
Abstract
Introduction
Visual field loss affects around 20% of stroke survivors, reducing quality of life. Eye movement training is a promising rehabilitation method, and several different interventions are used by occupational therapists. This study aimed to explore the feasibility and effects of four eye movement training interventions for stroke survivors with visual field loss.
Method
A mixed methods study – quantitative n-of-1 with qualitative interviews. The participants were 11 home-dwelling stroke survivors with visual field loss. The interventions used were MyHappyNeuron, NVT, Rainbow Readers and VISIOcoach, delivered in a randomised order. Visual search, reading speed, activities of daily living and quality of life were assessed three times before intervention use, then immediately after each intervention; these were analysed visually. A final semi-structured interview was then analysed using framework methods.
Results
Evidence of effect was divergent. Quantitatively there was no measured effect, but qualitatively participants reported benefits in visual skills, daily life skills and emotions, which varied by intervention. Median training time was 3–4 hours (range 0.5–6.5) for NVT, Rainbow Readers and MyHappyNeuron, and 9.5 hours (range 2.3–16.8) for VISIOcoach.
Conclusion
Eye movement training interventions were feasible for stroke survivors at home. Qualitative evidence suggests that variations in the eye movements trained and delivery modality underlie variations in perceived effect.
Introduction
Stroke causes lasting visual impairment in around one fifth of stroke survivors (Ali et al., 2013). Visual field loss, produced by damage to the visual pathway, typically causes loss of one half of the visual field on the same side in both eyes, effectively making the person blind to one side of space. Subsequent eye movement changes, involving smaller, repetitive movements, increase the time taken to view an entire scene (Zihl, 1995). The result is limited mobility and navigation (de Haan et al., 2015a), causing social isolation (Hazelton et al., 2019a). Reading and driving difficulties impact on leisure, occupations and return to work (Hepworth and Rowe, 2016), and psychological consequences include fear and lack of confidence (Hazelton et al., 2019a). Stroke survivors with visual field loss report limitations in activities of daily living (ADL) (Warren, 2009), poorer quality of life (QoL) (Chen et al., 2009), with restricted engagement in rehabilitation and poorer functional outcome (Ali et al., 2013). Occupational therapists have a key role in providing rehabilitation interventions for visual field loss in stroke survivors (Warren, 1993).
Identifying effective interventions for visual loss is a top ten research priority for stroke survivors, carers and clinicians (Pollock et al., 2012). Systematic review evidence suggests that training compensatory eye movements towards the side of visual field loss may improve QoL (Pollock et al., 2019). A range of approaches to training compensatory eye movements exist, including: (a) scanning training, which teaches broad horizontal eye (and head) movements to enable a full view of a scene; (b) search training, which stimulates a stroke survivor’s natural pattern of eye movements; and (c) reading training, which aims to improve the small left–right eye movements required to read across a line of text. Overall, eye movement training may lead to larger, less repetitive and more frequent eye movements (Passamonti et al., 2009; Schuett, 2009), improve visual search (Aimola et al., 2014) and mobility (Aimola et al., 2014; Hayes et al., 2012). However, high quality adequately powered studies providing evidence of benefits to stroke survivors’ activities and participation are needed (Pollock et al., 2011).
Eye movement training is utilised by occupational therapists and other professions (Rowe, 2013). Our earlier work identified therapist-supported specialist devices, paper-based tools, online training and computer programs in use to train eye movements (Hazelton et al., 2019b). These interventions vary in relation to the training aims, area of visual field covered, inclusion of head movements, cost and number, duration and frequency of training sessions (Hazelton et al., 2019b). We lack studies which directly compare these different eye movement training devices, despite their routine clinical use. Evidence on effectiveness and feasibility is required to inform clinical decisions and support optimal rehabilitation for stroke survivors with visual field loss.
The aim of this study was therefore to use mixed methods to explore and compare the feasibility of use and the effects of eye movement training interventions. We aimed to directly compare four eye movement interventions, selected for maximum variation, from those known to be used in clinical practice: MyHappyNeuron, NVT (NeuroVision Technology), Rainbow Readers, and VISIOcoach.
Methods
Our mixed methods approach combined a quantitative n-of-1 design with qualitative semi-structured interviews (Borglin, 2015). In an n-of-1 design each participant acts as their own control: quantitative outcome measures were conducted three times before the introduction of any interventions, spaced 2 weeks apart, in order to establish a baseline (Supplementary material 1). Participants were then provided with each of the four eye movement training interventions, delivered sequentially in a randomised order. After completing training with an intervention, the outcomes measures were repeated; these repeated quantitative measures were used to explore within-person effects associated with the use of each intervention. Qualitative interviews were conducted after all interventions had been used, to enable participants to compare their experiences with each. Baseline data were collected at a clinic-based assessment; all other study activities took place in participants’ own homes. Ethical approval was granted by the relevant ethical committees.
Recruitment
Participants were recruited from the waiting lists of two Scottish vision rehabilitation centres. Stroke-specialist low vision rehabilitation officers identified potential participants from their caseloads, by reviewing their notes in order to apply the inclusion criteria. The inclusion criteria were: clinical diagnosis of stroke at least 6 months earlier, hemianopic visual field loss, age 18 years or over, medically stable, living in the community and no prior community visual training. Visual field loss was assessed using confrontation, with any pattern of binocular field loss in the same vertical hemifield accepted. Exclusion criteria were: unable to provide informed consent, non-stroke visual impairment and involvement in another rehabilitation study. Low vision rehabilitation officers explained the study to eligible clients and provided large print/audio information and consent forms; participation was based on return of written consent forms.
Interventions
We tested MyHappyNeuron, NVT, Rainbow Readers and VISIOcoach. Table 1 provides a description of each intervention, derived in a previous study (Hazelton et al., 2019b) (for full TIDieR description see Supplementary material 2).
Intervention description.
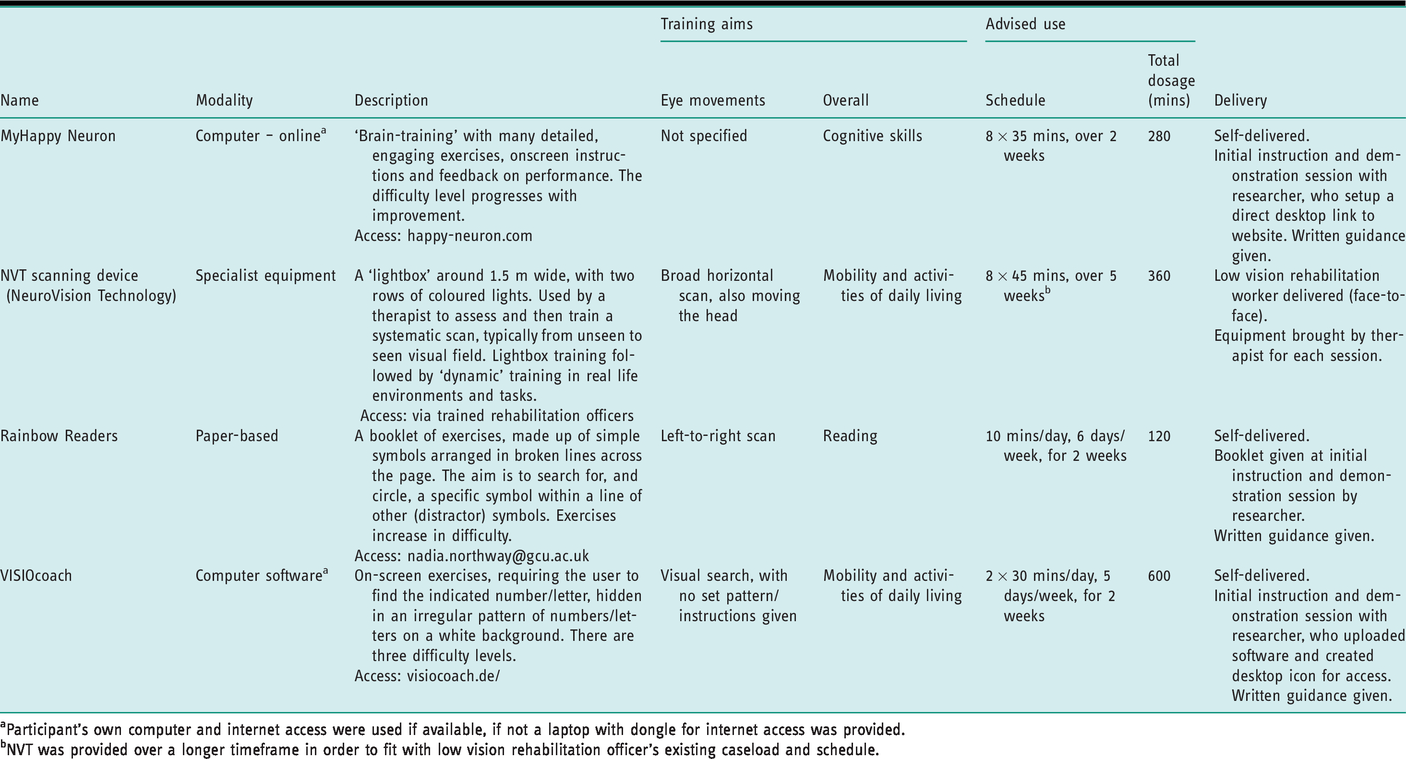
aParticipant’s own computer and internet access were used if available, if not a laptop with dongle for internet access was provided.
bNVT was provided over a longer timeframe in order to fit with low vision rehabilitation officer’s existing caseload and schedule.
Data collection
Baseline demographic data, including data on their stroke and vision were collected by an experienced optometrist (Supplementary material 1).
Quantitative measures collected at each of the seven timepoints were: visual search speed and accuracy – computer-based conjunction visual search (Treisman and Gelade, 1980); reading speed – International Reading Speed Texts (Trauzettel-Klosinski et al., 2012); self-reported abilities in ADL – Veteran’s Affairs Low Vision Visual Function Questionnaire (Stelmack et al., 2004); self-reported quality of life – Visual Core Measure 1 (Lamoreaux et al., 2008).
Participants used diaries to record adherence to the advised intervention regimen for each intervention. For NVT the diary was completed by the low vision rehabilitation officer delivering training.
Qualitative semi-structured interviews were conducted with each participant after using all four interventions, to explore and compare how well they could use each of the interventions, and any possible effects each had on them. A topic guide (Supplementary material 3) was used to ensure core questions were included and minimise interviewer biases; this was refined to explore unexpected responses and emergent themes (Rubin and Rubin, 2005).
Data analysis
Outcome measure data for each participant were plotted in line graphs, and analysed using visual inspection (Smith, 2012), with input from a methodological specialist (DD), and following a systematic process with clear guidelines to minimise bias and inconsistency (Kazdin, 2011). This involved assessment of the trend or stability of each phase and comparison of the intervention and baseline phases. A process of considered judgement (Kazdin, 2011) recorded the intervention effect as either possible effect (beneficial/detrimental), no effect or unclear. Diary data were analysed using descriptive statistics.
Transcribed interview audio files were analysed inductively with a five-stage thematic framework method (Ritchie and Spencer, 2002), using NVivo v10 software. This involved: (a) analysts developed a ‘feel’ for the data, by reading the transcripts; (b) line-by-line coding of the first four interviews to create a thematic framework of higher-order ‘categories’; (c) applying the framework to remaining transcripts; (d) creating charts, with intervention data displayed in rows and categories forming the columns; and (e) interpeting the data, looking for emergent connections, patterns or ‘themes’.
The first two analysis stages involved two authors (CH and BD), with one (CH) conducting the subsequent stages, with input throughout from a topic expert (AP) and methodological expert (AT). A framework of 52 codes in nine categories was developed, which covered intervention effect, intervention feasibility and opinions of the study (Supplementary material 4).
Results
Seventeen eligible stroke survivors were identified and 12 were enrolled, but one dropped out before intervention delivery due to changed family circumstances (Figure 1). Demographic data are given in Table 2. Service changes meant low vision rehabilitation officers did not deliver NVT to the final two participants. Quantitative outcome measure completion rate was 10/11 for ADL and QoL scales, with one participant not completing each due to fatigue, 7/11 for reading speed, due to language-based reading problems, and 9/11 for visual search, due to poor comprehension of the test.
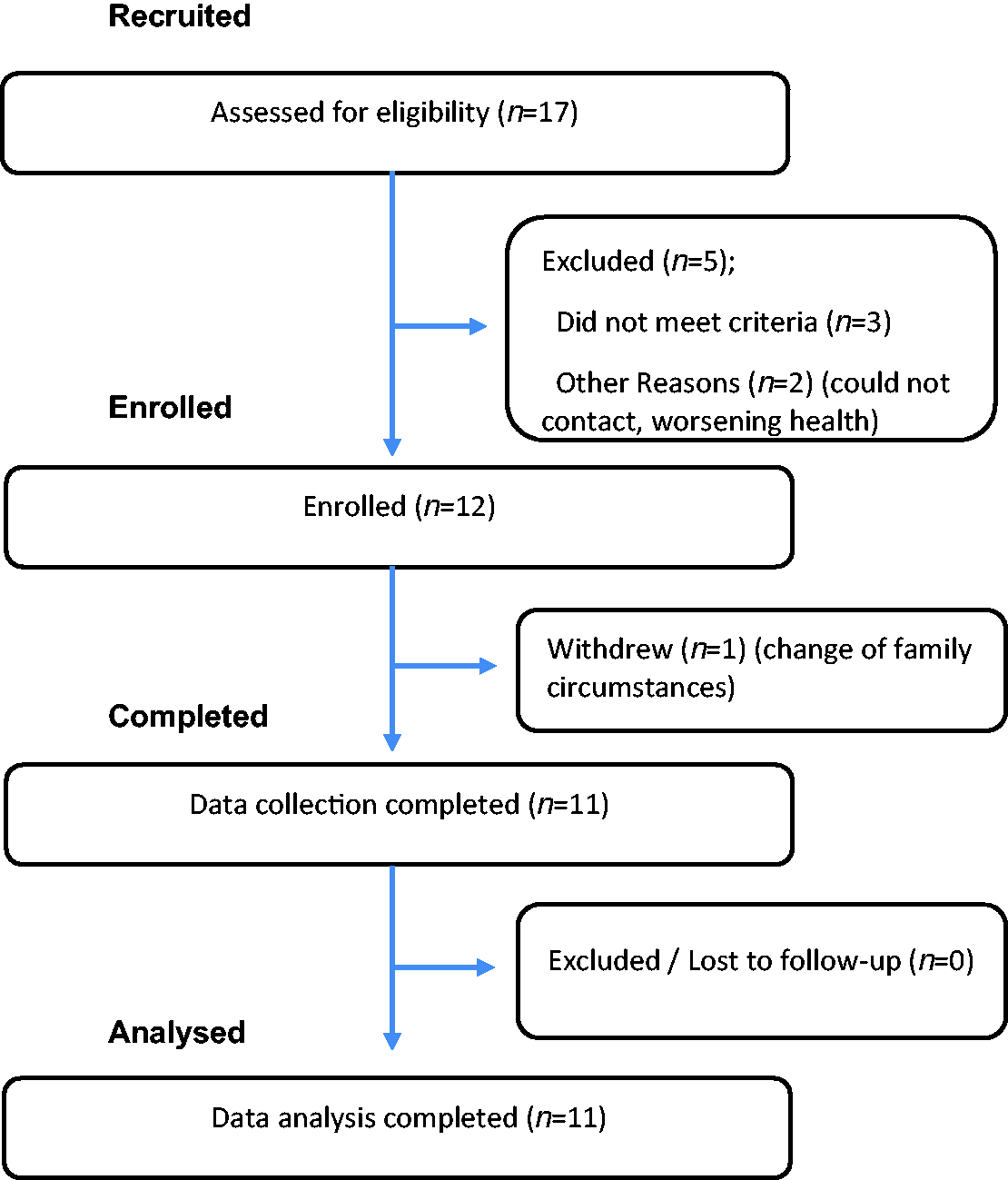
Participant involvement flowchart.
Baseline data for participants.
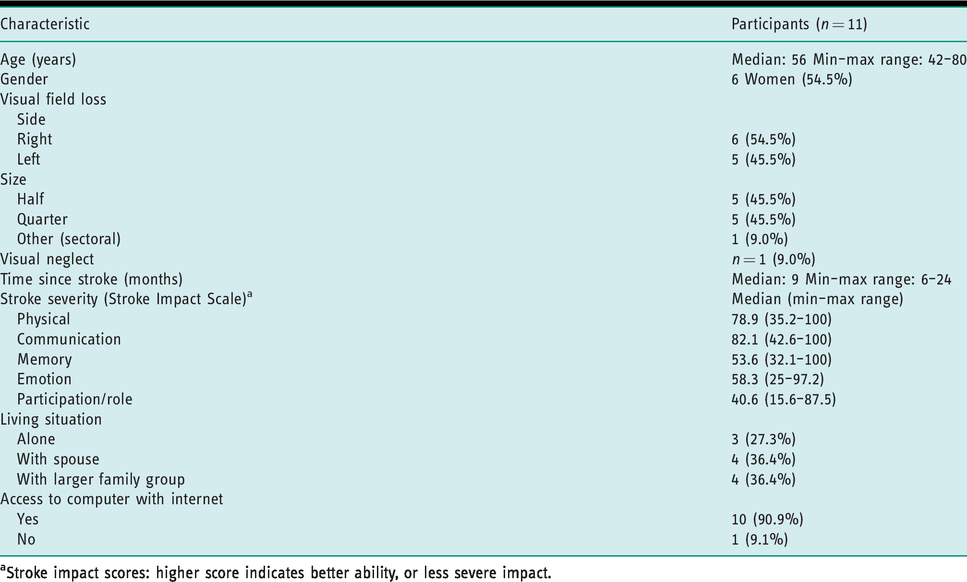
aStroke impact scores: higher score indicates better ability, or less severe impact.
The Results section presents the feasiblity data first followed by those on effects, to reflect the study aim, and quantitative data followed by qualitative data, to reflect the order of their use within the study.
Feasibility
Quantitative results
The training times recorded are given in Table 3.
Intervention feasibility: training time recorded.
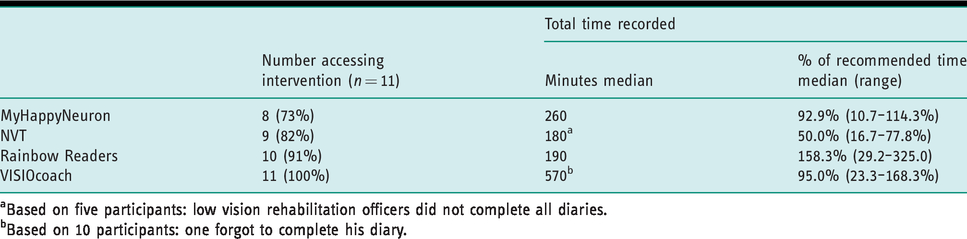
aBased on five participants: low vision rehabilitation officers did not complete all diaries.
bBased on 10 participants: one forgot to complete his diary.
Qualitative data
When asked about their ability to use interventions, participants typically identified the difficulties they experienced, relating to ease of use (the most important factor), ease of initial set-up and level of carer support required.
MyHappyNeuron: Most reported difficulties with set-up or use were related to MyHappyNeuron. A clear split was apparent between those who those who found MyHappyNeuron usable and enjoyable and found it too complicated. The latter group reported struggling to read and understand the instructions, remember the ‘sequences’ within exercises and comprehend their aim. This was exacerbated by the task speed and short time limits for exercises. we tried it and we tried it, and … it was too quick, if it gave you more time.… (Participant 10, right half-field loss)
NVT was set up and delivered by low vision rehabilitation officers, therefore as participants were less involved in accessing the intervention, they spoke relatively little about its feasibility. The ease of training varied from ‘very simple’ (participant 10) to ‘really difficult at times’ (participant 5). For some, the ‘dynamic’ part of training, involving practising scanning in daily life tasks was limited by stroke-related lower-limb, pain or balance problems. Dynamic exercises were then tailored by low vision rehabilitation officers to the participant’s specific limitations.
Rainbow Readers was seen as the easiest intervention to set up, as the process of opening the book and selecting the page to start on was quick and straightforward: That’s not too taxing, not any set-up (Participant 5, right half-field loss) I’d like to do that for myself. But the thing is, the problem being is I don’t know if I’m going wrong […] because if I was doing anything wrong I liked somebody to say ‘That’s alright’ (Participant 1, left quadrant loss) I just switched the computer on and it was there … there wasn’t lots of sequences to go through (Participant 1, left quadrant loss) I would sit at the kitchen table and do it … and it would only be if I got stuck that I would say [to his wife to help him] (Participant 6, left half-field loss)
Effects
Quantitative results
The effect of the four interventions across the group is summarised in Table 4. Visual plots were created for each outcome measured for each participant; an example using data from the visual search test is given in Supplementary material 5. The was no evidence of effect arising from the use of MyHappyNeuron or VISIOcoach, with very limited evidence that NVT had a potentially beneficial effect on ADL and QoL and Rainbow Redears potentially improving reading speed.
Summary of outcome measure results for each intervention.
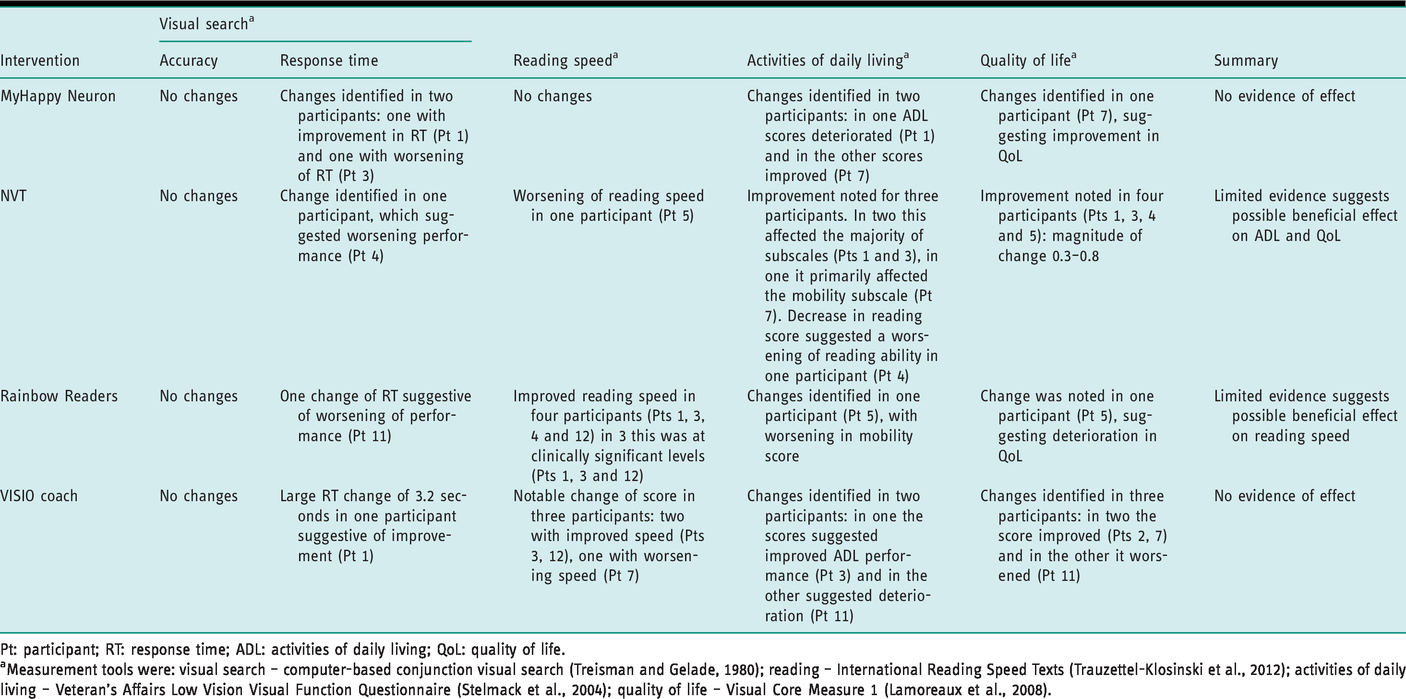
Pt: participant; RT: response time; ADL: activities of daily living; QoL: quality of life.
aMeasurement tools were: visual search – computer-based conjunction visual search (Treisman and Gelade, 1980); reading – International Reading Speed Texts (Trauzettel-Klosinski et al., 2012); activities of daily living – Veteran’s Affairs Low Vision Visual Function Questionnaire (Stelmack et al., 2004); quality of life – Visual Core Measure 1 (Lamoreaux et al., 2008).
Qualitative results
Participants described that using each of the four interventions had different effects: Well there was a different outcome from … (each) obviously (Participant 7, right quadrant loss)
MyHappyNeuron was reported to have little effect on visual skills. Instead, participants felt it provided mental stimulation and improved general knowledge, memory, problem-solving and overall mental agility.
Improved confidence was a key emotional effect of using all four interventions, including MyHappyNeuron. This was both general self-confidence or confidence related to specific tasks. It was founded on successful exercise completion. (MyHappyNeuron) was building up my confidence ‘I can do this, I can do this!’ (Participant 5, right half-field loss) Yes I think I … [laughs] how stupid am I? I do think it’s made me aware of what I can’t do, not what I can do and that’s sadly so (Participant 3, left quadrant loss) Definitely NVT (was most effective) because I hadn’t realised until then that if I turned my head to the left […] but I hadn’t realised that … It hadn’t clicked, hadn’t clicked. (Participant 1, left quadrant loss) it helped me with going outside and not walking into things (Participant 9, right half-field loss) It helped to make me more confident…. It let me get out and see what I could do, what I could see […] and I realised I can do this myself without anybody (Participant 10, right half-field loss) Rainbow Readers kind of teaches you to read properly along the lines (Participant 1, left quadrant loss) I found it good in as much as it wasn’t just teaching you to scan from left to right, it was teaching you to scan the whole page (Participant 5, right half-field loss) Something just clicked in my brain that, you know, do it that way and it’s better…. I think it probably did make me quicker as well by doing it up and down. (Participant 12, left quadrant loss)
Participants were asked if there was a preferred intervention, or combination: they clearly appreciated the use of a range of tools. It was felt the affects of each was different, but ‘complementary’ (participant 12). Learning different patterns of eye (and head) movements meant participants felt they had a range of methods they could potentially use to approach a visual task: It just expanded your visual possibilities … it was giving you the flexibility to do it different ways, which again I found good (Participant 5, left half-field loss)
Discussion
This study explored the feasibility and effect of eye movement training interventions for 11 home-based stroke survivors with visual field loss. The effect of each intervention on four outcome measures was explored in a series of experimental n-of-1 studies, with diaries used to gather usage data, and qualitative interviews conducted.
Feasibility
This study has demonstrated that eye movement training was generally feasible for home-dwelling stroke survivors with visual field loss. The median training time was 3–4 hours for NVT, Rainbow Readers and MyHappyNeuron, and around 9.5 hours for VISIOcoach. For the self-delivered interventions, participants typically achieved at least 93% of the recommended training time. For NVT, the low vision rehabilitation officers reported tailoring the training time to individual’s needs and abilities, resulting in an average training time of 50% of that expected. Few studies have explored this aspect of eye movement training: Aimola et al. (2014) found that only three (of 28) participants achieved the training goal of 35 hours of therapy over 5 weeks, (equivalent to around 1 hour training per day), in an unsupervised computer-based training. However, in our study 11 participants using computer-based VISIOcoach (which also recommended 1 hour training per day) achieved 95% of this training time, suggesting acceptable adherence to the intervention.
The qualitative data from this study help explain some of the variation seen in the quantitative results. Stroke-related impairments, primarily in cognition but also language, motor or visual skill, appeared to contribute to barriers to access, limiting training time or necessitating carer support. Low vision rehabilitation officers delivering NVT reported modifying training sessions according to participants’ ability, to ensure it was accessible. The level of intervention challenge relative to participant ability, and the ability either to reduce intervention difficulty or provide stroke survivors with support, appears critical to the feasibility of intervention access.
Effect
Evidence from the quantitative and qualitative methods was essentially divergent, with no, or very limited, measured effect of eye movement training on visual search, reading, ADL and QoL, but participants reported a range of perceived beneficial effects from all four interventions. The reported effects were on visual and cognitive skills, functional abilities, including using the internet, walking and using public transport, and emotions. Increased confidence was a key effect, particularly in response to NVT training. Thus, the lack of quantitative evidence of effect cannot be interpreted as evidence of no effect, as this is contradicted by the qualitative data.
Previous quantitative research suggests VISIOcoach increases visual search results (Roth et al., 2009), and NVT can improve visual search, peripheral vision and mobility (Hayes et al., 2012). Possible explanations for the difference between our results and previous research may relate to this study design: there was a relatively short training period of 2 weeks, so the full training effect may not have been established and therefore was not captured by quantitative outcomes. A key issue is that our qualitative results may have overstated training impact; with participants aware they are receiving ‘additional’ intervention they may have sought to report positive experiences (Patton, 2002). This is a central factor in contradictory qualitative and quantitative results (Campbell et al., 2003). However, the value of mixed methods research lies partly in the fact that the two methodologies explore different aspects of the same phenomenon (De Lisle, 2011). For participants, one of the key effects was emotional, improving their sense of confidence, motivation and hope, which have not been considered in detail in prior work. No quantitative outcome measure that directly addressed emotional changes was included; the interviews allowed the participants to report their experience more freely, enabling identification of this broader range of potential effects.
Our qualitative data helped explore and explain several variations noted between interventions. One important factor for participants was the use of head movements in combination with eye movements. This combination was taught by NVT, with Rainbow Readers and VISIOcoach minimising use of the head and aiming to improve eye movements only. The use of scanning head movements has been criticised as slower and potentially detrimental to functional ability (Kerkhoff et al., 1992); however, our findings contradict this. Participants clearly felt their use was beneficial, and for some was key in achieving improvements in ADL (such as walking outside and navigating safely). A clear variation was also identified in the task and activity improvements participants reported. These suggested that improvement in functional abilities reflected the intervention modality, with limited transfer to non-trained tasks reported; paper-based Rainbow Readers was perceived to improve reading, and computerised VISIOcoach training was perceived to improve computing and reading skills, with no reported impact on wider mobility or ADL skills, even though it aimed to do so (Table 1 and Supplementary material 6). Within the literature there are two opposing theories relating to transfer: (a) that eye movements learnt in one task will carry over into other activities, as the new eye movement patterns will be internalised and applied automatically in new tasks (Pambakian et al., 2004); and (b) that scanning training is non-transferrable, and therapy must include training of eye movements during the activities of interest, such as mobility and ADL (Hayes et al., 2012; Pommerenke et al., 1989).These findings give some support to the latter theory, with only NVT, which included task-specific training, showing improvements in these skills within the timeframe of this study.
Data from this study suggest that participants favoured using a combination of interventions. Participants felt the effects and visual skills acquired differed between interventions (Supplementary material 6) and were complementary, giving greater versatility in the skills available to use. Studies of stroke survivors with visual field loss have suggested that different eye movements are used for different tasks (Hardiess et al., 2010), so training that encourages a broad visual scanning movement is unhelpful in tasks that require visual search (de Haan et al., 2015b). In addition, reading-specific training which encourages small left-to-right horizontal eye movements does not improve visual search and vice versa (Schuett et al., 2012). Our results therefore support the need for training across several strategies (using a range of tools) to give participants the flexibility of visual skills required to tackle the broad variety of activities seen in daily life, and the different visual demands they present to a stroke survivor with field loss.
Strengths and weaknesses
A key strength of this study was that our n-of-1 method allowed the inclusion of four interventions, which represented key differences (modality, mechanisms, area of visual field covered and training schedule) in current clinical practice and enabled the identification of variations in their feasibility and hours of training completed. Our qualitative data (rarely considered in this field) has allowed stroke survivor experiences and perceptions of each intervention to be explored, providing valuable insight into the reasons for variation in feasibility and range of effects of each training method. Our comprehensive semi-structured interviews and rigorous analysis increased the insights provided by the participants’ accounts. Combining and comparing the quantitative and qualitative results has allowed further interpretation of study findings, especially in relation to the conflicting data of the intervention effect.
A number of limitations of this study must be noted. The degree to which our findings are applicable to the wider population is uncertain given our small sample size, use of convenience sampling strategy and recruitment from the vision-specific centres, which may only see the more severe cases. The number of participants using each intervention was also not equal, which may limit the ability to draw consistent conclusions. The use of the n-of-1 study design means that placebo effects cannot be accounted for, and factors other than the interventions may have created the effects reported. For practicality, training duration for each intervention lasted around 2 weeks; although eye movement training has been shown to have an effect after just one session (Jacquin-Courtois et al., 2013), this short duration may have reduced training effect. Training dosage was recorded by participants and therapists – in some cases diaries were not fully completed and the method is open to errors of recording or recall so data may not be accurate. Some participants had memory difficulties (Table 1), which may have affected their ability to recount their experiences, a difficulty inherent in interviewing individuals post-stroke. As noted previously, the qualitative aspect is open to bias on the part of the interviewer, analyst and participant, and this may have acted to over-state the perceived effect of the interventions.
Implications for occupational therapy
Several eye movement training interventions were feasible, and could be provided to home-dwelling stroke survivors with visual field loss. Individuals’ abilities (especially cognition and language) may impact on the accessibility, so occupational therapists should consider these and the ability to tailor the level of challenge an intervention presents when developing a care plan. Our study suggests that interventions may have different, but complementary effects, and that these appear modality specific. Consequently, clinicians should consider providing a range of interventions, using diverse modalities (paper based, computer based and specialist equipment) to maximise the functional impact for stroke survivors. Furthermore, the choice of intervention should be related to an individual’s occupational performance needs and goals. Our qualitative evidence suggests that for a reading goal, Rainbow Readers would be the first choice of intervention, for a goal of returning to computer use VISIOcoach or MyHappyNeuron may be appropriate, with NVT most relevant for someone with navigation and community access goals. Given the value placed on learning new head movements alongside eye movements, clinicians should aim to teach both aspects to improve compensatory abilities.
Our study suggests further investigation of the effectiveness of NVT, Rainbow Readers and VISIOcoach eye movement training interventions (potentially in combination) may be warranted. Given the disagreement surrounding the eye movements required to compensate for visual field loss, the rationale for targeting specific eye/head movements should be stated alongside exploration of how variations in eye movement may impact on functional ability. Researchers should also consider the use of qualitative methods and their choice of quantitative outcome measures used to capture the effectiveness of treatment. Stroke survivors stated that tasks and activities plus the emotional effects of training were most important to them; however, our results suggest that current vision-based ADL and QoL scales may be insensitive to change and may inadequately capture the emotional impact of eye movement training.
Conclusion
Eye movement training interventions were essentially feasible for home-based rehabilitation. Feasibility was limited in tools which used fast, complex exercises, as they posed too high a linguistic or cognitive challenge. Quantitative data gave no clear evidence of intervention effect from, but there were perceived effects on visual skills, cognitive skills, emotions and functional abilities, which varied by intervention. Variations were linked to intervention modality, with a lack transfer to untrained tasks suggested, and to the training of head movements in combination with eye movements, which was perceived as beneficial.
Key findings
Eye movement training is feasible for home-dwelling stroke survivors, and may improve ADL. Effects may vary by intervention and modality: using several interventions may maximise effects.
What the study has added
This study suggests eye movement training is feasible, with a range of perceived benefits. By exploring the factors affecting intervention success, it enables occupational therapists to choose interventions relevant to individuals’ rehabilitation needs.
Supplemental Material
sj-pdf-1-bjo-10.1177_0308022620936052 - Supplemental material for The feasibility and effects of eye movement training for visual field loss after stroke: a mixed methods study
Supplemental material, sj-pdf-1-bjo-10.1177_0308022620936052 for The feasibility and effects of eye movement training for visual field loss after stroke: a mixed methods study by Christine Hazelton, Alex Pollock, Diane Dixon, Anne Taylor, Bridget Davis, Glyn Walsh and Marian C Brady in British Journal of Occupational Therapy
Footnotes
Acknowledgements
The author(s) would like to thank the designers of all included scanning training tools for providing free access during this study. They wish to note that MyHappyNeuron is designed for a general population, and a version specifically for healthcare use (HappyNeuron Pro) is also available. We would also like to thank the low vision centres and rehabilitation officers invovled in this study.
Research ethics
Ethical approval was obtained from the NHS West of Scotland Research Ethics Service (reference 13/WS/0171).
Declaration of conflicting interests
The author(s) confirm that there are no conflicts of interest.
Funding
This study was funded by the Stroke Association (UK) by way of a Junior Research and Training Fellowship held by the lead author (TSA JRTF 2011/02). MCB, AP and the NMAHP Research Unit are funded by the Scottish Government Health and Social Care Directorates. The views expressed here are those of the authors and not necessarily those of the funders.
Consent
All participants provided written informed consent to participate in the study.
Contributorship
All authors contributed to the design of the project and data analysis plan. Data was collected by CH, quantitative analysis was conducted by CH, AP, DD and qualitative analysis by CH, BD, AT, and AP with further interpretation involving GW and MB. CH wrote the first draft of the article, all authors commented on and/or amended this and all authors read and approved the final manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.