
Abstract
Individuals who engage in criminal behavior for which they are found not criminally responsible (NCR) may be at increased vulnerability to experience moral pain and, in extreme circumstances, moral injury after regaining insight into the consequences of their behavior. Yet, almost no research exists characterizing the nature, severity, or impact of moral pain in this population. Semi-structured interviews were conducted with nine forensic psychiatric patients and 21 of their care providers. Narratives were explored using thematic analysis. Findings demonstrate that NCR patients endorse symptoms consistent with moral injury, including feelings of guilt toward victims, shame for one’s behavior, and a loss of trust in one’s morality. Moral pain is a strong driver of behavior and must be understood as part of a constellation of factors influencing criminality, risk, and recovery. Future research must develop adequate tools to measure and characterize offense-related moral injury to understand its impact on this population.
Background
Moral pain involving the experience of negative moral emotions like guilt, shame, and anger provides immediate feedback as a consequence (or in anticipation) of our own behavior or that of others and can influence future behavioral decision-making (Tangney et al., 2007). When an individual behaves in a way that violates their moral code (committing interpersonal violence, engaging in criminal behavior, cheating, stealing, etc.), moral pain serves as punishment that deters reengaging in similar behavior in the future.
Mild experiences of moral pain are likely socially adaptive, discouraging immoral behavior that may harm the social group (Haidt, 2003; Teper et al., 2015). More recently, however, researchers have become interested in examining the psychological impact of more extreme and prolonged experiences of moral pain. Here, the term moral injury (MI) has emerged to describe a syndrome characterized by psychological distress and impairment following the perpetration or witnessing of morally violating behavior (Drescher et al., 2011; Litz et al., 2009). To date, MI has been studied primarily in military members following deployment (Hoffman et al., 2019) and has yet to be examined in contexts where the moral violation is not legally justified, for example, after committing a criminal offense. The current investigation qualitatively explored morally injurious symptomology in a sample of justice-involved individuals found not criminally responsible (NCR) on account of mental disorder to determine the emotional experiences of these individuals following their index offense.
MI
Emerging from the military trauma literature, MI was first defined as an emotional, spiritual, and psychological wound resulting from acts of commission or omissions that violate one’s sense of morality and give rise to profound inner moral conflict (Drescher et al., 2011; Litz et al., 2009). Initial measures of MI assessed for the experience of potentially morally injurious events that fell under one of two categories: perpetration via commission or omission of morally violating acts (e.g., killing nonenemy combatants in the line of duty, failing to save a life) or morally violating betrayals (e.g., receiving orders from superiors to stand down and be complicit in the suffering of others). These early characterizations of MI were phenomenological in nature and were criticized for their focus on population-specific exposure to potentially morally injurious events rather than the experience of a moral wound (Frankfurt & Frazier, 2016; Litz & Kerig, 2019; Yeterian et al., 2019).
More recently, work has been done to expand both the definition of MI and the populations in which it is studied. For example, syndromal definitions of MI have been put forward in an effort to offer a clear and cohesive description that can be used to identify MI symptomology regardless of the population being studied. One such perspective comes from Jinkerson (2016), who described MI as “a particular trauma syndrome including psychological, existential, behavioral, and interpersonal issues that emerge following perceived violations of deep moral beliefs by oneself or trusted individuals” (p. 126). Here, four core symptoms of MI are identified: guilt, shame, spiritual/existential conflict, and a loss of trust in oneself, others, or higher beings. Secondary symptoms are then noted to result from core symptoms, including feelings of depression, anxiety, and anger; reexperiencing the moral conflict; self-harm; and social problems (Jinkerson, 2016). Although this syndromal definition does not preclude incorporating traditional understandings of MI development (i.e., most often following moral perpetrations or moral betrayals), it offers a way to explore and characterize MI across populations by focusing on its consequences rather than its determinants.
Research examining MI outside of the military context has only recently begun to consider its relevance to populations including youth and teachers exposed to violence (Chaplo et al., 2019; Currier, Holland, Rojas-Flores, et al., 2015), refugees (Hoffman et al., 2019; Nickerson et al., 2018), as well as health care providers and public safety personnel (Førde & Aasland, 2008; Fourie, 2015; Huffman & Rittenmeyer, 2012; Papazoglou et al., 2020; Papazoglou & Chopko, 2017; Roth et al., 2021a, 2021b). For example, individuals in public health and safety positions are often faced with morally conflicting, high-stakes decision-making in which they must take responsibility for life-or-death choices and outcomes (e.g., lethal use of force, allocating life-saving resources to one patient at the expense of another). Chronic and repeated exposure to these events may increase experiences of moral pain and the likelihood of developing MI (Papazoglou et al., 2020; Papazoglou & Chopko, 2017).
Increasingly, MI has been associated with several adverse social, psychological, and spiritual outcomes. This is due, in part, to the profound experiences of guilt and shame known to be associated with MI. Both guilt and shame are negative moral emotions that have been independently implicated in the development and maintenance of depression, anxiety, and posttraumatic stress disorder (PTSD; Leskela et al., 2002; Marx et al., 2010; Nazarov et al., 2015). Although often incorrectly synonymized and confounded in moral emotion research, guilt and shame are distinct affective experiences with unique psychological and behavioral implications (Lewis, 1971; Tangney, 1999). Shame is a painful self-conscious emotion associated with self-depreciation, defensive avoidance, and a desire to hide or externalize blame (Tangney et al., 2007). By contrast, guilt is typically behavior focused, less painful than shame, associated with remorse and worry about the consequences of one’s actions, and more likely to motivate reparative actions (Tangney et al., 2007). To date, no studies have attempted to disentangle the unique contributions of shame, guilt, and other morally relevant emotions in the experience of MI (Yeterian et al., 2019). This may be particularly relevant for justice-involved populations where these emotions—experienced individually or as part of a syndrome like MI—may hold distinct implications for risk and recidivism.
Above and beyond the established impact of emotions like guilt and shame on psychological health, more recent work has linked MI directly to adverse mental health outcomes. Across populations, MI has been associated with depression, anxiety, and PTSD, as well as other adverse psychiatric and psychological sequelae such as suicidality and self-harm, self-handicapping and risk-taking, anger and hostility, and social withdrawal (Bryan et al., 2014; Currier, Holland, & Malott, 2015; Currier, Holland, Rojas-Flores, et al., 2015; Hoffman et al., 2018, 2019; McEwen et al., 2020; Nash et al., 2013; Nazarov et al., 2018; Nickerson et al., 2015, 2018; Papazoglou et al., 2020; Worthington & Langberg, 2012). In addition, meta-analyses have shown moral pain and MI to be negatively related to resilience, social adjustment, positive affect, and occupational functioning (Crane et al., 2015; Williamson et al., 2018). Although still in its infancy, the existing MI literature points toward common psychosocial sequelae associated with MI across contexts, suggesting that adopting a syndromal perspective of MI would be most useful to expand its research to new populations.
Moral Pain in Forensic Psychiatry
To date, no studies have explored MI in perpetrators of nonlegally justified moral violations, for example, following the commission of a criminal offense. Here, it is possible that many justice-involved individuals will be susceptible to moral pain and subsequent MI. For example, an individual may experience guilt or shame if their offense involved behavior that violates their own moral code (i.e., a moral perpetration), or feelings of anger and injustice if they felt compelled to offend by necessity due to a perceived failure of an institutional safety net (i.e., a moral betrayal).
Moral pain resulting from a discrepancy between an individual’s moral code and their criminal offense may be particularly salient for individuals in forensic psychiatry who were found NCR on account of mental disorder. Under provisions made by the Canadian Criminal Code, NCR verdicts are reserved for those who commit criminal offenses while experiencing symptoms of a major mental disorder that renders the individual incapable of appreciating the nature and quality of the act or omission, or knowing that it was wrong (Criminal Code, R.S.C., 1985, c. C-46). Here, individuals undergo a thorough psychiatric assessment that provides a recommendation to the Court regarding the question of NCR on account of mental disorder. While specific conditions for NCR eligibility are not delineated in the Criminal Code of Canada, typical psychiatric diagnoses examined for this purpose include schizophrenia, delusional disorder, bipolar disorder, and organic mental disorders. Less typical diagnoses include PTSD, personality disorders, and paraphilias. While only a relatively small proportion of those who come into contact with the law in Canada meet the threshold of NCR (~1% of annual criminal court cases; Latimer & Lawrence, 2006; Miladinovic & Lukassen, 2014), the incongruence between one’s offense-related behavior and their typical demeanor may leave individuals found NCR particularly vulnerable to symptoms of MI. This may be most notably relevant for individuals who experience a reduction in psychiatric symptoms as they progress through treatment and recovery, thereby (re)gaining insight into their offense and the consequences of their actions.
Surprisingly, very few studies have explored the relation between offending and moral emotions more broadly, and those that have are limited in several ways. These studies tend to examine trait levels of independent emotions and their relation to antisocial activity rather than moral pain as a complex construct resulting from a specific offense (Barón et al., 2018; Tangney et al., 2007). This body of research has also been critiqued for producing inconsistent results surrounding the presence and impact of certain moral emotions, particularly guilt and shame (likely due to the tendency to confound the two emotions; Stuewig et al., 2015; Tibbetts, 2003). Moreover, most research concerning offending behavior and moral emotions has been conducted in nonclinical samples and in situations involving minor law violations where profound moral pain is less likely (Tangney et al., 2007).
Nonetheless, a small body of psychological and criminological research suggests that the perpetration of a criminal offense may precipitate more profound levels of distress. Research exploring PTSD in justice-involved individuals experiencing mental health issues reveals that the perpetration of a crime, especially when violent in nature, may lead to offense-related guilt and the development of PTSD, a stress disorder related, but distinct from MI (Crisford et al., 2008; Gray et al., 2003; Papanastassiou et al., 2004; Pollock, 1999). Although preliminary, these findings are important in identifying a relation between committing an offense while mentally ill and the subsequent development of psychological distress and suggest that individuals found NCR may be particularly vulnerable to the development of MI.
The Current Study
Relative to others who engage in morally violating behavior, individuals found NCR may be more susceptible to moral pain following an offense due to their diminished access to morally relevant information and decision-making related to the presence of acute psychiatric symptoms. To date, however, MI in NCR populations remains unexamined. The current investigation is the first stage of a multiphased, mixed-methods project aimed at exploring, measuring, and characterizing the morally injurious experiences of individuals found NCR. The study presented here has the following aims:
To preliminarily and qualitatively explore the presence of symptoms consistent with MI in justice-involved individuals found NCR.
To provisionally determine the utility of including staff perspectives of patient experiences by exploring the relation between patient and staff accounts.
With these aims in mind, the current study is a pilot investigation into the moral emotional experiences of individuals found NCR that will serve to inform later phases of the current project and future research in the area more broadly. This study was not conducted to provide an in-depth model that explains why or how MI occurs in forensic psychiatric patients (e.g., grounded theory analysis). Instead, utilizing accounts from both patients and their care providers, we employed descriptive thematic analytic procedures to provide an initial survey of the emotions experienced after committing a crime that might be indicative of MI in this population and provide justification for future work in this area.
We hypothesized that while many of the characteristic symptoms of MI would be endorsed by individuals found NCR, distinct presentations with unique catalysts would also be present. In light of these aims, the syndromal definition of MI formulated by Jinkerson (2016) was used to guide the query of known MI symptoms while also allowing for novel symptom manifestations to emerge under careful and structured examination, given the unique experiences of this population.
Method
Design
A qualitative descriptive approach using thematic analysis was used to explore the moral affective experiences of forensic psychiatric patients. Thematic analysis is a qualitative research method that allows for respondents to present their experiences and perceptions in interview format and provides a framework for identifying, analyzing, and reporting patterns within data (Braun & Clarke, 2006). This approach was deemed most suitable given its flexibility in allowing for both deductive and inductive approaches. A top-down, theoretical approach was necessary to conceptualize and interpret the data in light of our current understanding of MI; however, a bottom-up, data-driven approach was also necessary to avoid overlooking any themes of MI that might be uniquely relevant or present in a forensic psychiatric population.
Materials
With the intent to increase patient-participants’ sense of agency, openness, and trust, we chose not to request consent to conduct a medical chart review and instead collected demographic information (psychiatric diagnosis, length of time as an inpatient, etc.) via an optional demographics questionnaire. Study materials also included an Interview Guide (see the appendix) that was generated through discussions with experts in trauma, MI, and forensics research and that queried four broad domains: (a) the kinds of emotions experienced before, during, and after the offense; (b) the experiences of negative moral affect like guilt and shame around the index offense; (c) general feelings around morality and “right and wrong”; and (d) general feelings toward the forensic system (i.e., the criminal justice system and the mental health care system).
Participants
Following approval by the Hamilton Integrated Research Ethics Board, participants were recruited from a Forensic Psychiatry Program situated within a larger mental health and addictions facility in Canada. Participants (N = 29) included (a) forensic psychiatry inpatients found NCR who were asked to reflect on their own emotional experiences, and (b) clinical care team staff members who were asked to reflect on the emotional experiences they have observed in their patients throughout their career in forensic psychiatry. The total inpatient census at the time of recruitment was 70. The eligible staff at the time of recruitment included 93 nurses, 11 psychiatrists, four social workers, and three occupational therapists.
Participating staff (n = 20) represented providers across all disciplines and four inpatient units and reported between 2 months and 30 years (M = 7 years, SD = 8.4) of specialized experience in forensic psychiatry. Eleven patients were identified by members of their care team as fitting our inclusion/exclusion criteria (fluent in English and not acutely psychotic); of those, nine NCR individuals consented to participate in the study. While participation in our study was open to both male- and female-identifying individuals, our male-to-female ratio (8:1) is reflective of an overrepresentation of males in the Forensic Psychiatric System. Patient self-reported demographics of interest are presented in Table 1.
Patient-Participant Demographics
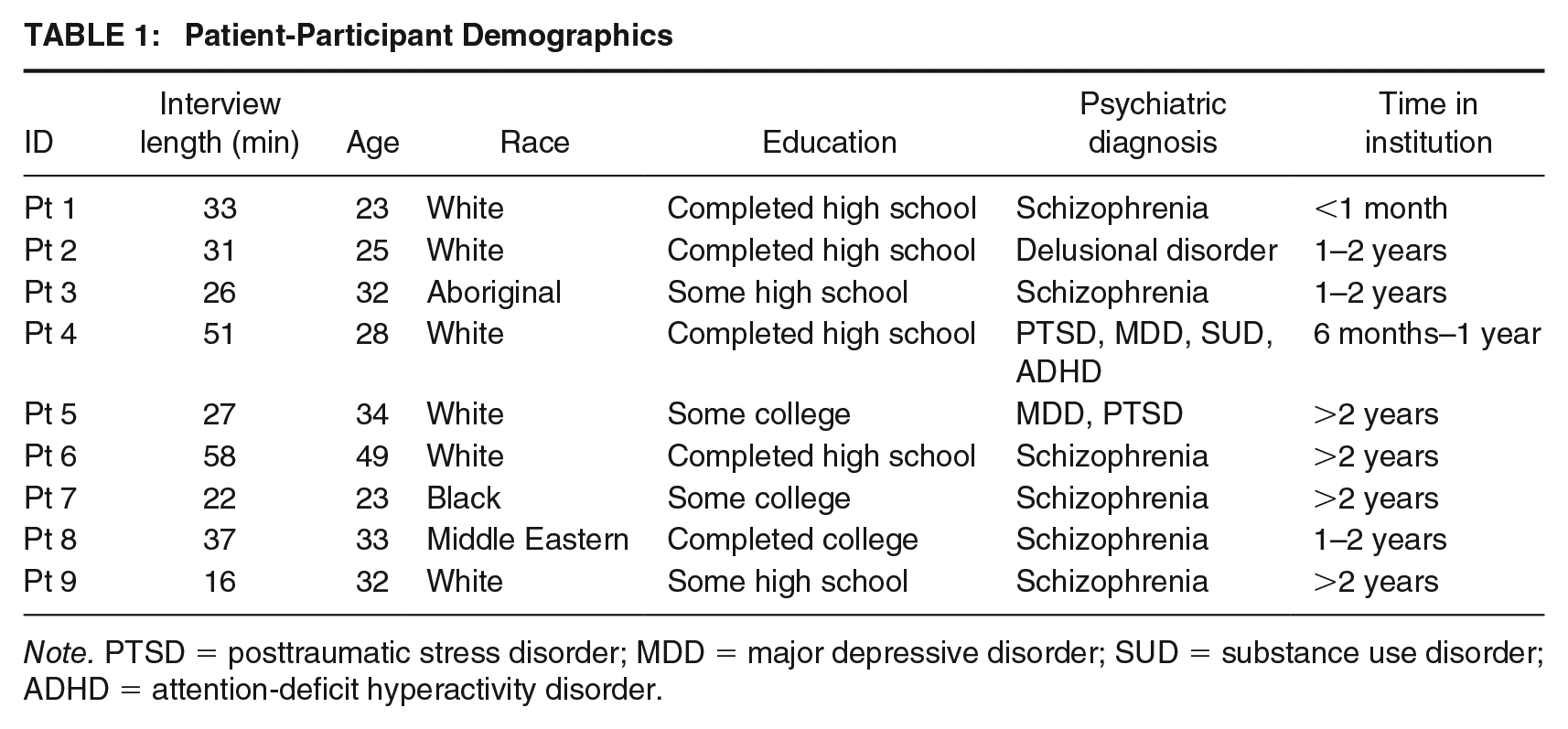
Note. PTSD = posttraumatic stress disorder; MDD = major depressive disorder; SUD = substance use disorder; ADHD = attention-deficit hyperactivity disorder.
Procedures
Recruitment
As is commonplace in qualitative research, purposeful sampling was conducted in phases and included both convenience and snowball sampling methods. First, staff members were made aware of the study during regularly scheduled clinical team huddles that took place on each unit. At these meetings, the purpose and rationale of the study were briefly outlined and staff were made aware of the date, time, and location of six focus groups that were to take place in the coming weeks. One interested staff member was not able to attend focus group sessions and was offered an individual interview instead. At the end of each focus group, participating staff members were asked about current inpatients who might be interested in participating in an individual interview. Staff were asked to consider factors such as the general disposition of their patients (i.e., patients who reported or were observed to express strong emotions would be most fitting) as well as the patient’s general ability and willingness to engage in emotionally salient conversations. Once potential patients were identified, each unit’s charge nurse made initial contact with patients to briefly describe the study and to obtain consent for a research team member to approach the patient with further study details. Interested patients were given an interview date within the following week.
Interviews
Prior to the start of focus groups and interviews, all participants were oriented to the purpose of the study via a formal letter of information that was read by the interviewer and participants together with opportunities for any questions. After all questions were addressed, written consent was obtained to move forward with interviews and audio-recording. Focus group interviews with staff were led by a moderator and co-moderator and lasted between 30 min and 1 hr. Staff were instructed to reflect on their general observations of their patients throughout their career in forensic psychiatry and to give specific examples (omitting any identifying information) where possible. Staff members were thanked for their participation with token gifts of consumable treats. Patients were interviewed individually to maintain privacy and confidentiality; these interviews ranged in length from 16 to 58 min with an average length of 33 min. Patients were asked questions about their own emotional experiences since the commission of the index offense. Patients were also asked to complete the demographics questionnaire at this time. Importantly, patients were informed prior to consent that participation did not require disclosing specific details surrounding the index offense, but were encouraged to share any details they deemed important in recounting their experiences. Of those patients who voluntarily disclosed details about the type/severity of offense, index offenses as described by patients ranged from relatively minor offenses (e.g., parole violations, dangerous possession of a weapon) to more severe offenses (e.g., assault, murder). Patients were compensated with a Can$10 gift card for their time and informed that support resources would be made available to them should they experience any psychological distress as a result of their participation. Nursing staff were aware of all patient interviews taking place and were asked to be mindful of any signs of distress that may occur to patients following participation.
Data Analysis
Data were collected and transcribed by one researcher. Upon completion of transcription, quality checking was conducted by a second researcher to ensure transcripts were accurate and anonymized.
To analyze the data, two members of the research team independently read, reread, and coded each transcript using open coding (Straus & Corbin, 1990). After three transcripts were independently coded, the researchers met to discuss preliminary patterns generated from the data and to assess their level of agreement and disagreement; anywhere that disagreements occurred, the researchers discussed the code under consideration until a consensus was reached. From these discussions, a codebook with a systematic coding scheme was generated that included a list of all codes and their definition, as well as examples and nonexamples. This codebook was then used for the analysis of each subsequent interview transcript and was supplemented when new patterns arose.
The researchers met following the independent coding of every transcript to discuss and come to a consensus on any disagreements. An iterative approach was used in which the researchers revisited previously analyzed interviews when changes to the codebook were made to assure that the most up-to-date coding scheme was systematically applied to the entire data set. As open coding continued, axial coding (Lune & Berg, 2016) was simultaneously applied to account for higher level themes being generated from the data. This allowed for the organization of lower level codes into hierarchical categorical structures and themes, presented next.
Findings
Several themes generated from the data and presented next are consistent with a syndromal perspective of MI. Unique manifestations of both core and secondary symptoms identified by Jinkerson (2016) emerged as primary themes with the exception of existential/spiritual conflict. Regarding our secondary aim of preliminarily assessing the utility of including staff accounts of patient experiences, analyses revealed significant overlap between descriptions generated by patients and staff members. Moreover, relative to patient accounts, staff members were more likely to discuss contextual factors relating to MI, and it was primarily from staff data that the final primary theme, Factors Influencing MI, was generated. Given the shared themes identified from both staff and patient interviews, results are presented together next.
Core Symptoms
The core MI symptoms queried and endorsed in our investigation included guilt, shame, and loss of trust. While staff reported that witnessing expressions of guilt and shame was not overly common, remorse was often the first feeling discussed by patients. Notably, and consistent with a general understanding of moral emotions, words such as guilt, shame, regret, remorse, and feeling bad were often used interchangeably. To delineate, guilt was coded when participants described remorse that was behavior focused, relating to the consequences of their actions and/or motivating reparative action. Here, guilt was often associated with patients spending a lot of time thinking about their offense and the victims, feeling responsible for their actions, and wishing that they could have acted differently: I [don’t] forgive myself, I still carry that burden on me . . . Every day, I think about it every day. I wish I could turn back the hands of time. . . (Pt 7) Not a day goes by where I’m glad I did what I did . . . The fact that I hurt another person so badly, and living with that is very hard. Knowing I’ve brought a lot of people suffering . . . I don’t know, it makes me sad, and sometimes I cry because of what I’ve done and how I inflicted pain on people. (Pt 1) I felt remorse and stuff, I felt upset, I felt I could have done something different . . . The thought never came to my head to go to [hospital] . . . That’s what I kind of feel bad about. Because it could have been avoided. This whole situation could have been avoided. (Pt 8)
In contrast, shame was described as more self-focused, harder to cope with for patients, and harder to identify for staff. Participants described shame as resulting from both internal and external sources. Internal shame was coded when participants endorsed intense remorse that affected their self-image, made them question their value, and was associated with painful rumination despite attempts to avoid thinking about it. External shame relating to embarrassment and stigma was described by patients and staff as involving fear and doubt about how others would perceive and evaluate their value and was associated with withdrawal and reluctance to discuss the offense with care providers, family, or co-patients: When you think of people ashamed, they are trapped in their shame and it almost paralyzes them to even move forward at all, because they can’t. They’re trapped in their shame. (Staff member) The regret is something that I think of when I wake up, when I go to bed, and all throughout the day, and it kind of eats at me, knowing I did something so heinous toward another person . . . Just living with the regret is probably one of the hardest parts because, for most of my life I thought I wouldn’t be involved in violence . . . I guess I try to hide how I feel a lot of the time by um, just moving on and carrying on with my day, doing what I have to do to get through the day. Until the night, when I remember everything, all the time. So getting through the day is one of the toughest parts, and not just breaking down all of the time. (Pt 1) Well, for the rest of my eternal existence I’m going down as basically, I killed a guy. I have that basically tattooed on me for the rest of my life. (Pt 9) Index offense aside, I think the title “forensic patient” is extremely stigmatizing and induces shame. It’s a shameful title. And that affects a lot, like a lot of patients where we’re at are trying to move forward and get a job, even [name] on our unit, he’s one of our patients who’s conflicted because he’s not motivated and will be like “well I have a criminal record so I’ll never get a job,” so there’s lots of obstacles that they have to go through before even getting out there which is a struggle. (Staff member) Sometimes it’s just like a hopelessness, or a “I did this horrible thing and now I am not a good person,” like that kind of thing. (Pt 3)
Participants also discussed profound loss of trust following an index offense. These feelings were identified by patients and staff as being both self- and other-focused. For example, many participants described the loss of trust NCR individuals experience in themselves, including doubts about their own sanity, their morality or goodness, or their ability to refrain from reoffending in the future: I guess, for a long time I had thought that I was just obviously insane for what I had done, which, is questionable, and I may be, I don’t know. But I think I’m a good person . . . But I don’t know, it just makes me question my own morality and my own judgement. (Pt 1) Some people are sort of quite evidently traumatized by having done something that . . . they consider to be awful, and a few patients who seem really terrified of ever getting in that state again and doing something similar again . . . I sometimes have patients who do not want to make progress . . . they want to stay in hospital, they don’t want to be given too many privileges and they’re sort of fearful of going out into the community again or of having supports reduced. I just recently had a case where we . . . were asking for an absolute discharge from the forensic system and the patient was opposing it . . . and it was sort of driven by this fear that he might get sick again. (Staff member)
In contrast, participants also described the experience of loss of trust in others. These feelings were most frequently associated with perceptions of unjust behavior and betrayal by systems or individuals meant to protect or support. For example, nearly all participants described feelings of betrayal and loss of trust toward family members involved in their arrest and/or toward the forensic system due to perceptions of poor care and unjust confinement (e.g., unreasonably in length or severity) given their NCR verdict: I’m overwhelmed with defeat. The police, the mental health care act, my family, every friend I’ve ever had has debilitated me with denial . . . Every person I’ve ever trusted . . . I don’t feel that I deserve it . . . I’m overwhelmed with the prolonged stay in the system . . . I’ve received zero psychological benefit. (Pt 6) [Patients] feel betrayed by the system, [they] feel that they’ve done “this program” and “this program” and they’ve done everything that the psychiatrist has recommend they do, but yet they find themselves here . . . So they sense “I’ve done all this stuff, I’ve had no positive urine, I’ve done some programs, I’ve done this, but yet still I am getting nothing in return” . . . “I’ve done it, it didn’t get me anywhere, so what’s the point?” (Staff member)
Secondary Symptoms
Secondary MI symptoms queried and described included both emotional and behavioral sequelae resulting from one or more of the primary symptoms. Emotional sequelae described by participants included righteous anger, anxiety, and depression. Anger was most often discussed as resulting from feelings of betrayal and loss of trust for reasons discussed above, for example, perceptions of not being believed and untruthful retellings of index events by psychiatrists: They’re just psychiatrists that spin wild tails and try to spin everything out of proportion and make things worse. . .they can take anything they want, switch it around, make up things, fraud and everything, you know. And say “this never happened,” you know, “I was delusional and crazy,” this and that. (Pt 2) [The patients] are just frustrated with the system mostly. And then they’re just angry. And then by the time I’m trying to have a conversation, they just blow up, because they’re already building inside that they shouldn’t be here or “this is too much.” (Staff member)
Participants also discussed the experience of chronic anxiety and depressive symptoms following index events. Many staff and patient-participants described fears of psychiatric relapse, reoffending, and reincarceration relating to loss of trust in themselves, as well as worry of victim retaliation. Anxiety and depressive symptoms (intense feelings of sadness, worthlessness, rumination, etc.) were also frequently discussed by participants and attributed to uncertainty and hopelessness around the duration or severity of hospitalization, which was often exacerbated by the lack of trust and transparency within the forensic system: By bringing violence to the table I made it worse . . . [I felt] a lot of anxiety after I had attacked him because I thought he might come back for revenge . . . That he’ll take retribution on me or my family, for what I did to him . . . that brings fear, anxiety into the core of my soul. (Pt 1) My hope has been diminished. This institution has literally destroyed my hope for the future. And uh, I’ve come to a point where I’ve accepted the fact that I’m going to be associated with this institution for the rest of my life . . . I’ve lost all hope. (Pt 6)
Participants also identified several behavioral sequelae consistent with MI and resulting from the emotional consequences of the index offense. Most notably, participants identified social problems relating to internal and external experiences of shame and a loss of trust in others. Here, participants identified problems initiating new social relationships and maintaining existing ones, often due to fear of judgment and feelings of distrust, betrayal, and anger: . . . you can’t tell somebody, just like “you killed your dad” . . . they’re going to judge you before they even know you . . . It’s very hard to have a relationship in this hospital. Because they just think “why are you in the nuthouse?” (Pt 7) There’s a lack of trust. I feel I have a hard time opening up or elaborating to new friends or, or, associating with new people or letting people into my life. And this goes as deep as my family who has left me in denial (Pt 6) I think you see a decline in relationships they have prior to the index offense. Because they’re not the person that they were when they committed the crime, so I think it might be the shame and embarrassment of facing these family members when you thought you could never do something like this and all of a sudden you did. So, I think pulling away from those relationships is, at the time, the only thing that they can really do. (Staff member)
Reexperiencing and self-harm were also identified as common behavioral sequelae resulting from moral pain. Patients described struggling with unwanted and intrusive thoughts, memories, and dreams precipitated by intense feelings of shame. As a result, participants described witnessing or engaging in suicidal ideation and self-harm behavior—most notably substance abuse—as a strategy to cope with painful experiences of shame, rumination, sadness, and hopelessness: Well, that’s why I used for so long, used like the methamphetamine and the heroine and speedballing every day after the index offense because I couldn’t deal with what I had done. So I tried to numb how I felt all the time, with using the speedball intravenously, that alleviated how I felt, and I felt numb, so I felt nothing, which was better than feeling what I had done. (Pt 1)
Factor Influencing MI Symptomology
Discussed primarily by staff, factors affecting the propensity to experience moral pain emerged as a final theme and included index offense severity, patient relation to victim, and patient level of insight. Here, patients who commit more serious offenses involving violence—and particularly those involving loved ones—are more likely to demonstrate symptoms consistent with MI. Regarding insight, multiple staff noted that patients without insight into the events surrounding their index offense are more likely to demonstrate other focused MI symptoms, for example, intense anger around the discrepancy between a patient’s account of their offense and formal police or medical records. In contrast, staff described patients who experience a reduction in psychiatric symptoms and regain insight into the index events as more likely to demonstrate the self-conscious moral emotions associated with MI, such as guilt and shame: I think as they begin to get well—because often they enter the hospital quite unwell—so, as they become medicated and realize the gravity of what has happened and why they’re like this, there’s a lot of guilt and shame and negativity around it. Emotional distress. (Staff member) The anger usually stems from their lack of understanding because of their lack of insight. They don’t have an understanding of why they’re here, why they’re being held here, why they can’t leave, and they don’t understand that they need to be treated . . . But just the anger of them being kept here. (Staff member)
Finally, staff noted that the experience of moral pain is dimensional and that not all patients who endorse negative moral emotions are at risk of other symptoms of MI. Here, staff noted that in some cases, expression of emotions like guilt and shame may be indicators of recovery and intentionally targeted as a treatment objective. However, numerous staff agreed that when moral pain is profound, persistent, and pervasive, and when patients are not able to find healthy ways to cope with their emotions, moral pain can become detrimental to healthy functioning and recovery and potentially be indicative of MI: I can think of another patient who I don’t think this gentleman’s dealing with his guilt and shame, and he’s completely reclusive to his room, he doesn’t go out, so I think that is impeding his recovery. So of course we want him to understand what we did is wrong, but when it gets to a point where these emotions are completely taking over and stopping him from being able to engage in the reason he’s here, then that’s really going to impede him from being able to recover and get back into the community. (Staff member)
Reflective Statement
The staff members and patients who volunteered to be interviewed for the study were enthusiastic to participate and offer their opinions. Several patients, in particular, described feelings of catharsis while being able to speak freely and openly about their experiences without feeling judged or scrutinized. While patients were, at times, initially hesitant to speak in detail about their offense or some of the more painful moral emotions that arose in consequence, patients appeared to relax over time and were noted to elaborate increasingly with the realization that the interviewer was accepting their experiences as valid. A final reflective observation surrounds the overlap between patient experiences and staff members’ understanding of those experiences. While almost all patients endorsed feelings of guilt and/or shame to some degree, some staff were initially hesitant to identify these emotions in their patients. However, as interviews with staff progressed and emotional presentations were reframed behaviorally (e.g., patients becoming withdrawn or angry when asked about their offense may be experiencing shame), staff were more readily able to reflect on and identify the potential impact of moral emotions that was being described by patients in their interviews. Overall, the staff’s observations and accounts of patient experiences were consistent with patient reports in a way that complemented and aided in the interpretation of data derived from patients.
Discussion
The current study aimed to investigate the moral emotional experiences of individuals found NCR for symptoms consistent with MI and to explore the utility of including staff accounts of patient experiences in doing so. Integrating top-down and bottom-up approaches to data analysis resulted in the emergence of several themes highlighting the relevance of MI to justice-involved individuals found NCR.
Notably, using a syndromal framework of MI to guide our investigation provided preliminary evidence that both core and secondary MI symptoms are also pertinent to forensic psychiatry. Theoretical and empirical studies of MI have described it as including impairing moral emotions (guilt, shame, and anger), negative appraisals of self and others, behavioral problems (withdrawal and self-harm), and symptoms of anxiety and depression (Currier et al., 2017; Jinkerson, 2016; Litz et al., 2009; Nickerson et al., 2018; Yeterian et al., 2019); our results are the first to demonstrate similar findings for justice-involved individuals found NCR resulting from the moral pain associated with the commission of a criminal offense.
Consistent with traditional definitions of MI that distinguish between experiences of moral perpetrations (via commission or omission) and moral betrayals, our findings suggest that a symptom-based perspective can be used to capture the consequences associated with both types of moral violation. For example, paralleling existing work demonstrating the relation between the commission of perceived immoral acts and intense moral pain, individuals found NCR described profound guilt, shame, remorse, and regret relating to their offense as well as self-directed anger, a loss of trust in one’s morality, increased substance use as a means of coping, and suicidality. It is important to note that as participants were not required to disclose the specific details of their index offense, it is unclear whether these findings can be applied to perpetrated acts of commission, omission, or both; however, we consider this an interesting area for future query. Furthermore, participants also described outwardly directed moral pain, most notably a loss of trust and anger toward the forensic system, friends, and family—experiences more in line with perceived moral betrayals. Interestingly, existential/spiritual conflict was the only symptom outlined by Jinkerson (2016) that did not emerge as a significant theme from our data; given the preliminary nature of our investigation, it is unclear whether this discrepancy reflects a distinct aspect of MI in forensic psychiatry or simply a product of our study design characteristics. To our knowledge, this study is the first to employ a symptom-based definition of MI outside of military contexts to explore its utility across populations and, in doing so, provides preliminary empirical support for the adoption of a syndromal definition of MI for cross-population research.
While our top-down approach highlights how a syndromal framework can be useful in integrating traditional understandings of MI with the experiences of novel populations and lends credibility to the construct as a whole, our data-driven, bottom-up approach allowed for the emergence of symptom manifestations unique to justice-involved individuals found NCR and provides preliminary evidence that core and secondary symptoms of MI could have distinct triggers and consequences for this population. For example, participants described feelings of guilt relating to regret for their actions, concern for the victim, and a desire to make amends throughout treatment and recovery. In contrast, shame was more insidious, harder to identify, and more likely to be associated with secondary symptoms. For example, shame was often discussed as relating to both self- and other-directed anger (e.g., anger at self for committing the offense), suicidality and self-harm (e.g., substance abuse), and social problems (e.g., social avoidance and withdrawal from supports). Unique to this population, participants also described moral pain relating to their experience with the Forensic System. For example, participants reported a loss of trust in their own ability to navigate treatment and recovery and add value to society, as well as significant anger, anxiety, and hopelessness relating to not being believed by loved ones and care providers and to perceptions of an indefinite and unjust sentence length. Moreover, and as described by participating staff members, behavioral presentations commonly observed in forensic settings (privilege violations, substance use, extreme mistrust/anger toward care providers, withdrawal, refusal to discuss details of index events, etc.) may, in fact, be morally relevant and driven in part by negative moral emotions. Although future research is needed to better understand the relation between these behavioral presentations and moral pain, these preliminary results are consistent with existing literature reporting similar findings.
A secondary aim was to explore the utility of including staff accounts of patient experiences. While it is important to note that staff interpretations could never fully capture the private emotional experience of a patient and thus should be considered carefully, our findings suggest that the inclusion of staff accounts both complemented and enriched patient-derived data. This was most apparent in the discussion of factors that might influence the prevalence, type, and severity of MI symptoms. Notably, themes generated from staff interviews highlight the potential role of patient insight in the experience of MI symptomology. Here, our findings suggest that symptoms of MI may differentially present over the course of inpatient stay via the reduction of psychiatric symptoms impeding insight. Although outside the scope of the current study, future research should aim to better understand the ways that other-focused moral emotions like anger (associated with lower insight) and self-conscious moral emotions like shame and guilt (associated with higher insight) are differentially impeding, impacting, or otherwise influencing progress through treatment and recovery. Finally, staff noted that in some cases, expressions of moral pain may be indicative of successful progress through treatment and recovery; however, when moral pain was extreme in intensity and duration, and particularly when the painful experience was focused on “a bad self” rather than “a bad behavior” (indicating primary shame over guilt), staff were more likely to view the experience as maladaptive and related to MI symptomology.
While findings from this study should be considered preliminary, they offer important insight into understanding the role that moral pain may play in offense-related risk and recidivism. Few studies exist that examine moral emotions in offending populations—even fewer within NCR populations—and those that do have primarily focused on experiences of guilt and shame. Most relevant to the findings presented here, the extant psychological research on moral emotions conducted with offending populations suggests that guilt and shame represent overlapping but distinct concepts with differential implications for offending behavior (Hosser et al., 2008; Tangney et al., 2014; Wright et al., 2008; Wright & Gudjonsson, 2007). These studies have found guilt to be consistently negatively associated with measures of criminal risk such as psychopathy, anger and violence, levels of antisocial personality, criminogenic cognitions, and risk of recidivism (Tangney et al., 2011, 2014). Shame, in contrast, has been found to be either positively or negligibly related to the same criminogenic factors and instead predictive of a failure to accept responsibility and externalize blame (Tangney et al., 2014). These studies suggest that while guilt may be protective against criminal behavior, shame does not offer the same protection and may increase the likelihood of antisocial behavior. These relations held true for offending populations, including perpetrators of white-collar crimes, first-time incarcerated youth, and one study involving forensic psychiatric inpatients (Hosser et al., 2008; Murphy & Harris, 2007; Wright et al., 2008). Taken together with our findings, it is plausible that intense shame (rather than guilt) is the MI symptom most relevant to forensic populations with the strongest implications for maladaptive behavioral and emotional experiences like anger, avoidance, withdrawal, and substance abuse. It is important to keep in mind, however, that the vast majority of this research has examined trait levels of moral emotions rather than an individual’s experience of moral pain resulting directly from their offense.
As such, future research must examine not only the individual impact of moral emotions like guilt or shame but how the clustering of emotional symptoms into a syndrome like MI might influence an offending individual’s progress through treatment and recovery and future risk of recidivism. To date, no tools exist to measure MI in offending populations, nor do any MI scales in use attempt to measure the unique contributions of its symptoms (e.g., anger vs. guilt vs. shame); this may be particularly important in forensic psychiatry where these emotions may differentially interact with factors like patient insight and have different implications for offending behavior.
The current study provides novel insight into the moral pain experienced by justice-involved individuals found NCR. While our findings provide the first empirical evidence for MI in this population and lay the foundation for future work in the area, interpretations must be made in light of certain limitations. First, participants were recruited from a single site with purposeful and convenient sampling and the patient sample included primarily White, male-identifying individuals. While purposeful sampling is often advantageous for qualitative investigations, it limits the generalizability of our results to other NCR individuals or other justice-involved individuals not under the NCR provision. This is a particularly important consideration for future investigation given the relative paucity of research focusing on diverse offending populations, for example, women who offend. The National Trajectory Project of Individuals Found Not Criminally Responsible on Account of Mental Disorder found that relative to men, women who offend had substantially more offenses causing (or attempting to cause) death and were more likely to commit offenses involving a loved one (Nicholls et al., 2015). Although existing investigations into military-related MI have not found significant sex differences (Kelley et al., 2019), the findings from the National Trajectory Project taken together with our results suggest that women who offend may be particularly susceptible to symptoms of MI and should be the focus of future work in this area.
A second methodological limitation of the current study involved the use of self-selection by respondents, which may have limited our findings as those most impacted by morally injurious symptoms (e.g., shame) may be least likely to consent to participate in interviews about emotional experiences. This was reflected in the relatively small number of patient-participants and limited the depth at which we could speak to each theme. This last limitation was somewhat expected and compensated for by the recruitment of several staff participants with expertise in forensic psychiatry who were able to offer their own nuanced accounts of patient emotional processes and behavioral observations. Despite its limitations, this design ultimately helped strengthen the analysis by allowing for data and method triangulation through the use of multiple data collection strategies and resulted in the emergence of themes that may have otherwise been missed. Consolidating patient and health care provider accounts of the emotional processes impacting forensic psychiatric patients stands as a unique contribution to an area of research that is already too often neglected.
Conclusion
Moral emotions are strong drivers of behavior and must be understood as part of a constellation of factors influencing criminality, risk, and recovery. Results from the current study provide preliminary insight into an often-overlooked area of research, allowing for a more nuanced understanding of the moral emotional experiences of NCR individuals and laying the foundation for future studies to measure MI in forensic psychiatry and more deeply characterize its impact on an individual’s progress through treatment and recovery. Beyond the realm of forensic psychiatry, this work has important implications for the emerging field of MI and the methodological choices used to study it. Our findings offer support for the integration of traditional theoretical understandings of MI with novel outcome-focused perspectives. This approach will be instrumental in driving the field forward beyond the military arena and into the many contexts where insight into moral pain will add to our understanding of mental health and social behavior more broadly.
Footnotes
Appendix
Authors’ Note:
First, we would like to sincerely thank the patients and staff members who volunteered to share their experiences with us. In addition, we would like to thank the following individuals for their contributions to the project and manuscript development: Andrea Brown, Heather Millman, and David Streiner. This study was supported in part by an award from the Forensic Psychiatry Program at St. Joseph’s Healthcare Hamilton and by Canadian Institutes of Health Research (CIHR) grants to Margaret C. McKinnon and Ruth A. Lanius. Margaret C. McKinnon is supported by the Homewood Chair in Mental Health and Trauma at McMaster University. Ruth A. Lanius is supported by the Harris-Woodman Chair in Psyche and Soma at Western University.