.9 weeks (Carey et al., 2011). Five studies were conducted in hospital settings and one in a university setting (Ghanjal et al., 2016). Studies were conducted in the United States, Australia, Iran and Japan. All six studies used manual tactile discrimination including hardness, temperature, weights, textures, shapes, objects, vibrations, graphesthesia and localisation as the stimulus for the experimental intervention. The duration of individual SDT sessions ranged from 30 to 120 min, with a range of 10–20 sessions, with treatment periods from 2 to 10 weeks in duration.
All six studies assessed sensorimotor performance using a variety of outcome measures, with the box and block test, wrist proprioception sensation test and Semmes–Weinstein monofilaments being the most commonly used (two studies each). None of the six studies used secondary outcome measures as defined in this review. All studies recorded a measure at baseline and immediately post treatment. The follow-up outcome measurement period ranged from 2 weeks (Lynch et al., 2007) to 6 months (Carey et al., 2011) post-treatment.
Adverse effects reporting
Only one study (Carey et al., 2011) reported that there were no adverse events associated with the intervention, and the other five studies made no statements regarding adverse events. Three studies (Ghanjal et al., 2016; Taghizadeh et al., 2017; Weinberg et al., 1979) did not report retention (withdrawals and exclusions). Morioka and Yagi (2003) reported that two participants in the experimental group were lost from the study due to discharge prior to completion, compared to zero lost in the control group. Lynch et al. (2007) reported one participant was lost to follow-up in the experimental group due to discharge to their own country prior to final assessment, and one discontinued sensory retraining and standard care as acutely unwell, compared to zero lost to the control group. Carey et al. (2011) reported one participant was lost to follow-up in the intervention group due to being unwell and two were lost in the control group due to being unwell, but zero participants discontinued the intervention.
Analysis and effect measures
Meta-analysis was not carried out as the delivery of the interventions, the specific outcome measures used and the targeted body parts and specific populations were too diverse. Standardised ESs were calculated as a means of quantifying effectiveness. ESs are displayed in Figure 2 and are discussed below. Effect sizes for each outcome measure. NDH: non-dominant hand; DH: dominant hand; PPT: Purdue pegboard test; WPST: wrist proprioception test; HAST: hand active sensation test; HORT: haptic object recognition test; SSD: standardised somatosensory deficit; BML: body midline left; BMR: body midline right.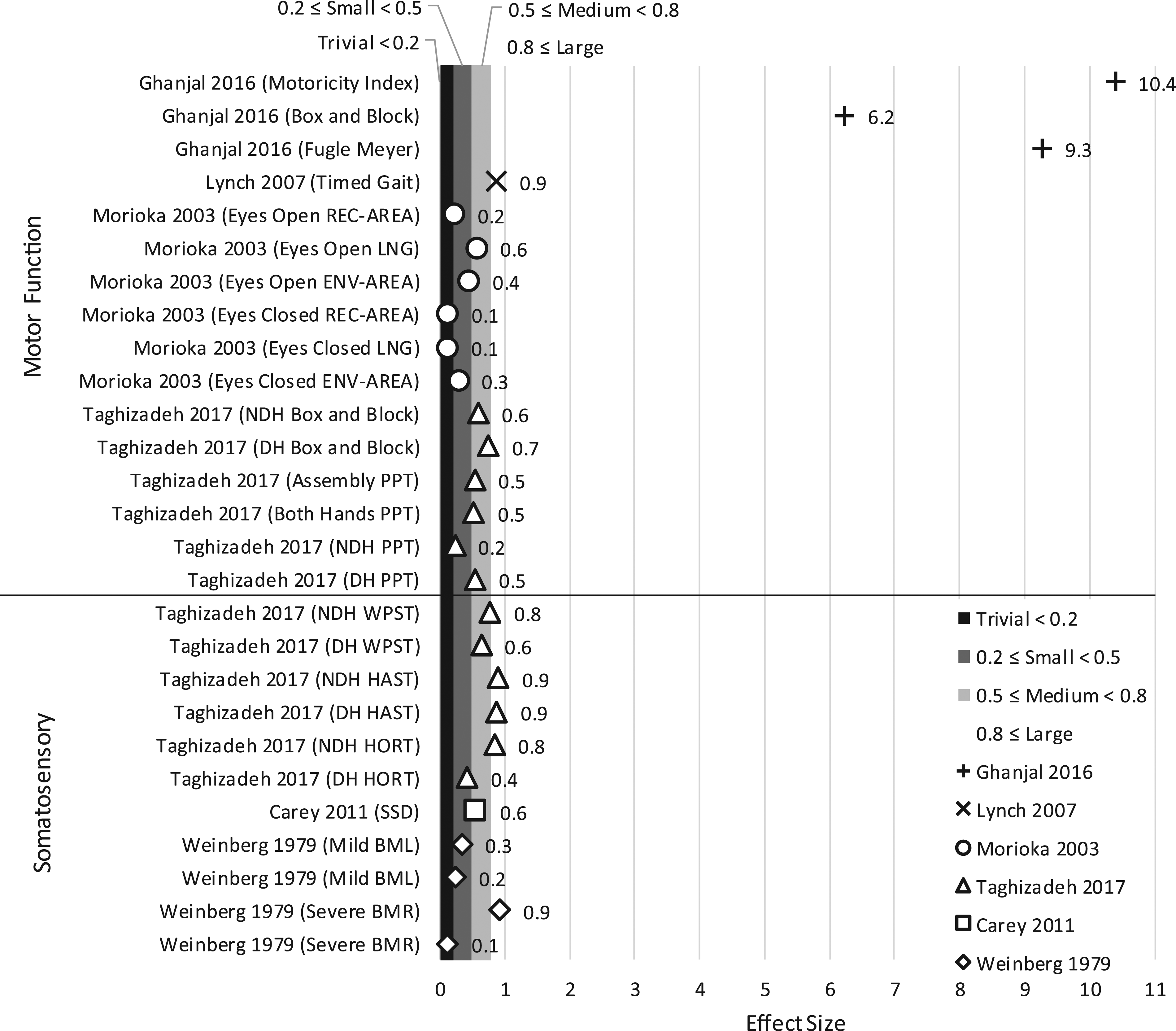
Methodological quality summary
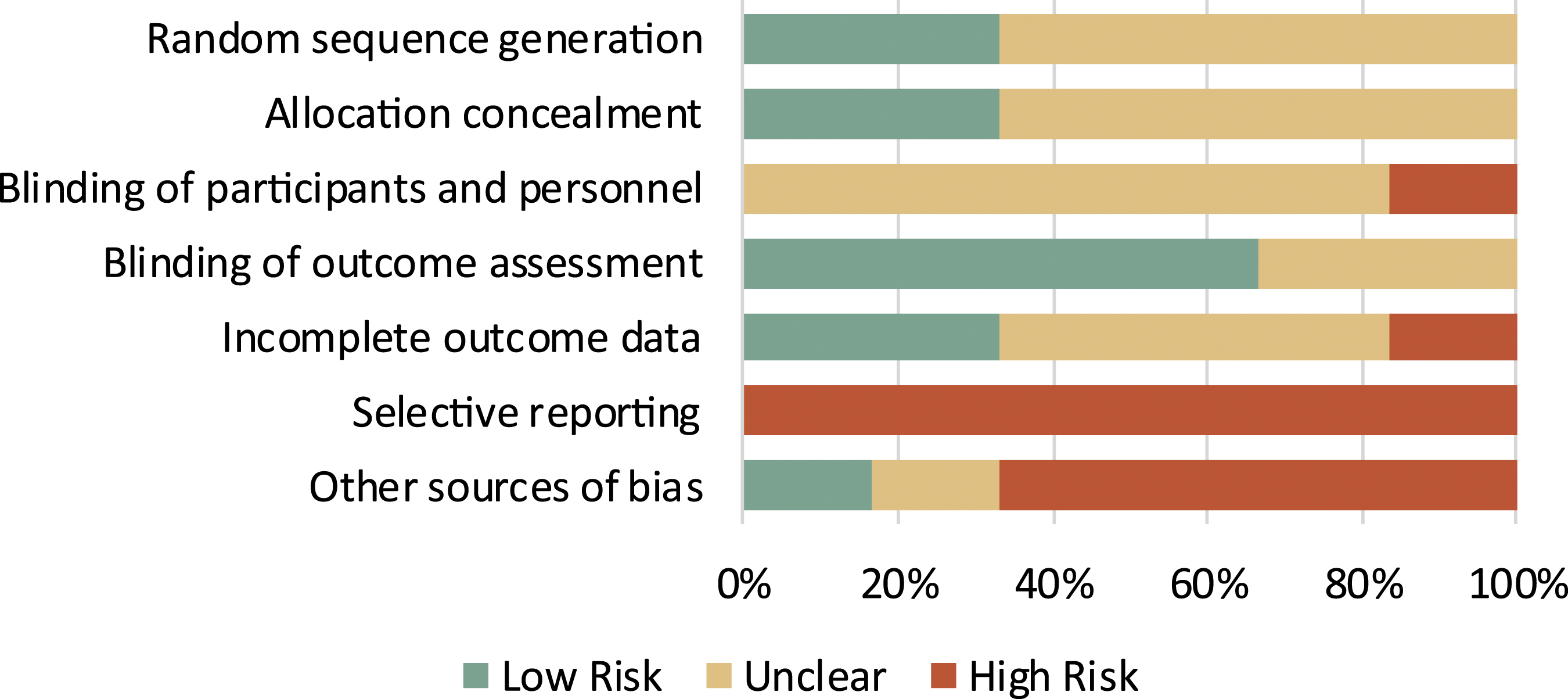
All six included studies were deemed to possess a high risk of bias (Figures 3 and 4). In five of the six studies, there was a considerable lack of information. Carey et al. (2011) was the only trial not scoring an ‘unclear’ in any of the components of the tool demonstrating more comprehensive reporting. Risk of bias summary for each study based on GRADE. Risk of bias graph for each study based on GRADE: each risk of bias component is presented as percentages across all included studies.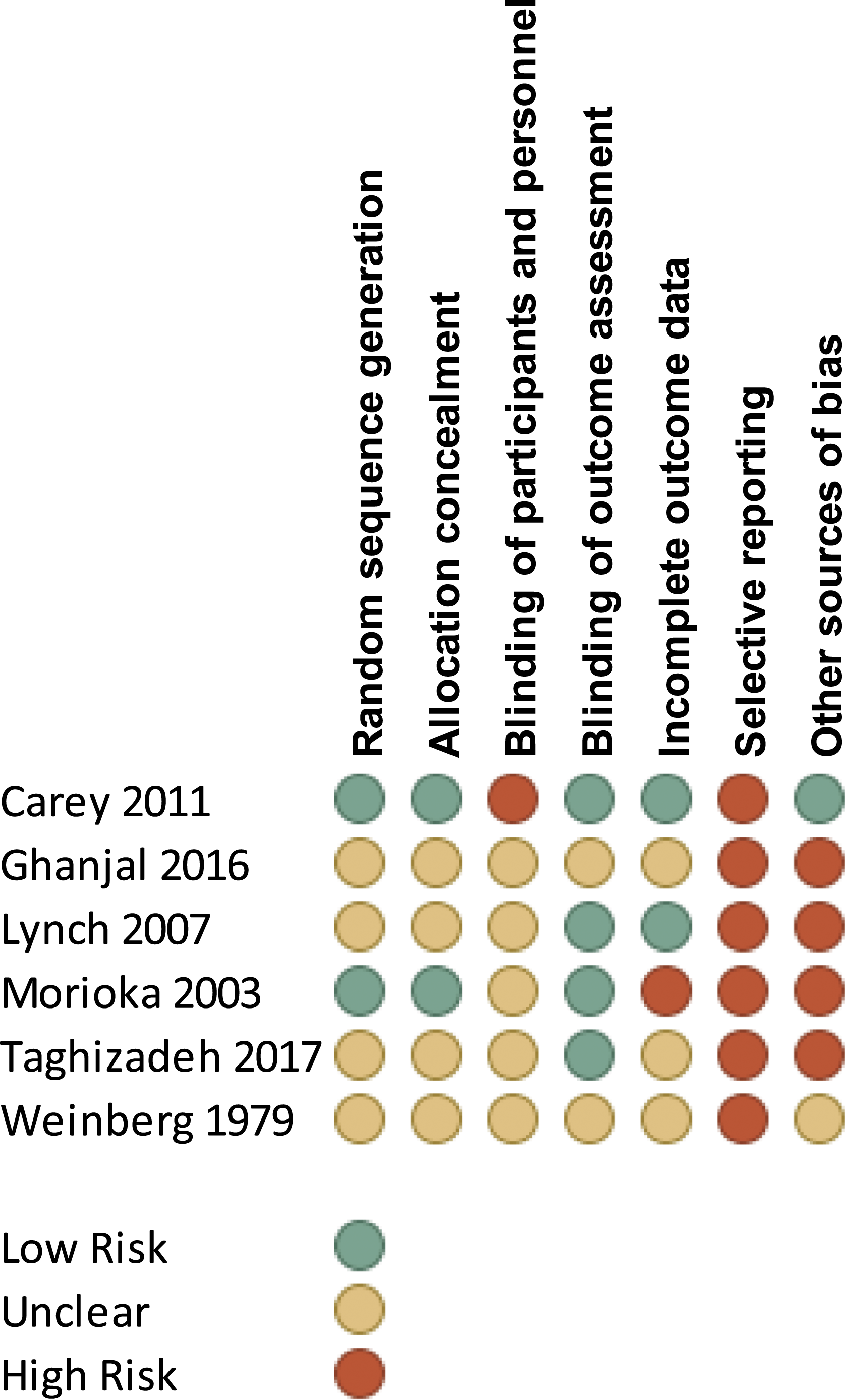
Selective reporting bias was high risk in all six studies due to the fact that only one study published a protocol, and the single study that did publish a protocol (Carey, 2005) did not report in the full paper data from three secondary outcome measures specified in the protocol.
Summary of findings for included stroke RCTs (GRADE).
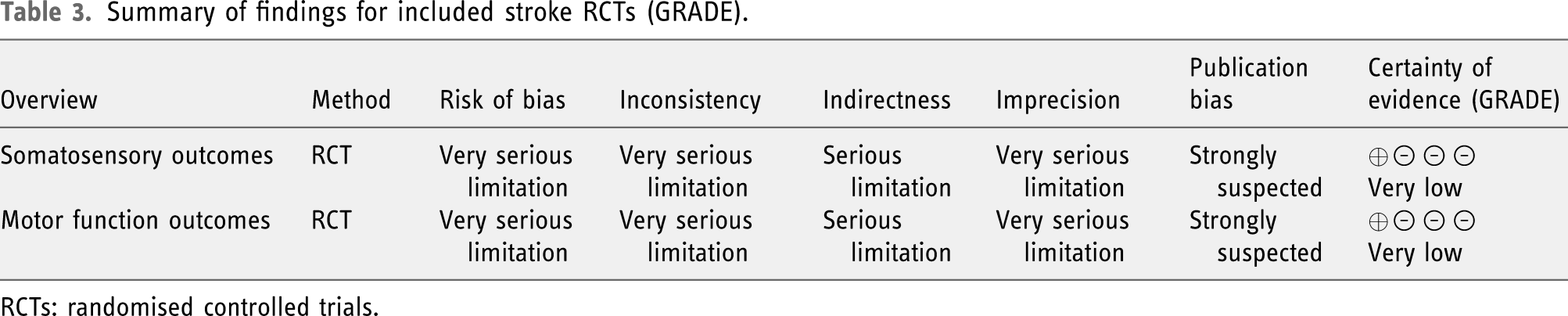
RCTs: randomised controlled trials.
Summary of findings for included PD RCTs (GRADE).
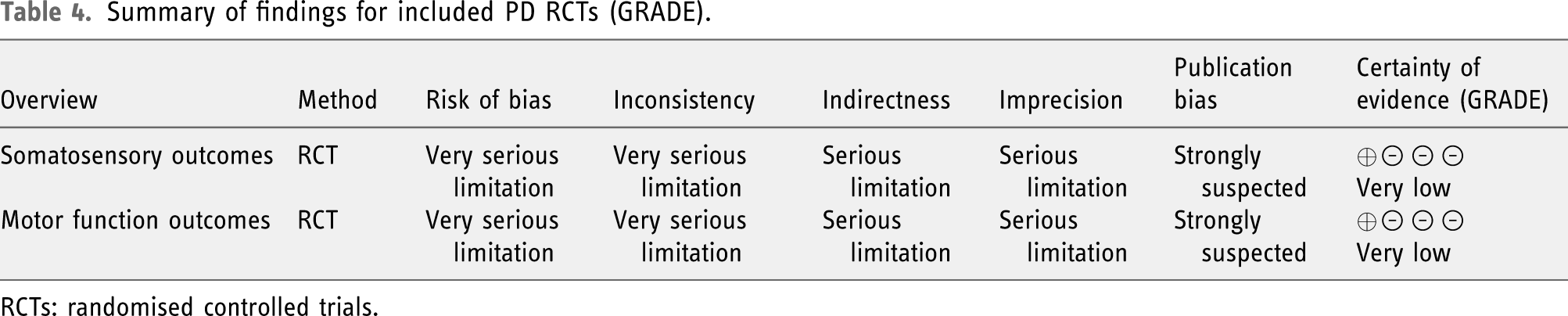
RCTs: randomised controlled trials.
Narrative synthesis of included studies
Five studies (Carey et al., 2011; Ghanjal et al., 2016; Lynch et al., 2007; Morioka and Yagi, 2003; Weinberg et al., 1979) assessed the efficacy of SDT in people who had experienced a stroke affecting the upper and lower limb, and one study (Taghizadeh et al., 2017) looked at individuals with PD. All interventions focussed solely on retraining somatosensation accept one study (Weinberg et al., 1979) that also used additional therapeutic modalities to focus on scanning and spatial organisation to target visual neglect and thus administered associated outcome measures. Although these additions are reported in Table 2, only the training in sensory awareness and relevant perceptual outcomes (body midline left and body midline right) were investigated in this review to keep the review focussed on its primary objective to evaluate sensorimotor performance.
All six studies used SDT activities in the intervention that differed from the assessment outcome measures. In all studies apart from one (Morioka and Yagi, 2003), the intervention targeted retraining of more than one somatosensory modality. Morioka and Yagi (2003) only targeted retraining hardness discrimination. In all six studies, the SDT intervention focussed on one or more of the following somatosensory modalities: tactile detection, localisation, discrimination, object recognition and proprioception.
On average SDT occurred for a total of 17.3 sessions (SD = 8.6), across 2–10 weeks, 3–5 times per week. The average treatment session lasted 57 min (SD = 40.2), with an average of 16.8 (SD = 11.3) total treatment hours. The intervention was delivered one-to-one by a trained therapist in all six studies, but there was insufficient/limited information regarding characteristics of the therapists (e.g. their training, experience and specialist skills).
Outcome results
Included stroke studies
Somatosensory skills
A variety of somatosensory outcome measures were used in four of the studies (Table 2), but the intervention effect could be quantified for only two of these (Carey et al., 2011; Weinberg et al., 1979). All somatosensory outcomes improved with training relative to control groups and ESs are displayed in Figure 2 (Carey et al., 2011; Weinberg et al., 1979). The total sample for this outcome category (two studies) was small (n = 103).
In one study (Lynch et al., 2007), narrative analysis suggested improvements over time in light touch threshold at three points of the foot (heel, lateral border and big toe), but no significant difference was observed between the intervention and control group (Lynch et al., 2007). However, a between-group difference was detected in light touch sensation at the first metatarsal at follow-up, with the intervention group showing significant improvements over the control group. No significant difference in proprioception was observed over time or between groups. Again, the sample for this study was very small (n = 21). Morioka and Yagi (2003) observed that the mean number of incorrect answers given by the intervention group during the hardness discrimination exercise, decreased significantly through the training period (p < 0.01) suggesting an improvement in hardness discrimination.
Overall, there was very low-quality evidence from the five studies supporting the efficacy of SDT for somatosensory discrimination skills in the stroke population compared to a control treatment in the immediate to medium term. The quality of the evidence was downgraded due to very serious limitations in terms of risk of bias, inconsistency and imprecision (Tables 3 and 4).
Motor function
Several measures of motor function were used (Table 2) to assess postural sway, balance, gait, upper extremity function and general motor performance within three studies (Ghanjal et al., 2016; Lynch et al., 2007; Morioka and Yagi, 2003). All areas improved with training and ESs are displayed in Figure 2. Motor function ESs ranged from 0.12–10.39, spanning a trivial to large intervention effect in favour of the intervention group. The total sample was small (n = 75).
It was not possible to calculate ESs for all the motor function measures used in one study (Lynch et al., 2007). However, narrative analysis suggested an improvement in balance detected through the Berg Balance Scale (BBS) which improved from baseline to the end of treatment in both the control and intervention groups (p < 0.005). However, there was no significant difference in scores between groups at any time period. Lynch et al. (2007) also found that the scores for use of a walking aid over the 10 m timed walk test decreased over time, indicating that the walking aids required became progressively less supportive over time suggesting an improvement in balance. However, they also found no significant change over time or between groups in the amount of assistance participants required from the therapist to walk 10 m.
Overall, there was very low-quality evidence from three studies supporting the efficacy of SDT for motor function in the stroke population compared to a control treatment in the immediate to medium term. The quality of the evidence was downgraded due to very serious limitations in terms of risk of bias, inconsistency and imprecision (Tables 3 and 4).
Included PD studies
Somatosensory skills
Five somatosensory outcomes measures were used in the single PD study (Taghizadeh et al., 2017) as shown in Table 2. ES was quantified for three of these ranging from 0.42–0.90 spanning a small to large effect in favour of the intervention group.
It was not possible to calculate ESs for two outcomes (tactile acuity: moving 2-point discrimination test (MTPD) and touch threshold: Weinstein enhanced sensory test; however, the authors of the study report that the main effect of the group and time, as well as the interaction of group time in the MTPD in both dominant hand (DH) hand non-dominant (NDH), was not significant, and the WEST showed only interaction of group and time in NDH was significant (p = 0.02 and ES = 0.14).
Two motor outcomes were used in the PD study (Table 2). ES was quantified ranging from small (0.22) to medium (0.75) in favour of the intervention group.
Overall, there was very low-quality evidence from one study supporting the efficacy of SDT for somatosensory and motor function in people with PD compared to a control treatment in the immediate term. The quality of the evidence was downgraded due to very serious limitations in terms of risk of bias, inconsistency and imprecision (Tables 3 and 4).
Discussion
The aim of this systematic review was to investigate the efficacy of SDT on sensorimotor performance in individuals with a neurological condition affecting the central nervous system. Six RCTs were included in the final review including 220 participants incorporating two distinct conditions, stroke (five studies) and PD (one study). The general findings from this review suggest that SDT has the potential to be an efficacious treatment option for improving sensorimotor performance in individuals with neurological disease, specifically, the ability to discriminate bodily sensation in the upper and lower limbs in people who have had a stroke or who have a diagnosis of PD based on the majority of ESs falling in the medium range (0.5–0.8) (Cohen, 2013). However, for several reasons, these improvements must be interpreted with caution. These reasons include the broad range of ESs in both populations as well as the small sample sizes and high risk of bias of the individual studies. Thus, at present, there is limited evidence on which to base any firm clinical recommendations.
Four previous systematic reviews have investigated the efficacy of somatosensory discrimination training interventions for people following stroke (Chia et al., 2019; Schabrun and Hillier, 2009; Serrada et al., 2019; Turville et al., 2019). Although there was some evidence in favour of the experimental interventions as an efficacious treatment option, like the findings in this review, the evidence was limited by small sample size, inconsistency in clinical outcome measures and poor-quality studies. Furthermore, all four reviews stressed the need for high-quality RCTs, sufficiently powered with meaningful clinical outcome measures to accurately assess intervention effects. Specifically, Schabrun and Hillier (2009) and Serrada et al. (2019) both assessed intervention effects of six RCTs targeting the lower and upper limbs which included two studies (Lynch et al., 2007; Morioka and Yagi, 2003) also included in this review (two of the additional included studies were not in keeping with the definition of SDT used in this review because direct feedback on task performance was not given, one was not sufficiently randomised and the other study did not have a control). Turville et al. (2019) assessed the efficacy of somatosensory training interventions in the upper limb including both randomised and non-randomised controlled trials – only two RCTs were reviewed – one also included in this review (Carey et al., 2011) and a second in which the sensory intervention was not in keeping with the definition used in this study because direct feedback on task performance was not given. Chia et al. (2019) reviewed the efficacy of somatosensory retraining of the lower limb including all quantitative types of studies, two RCTs (Lynch et al., 2007; Morioka and Yagi, 2003) of which were also included in this review. This systematic review serves to fill a gap in the literature because it includes a more diverse population expanding from stroke to neurological conditions; its included studies are in keeping with the recommended gold standard (RCTs) and it has followed the Cochrane Collaboration methodology adopting use of the GRADE approach in an attempt to capture high-quality studies (Higgins et al., 2020a, 2020b). In addition, the findings are consistent with the four systematic reviews previously mentioned: SDT may have potential to be an efficacious treatment option for improving sensorimotor performance in individuals with neurological disease. However, at present, there is limited evidence on which to base any firm clinical recommendations due to the poor quality of the studies (despite being RCTs), and the heterogeneity seen within clinical outcome measures thus although this review has seen an advancement still further research studies are needed to obtain a more precise estimate of intervention effects.
Limitations
The studies included in this review were limited to individuals who have experienced stroke or have a diagnosis of PD and thus are under representative of the entire population group of neurological disease or injury affecting the central nervous system, so the findings should be applied with caution to the population as a whole. Only a small number of studies were included in the review and they were all adjudged to be of high risk of bias. Furthermore, the total number of participants included in this review (n = 220) was relatively small, well below the recommended 400 (Ryan and Hill, 2016) making it difficult to apply the findings with precision.
An additional limitation is that the intervention itself (SDT) is ill defined. Although SDT is clearly defined in this review, the lack of clarity in the literature in general could mean that some studies did not fit the definition required in this review but did in fact address somatosensory discrimination training.
In general, the outcome measures were heterogeneous across studies and measured different aspects of sensorimotor performance despite having similar interventions. For example, some focussed on measuring balance and limb function whilst others focussed on somatosensory skills, such as discrimination or proprioception hence making it difficult to draw comparisons. Furthermore, due to this heterogeneity a traditional meta-analysis was not possible, and although ESs were calculated, there is uncertainty that could only be addressed with an inferential meta-analysis. In addition, there is a high degree of inconsistency in the results seen in the large variations in the intervention ESs across studies deeming findings inconclusive. Specifically in the stroke studies, there is a wide variation in time since stroke among participants which could have impacted on recovery potential in the intervention groups and thus contributed to the inconsistency in intervention ESs.
Clinical implications and future research
There is a need for RCTs of sufficient quality and power to detect a precise SDT intervention effect in participants with neurological disease or injury affecting the central nervous system. It is particularly worth noting that no SDT RCTs meeting the inclusion criteria for this review were identified for conditions such as MS and focal dystonia, conditions where SDT has been identified as potentially beneficial (Jamali et al., 2017; Konczak and Abbruzzese, 2013). Thus, RCTs in these specific neurological clinical groups are particularly warranted. Furthermore, suitable quantitative outcome measures that capture sensorimotor performance in terms of somatosensory discrimination and motor function in this population group need to be further developed with a predefined minimal clinically important change so that size of effect can be accurately quantified and contextualised. Until then, SDT in people with neurological disease or injury affecting the central nervous system for the specific improvement of somatosensory and motor function should be treated with caution in an individual clinical setting.
Conclusion
Although within the previous literature there was some evidence in favour of SDT as an efficacious treatment option, the evidence was limited by small sample size, inconsistency in outcome measures and poor-quality studies, specifically a lack of RCTs. This systematic review has found similar findings that SDT may have potential to be effective for improving sensorimotor performance in individuals with neurological disease or injury affecting the central nervous system. However, currently there is insufficient evidence to make any firm clinical recommendations. Future, adequately powered, high-quality RCTs are needed in this population group to provide more robust evidence regarding this intervention.
Key findings
Sensory discrimination training may potentially be an efficacious treatment for improving sensorimotor performance in individuals with central neurological disease. Currently there is insufficient evidence to make any firm clinical recommendations and so future robust randomised controlled trials are needed in this population group.
What the study has added
There is a paucity of robust randomised controlled trials investigating sensory discrimination training as an intervention to improve sensorimotor performance in individuals with central neurological conditions. Whilst the limited available evidence appears positive, no firm recommendations can be made at this time.
Supplemental Material
sj-pdf-1-bjo-10.1177_03080226211018150 – Supplemental Material for The effect of sensory discrimination training on sensorimotor performance in individuals with central neurological conditions: A systematic review
Supplemental Material, sj-pdf-1-bjo-10.1177_03080226211018150 for The effect of sensory discrimination training on sensorimotor performance in individuals with central neurological conditions: A systematic review by Sarah C Taylor, Chris McKenna, Jillian Kent, Mary-Anne Jess, Jonathan R Robinson, John Dixon and Cormac Ryan in British Journal of Occupational Therapy
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Prof. C G Ryan is a named inventor on a sensory discrimination training device that could be used to train tactile acuity in people with a range of conditions including central neurological conditions. The remaining authors have no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.