
Abstract
This paper describes the qualitative findings of a systematic literature review of research on patients on conditional discharge from forensic mental health services in England and Wales (part two of two). In total, 15 qualitative and five mixed-methods studies were included. A thematic synthesis of the findings produced familiar themes addressed in the wider desistance literature: tensions between agency and social structures; the importance of bonds to (in)formal social institutions and meaningful relationships; and the assessment of criminogenic risk factors such as substance use, antisocial peers and inadequate accommodation. We draw on the concepts of identity-desistance and relational-desistance and suggest that our findings encourage modifications or adaptations to desistance theories to better explain the experiences of forensic mental health patients (e.g., epistemic injustice, mental health stigma, shared decision-making). We discuss how insights from desistance theories can be used to support recovery in forensic mental health patients in practice.
Introduction
Forensic mental health services provide care and treatment to people who are living with a serious mental disorder, have been involved in offending or harmful behaviour and are deemed at risk of harm to themselves or others. In England and Wales, conditional discharge is a commonly used discharge option that enables patients to receive support in the community, but where they can be recalled to hospital by the Secretary of State under the Mental Health Act 1983 if the mental disorder is of a nature that warrants detention in hospital and this is necessary for the protection of other persons. On December 31st 2023, there were 3,185 conditionally discharged restricted forensic mental health patients (Ministry of Justice, 2024).
Research that seeks to explain outcomes for forensic patients after discharge is predominantly positivist. Studies use quantitative indicators to identify risk and, less frequently, protective factors associated with reoffending or recall to hospital (e.g., Baudin et al., 2020; Doyle et al., 2021). This work draws on the Risk-Need-Responsivity paradigm and findings are meta-analysed (e.g., Bonta et al., 2014). Explanatory frameworks and theoretical perspectives unpacking these findings are rarer. The frameworks that do exist offer helpful insights as to why and how forensic patients discharged from care live fulfilling, offending-free lifestyles alongside or after mental illness. The ‘Good Lives Model’ suggests that there are 11 life domains that, where fulfilled or pursued legitimately, are associated with positive wellbeing and reductions in offending (e.g., knowledge, play, agency, relatedness; see Ward & Brown, 2004). ‘Secure recovery’ explores ways conceptualisations of recovery in mental health (e.g., the CHIME framework; Leamy et al., 2011) can be localised to secure criminal justice settings.
However, research into outcomes for forensic patients in the community would benefit from greater engagement with the desistance literature in non-forensic populations. Desistance research asks why and how people who have committed offences maintain offending-free lifestyles (Weaver, 2019). Though most theories of desistance do not explicitly address mental health, the endogenous variable in these theories is oftentimes a rich and meaningful life that lacks offending, rather than pauses in offending per se. Desistance theories emphasise the causal roles of socio-structural factors, maturation, social bonds, individual agency and narrative/identity factors in desistance (see Weaver (2019 for an overview). Thus, they offer potential insights into the causal relationships that are inferred in positivist models of risk/protective factors in the forensic mental health population (see part one of this review for summaries of hypothesised causal relationships).
Certain micro-level desistance theories argue that people who offend will have made a considered decision that the benefits of an offending lifestyle outweigh the costs. Paternoster and Bushway (2009) argue that people who offend have working selves – that is, preferences and social networks – consistent with an offending lifestyle, possible future selves and feared future selves. Desistance can occur when people who have offended no longer consider the benefits of the criminal working self to outweigh the costs of maintaining this lifestyle, or where a series of life failures indicate to the individual that they may become a feared future self should they continue offending. In the latter case, someone who desists will adopt an offending-free possible future self.
Meso-level theories emphasise the role of prosocial networks (Sutherland, 1947), and informal social institutions such as marriage, employment and community networks. These bonds are thought to give an individual something to protect and fear losing (Hirschi, 1969). Identity is implicated here too as the social roles of, for example, father, employee, husband, etc. carry normative expectations and duties that are often incompatible with an offending identity. Individuals desist from offending to maintain these attachments and the positive regard others hold them in.
A third category of perspectives highlights the interplay between broad socio-structural factors (e.g., relative deprivation, unemployment, racism, and poor education and health opportunities) and individual agency (i.e., to what extent individuals choose to maintain or desist from an offending lifestyle; Dufour et al., 2015; Farrall et al., 2010). Giordano et al. (2002) suggest that an individual’s concerted efforts to desist (agency) are shaped by the accumulation of structural factors that increase the likelihood that they will offend. Opportunities to offend and benefits linked with offending decrease as individuals’ social capital and social position increase. Desistance is contextual and contingent, more or less likely based on one’s social position.
These theories can offer helpful insights into how and why people desist. However, they typically focus on individuals for whom mental illness is not a major factor in their recovery and reintegration. The desistance literature has much to offer research with forensic mental health patients on conditional discharge. In what follows we present the findings of a qualitative systematic literature review on the experiences of this population, their carers and staff, and situate our findings within the desistance scholarship. Specifically, we draw on the concepts of identity- and relational-desistance in our discussion. We suggest that our review findings encourage modifications or adaptations to desistance frameworks to better accommodate the experiences of individuals in the criminal justice system with mental health needs (e.g., forensic patients on conditional discharge).
Aims
This review aimed to synthesise and summarise in a narrative form the extant literature on the conditionally discharged forensic mental health patient population in England and Wales. The purpose of this paper was to report the qualitative findings of the review; the quantitative findings are reported in a separate publication (part one; Kilbane et al., 2025). The research question addressed in this paper is: How do patients, staff and carers/family experience and describe the conditional discharge process?
Methodology
Publications were synthesised and summarised according to the narrative synthesis approach (Centre for Reviews and Dissemination, 2009). The PROSPERO registration code is: CRD42022343632. This paper follows the PRISMA reporting guidelines (Page et al., 2021). The findings of 23 additional studies reporting quantitative findings included in our review are reported in part one (Kilbane et al., 2025).
Search Strategy
The following databases were included in the review: PubMed; Web of Science; PsycINFO; MEDLINE; Cochrane Library; Google scholar (first 10 pages); Google search (first 10 pages); the references of included articles were scanned to identify further studies; researchers in the field were contacted for additional papers. The Boolean search strategy included: ((psych* or mental*) AND (forensic* or secur* or ‘special hospital*’) AND (conditional* or discharge* or release* or supervi*) AND (England or Wales or English or Welsh or UK or U.K. or ‘United Kingdom’)). All publications were published in English. The time limit for inclusion encompassed all publications published from 1983 to the date of the search to include studies conducted after the introduction of the Mental Health Act 1983. Databases were initially searched between 29/07/2022 and 11/08/2022. Updated searches were conducted on 14/09/2023 and 11/03/2025 to identify studies published during the review period (see Figures 1 and 2).
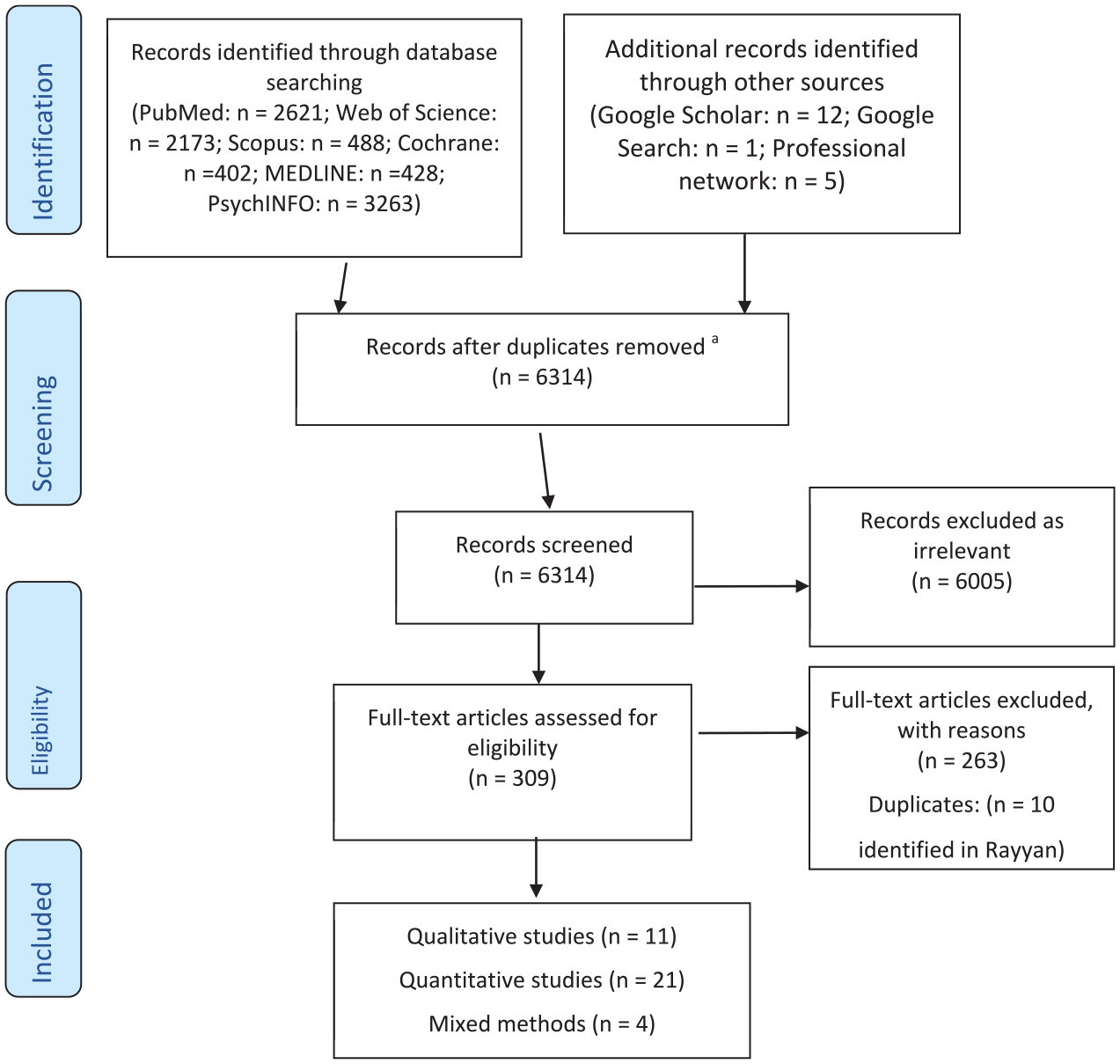
Study flow diagram using the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) template First Search.
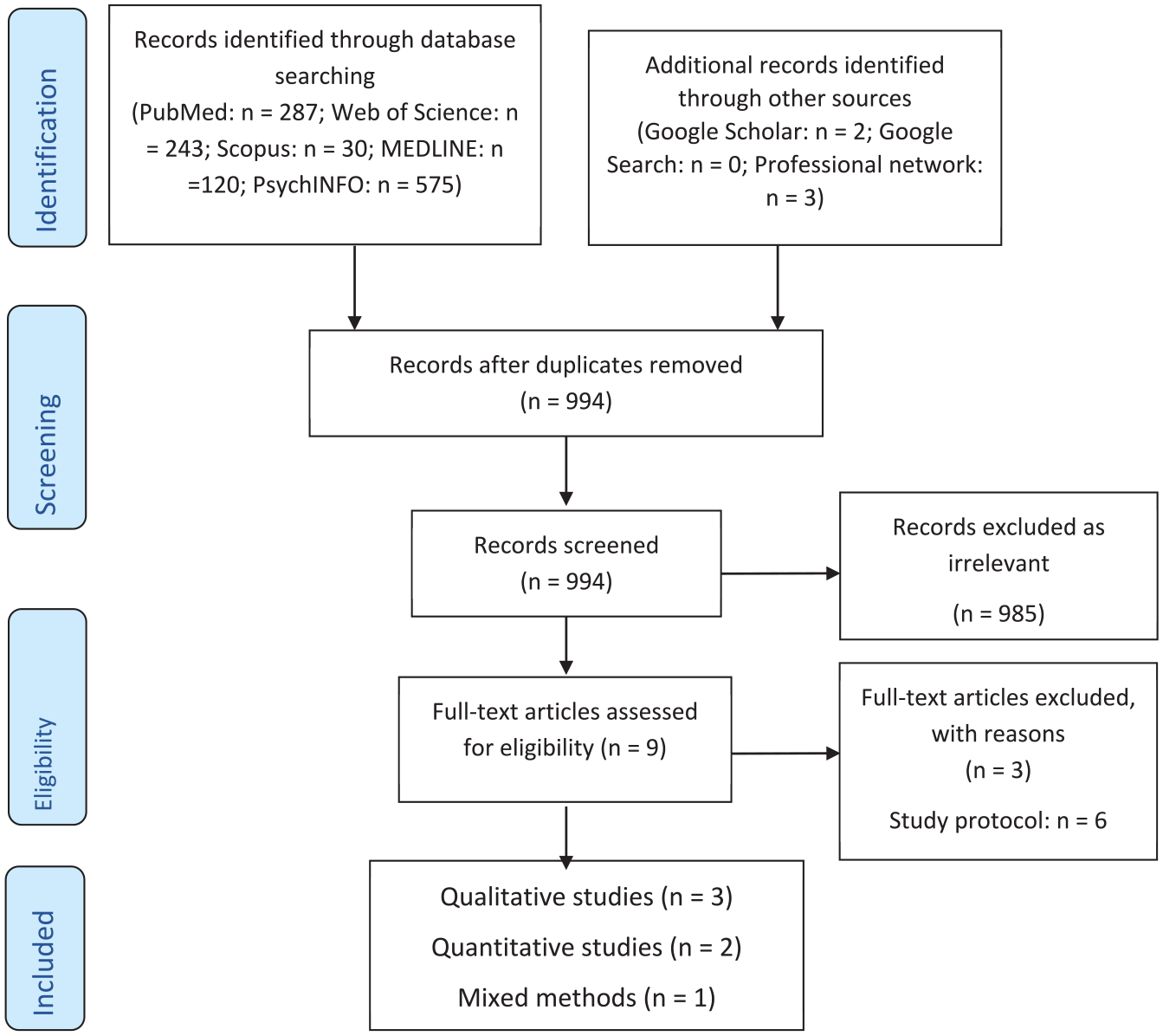
Study flow diagram using the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) template Updated Search.
The inclusion criteria included: Studies with empirical data (qualitative or quantitative; any study design); studies of, or including, patients who are on or who have previously been on, or are about to be conditionally discharged from secure psychiatric care (where patients were previously on conditional discharge but not at the time of the study, data must pertain to the conditional discharge experience (e.g., studies of recalled patients)); studies in England and/or Wales. Studies of staff, family and carer views and experiences of conditional discharge were also included.
Screening and Data Extraction
Studies were screened for relevance by two research assistants (MZ and AR). Those identified as being potentially eligible were judged against the inclusion criteria. Study data were then extracted and recorded in a summary table (available as a Supplemental Material). These data included: authors, year of publication, aim/purpose, population and sample size, study design, follow-up and key study findings.
The research assistants extracted data from 50% of publications each and then checked the accuracy of the other’s work. JT, SK, MJ and ST reviewed 25% of the papers each for inter-rater reliability. JT and SK then reviewed data extraction for a final time. Findings were subject to discussion, with any discrepancies resolved through team dialogue. SK and JT conducted data extraction for all papers in the updated search.
Data Analysis and Synthesis
Thematic analysis was conducted using NVivo software version 1.7.2. Qualitative data – both first-order, for example patient or staff quotes, and second-order, for example author interpretations – were coded line-by-line to facilitate a synthesis of the data and derive third-order themes. This coding followed the thematic analysis approach articulated by Thomas and Harden (2008). JT and SK coded 50% of the qualitative papers each and generated initial descriptive codes before meeting to discuss and agree analytic codes. Findings are presented thematically.
Quality Assessment
Studies were assessed for their quality and risk of bias using quality assessment tools from the Joanna Briggs Institute family of critical appraisal tools. Quality assessment was conducted by two research assistants under the supervision of JT, SK, MJ and ST. Doublechecking of work and inter-rater reliability checks were carried out as for data extraction.
Results
Overview
N = 6,314 publications were identified after our initial search, with N = 994 additional publications in our updated searches. After deduplication, screening and full text search in accordance with our inclusion and exclusion criteria, N = 15 qualitative and five mixed methods publications were included in the qualitative review (with 23 quantitative papers reported in part one). All papers are summarised in a table included as Supplemental Material. The quality of the studies ranged from low to high; results from the JBI critical appraisal tools are summarised in Table 1.
Quality Assessment of Papers Using JBI Critical Appraisal Tools.
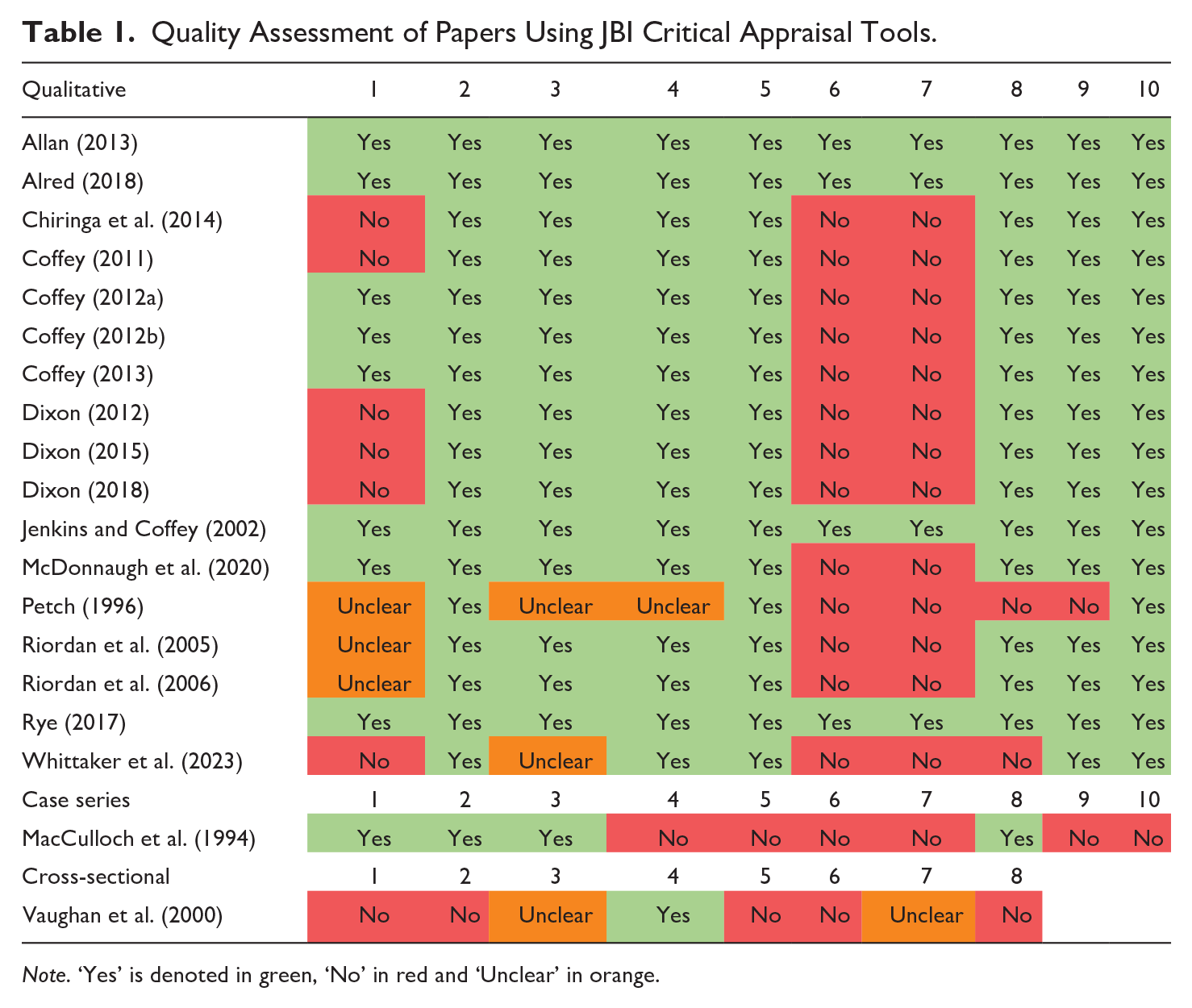
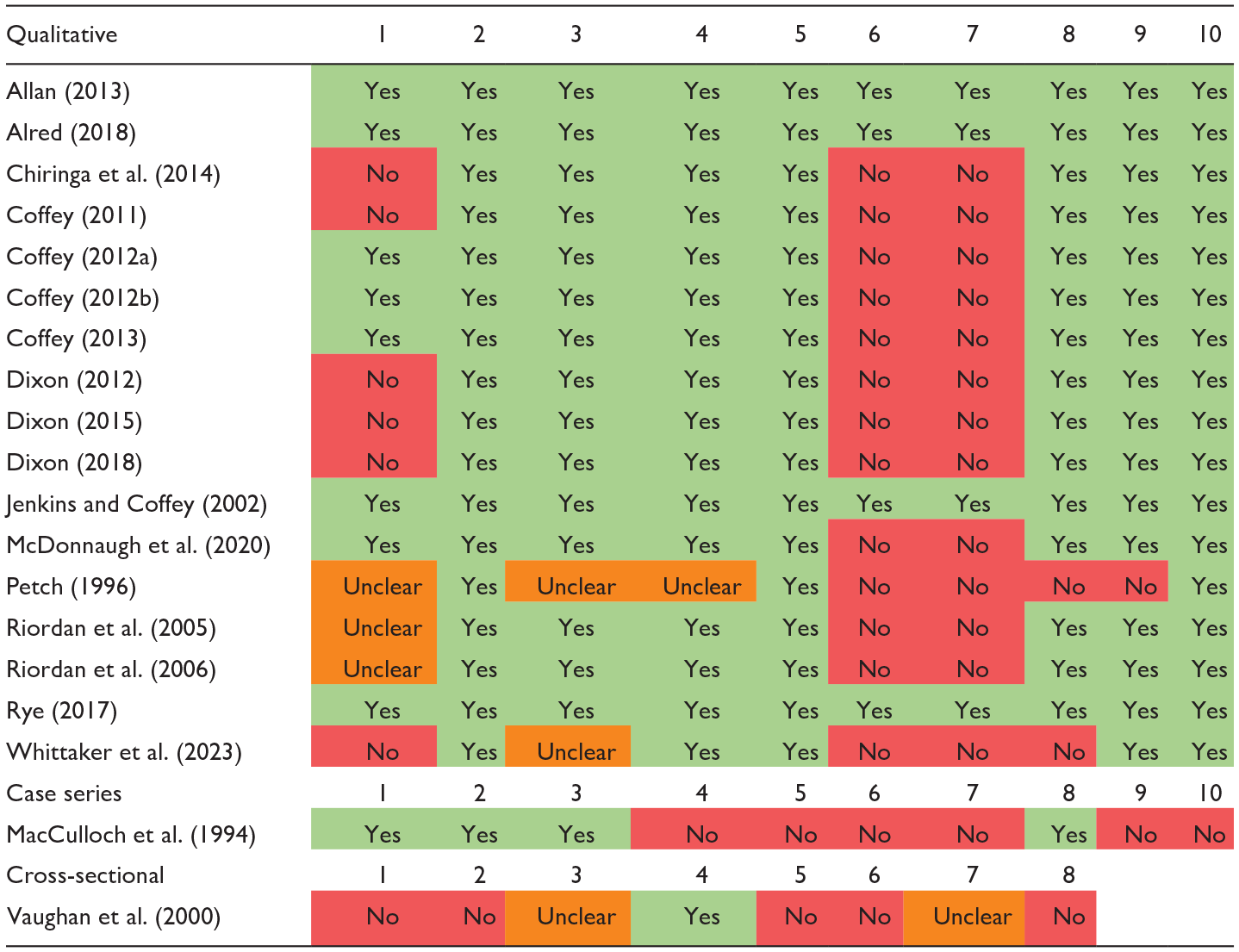
Note. ‘Yes’ is denoted in green, ‘No’ in red and ‘Unclear’ in orange.
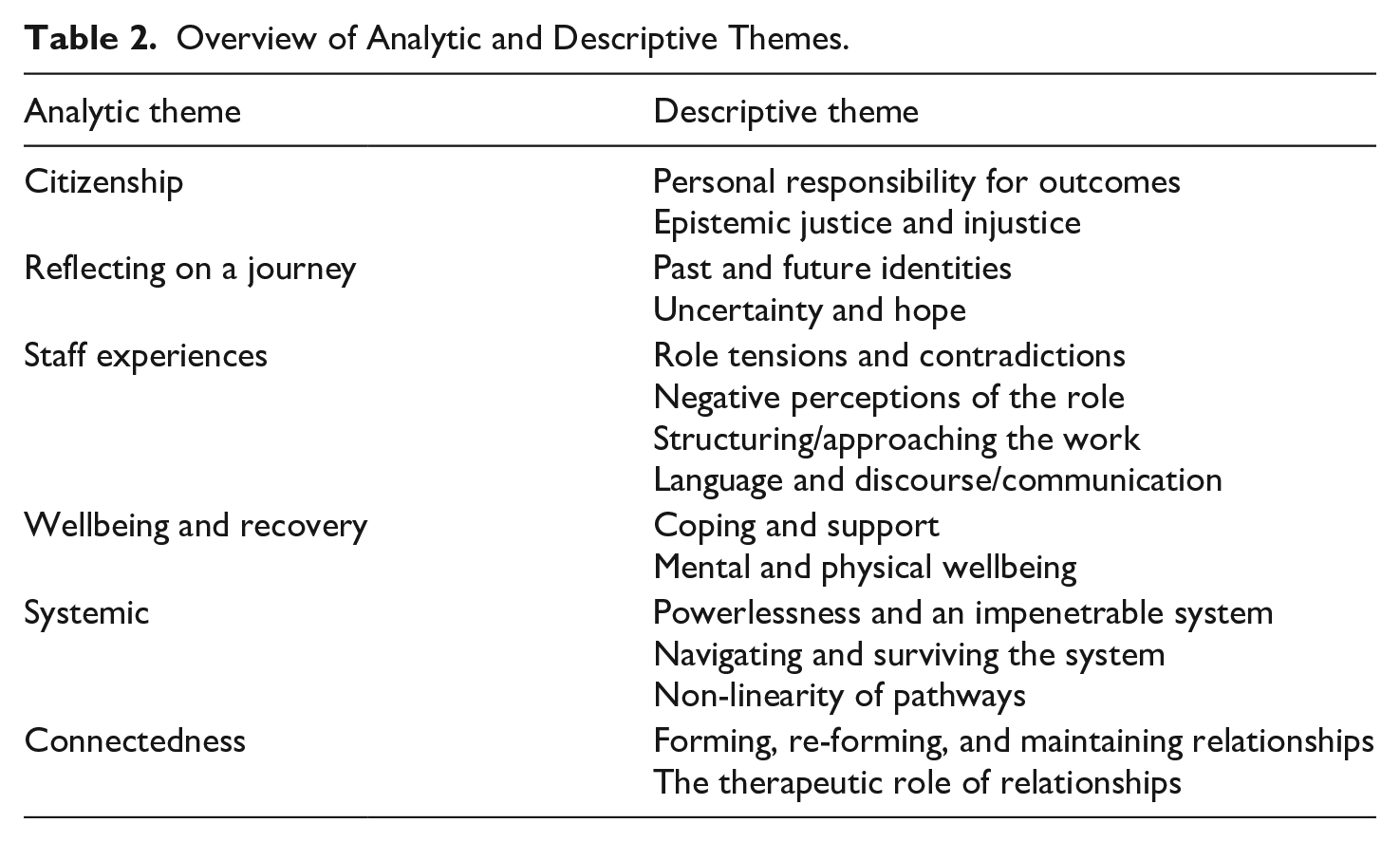
Six hundred and twenty-one codes were created across all coders prior to developing descriptive and analytic themes (a full list of codes is available from the authors on request). After thematic analysis and discussion across the team, six analytic themes and 15 descriptive themes were developed. The large number of descriptive themes is illustrative of the wide range of research areas in the included studies. Of the analytic themes, ‘Citizenship’ signifies discharged patients’ desire for greater involvement and decision-making power in their care, contrasting with feelings of voicelessness they and their parents described. ‘Reflecting on a journey’ explores how patients handled changing identities, such as moving from ‘mentally ill’ to ‘community member’. ‘Staff experiences’ covers role conflicts, training needs and professional impacts. ‘Wellbeing and recovery’ describes patients’ health needs and support sources, including how housing and substance use contribute to recall. The ‘Systemic’ theme describes patient, carer and staff challenges in dealing with services and recovery’s non-linear nature. ‘Connectedness’ highlights the importance study participants attached to relationships, which can be either supportive or detrimental to recovery and desistance. These themes are summarised in Table 2 and presented in turn.
Overview of Analytic and Descriptive Themes.
Citizenship
The first analytic theme focuses on patients’ agency in care. This includes being empowered to contribute to or to make choices in their treatment and a sense of feeling heard – and responded to – by care providers.
‘I wanted a total cut out from where I was in, so I asked for help in a, in, in a way, say look can you take me to hospital and let me sort my head out’ (Rye, 2017, p. 109)
Engagement was also emphasised as a key component in the recovery process. There were frequent discussions of the importance of patients choosing to engage with their care team or plan their aspects of their care. A patient’s responsibility for their own care was in part echoed by patients’ parents as well: ‘He is the only one who is in charge of his own destiny’ (Allan, 2013, p. 76).
However, not all patients reported having agency over their outcomes: ‘Well the doctor and the teams decide to bring you back in, um, but I think, yeah, if it was down to me I probably would’ve just stayed out there’ (Rye, 2017, p. 109).
Agency and responsibility were also related to mental illness. Some patients saw mental illness as the cause of their offending, some drew on it to explain certain behaviours and actions, though not all and yet others acknowledged mental health needs but didn’t link these to their offending (Dixon, 2018).
One individual discussed the difficulty in getting others to listen:
‘I: Do you see yourself as being dangerous? P: No I’m not dangerous, but like I said though, it’s like talking to the brick wall, isn’t it? I can’t get no sense into anybody’ (Coffey, 2012a, p. 473).
While parents may have had valuable information to contribute, many reported feeling dismissed given their lack of professional expertise:
‘I spent six months at least [. . .] telling the people who were supposed to be supervising him that he wasn’t; that ‘he’s not taking his medication, I know he’s not, I just know it’. And they ‘well, we can’t do anything, you know, until we have the proof’. I said ‘but, you know, I know he’s not taking it, I know he’s not well’ (Allan, 2013, p. 85).
Reflecting on a Journey
This theme focuses on how patients made sense of and told the stories about their own experiences. They did this by reflecting on their pasts, forging new identities and dealing with uncertain futures.
‘Victim empathy wasn’t easy . . .you’re in a situation you have to accept you are convicted of a crime of assault’ (Alred, 2018, p. 120).
However, some service users were able to turn their history around and help make it an integral part of their recovery:
‘My forensic history is an issue and I do carry that around with me as baggage day-to-day. It kind of explains the reason that I am so keen to work as an ex service user because in that capacity my baggage is accepted and it actually, what’s the word, it’s relevant’ (Alred, 2018, p. 138).
In moving away from their ‘criminal pasts’, patients also spoke of ways that they attempted to create new identities outside of hospital. Some patients compared their journeys to others to remind themselves of where they had come from, or that they were on a positive pathway to recovery by comparison (Alred, 2018, p. 117). While some distanced themselves from others, some patients reported feeling more comfortable around those with similar backgrounds:
‘I feel a lot more at home with my people, people um who have mental health. . .that’s why I go to church services because I meet mental health service users there and a lot of my friends now they just don’t understand me anymore’ (Alred, 2018, p. 126).
A lack of certainty or clear plan for progression were often reframed and managed as ‘taking it day-by-day’ (Alred, 2018, p. 118) or ‘one-day-at-a-time’ (Alred, 2018, p. 131). Use of such language operated a form of coping, focusing on recovery in the short-term.
This was echoed in parents’ accounts:
‘At this stage I was hoping for a, a little steady job for him, you know, something that he could actually cope with and hold down [. . .] I just wanted to play it all by ear, deal with it stage by stage, as something come along you deal with that, and then, it’s time to go on to the next, you know; perhaps this could happen, you know?’ (Allan, 2013, p. 58).
Short-term, smaller goals were seen as more manageable or realistic.
Hopefulness was present in patient and parent narratives (Whittaker et al., 2023). These typically pertained to working towards autonomy and self-sufficiency. Interestingly, these hopes were recalibrated over time:
‘Laura had previously described her hope that her son would become an engineer. She now saw his achievements in terms of overcoming his mental health difficulties, which gave her a sense of pride in him’ (Allan, 2013, p. 61).
Staff Experiences
This theme describes how practitioners reflected upon their experiences. They highlighted tensions in their role, aspects they dislike, how they structure and approach their praxis and the importance of communication.
‘The role of the social supervisor is much to do with control, challenge and change. You balance that with advise, assist and befriend’ (Riordan et al., 2006, p. 7).
Some staff interviewees sought to make sense of this by conceptualising an appropriate degree of control:
‘Compulsory powers are generally perceived as ‘a necessary evil’ and indiscriminate use of compulsory powers is regarded as poor practice’ (Jenkins & Coffey, 2002, p. 558).
Other staff used the legal framework obligating engagement in supervision as a form of ‘insurance’, in which ‘They [patients] are more likely to see me as an authority figure . . . more likely to comply with suggestions, take medication’ (Jenkins & Coffey, 2002, p. 558; brackets added by authors).
The push-and-pull of the competing priorities and responsibilities meant that for some staff the therapeutic relationship was affected detrimentally.
Some staff didn’t want to be involved in certain cases at all. This was to a degree due to perceptions of patient dishonesty and inadequate communication. In Riordan et al. (2006, p. 8) study, this was linked to anxiety:
‘He doesn’t always tell you the problems until it’s too late. . . If he were more honest it would help my anxiety levels’.
Others reported feeling threatened by some patients:
‘He’s quite a dangerous man. He’s forced to see me, that doesn’t make me feel very comfortable. He’s a difficult person to get on with; I don’t like to see him on my own’ (Riordan et al., 2005, p. 175).
There were also instances of unacceptable staff behaviour towards patients, emphasising the necessity of setting clear boundaries. Chiringa et al. (2014) found that several patients gave accounts of hostel staff taking illicit substances and drinking with patients.
They also described challenges collaborating with other services to arrange healthcare or housing interventions (Vaughan et al., 2000). Making and maintaining contact with patients was seen as difficult with those patients who live mobile and ‘chaotic’ lives, especially when caseloads were high. They also reported that increasing supervision in light of a lack of patient engagement lead some patients to feel threatened by the risk of recall – that more intervention could be counterproductive (Whittaker et al., 2023).
Planning patient activities and aligning schedules was raised as important but challenging. Coffey (2013) noted that patients and staff have different expectations on the duration and frequency with which things can be planned. Social workers reported not wanting to be pinned down to any specific timetable until they knew more about their patient. Time allowed for developing a relationship, understanding risk and information gathering. Dixon (2012) found that patients believed risk assessments existed but were unaware of their content. This was an area for improvement as patients often disagreed with risk assessments and identified risks that staff were not aware of.
In Vaughan et al. (2000), staff identified areas of specialisation they felt they most needed to develop, these included substance misuse, learning disabilities and offending behaviour. The need for training on substance use was echoed in Riordan et al. (2005).
‘I was supposed to see the doctor, that night where the staff, that one particular night, they said I had to go and see the doctor the following day. So I slept, and the next day, they said, ‘you do not have to go and see the doctor.’ So I didn’t see the doctor that day then the doctor and (name) . . . and the doctor said you should come and see me. There was confusion. It wasn’t my fault. (Participant A)’ (Chiringa et al., 2014, p. 342).
Whittaker et al.’s (2023) study reported that staff felt patients were sometimes withholding information to downplay symptom severity and reduce the risk of recall. A patient in the same study noted that trust was needed to overcome this fear.
Coffey (2011) observed that over time and across a series of turn-by-turn interactions with staff, patients’ developing social identities were to some extent shaped by social supervisors and the legal and clinical frameworks within which they meet. Coffey (2012a) noted some patients drew on their status as a restricted patient to legitimate a sick role claim.
The same author made the case that staff categorised patients and adopted language descriptive of these categories to discursively steer cases towards certain outcomes or downplay the reliability of certain patients’ accounts if they challenged those of staff (Coffey, 2011). He proposed that a community psychiatric nurse (CPN) interviewee categorised a patient and inferred certain kinds of behaviours and an unreliability from this:
‘The CPN implicates Iestyn [patient] as a particular category of person. The presence of a category was established with the phrase ‘somebody like [Iestyn]’’ (p. 754).
These excerpts highlight the discursive powers social supervisors have.
Wellbeing and Recovery
This theme describes aspects of care, recovery and wellbeing discussed by patients and staff. Strategies for managing the challenges – affective, social and psychological – of life in the community are highlighted, as are accounts of patients’ wellbeing.
For one patient, their struggles came from difficulties coping with life in the community and managing everything:
‘I had so much going on, with this, that, and the other [. . .] and <oogh!> everything flew in the air!’ (Rye, 2017, p. 104).
Being evicted from or lacking accommodation was a reason for recall (Whittaker et al., 2023). Patients reflected that the housing they were placed in was too far from family or didn’t have any patients from a similar ethnic background. These factors made it hard for them to connect to others. Moving to less supportive housing was seen by staff as an important step in the conditional discharge process, as it gave patients a chance to demonstrate progress.
Regular opportunities to speak to members of staff about anxieties and concerns were important for patients:
‘If I’m in independent living I hope I’ve got a phone number of a CPN or something like that so I can ring them and say “look, look at this I’m having problems”’. (McDonnaugh et al., 2020, p. 64).
Some patients described the role of work and hobbies in coping with life in the community. Rye (2017) found that for some patients, having a job was linked to getting back on track and coping.
‘Most of those participants relapsed into taking drugs, and two other participants described taking drugs to cope with the stress they were experiencing’ (p. 104).
Riordan et al. (2006) found that the majority of social supervisors they interviewed supported standardised drug testing for service users.
Studies noted that patients often felt lonely in the community (Allan, 2013; Alred, 2018; Whittaker et al., 2023). The literature identified that although some patients were transferred into supported housing with other residents, patients did not feel connected and struggled with loneliness, with one comparing this to the supportive presence of others in hospital (Chiringa et al., 2014).
Self-harm was reported in several studies (inc. Coffey, 2012a). Jenkins and Coffey (2002) noted that most social supervisors saw restriction orders as unhelpful to managing self-harm and that care planning and therapeutic intervention are more important.
Systemic
This theme relates to challenges that respondents encountered with different services, teams and procedures within the system.
‘I never realised how [. . .] difficult it was to get somebody out of the system when we found it so hard to get him into the system. Seems so strange, that it took 90% illness to get him in, and it takes a perfection illness, or a lack of illness to get him out’ (Allan, 2013, p. 88).
Parents described the system having its own rules and language (Allan, 2013):
‘We don’t have open communication with them because [. . .] actually we don’t seem to have the same language as them’ (p. 88).
Beyond the system itself, parents also noted a sense of powerlessness over their child’s care, perhaps as a consequence of the desire for their child to have increased autonomy and freedom.
‘All I can honestly say here in 2015 I’ve landed and I have survived’ (Alred, 2018, p. 122).
Such accounts paint a picture of patients having been through an ordeal, with some highlighting how the ‘uncaring’ environment was not a place where one could focus on changing for the better.
There was also a sense of conditionally discharged patients ‘ticking boxes’, with the belief that they were often going through the motions, as opposed to doing something that would generally benefit themselves.
There were also descriptions of bureaucratic challenges for example, discharge conditions specified where patients were able to live even though this removed them from their familial support system (Chiringa et al., 2014).
Dixon (2015) explored patients’ views on their restriction orders. He found that some saw it as necessary for treatment, while others viewed it as disciplinary control. A third group felt it unfairly labelled them, restricting their identity.
‘I moved in had a breakdown, floods of tears because I couldn’t believe the journey I’d been on. I just stood in [t]his empty flat that I knew had been signed over to me. I knew it was my first home for a long, long time’ (Alred, 2018, p. 140).
For others, discharge and recall was a recursive process. In being unable to obtain help for her son when she realised he wasn’t taking his medication, one parent reported:
‘I was just so, so, well, frightened, quite frankly, and thinking, what am I going to do now? Here we go again’ (Allan, 2013, p. 71).
Patients also described situations where they were faced with trauma from their pasts (Whittaker et al., 2023), and having to be around people and behaviours that they associated with their past selves, which could mean sliding towards relapse:
‘You go through all that process and right at the end when they have got you well they plonk you in the deep end back into a world where people have still got all them problems and you’ve already dealt with it and you don’t want to deal with it again’ (Alred, 2018, p. 139).
This non-linearity spoke to a sense some had of inevitability, that recall is part of the journey and something to accept. Some patients reflected that recall was helpful: ‘I definitely needed to come into hospital as my mental health was really poor’ (Whittaker et al., 2023).
Connectedness
Patients’ relationships and interactions with others were seen as key indicators of success and recovery, as well as contributors for recall.
Difficulties also arose for patients who wanted to avoid acquaintances whom they thought were negative influences or untrustworthy:
‘At odd times they’d come and knock and it was just getting to me, and it was frustrating me, annoying me, and all of that circle - I didn’t, don’t need that’ (Rye, 2017, p. 104).
A participant in Chiringa et al.’s (2014) study felt that it was only possible for them to make friends with certain groups of people, all of whom were the wrong kind of people:
‘. . .derelict people in the community like alcoholics, drug addicts and prostitutes, these three types of people are not decent people. You don’t know them, you have just got back after 3 to 5 years so you have to be wary of these type of people again . . . these are the people you have to escape. But it is only these people, they are the only people available to you freely to be friends with. (Participant B)’ (p. 341).
More frequently, connections were described as a source of support. Rye (2017) observed that patient participants who were enjoying life in the community felt more connected to others. Jenkins & Coffey (2002) and Riordan et al. (2005) found that, in contradiction to the staff participant described in the previous paragraph, staff viewed restriction orders as improving engagement in services, which allowed trust and therapeutic relationships to develop over time.
Rye (2017) describes two patients for whom children were important factors in their recovery. One participant recounted losing contact with his son, after which he used ketamine to achieve a sense of escapism to avoid ‘thinking the worst’ and was then recalled. A second participant, Caleb, saw parenting as a motivation:
‘I’m being totally honest now, and, and er I wanna change my ways and I want a different lifestyle, y’know, I got, I got motivation like my daughter, family, y’know all that plays a part but (1 second inaudible), the point is that I’m, I’m cooperating more than I was before, and that makes a lot of difference, you see?’ (p. 113).
Discussion
This review aimed to identify and synthesise the available qualitative research evidence regarding patients on conditional discharge from forensic mental health services in England and Wales published since 1983. Qualitative findings from 15 qualitative and five mixed-methods studies were included.
The key finding of our review is that existing desistance theories can and should be expanded to better account for the unique experiences of forensic mental health patients on conditional discharge. Specifically, epistemic injustice and stigma present significant barriers to identity- and relational-desistance, making it harder for patients to transition into non-offending identities and reintegrate into the community. To support desistance in this population, approaches such as procedural justice, shared decision-making and peer support should be emphasised, as they help counteract stigma, empower patients and foster community belonging. We unpack this below.
Desistance has been described as a process. Maruna and Farrall (2004) identify primary and secondary desistance, the former a reference to a gap or cessation in offending and the latter the adoption of a non-offending identity. This identity shift can precede or be influenced by shifts in social roles, ‘turning points’ or changes in attachments to informal social bonds. This adoption, though inescapably informed by socio-structural factors (Farrall et al., 2010), marks a reappraisal of the perceived benefits of a prosocial life. McNeill (2016) has added ‘tertiary desistance’ to this conceptualisation. This is the social recognition of change and the development of belonging and sense of community that comes with such recognition. Emphasising the non-linearity of desistance (an observation also made in our review with respect to recall to hospital), Nugent and Schinkel (2016) reframe these three ‘phases’ as: act-, identity-, and relational-desistance. It is the latter two with which our review findings are most related.
Interviewees in our review described the challenges (and opportunities) of escaping past offending identities and experiencing barriers to recovery/reintegration due to stigma. These accounts are accompanied by experiences of not feeling listened to or believed. These findings reflect qualitative studies with forensic in-patients (Tomlin et al., 2020), and general mental health patients (e.g., Fusar-Poli et al., 2022). Maruna and Farrall (2004) propose that Gidden’s description of ‘social identities’ and ‘position practices’ can help us frame why such perceptions exist for ex-offenders. These can be applied to forensic mental health patients too. ‘“Social identities, and the position-practice relations associated with them, are. . .associated with normative rights, obligations and sanctions which, within specific collectivities, form roles”’ (Giddens, 1984, pp. 282–283; cited in Maruna & Farrall, 2004). Social identities define expectations around who people are and how they are expected to act.
Patients on conditional discharge carry a social identity and position practices that are clearly delineated in public perception. These are highly stigmatised identities, wherein patients are considered mad, bad and sad, whose actions are unexplainable or violent (Mezey et al., 2016). This social identity is hard to change given the link between power, influence and social capital in establishing and maintaining stigmatised identities (Dufour et al., 2015; Link & Phelan, 2001). Contributing to the fixity of this social identity is the phenomenon of pathologisation: that forensic mental health patients’ beliefs, experiences and behaviours (position-practices) are seen by some as evidence of mental illness, perhaps to be ignored or dismissed. This renders forensic mental health patients as less trustworthy/believable and their motivations irrational in the eyes of some observers.
The concept of epistemic injustice captures this well. Drawing on Fricker (2007), Markham (2022) defines epistemic injustice as ‘a phenomenon in which a person is wronged in their capacity as a knower due to prejudice, and thus transmission of knowledge via testimony is impaired’ (p. 152). Occasions of epistemic injustice, seen where the social identities and the position-practices of forensic patients are given primacy over epistemic justice, make it less likely that identity and relational desistance are realised. Community members may find it hard to believe and trust forensic patients’ motivations to engage in recovery and live offending-free lifestyles. This makes developing a sense of belonging and community challenging. Identity desistance is harder to achieve as self-expression, sharing and feeling listened to by peers are crucial components of identity development (Maruna & Farrall, 2004; Weaver, 2019). Theories of desistance would benefit from accounting more fulsomely with experiences of epistemic injustice reported by individuals in the criminal justice system with mental illness.
The literature offers several avenues though which to counteract epistemic injustice and support the dialectic relationship between identity- and relational-desistance. Procedural justice theory suggests that where interlocutors are treated by individuals in positions of authority in a way that maximises voice, dignity and respect, neutrality, clear communication and evidences a motivation to work in that person’s best interests, satisfaction with the interaction and engagement in treatment and criminal justice proceedings are improved (Tomlin et al., 2024). Shared decision-making practices in healthcare prioritise patient empowerment and agency by offering clinicians structured approaches to co-produce treatment plans with, rather than for, patients (Slade, 2017). Peer support roles and recovery colleges value the lived experience of patients and use this to support recovery through empathy, shared experience, individualising care in ways not typically included in traditional psychosocial approaches and creating a sense of belonging and community (Arbour & Rose, 2018). These activities would go some way to supporting patients to develop non-offending identities and belonging in communities that come to see their motivations, behaviours and position-practices as inconsistent with stigmatised social identities often associated with the forensic mental health patient social identity.
Future research should explore patient experiences of desistance to explicitly address the relevance of these theories to this population. Interviewing patients and members of their social networks would help unpack how others view and consequently interact with patients and how this is linked to (non-)offending identities and group belonging. This work should draw on concepts like ‘social identities’, ‘position practices’, ‘pathologisation’, ‘epistemic standpoints’ and ‘turning points’. Future research should more explicitly focus on the experience of this population using an intersectional approach. This is due to (1) the absence of qualitative research in this review addressing specific personal characteristics and (2) the findings of our quantitative review (part one; Kilbane et al., 2025), which found that age, ethnicity, gender and diagnosis were differentially linked to positive and negative outcomes (e.g., recall, recidivism, and meaningful relationships).
Conclusion
This paper described a thematic analysis of 15 qualitative and five mixed methods publications found in a systematic literature review exploring the experiences of forensic patients on conditional discharge in England and Wales. Six analytic themes were developed that describe the experiences of patients, carers and staff. We chose to situate our findings in the desistance literature to offer additional insights into the experiences of this population and guide future research and scholarship. Our review extends this literature by highlighting a need to engage more richly with the experiences of individuals in the criminal justice system who have mental health diagnoses and the epistemic injustice and stigma pertinent to this group and how these impact on the maintenance of identity- and relational-desistance.
Supplemental Material
sj-docx-1-ijo-10.1177_0306624X251357614 – Supplemental material for Systematic Review of Forensic Mental Health Patients on Conditional Discharge: Part Two – Qualitative Findings Using a Desistance Lens
Supplemental material, sj-docx-1-ijo-10.1177_0306624X251357614 for Systematic Review of Forensic Mental Health Patients on Conditional Discharge: Part Two – Qualitative Findings Using a Desistance Lens by Jack Tomlin, Alison Romero, Maria Zamorano, Mel Jordan, Shelley Turner and Sarah Kilbane in International Journal of Offender Therapy and Comparative Criminology
Footnotes
Acknowledgements
We would like to thank David Cochrane for his support of this work.
Ethical Considerations
As a literature review of publicly accessible data, no ethical issues arose. No formal ethical review was required.
Consent to Participate
As a literature review of publicly accessible data, no consent was required.
Consent for Publication
As a literature review of publicly accessible data, no consent was required for publication.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was funded by Health Education England to assist the New Roles Social Work Group to establish Health Education England e-LfH training on social supervision. Additional support was provided by West London NHS Trust.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
As a literature review of publicly accessible data, data are publicly accessible.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.