
Abstract
This paper describes the quantitative findings of a systematic literature review of research on patients on conditional discharge from forensic mental health services in England and Wales (part one of two). Conditional discharge is a frequently used discharge option which allows forensic patients to receive care within the community, while subject to certain restrictions. In total, 23 quantitative and five mixed-methods studies were included. A synthesis of the quantitative findings identified factors associated with recall and recidivism, as well as positive outcomes for patients. Patients on conditional discharge showed lower violence and recidivism rates compared to those on absolute discharge. We develop hypothesized causal links between predictors and patient outcomes using a novel method of directed acyclic graphs (DAGs). The methods of this review, implications of findings, and directions for further research are discussed.
Plain Language Summary
Background In England and Wales, over 3,000 people with serious mental health conditions who have previously caused harm or committed crimes leave secure hospitals under “conditional discharge.” This means they live in the community under rules—like taking medication or living in a set place—while being supervised by a doctor and social worker. If they break the rules or safety concerns arise, they can be returned to hospital. Until now, no one had reviewed all the quantitative (number-based) research on what helps them stay well and safe. Aims and Purpose We aimed to bring together all quantitative research on people under conditional discharge in England and Wales to answer three questions: – What helps people do well (e.g., stay well or be fully discharged)? – What increases the risk of things going wrong (e.g., hospital readmission or reoffending)? – How often do studies examine factors like age, gender, ethnicity, or disability? Methods We searched multiple research databases for quantitative studies since 1983 and summarised the results to combine findings from diverse sources. We also used diagrams to map links between factors like age, diagnosis, and hospital recall or reoffending. We included 23 quantitative and 5 mixed-methods studies. Results Most people on conditional discharge were single men, around age 40, with serious mental illness and a history of violence. Doing well was linked to being older, female, having a mental illness (like schizophrenia rather than a personality disorder), and living in supported housing. Being sent back to hospital was more likely for those who were younger, from non-White backgrounds, had substance use problems, or did not engage with treatment. Why it matters This review showed some clear patterns but also gaps, especially around what helps people succeed, not just avoid failure. The findings can help shape future research and guide policy and practice. Research should focus more on patient strengths a
Introduction
Inpatient secure forensic mental health services provide care and treatment to people who are living with a serious mental illness, have been involved in offending or harmful behaviour, and are deemed at risk of harm to themselves or others. These services are highly restrictive, resource-intensive, and can significantly curtail patient liberty and meaningful interaction with the wider community for significant periods of time (Völlm et al., 2016). Accordingly, an aim of forensic services is to support patients’ progress towards being discharged into the community as soon as is clinically appropriate, safe and practicable.
Conditional discharge is a commonly used discharge option in England and Wales. This discharge involves community care for patients, with the potential for the Secretary of State to recall a patient if the nature of their disorder warrants detention in hospital and this is deemed necessary for the protection of others under the Mental Health Act 1983 (Ministry of Justice, 2009). Conditions of discharge may include: taking medication, living at a specific residence, not contacting victims, or not entering certain geographical areas. Patients on conditional discharge are typically supervised by a psychiatrist and social worker (HM Prison and Probation Service, 2011). An absolute discharge is issued when it is deemed that the patient no longer meets the statutory criteria for detainment, and it is no longer appropriate for the patient to be liable for recall (HM Prison and Probation Service, 2017).
Discharge can be ordered by the Secretary of State for Justice or a Mental Health Tribunal. The number of restricted patients on conditional discharge has been increasing since 2013 and exceeds the number given an absolute discharge (Ministry of Justice, 2023). In 2021, 540 patients in secure care were conditionally discharged by the Secretary of State or a tribunal, four were given an absolute discharge (Ministry of Justice, 2023). On 31 December 2023, there were 3,185 conditionally discharged restricted forensic mental health patients; that is, patients who were receiving treatment in forensic settings under, for example, section 37/41 MHA 1983 (Ministry of Justice, 2024). This combined section 37/41 is a hospital order with additional legal restrictions imposed by the Ministry of Justice.
Conditional discharge represents an important phase in a patient’s individual recovery journey. It is an important consideration in the forensic mental health system’s capacity to manage caseloads and resources, and provide care in the least restrictive environment possible. Several studies have sought to better understand the outcomes and experiences of conditionally discharged patients, most typically to explore factors associated with recall to hospital (e.g., Jewell et al., 2018). However, despite the significant legal, clinical and social implications that a conditional discharge brings, no systematic review of the research has been conducted to our knowledge. Additionally, a recent report on forensic social work commissioned by Health Education England concluded that there is a need to establish a nationally recognized training framework for social supervisors working with conditionally discharged patients (Daly, 2020). This review was conducted to inform the development of ‘Social supervision and conditional discharge’ online training module hosted by Health Education England in light of this need.
Aim and Research Questions
This systematic review aims to fill a clear gap in knowledge by summarising the existing research on the conditionally discharged forensic mental health patient population in England and Wales. This paper will focus specifically on the quantitative findings of the review, addressing the following research questions:
Which factors have been associated with (a) positive outcomes (e.g., absolute discharge, good psychosocial outcomes), and (b) negative outcomes (e.g., reoffending or aggression, recall to hospital) in this population? To what extent are protected characteristics addressed in these studies?
Method
The reporting of the review follows the PRISMA guidelines (Page et al., 2021). Publications were synthesized and summarized according to the narrative synthesis approach (Centre for Reviews and Dissemination, 2009). This involves ‘the adoption of a textual approach that provides an analysis of the relationships within and between studies and an overall assessment of the robustness of the evidence’ (Centre for Reviews and Dissemination, 2009: 48). The PROSPERO registration code for this review is: CRD42022343632.
Search Strategy
The following search terms were used: ((psych* or mental*) AND (forensic* or secur* or ‘special hospital*’) AND (conditional* or discharge* or release* or supervi*) AND (England or Wales or English or Welsh or UK or U.K. or ‘United Kingdom’)).
The following databases were included in the review: PubMed; Web of Science; Scopus; PsycINFO; MEDLINE; Cochrane Library; Google scholar (first 10 pages); Google search (first 10 pages); the references of included articles were scanned to identify further studies.
The following search parameters were set: the time limit includes all publications published from 1983 to the date of the search. This date was chosen so as to include studies conducted after the introduction of the Mental Health Act 1983. All publications were published in English. Only studies of services in England and Wales were included.
Empirical qualitative and quantitative studies were included. There were no limits on study design (e.g., cohort, retrospective, quasi-experimental, case study, interview). All databases were initially searched on 29/07/2022, with the exception of MEDLINE and PsychINFO, which were searched on 11/08/2022. Updated searches were conducted on 14/09/2023 and 11/03/2025 to identify studies published during the review period (see Figures 1 and 2).
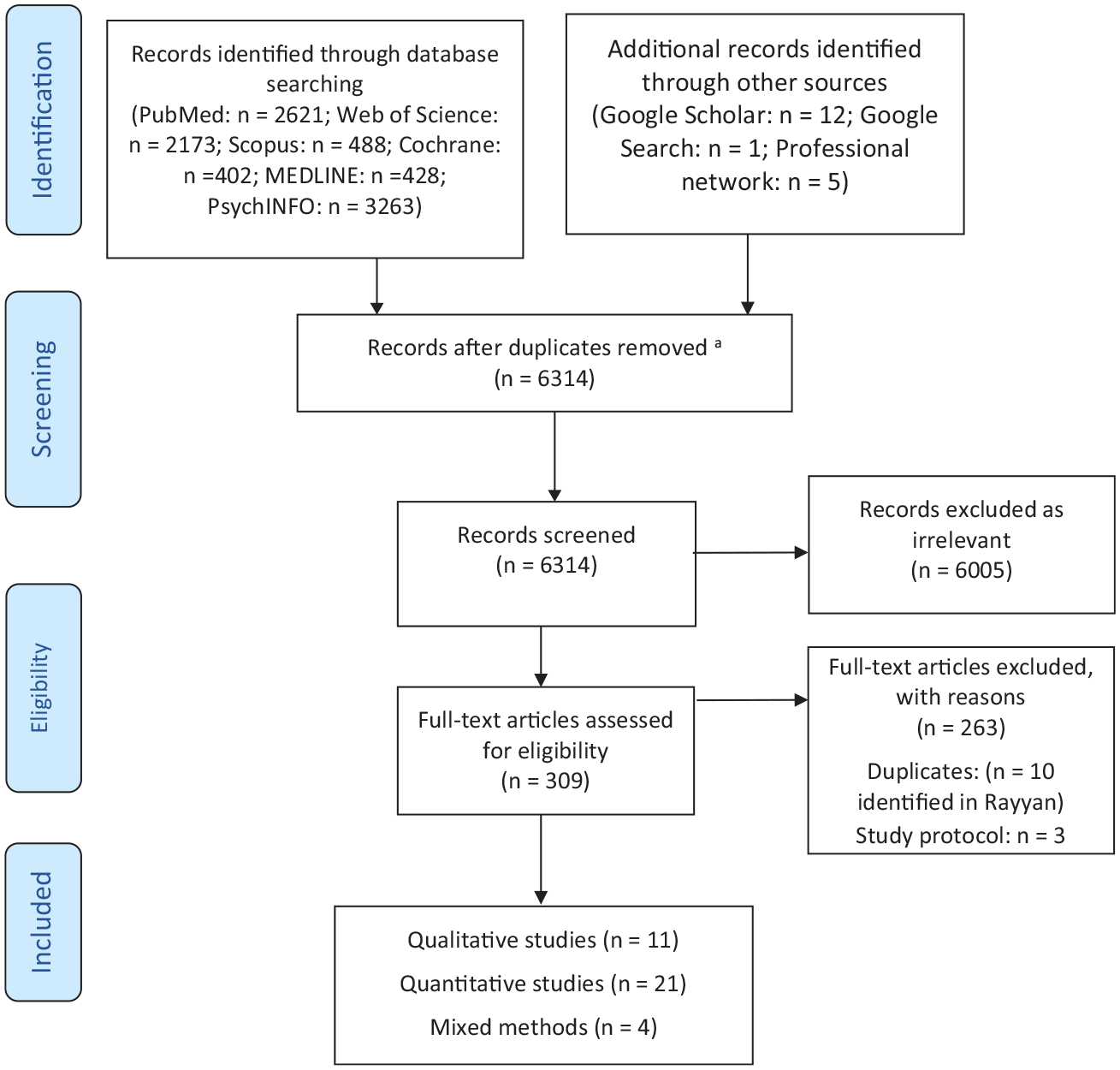
Study flow diagram using the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) template First Search.
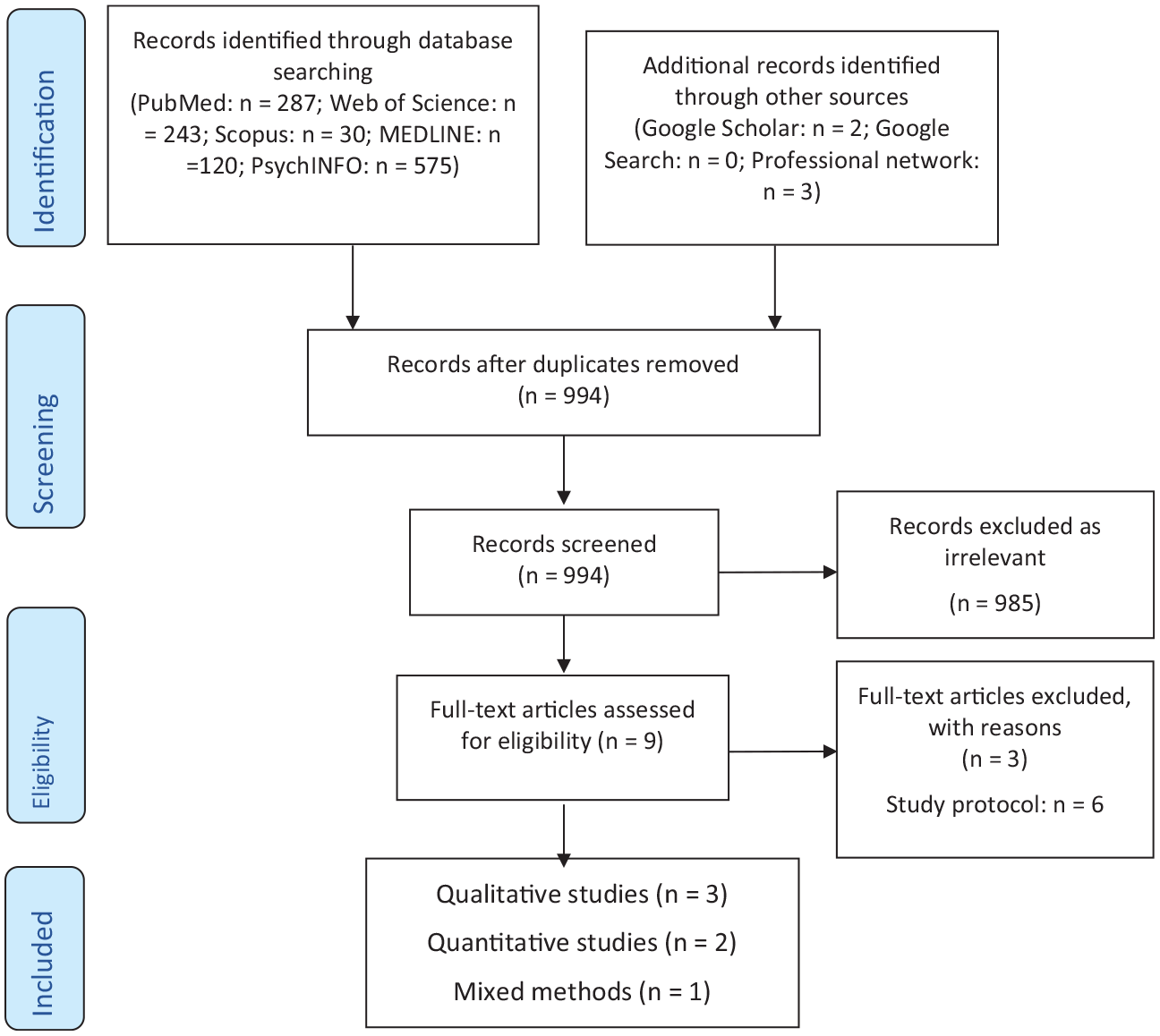
Study flow diagram using the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) template Updated Search.
PICOS
Population
Forensic mental health patients conditionally discharged under the Mental Health Act 1983 in England and Wales. We include patients who are about to be conditionally discharged or who have been recalled after a period of conditional discharge.
Intervention
Patients in this population receive social support, alongside mental health and physical health care, typically supervised by a psychiatrist and a social worker.
Comparison Group
Outcomes and profiles of patients on conditional discharge when compared to patients given other discharges/transfers, for example, absolute discharges, transfer to prison.
Outcomes
Outcomes include the lived experiences of conditionally discharged patients; mental and physical health outcomes; readmission to psychiatric hospital; reoffending, defined as official reconvictions and self-report offending; reasons for recall following conditional discharge. This list is not exhaustive.
Setting
All patients conditionally discharged into the community. Some patients may have been recalled to hospital at the time of the study or were about to be conditionally discharged.
Inclusion Criteria
Inclusion. 1
Studies with empirical data (qualitative or quantitative); studies of, or including, patients who are on, or who have previously been on, or are about to be conditionally discharged from secure psychiatric care; and studies in England and/or Wales.
Data Extraction
The studies retrieved during the searches were stored in the reference management software Rayyan and were screened for relevance by two research assistants (MZ and AR). Those identified as being potentially eligible were judged against the inclusion criteria. Study data were then extracted and recorded in a summary table (available as a supplement). These data included: authors, year of publication, aim/purpose, population and sample size, study design, follow-up, and key study findings.
The research assistants extracted data from 50% of publications each and then checked the accuracy of the other’s work. JT, SK, MJ and ST reviewed 25% of the papers each for inter-rater reliability. JT and SK then reviewed data extraction for a final time. Findings were subject to discussion, with any discrepancies resolved through team dialogue. SK and JT conducted data extraction for all papers in the updated search.
Quality Assessment
Studies were assessed for their quality and risk of bias using quality assessment tools from the Joanna Briggs Institute family of critical appraisal tools. Quality assessment was conducted by two research assistants under the supervision of JT, SK, MJ and ST. Doublechecking of work and inter-rater reliability checks were carried out as for data extraction.
Data Synthesis
Findings were inputted into the study data extraction spreadsheet described above and then combined and presented according to topic following the narrative synthesis method (e.g., factors associated with recall, demographics, etc.).
Directed Acyclic Graphs
In order to further synthesise quantitative findings, directed acyclic graphs (or DAGs) were created for the papers included in this review. DAGs offer a graphical representation of exposures and outcomes, and can be helpful in synthesising information in systemic reviews and creating proposed causal models (e.g. Mathlin et al, 2022). This method was chosen given the heterogeneity of the data across studies, which made more complex statistical analyses for comparing data impractical (see limitations for further discussion).
In creating DAGs, an arrow is drawn between a study’s exposure and outcome variables, implying a possible causal effect. Bidirectional arrows are subsequently drawn between all exposures in a process referred to as ‘saturation’, with individual arrows then removed if no causal relationship is possible. For example, arrows could be removed if the proposed effect preceded the cause in time (temporality), if the relationship is implausible (face-validity), if the relationship is atheoretical (recourse to theory), or if the relationship fails a counterfactual thought experiment (Ferguson et al., 2020). In DAG creation, removing such an arrow – and thus stating no causal relationship may be present – is a stronger assertion than including the arrow (Ferguson et al., 2020). Additional control and mediating variables are then added to the DAG, allowing these models to aid in the identification of potential causal variables for the outcomes in question.
For this review, DAGs were created for results from individual papers by following the methods suggested by Ferguson et al. (2020) and Tennant et al. (2021). A DAG was not created for a study included in this review if results were purely descriptive, or if outcomes could not be identified for conditionally discharged patients specifically. Individual DAGs were then integrated based on outcome variables, with relationships included if they had been found in at least two separate studies (as in the work of Mathlin et al., 2022). These final integrated DAGs incorporated results from the following studies: Akram (2018); Bailey and Macculloch (1992a); Bailey and Macculloch (1992b); Doyle, Archer-Power, et al. (2014); Doyle et al. (2021); Harrison and Alves-Costa (2022); Hill et al. (2024); Jamieson et al. (2000); Jewell et al. (2018); McCarthy et al. (2001); Mohan, Murray, et al. (1998); Petch (1996); Riordan, Haque, and Humphreys (2006); Sahota et al. (2009); and Steels et al. (1998). DAGs were created using the DAGitty online platform (dagitty.net/dags.html; Textor et al., 2016).
Results
Overview
The results of the first and updated database searches are depicted in Figures 1 and 2. N = 6,314 publications were identified after our initial search, with N = 994 additional publications in our updated search. After deduplication, screening, and full text search in accordance with our inclusion criteria, N = 42 publications were included in the review. Some publications had an overt focus on this population, while others dedicated a single sentence to the conditionally discharged population. Publications ranged from 1984 to 2025. The majority were quantitative (N = 23), with five using mixed methods, and the remaining using qualitative methods (N = 15); the latter were not included in the current analysis (see Tomlin et al., 2025). Five of the publications were dissertations.
Of the quantitative and mixed methods studies, the most common design was retrospective and prospective cohort studies (n = 15) and case series studies (n = 8), followed by questionnaires (n = 3), case reports (n = 1) and case-control designs (n = 1). Individual sample sizes ranged from 11 to 183 conditionally discharged patients. As several different publications made use of the same data, 24 distinct data sets were identified for analysis. Studies were also heterogeneous, covering a variety of research questions, and often considering patients on conditional discharge as a subsample, rather than the focus of the study. The quality of the studies ranged from low to high as reported in Table 1.
Quality Assessment of Papers Using JBI Critical Appraisal Tools.
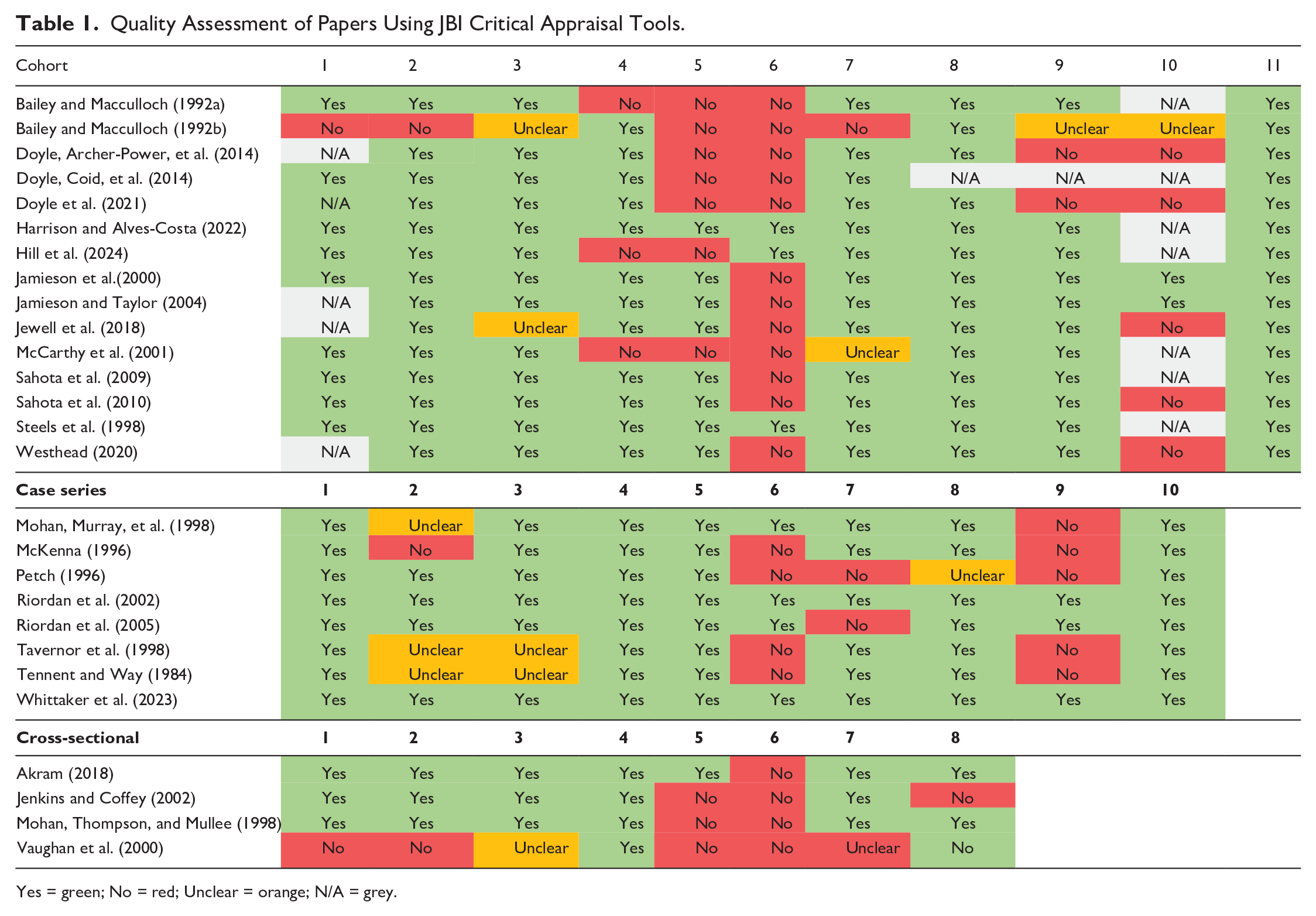
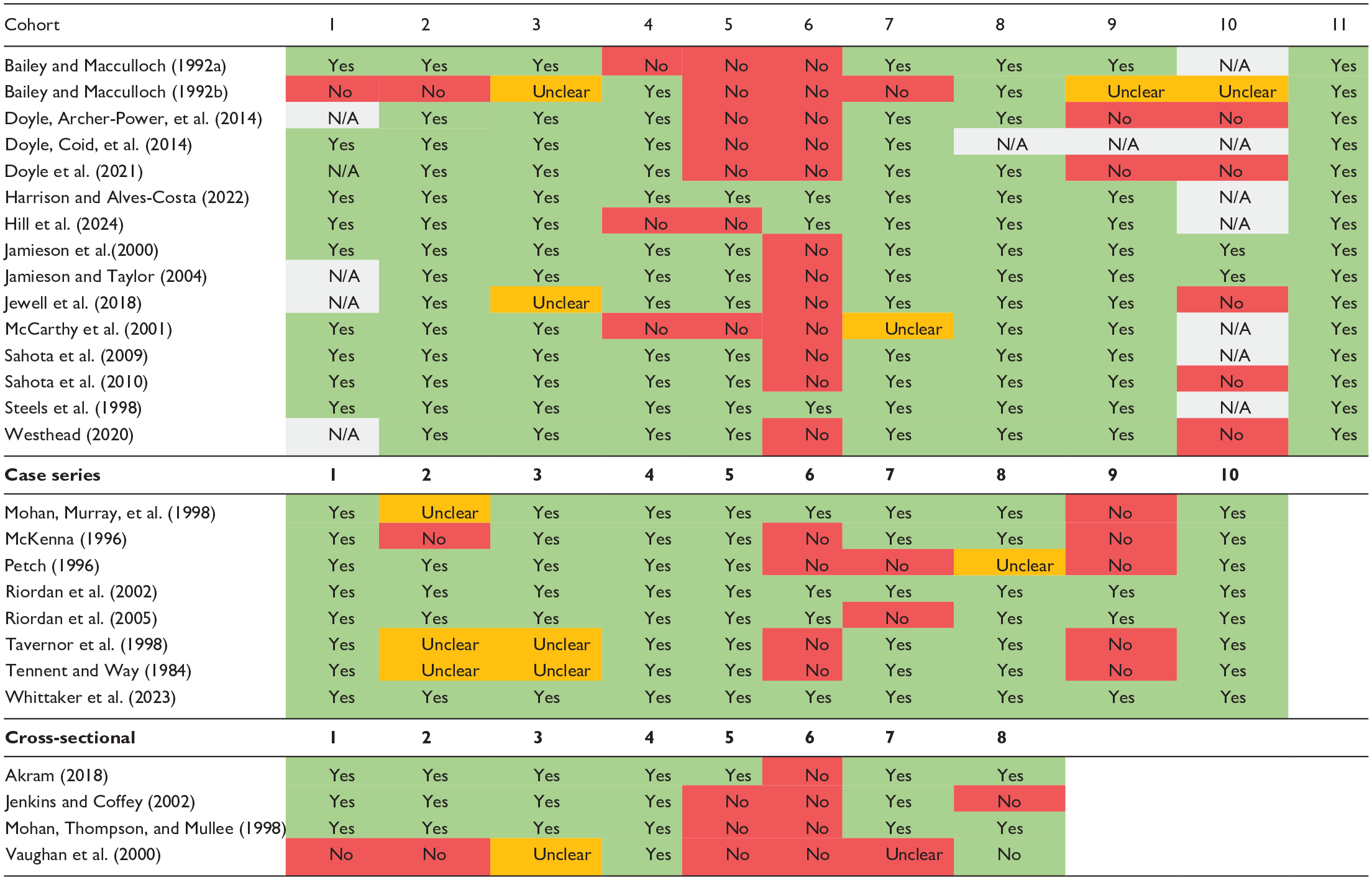
Yes = green; No = red; Unclear = orange; N/A = grey.
Background Factors
Demographics
Conditionally discharged forensic patients were primarily male (82%–89%), single (71%–76%), of non-white ethnicity (71%), unemployed or in ‘unskilled’ work (70%–87%), and with a median age of 40 (Riordan et al., 2002; Steels et al., 1998; Jewell et al., 2018). In a matched sample, Steels et al. (1998) found both men and women with a psychopathic disorder classification to be younger on admission than their counterparts with mental illness (PD men = 25.7 years, MI men = 35.8 years, t = 6.4, p < .0001; PD women = 23.5, MI women = 32.6, t = 2.9, p = .006). Patients from Black ethnic groups were also overrepresented (Riordan et al., 2002).
Mental Health History
Most individuals on conditional discharge (80%) were found to have had contact with psychiatric services prior to their index offence (Riordan et al., 2002). Schizophrenia or schizoaffective disorder was diagnosed for between 86% (Riordan et al, 2002) and 89% of patients (Jewell et al., 2018). Personality disorder diagnosis ranged from 7% (Riordan et al, 2002) to 40% (Jewell et al., 2018); while both studies made use of case notes, this discrepancy may be due to the reporting of a single (presumably primary) diagnosis per patient in the former compared to the inclusion of comorbid diagnoses in the latter. Rates of alcohol misuse (36%), drug-related problems (46%) and self-harm prior to admission (38%) indicate that these issues were not uncommon for those on conditional discharge (Riordan et al, 2002).
Offending History
Seventy-six percent had a history of previous offending, and nearly half (48%) had their first conviction between the ages of 14 and 17 (Riordan et al., 2002). Violent offences (e.g., manslaughter, attempted murder and grievous bodily harm) were common, making up 60% of patient index offences (Riordan et al., 2002). In comparing those on conditional discharge with individuals on absolute discharge, the former group had significantly fewer minor offences prior to admission (Bailey & Macculloch, 1992a). No difference was observed between the two groups when comparing serious offending (Bailey & Macculloch, 1992a).
The Discharge Process
In a sample of patients discharged from 32 medium secure units over a 12-month period, most were conditionally discharged (44%) or subject to a community treatment order (CTO; 29%) (Doyle, Coid, et al., 2014). In a comparison between the groups discharged to prison and into the community, the prison discharge group had more serious index offences, were six times more likely to have a personality disorder diagnosis and scored higher on measures of risk for future offending and symptoms of mental illness (Doyle, Coid, et al., 2014). Patients discharged to the community were twice as likely to have a diagnosis of schizophrenia, and scored higher on a measure of protective factors, particularly on ‘motivation’ (Doyle, Coid, et al., 2014).
Factors Associated with Recall
The studies reviewed found that between 25% (Petch, 1996) to 45% (Jewell et al., 2018) of those on conditional discharge were recalled to hospital at least once, with an average of 500 days (median = 395; range 26–1,970) until first recall (Jewell et al., 2018). No clear difference was identified between recalled and conditionally discharged groups on demographics, offending history, or psychological symptomatology (Akram, 2018). In one sample, 40% of those on conditional discharge were recalled for reasons other than danger to the public (Petch, 1996). Potential reasons for recall also included uncooperative behaviour (particularly in their supported accommodation) and money, family or employment issues (Akram, 2018; Petch 1996). Those with a lack of close social support were found to be 4.8 times more likely to be recalled (Riordan, Haque & Humphreys, 2006). Dangerous, threatening or potentially criminal behaviour and breaches of discharge terms were linked to recall (Akram, 2018; Petch 1996; Jewell et al., 2018).
Demographic Factors
Time to first recall was significantly shorter for patients aged 38 or younger (HR = 1.89; 95% CI = 1.02–3.49; p = .04; Jewell et al., 2018). Additionally, time to recall was also significantly shorter for non-white patients (HR = 3.44; 95% CI = 1.45–8.13; p = .005; Jewell et al., 2018).
Substance Misuse
On conditional discharge, patients using drugs were 6.1 times more likely to be readmitted to hospital (Riordan, Haque & Humphreys, 2006), and cannabis use was significantly more prevalent in those recalled than those who remained on discharge (Akram, 2018). In addition, patients using cannabis and alcohol spent a significantly shorter amount of time in the community (Akram, 2018).
Mental Health
Both deterioration in mental state and non-compliance with medication were linked to recall (Akram, 2018; Petch 1996; Jewell et al., 2018). Being known to mental health services prior to index offence (HR = 3.44; 95% CI = 1.06–11.16; p = .04), past psychiatric admission (HR = 2.44; 95% CI = 1.08–5.52; p = .03) and being on depot antipsychotic medication (HR = 2.17; 95% CI = 1.14–4.11; p = .02) were all associated with a significantly shorter time to first recall (Jewell et al., 2018). Additionally, patients were found to be 9.1 times more likely to be readmitted to hospital if they self-harmed (Riordan, Lewis & Humphreys, 2006).
DAG for Recall and Readmission
In the first integrated DAG constructed, three main exposures were found to play a role on both recall and readmission (see Figure 3). These were substance misuse, deterioration in mental state and service disengagement (including both medication non-compliance and dangerous or concerning behaviour). Both recall and readmission were included as outputs in this model due to their shared relationships with the exposure mentioned above, but also their interplay with one another. All arrows between exposure were retained.
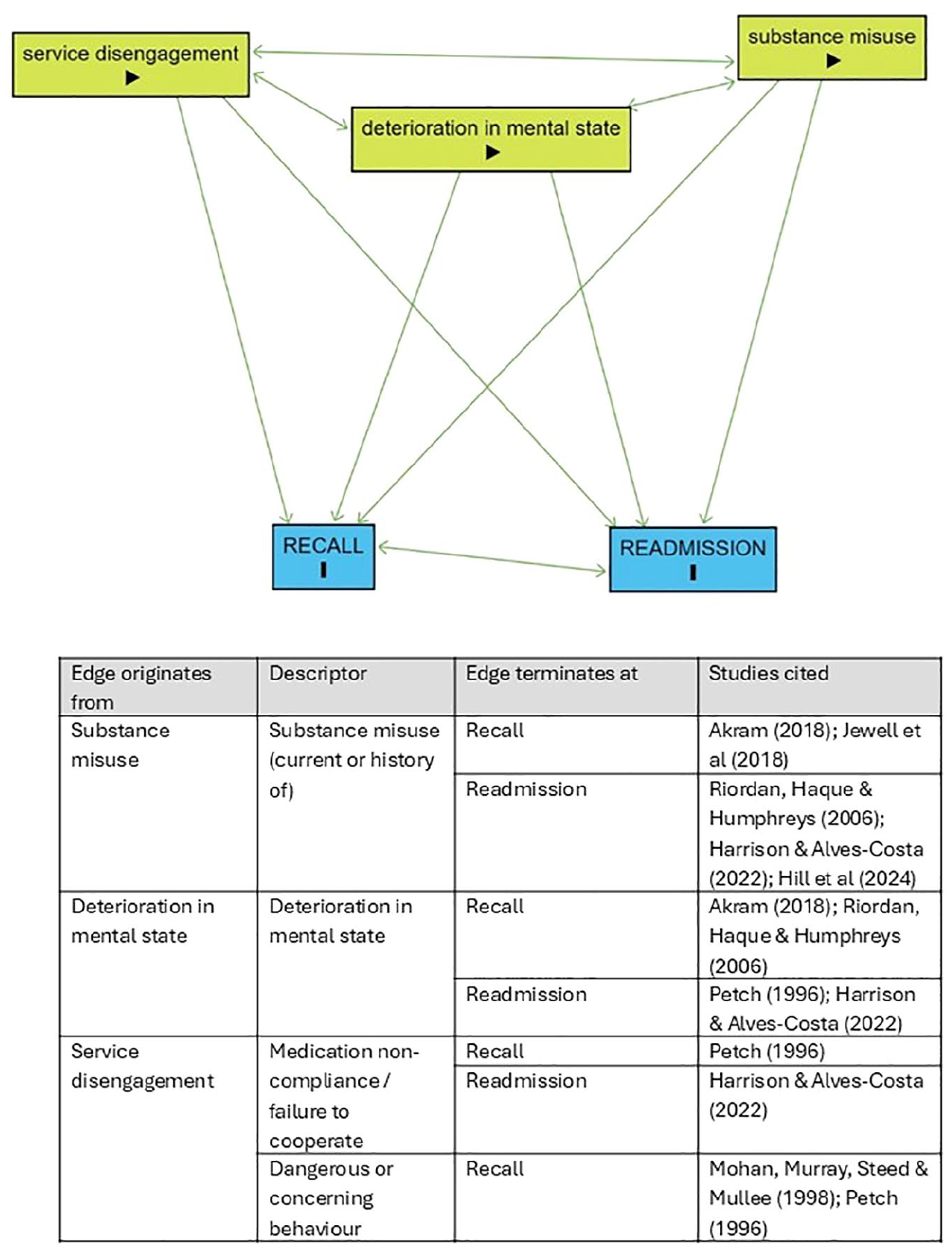
Integrated DAG for recall and readmission outcomes.
Factors Associated with Violence and Recidivism
Conditional discharge was found to be significantly associated with lower rates of post-discharge violence than absolute discharge or other discharges (χ2 = 4.96, p = .026 at 6 months post-discharge), with results increasing in significance over time (χ2 = 9.44, p = .002 at 12 months post-discharge; Doyle, Archer-Power, et al. 2014). Higher HCR-20 V3 scores were associated with higher rates of violence (Doyle, Archer-Power, et al. 2014; Doyle et al., 2021), and a previous conviction on admission was significantly associated with conviction after discharge (χ2 = 11.6, p = .0007; Steels et al., 1998).
Bailey and Macculloch (1992a) found that 27% of individuals on conditional discharge offended after discharge, with the highest rates of reoffending occurring in the first few years of follow-up. However, for patients found guilty of homicide specifically there was little recidivism at the end of the follow-up period, with between 8% and 15% of those discharged from high-security care reoffending (McCarthy et al., 2001).
In comparison to those who have been absolutely discharged, conditional discharge patients were significantly less likely to be convicted (63% vs. 27%; χ2 = 12.61, p = .0007; Bailey & Macculloch, 1992a). When controlling for confounders, patients discharged on a restriction order were significantly less likely to reoffend than those not on a restriction order (Sahota et al, 2010). In addition, higher SAPROF scores and having a longer stay in medium secure care were associated with lower rates of violence (Doyle, Archer-Power, et al. 2014; Doyle et al., 2021).
Age
Younger age on discharge was associated with a higher likelihood of reconviction (p = .0116; Jamieson & Taylor, 2004).
Personality Disorder
Patients with a personality disorder classification were more likely to reoffend than those with a mental illness classification for both conditionally and absolutely discharged groups (Bailey & Macculloch, 1992a). In a matched sample, Steels et al. (1998) found that men with personality disorder on conditional discharge were twice as likely to be convicted and four times more likely (HR = 4.4, 95% CI 1.9–10.8) to be imprisoned than those with mental illness. However, both men and women with a PD classification were more likely to have previous convictions on admission (Steels et al., 1998).
DAG for Recidivism
The second integrated DAG contained the five exposures of age on discharge, duration of admission, previous conviction, having a PD diagnosis, and time spent ‘at risk’ in the community post-discharge (see Figure 4). Absolute discharge (including other community discharges outside of a s.41 of the MHA 1983) was also included as an outcome, although it was noted that non-conditional discharges could also be tied to recidivism. As the reviewed studies used different terminology, the outcome ‘recidivism’ here also contains ‘reoffending’, ‘reconviction’ and ‘imprisonment’, which were combined during the integration stages of DAG construction outlined by Ferguson and colleagues (2020). Arrows between exposures were removed following the steps described previously. For example, the exposures ‘age on discharge’ and ‘PD diagnosis’ could not be caused by time spent at risk in the community, so arrows would be deleted in these cases on the ground of temporality and face-validity.
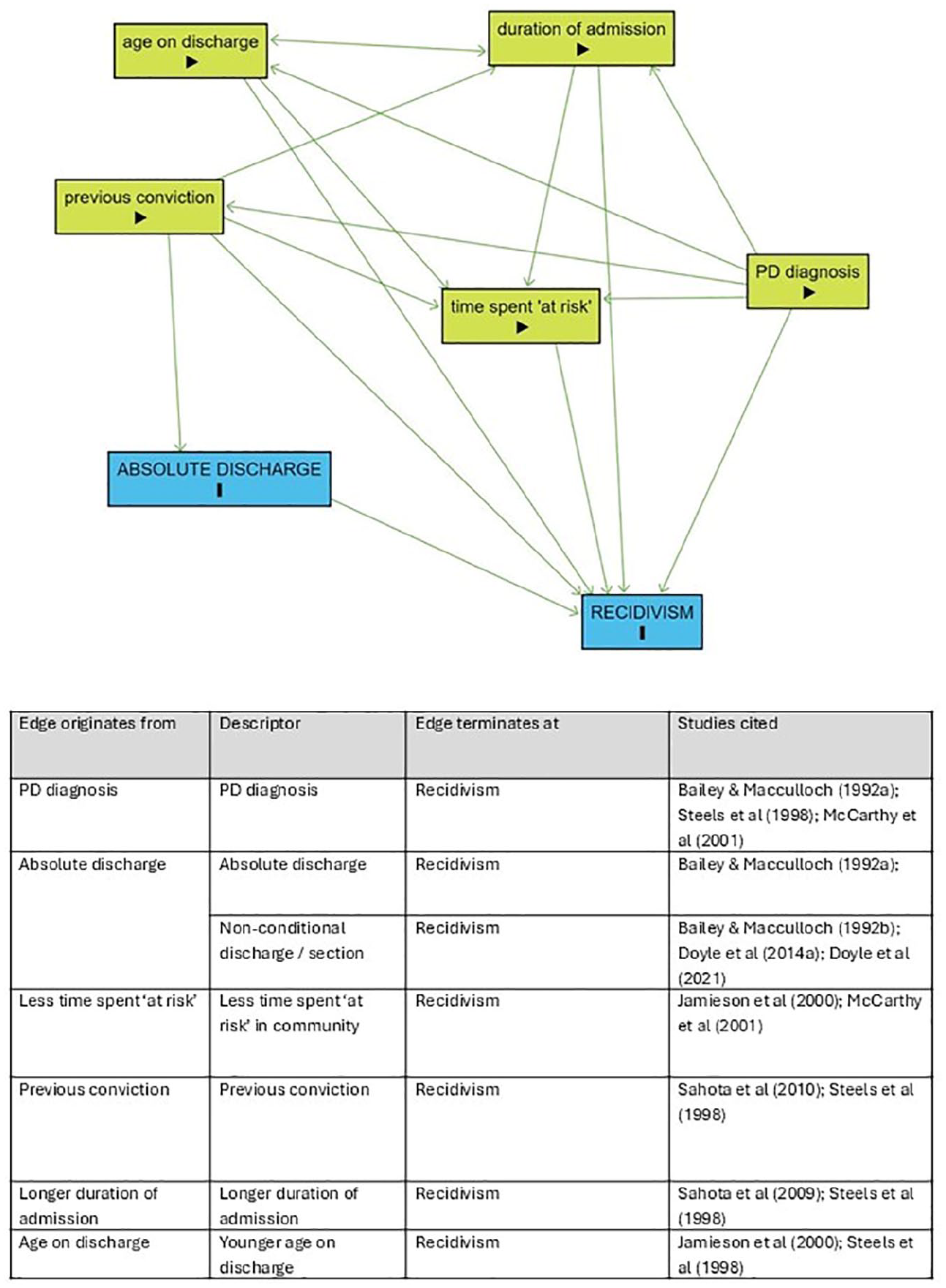
Integrated DAG for recidivism and absolute discharge outcome.
Mortality
In McCarthy et al. (2001), mortality was found to be greater than in the general population, with a rate of 11% over the course of the follow-up. Steels et al. (1998) found a mortality rate of 21% in their sample of individuals discharged from special hospitals, for a standardised mortality rate (SMR) twice that of the general population (SMR = 2.1 for men; SMR = 1.7 for women). This could be due in part to an increase in serious accidents when drugs (4.0× more likely) and alcohol (5.8× more likely) were being misused (Riordan, Lewis & Humphreys, 2006).
Factors Associated with Positive Outcomes
Demographic and Environmental Factors
Gender was not frequently examined given the small number of women on conditional discharge in comparison to men, although it has been found that women tend to have better outcomes overall (Steels et al., 1998). Women were twice as likely as their male counterparts to establish an intimate partnership post-discharge (Steels et al., 1998). However, it should be noted that the quality of such relationships was not taken into consideration.
Men with personality disorder were five times more likely to develop a romantic relationship (HR = 4.9, 95% CI 2.9–8.5) and obtain full-time employment (HR = 5.1, 95% CI 2.3–11.3) than those with a mental illness classification (Steels et al., 1998). Patients in supported accommodation were 4.5 times more likely to be absolutely discharged (Riordan, Haque & Humphreys, 2006).
DAG for Positive Outcomes
Due to a lack of multiple studies with the same findings, no integrated DAG could be created for positive outcomes.
Discussion
This systematic review aimed to identify and synthesize all available quantitative research evidence regarding patients on conditional discharge from forensic mental health services in England and Wales. Research questions also inquired about predictors of positive and negative outcomes for patients, and the relevance of (intersecting) personal characteristics to the conditional discharge process and experience. Some general patterns can be observed from these publications. Most of the earlier publications from the 1980s and 1990s describe studies using archival/hospital records and are mostly descriptive. Over time, quantitative studies increasingly addressed factors that predict outcomes of interest, most frequently recall and reoffending. The quantitative study designs are of mixed quality generally, using predominantly case note and observational cohort designs. Sample sizes tend to be small to medium, and confidence intervals when reported are typically large, indicating low statistical power (though these points are less applicable in more recent publications, that is, since 2010).
The publications in our review found that patients from a Black background were overrepresented and that patients on conditional discharge were mostly male, single, and around 40 years of age on average. A history of serious violent offences was common in this group. They had complex mental health histories, with most reporting previous general or forensic mental health service use. Patients on conditional discharge were more likely to have a mental illness diagnosis than personality disorder diagnosis when compared to patients discharged to prison. Patients with a personality disorder classification were more likely to develop a romantic relationship and obtain full-time employment than patients with a mental illness classification.
Factors linked with violence and offending were similar to those recognised in studies of recidivism in forensic patients globally (e.g. high HCR-20 risk scores, previous convictions, younger age, personality disorder classification; Baudin et al., 2020). Women, older patients, those with a mental illness classification, and patients in supported accommodation were at a lower risk of offending. Of those on conditional discharge, 25% to 45% were recalled to hospital at least once. Most common factors associated with recall were younger age; non-White ethnicity; money, family and employment issues; substance misuse; mental health deterioration and non-compliance with medication; and dangerous or threatening behaviour. Patients on conditional discharge were also less likely to engage in violence or offend than patients on absolute discharge or other discharges.
Several recent studies of factors predicting outcomes for forensic patients after discharge outside England and Wales help contextualise our findings. A study of factors linked with breaches, revocations and hospital readmissions for patients on conditional discharge in New South Wales, Australia, identified four significant predictors in a multivariate analysis: not being in employment or studying at the time of index offence, having a co-morbid substance use diagnosis, having a head injury, and index offences that were not homicide-related (Lyons et al., 2022). Bjørkly et al. (2023) investigated predictors of violence. They found that greater levels of hopelessness, low resilience, and prior criminal convictions were predictive of violence after discharge. This adds importantly to a literature that often focuses on recognised (often static) risk factors; however, as this was a small pilot study with N = 27.
Systematic reviews looking at outcomes for individuals released from prison help us to locate our findings in the wider health and criminal justice spheres. A meta-analysis of the effects of Community Treatment Orders (CTOs) on mental health service use, emergency visits, and violence, found that CTOs were associated with a greater number of service contacts, and lower rates of emergency hospitalisation and violence (Lam et al., 2023). In a recent review of post-release support programmes for incarcerated people who use illicit drugs and have mental illness reported a reduction in further criminal justice involvement in eleven of 13 included studies (Stewart et al., 2022). Programme characteristics linked to more positive outcomes included: earlier and longer implementation post-release, mental health support, housing assistance, financial aid, and group and individual psychological support.
Mathlin et al. (2022) reviewed 34 studies investigating factors associated with successful reintegration for adult males leaving prison. They suggest that few prison visits, witnessing victimization, poor recovery perceptions, the presence of dynamic risk of reoffending, not undertaking in-prison treatment, and poor pre-prison health are causally linked to post-release drug use, negative criminal justice outcomes, housing problems, and post-release mental health difficulties (via different pathways and mediated by barriers to reintegration such as familial conflict, lack of employment, and financial issues).
Limitations
This review has limitations. It is possible that we have missed some relevant literature. To mitigate this, we have conducted and updated a wide-ranging search of relevant databases and sought input from colleagues in the field. It is also possible we have identified literature that includes patients on conditional discharge but have excluded these from our synthesis. This is likely due to the challenges around defining this population and the extent to which authors describe their study samples. Some authors do not distinguish between types of discharge and analyse data for all patients. To ensure we only synthesise data pertaining to patients on conditional discharge, we have excluded studies where the proportion of patients on conditional discharged included in the analysis is not clear or is less than half the sample.
In addition, considerable diversity was observed in the studies reviewed. Some studies looked at discharges rather than individuals, meaning patients appeared more than once in a given sample. Multiple studies also used the same data sets or covered the same region, so that observations were not independent of one another. Samples differed in how they described conditionally discharged patients, making comparisons between subgroups impossible in many cases. Finally, some studies involved the opinions of professionals, rather than conditionally discharged patients themselves. These issues of heterogeneity precluded more advanced statistical analyses from being conducted, as ‘[m]eta-analysis should only be considered when a group of studies is sufficiently homogenous in terms of participants, interventions and outcomes to provide a meaningful summary’ (Deeks et al., 2024, p.17).
Conclusions and Future Research
This systematic review first aimed to identify factors associated with positive and negative outcomes in conditionally discharged forensic patients. Together, the narrative synthesis and DAGs emphasise the importance of service disengagement, deterioration in mental state and substance misuse in the recall and readmission processes. Age, personality disorder diagnosis, duration of admission and time spent ‘at risk’ in the community were found to be associated with recidivism. Importantly, absolute (and other non-conditional) discharges were also found to be associated with reoffending. The DAGs created for this study offer a starting point for future research by suggesting potential causal relationships, while also illustrating existing gaps between predictors and outcomes. A lack of studies focused on positive outcomes precluded the creation of an integrated DAG with such outcomes. As a result, future research should make greater effort to consider protective factors, with an increased focus on positive outcomes for those being discharged into the community.
Additionally, this review aimed to examine past studies’ identification and use of protected characteristics. Results highlighted that insufficient attention has been paid the outcomes and experiences of patients on condition discharge based on gender, sex, ethnic and cultural background, sexual preference, disability, physical health needs, religion and social-economic status. These are either not addressed at all (e.g., sexual preference) or addressed as part of multivariate regression analyses and would benefit from richer qualitative exploration (e.g., ethnicity). Additionally, mortality rates were found to be higher for conditionally discharged patients than the general population. Given that this was only briefly discussed in several of the studies reviewed, more longitudinal studies are needed to examine this increased mortality in more depth.
Supplemental Material
sj-docx-1-ijo-10.1177_0306624X251357615 – Supplemental material for Systematic Review of Forensic Mental Health Patients on Conditional Discharge: Part One – Quantitative Findings, Methodology, Limitations and Future Research
Supplemental material, sj-docx-1-ijo-10.1177_0306624X251357615 for Systematic Review of Forensic Mental Health Patients on Conditional Discharge: Part One – Quantitative Findings, Methodology, Limitations and Future Research by Sarah Kilbane, Maria Zamorano, Alison Romero, Mel Jordan, Shelley Turner and Jack Tomlin in International Journal of Offender Therapy and Comparative Criminology
Footnotes
Acknowledgements
We would like to thank David Cochrane for his support of this work.
Ethical Considerations
As a literature review of publicly accessible data, no ethical issues arose. No formal ethical review was required.
Consent to Participate
As a literature review of publicly accessible data, no consent was required.
Consent for Publication
As a literature review of publicly accessible data, no consent was required for publication.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was funded by Health Education England to assist the New Roles Social Work Group to establish Health Education England e-LfH training on social supervision. Additional support was provided by West London NHS Trust.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
As a literature review of publicly accessible data, data are publicly accessible.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.