
Abstract
This article explores the making and management of anomaly in scientific work, taking ‘medically unexplained symptoms’ (MUS) as its case. MUS is a category used to characterize health conditions that are widely held to be ambiguous, in terms of their nature, causes and treatment. It has been suggested that MUS is a ‘wastebasket diagnosis’. However, although a powerful metaphor, it does neither the category nor the profession justice: Unlike waste in a wastebasket, unexplained symptoms are not discarded but contained, not ejected but managed. Rather than a ‘wastebasket’, I propose that we instead think about it as a ‘junk drawer’. A junk drawer is an ordering device whose function is the containment of things we want to keep but have nowhere else to put. Based on a critical document analysis of the research literature on MUS (107 research articles from 10 medical journals, published 2001–2016), the article explores how the MUS category is constituted and managed as a junk drawer in medical science.
Introduction
In this article I explore the making and management of anomaly in scientific work, taking ‘medically unexplained symptoms’ (MUS) as my case. MUS is a category used to characterize health conditions widely held to be ambiguous in terms of their nature, causes and treatment (O’Leary, 2018). Sometimes referred to as ‘uncertain illness’ (Dumit, 2006), ‘illness without disease’ (Aarseth et al., 2016: 1391), ‘illness that cannot be diagnosed’ (Jutel, 2010: 230) or ‘symptoms that cannot be classified’ (Kornelsen et al., 2016: 367), MUS are known to cause a range of problems for doctors and their patients (Brown, 2007; Czachowski et al., 2011; Shattock et al., 2013). Patients with MUS are highly unpopular, as indicated by medicine’s use of unflattering monikers such as ‘frequent flyers’, ‘thick folder patients’ (Greco, 2012) and ‘heart-sink patients’ (Mathers and Gask, 1995), the latter so called because seeing the patients’ names on the appointment schedule is said to make a doctor’s heart sink (O’Dowd, 1988: 528). Although figures vary, it is generally agreed by researchers to be one of the largest categories of complaints in primary care (Brown, 2007; Greco, 2012; O’Leary, 2018).
The ambiguity of the clinic resonates with the ambiguity in medical science: As noted by members of the medical science community, research into MUS has been plagued by its lack of widely accepted modes of classification (Olde Hartman et al., 2008; Salmon, 2007: 247). The effects of this can be seen, for instance, in the confusingly unclear prevalence rates of MUS consultations in primary care, which have been estimated at 10–15% (Shattock et al., 2013) but also at 20% (Schaefert et al., 2013), 20–30% (Aiarzaguena et al., 2007), 3–39% (Koch et al., 2009) and 25–50% (Olde Hartman et al., 2004). The MUS category thus seemingly applies to anywhere between 3 and 50% of all primary care consultations. Moreover, years of research have not yielded any widely agreed evidence-based treatments, and in some cases (e.g. chronic fatigue syndrome, irritable bowel syndrome and multiple chemical sensitivity), the epistemic status of medical knowledge is loudly contested, often with patient activists and doctors pitted against each other (Aronowitz, 1998; Barker, 2010; Dumit, 2006; Lian and Nettleton, 2015).
In a review of the medical research literature, Jutel (2010) characterized the MUS category as ‘a wastebasket diagnosis’, a metaphor that has been taken up (e.g. Dimsdale et al., 2011). Wastebaskets are effective ordering devices, offering storage for discarded materials. However, although a powerful metaphor, it does neither the category nor the profession justice: Unlike waste in a wastebasket, unexplained symptoms are not discarded but contained, not ejected but managed. Just as patients with MUS are not chucked from the clinic, the category is not jettisoned from the jurisdiction of medical science. In fact, despite the lack of unitary classification, medically unexplained symptoms have become an increasingly hot topic of scientific inquiry. According to Web of Science, 951 research articles that topicalize MUS have been published in English between 1992 (earliest recorded) and 2018, with 5% (N = 47) published in the first 10 years compared to 73% (N = 692) in the last ten. 1 Although the numbers are not necessarily entirely representative, they capture a real surge in scientific activity: Research is booming. Less is known, however, about how medical scientists, given the lack of consensus, actually go about classifying MUS, how the category is understood and used in scientific work. Learning how is the aim of the present article.
To that end, I propose another metaphor. Rather than a wastebasket, I suggest that we think about MUS as a ‘junk drawer’. As I use it here, a junk drawer is a concept, referring to a particular kind of ordering device whose function is the containment of things we want to keep but have nowhere else to put. It frees us from having to leave disorderly things lying about, or from having to put them into neatly ordered drawers where they do not belong. Its job, then, is to help maintain order by containing disorder. Whereas a wastebasket is for getting rid of disorder, a junk drawer is for storage. As such, the latter facilitates future attempts at reordering: for puzzles to be solved or ‘junk’ to be reappraised at a later juncture. 2
In performing its ‘containment function’, a junk drawer also reveals ‘imperfections’ in the system. It does this in two ways. First, in its very establishment and use: A ‘junk drawer category’ is constructed to manage imperfections in the current cultural order that result from a lack of fit with material reality. Thus, the presence of a ‘junk drawer’ is an indication of the mismatch between reality and the classification system with which reality is grasped and wherein the category is embedded. It thus simultaneously expresses our imperfect grasp of reality and our pragmatic capacity to adapt – the more visible the category, the stronger the reminder. Second, systemic imperfections are revealed in the mundane experience with which we are confronted when opening the junk drawer to review the contents. Doing so reminds us that there is an outright mess in the middle of our system. As such, over time a junk drawer can signal the need to tidy, reconfigure and reorder. Omitting to inspect it, on the other hand, can make us forget the mess, deluding us with a pleasant sense of order and control.
In the following, I will provide a detailed examination of how medical scientists make and manage MUS as a ‘junk drawer category’. To that end, I have conducted a critical document analysis of the medical research literature (107 articles published between 2001 and 2016). My questions are: How is the MUS category constituted in research? And how do researchers manage it and its content?
Medical classification
Medicine is replete with formalized classification systems or ‘diagnostic manuals’, notably WHO’s International Classification of Diseases and Health Related Problems (ICD) and the International Classification of Primary Care (ICPC), and the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders (DSM). They provide a shared ‘terminological standard’, allowing for the commensurable codification of experience that renders ‘the world equivalent across cultures, time, and geography’ (Timmermans and Epstein, 2010: 69). Originally designed for statistical purposes, they are now increasingly integrated as a means of communication and coordination within professional work organizations and health insurance schemes and are used across the globe as a tool of accountability by states, hospital managers and other stakeholders (Bowker and Star, 2000; Harrison, 2009; Timmermans and Berg, 2003).
Although the MUS category is obviously medical, it is not a formal diagnosis, nor listed as a category of its own in any of the main diagnostic manuals. It was listed as a criterion for a cluster of diagnoses (somatoform disorders) in the fourth edition of DSM, but was intentionally excluded from the fifth edition, published in 2013 (see American Psychiatric Association, 2013; for criticism see Frances, 2013). Yet medically unexplained symptoms are continually and increasingly the object of clinical research. Paradoxically, then, despite being first partially then completely excluded from the formalized medical classification systems, the MUS category is increasingly enlisted in medical research and is thus steadily becoming a central medical category; it is pushed to the fringe yet drawn towards the centre of medical science. Therefore, rather than symptoms that defy classification (e.g. Kornelsen et al., 2016), MUS could be more appropriately described as subject to routine classification in scientific work. How do scientists do this work when there are no formal or widely accepted classification standards, and how they draw on their existing conventions and classifications in that regard?
Ambiguity and science
I explore the classification of MUS as a case of the larger theme of anomaly in science. A relevant piece of literature in this regard is that of Kuhn (2012). Following Kuhn, phenomena are not anomalous (or ambiguous, deviant, disorderly, strange, etc.) on their own, but within the context of a specific paradigm (an ‘exemplar’ or an accepted ‘problem-solution’ – see Barnes, 1982: 17–19). That is, phenomena are anomalous because they are found to deviate from ‘paradigm-induced expectation’ (Kuhn, 2012: 53), from what reality is supposedly like. This way, knowledge is causally implicated in making phenomena anomalous. It implies a relational perspective, between knowledge and anomaly. When transposed to the case studied here, this suggests that the anomalous character of MUS is the effect of their lack of fit with conventional expectation. Thus, it is against the backdrop of some shared epistemic convention that these symptoms are anomalous.
Anomalies are common in science, and often they are simply ignored (Barnes, 1982; Kuhn, 2012). When an anomaly is recognized as a relevant phenomenon for research, scientists will typically attempt to uncover if the deviation is a result of faulty equipment or some other form of error in the research process (Barnes, 1982). If, after this, the anomaly lingers, different procedures may be applied (e.g. Douglas, 2003: 48–49). Based on a sociological reading of Lakatos (1976), Bloor (1978) distinguishes two such procedures, namely ‘monster-barring’ and ‘monster-adjustment’ (the term ‘monster’ referring to the problematic character of the anomaly). 3 Monster-barring involves techniques for dismissing anomalies (Bloor, 1978: 253), either symbolically or physically. A wastebasket (whether physical or symbolic) is therefore a ‘monster-barring device’ to manage discarded items. Monster-adjustment involves techniques for reinterpreting or altering the anomaly, ensuring its fit with the established order (Bloor, 1978: 254). Some anomalies, however, resist attempts to resolve them and become intractable and annoying (Barnes, 1982; Hacking, 2012; Star, 1985). In these cases, anomalies may turn into crises, fostering changes to the paradigm that made the phenomena anomalous to begin with (Kuhn, 2012).
As I suggest below, MUS are continuously subject to monster-adjustment, yet the procedure has yet to succeed in removing the anomalous character of these symptoms. Learning more about the function of the MUS category may give us some clues about whether it represents a crisis in the making. In the following, I will show the ways scientists make and manage MUS as a ‘junk drawer’, beginning first by outlining the methods employed in this work.
Methods and materials
I analyse a sample of research articles that centrally or peripherally topicalize MUS. The focus is on MUS not as a health problem, but as a category enlisted and investigated by medical research. As the meaning and character of categories are determined in the situated practice of applying them (Barnes, 1982; Bloor, 1997), studying the application of the MUS category is a good way to understand its meaning, use and overall function in medical science. Here, I have studied the traces of the category’s application in the inscriptions found in research articles. Although inscriptions differ from the act of inscribing them, there is much to learn from studying them. Given that research articles as documents (Prior, 2003) are enlisted in systematic reviews, textbooks and procedural and policy guidelines, and have a bearing on the definition of MUS as a health issue and thus the provision of attention and funds in clinical practice and medical research, they are a ‘strategic site’ (Merton, 1987) for the study of scientific classification.
On 26 January 2017, I used Web of Science to search for research articles in English published between 2001 and 2016 with the phrase ‘medically unexplained symptoms’ either in the title, abstract or keywords. 4 2001 has been suggested as the year where MUS went from being a descriptive term to being a research category proper (Nettleton, 2006). The search yielded 753 articles. I limited this initial list to publications in the ten medical journals that had published most frequently on MUS in the period. From these journals, I read the ten most cited articles in each, apart from one in which I read twenty because of its unusually high output. After excluding three articles that did not match the criteria, I had a manageable sample of 107 articles (Table 1). The citation-based sampling procedure is skewed towards earlier publications because they have had more time to amass citations. However, the procedure yields a number of publications from each year and makes it easier to spot systematic changes – if any – in classification practices over time (however, I found no systematic changes). The choice to sample articles from only 10 journals might have introduced some homogeneity to the sample.
Sampled articles.
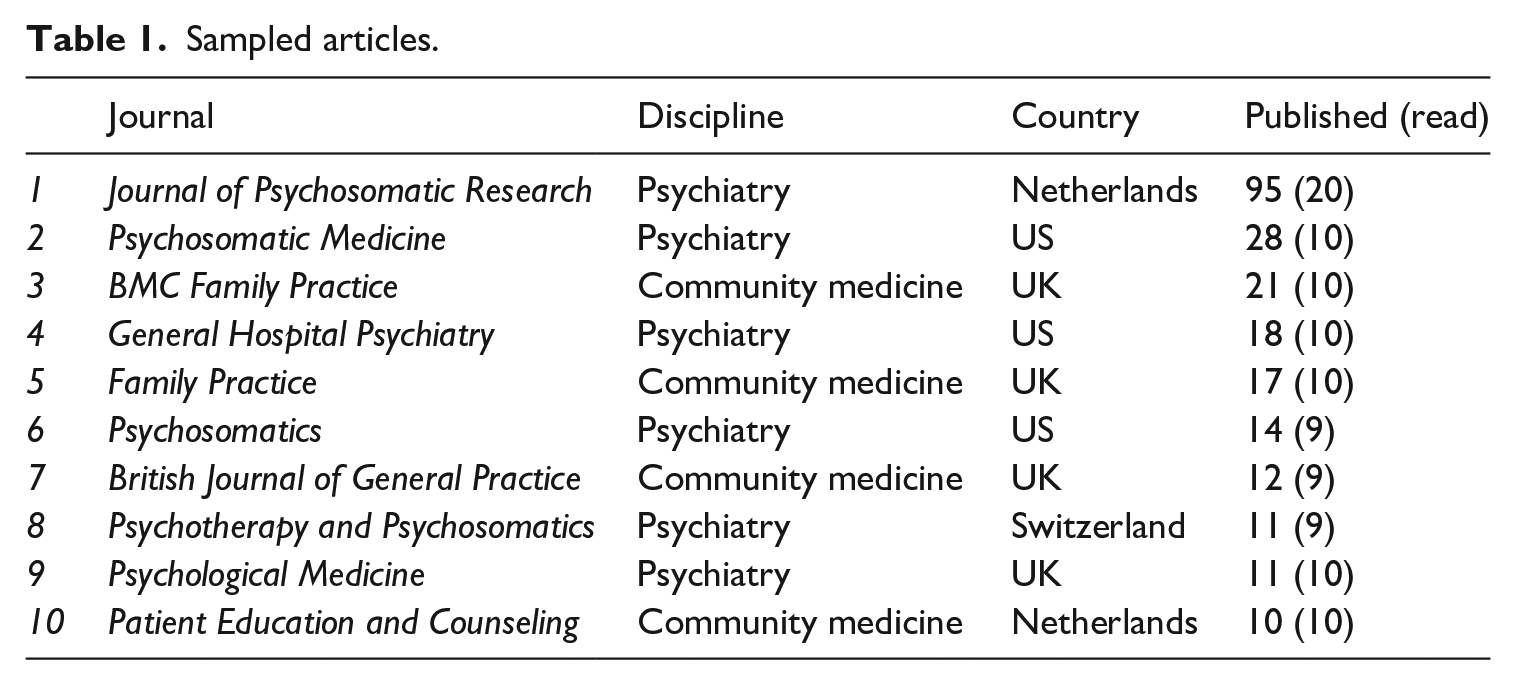
Judging by the publication rates in the journals sampled, the MUS category is used mostly in the context of psychiatric and primary care research (most frequently in the former) (177/60), though MUS is invoked in psychosomatic contexts more often than in psychiatry in general. Comparing the increase in publications that topicalize MUS with the total number of publications in the journals sampled shows that 2001 was indeed a pivotal year: While never rising above 1% of the total output before 2001, output increased from 1.3% (N = 11) to 7.4% (N = 88) of all publications between 2001 and 2016.
My analysis centres on definitions and operationalizations. Definitions were commonly found in the opening sections of articles, operationalizations in the methods sections. As both definitions and operationalizations are salient forms of classification in science, analysing them offers important clues about the classification of MUS in scientific work.
Articulations of definitions and operationalizations may deviate from what researchers actually think and do in practice. For the purposes of this study, it is more important what researchers want to communicate than what they think for themselves. Deviations from actual practice are, however, a possible problem. In the analysis, I therefore focus on what seem to be straightforward differences in classification practices (e.g. it seems clear that researchers requiring four unexplained symptoms for admission in a study have classified differently from those requiring only one, even though we do not know how they actually counted). In the discussion, I raise the issue of how much crucial information is missing from the accounts.
I coded articulations of MUS thematically, first in a broad-brushed manner in Nvivo, then in a more finely grained manner in Word. During the analysis, I wrote memos subsequently incorporated in the analysis. I was interested in classification practices from the outset, but the interest in methodological variations as varied classification practices stemmed from engaging with the data. Early versions of the analysis have been presented to audiences of social scientists and medical researchers on four occasions.
All documents in the sample are listed in the
Appendix
, each with its own code consisting of two numbers (e.g.
Constituting the junk drawer
The core criterion
As an ordering device, a junk drawer is a means of controlling anomaly by containing it. The MUS category is thus a means to manage cases that are in some way considered anomalous. But what makes them anomalous? What defines a case of MUS? According to medical science, the most fundamental feature of MUS is the co-occurrence of present somatic symptoms and the absence of evidence/signs of somatic disease: Patients complain that something is physically wrong with them, but doctors find nothing to support that claim in or on their bodies. This is exemplified in the following list of brief and more or less explicit articulations, where MUS are defined as referring to:
There are differences between the examples, such as the degree to which symptoms are unexplained – ranging from when examination does not yield ‘sufficient organic findings’ (
In medicine, the interest in this co-occurrence of present symptoms and missing signs seems self-evident. It is almost never discussed or thematized explicitly in the literature or in my sample (but see
In some cases, MUS are not defined explicitly but simply referred to as a familiar concept whose meaning is taken for granted (e.g. Criteria for a medically unexplained episode …: (a) the patient presented with physical symptoms; (b) they received investigations for these; and (c) the investigations and clinical examination revealed no abnormality, or abnormalities that were thought to be trivial or incidental (
Therefore, MUS are constituted as anomalies by their lack of fit with some ruling epistemic convention or paradigm (Barnes, 1982; Kuhn, 2012). As indicated both by the expectation that somatic symptoms should be accompanied (and indeed caused) by underlying somatic disease, and by the emphasis on terms such as ‘disease’, ‘organic’, ‘pathology’ and ‘tissue abnormality’, the paradigm in question is that of scientific biomedicine and its biomedical model of disease. Central to that model are the notions that: (i) psyche and soma (body) are separate domains (though not necessarily independent), (ii) symptoms are effects that should have causes, (iii) somatic symptoms should have somatic causes, known as ‘disease entities’, (iv) such entities may be detected upon physical examination (blood tests, imaging technologies, palpation, etc.) in the form of objective ‘signs of disease’ (tissue abnormalities, organic pathology, etc.), and, (v) upon detection, the objective signs explain the subjective symptom (e.g. Lock and Gordon, 1988). As historians of medicine and science have shown, this is a culturally contingent understanding of disease, contrasting sharply with, for instance, the symptom-oriented 17th century classification of Sydenham or the ‘humoral pathology’ of Galenic medicine (Jewson, 1976; Jutel, 2010; Porter, 1999). Likewise, the distinction between ‘objective signs’ and ‘subjective symptoms’ is a sociocultural achievement consisting of the symbolic decoupling of facts from their observer (Shapin and Schaffer, 2011). The biomedical paradigm is, however, an important influence, not least in the medical research into MUS: It is what makes the core criterion reasonable.
MUS may thus be characterized as anomalies constituted by their lack of fit with scientific biomedicine, by their violation of expectations induced by the biomedical paradigm. When MUS are defined by the co-occurrence of present symptoms and absent signs, therefore, it is not simply that signs, like a great number of things, are not there. Rather, from the point of view of biomedicine, they are missing. When they are missing, the symptom is unexplained, since underlying disease entities are the explanans, or what ‘does the explaining’ (i.e. causes), in biomedicine; or the symptom is dubious, since objective evidence are what identifies symptoms as real. It is thus against the background of these conventions that MUS are anomalous: their violation summons up the possibility that there is something medicine has not found or understood. The ‘discordance’ between what the patient says and what the doctor can find must thus be accounted for.
Another way of putting this is that the system of medical knowledge is causally implicated in the construction of MUS as a ‘junk drawer category’ – it causes the need for a category to manage anomalous symptoms. Cases of MUS thus become interestingly similar within the context of modern biomedicine, giving the category some sense of coherence. Typically, however, due to the framing of the core criterion, the deeper connection between biomedicine and the ambiguity of MUS is hidden from view.
Framing the core criterion
We can discern two main ways of framing the core criterion, which I call the doxic and the heterodoxic framing. They form a continuum rather than a neat dichotomy, with some articulations ambiguously poised in the middle.
The doxic framing earns its name from its frequent occurrence in the sample and from the way it takes biomedicine for granted (doxa) as the basis for thinking about MUS. Its main characteristic is thus the silencing of how taking biomedicine for granted conceals its constitutive role in making MUS anomalous. The doxic framing thus centres on symptoms and patients, while keeping doctors and their knowledge more or less out of the picture. Consider the following example (an extended version of example International studies show that 10–20% of patients in primary care suffer from physical symptoms without any sufficient organic findings. In some medical specialties, such as gynaecology, neurology, or gastroenterology, in 30–70% of cases no organic causes for the patients’ symptoms can be found. These patients with medically unexplained symptoms (MUS) constitute an economically relevant group in the health care system, since they receive many elaborate diagnostic examinations and medical interventions, in spite of the absence of an organic disease. (
The focus is clearly on symptoms and patients (and budgets). Of course, such a focus is not out of place in a medical context. But the (unintended) consequence that stems from this focus is important: By the very act of fixing its gaze on symptoms and patients, the text effectively turns its back on medical knowledge and medical professionals, rendering them almost invisible. Note, for instance, that we are told nothing of the doctors who are unable to come up with the right sort of evidence and the specific and limited techniques they have at their disposal in that regard, or that the demand for evidence of specific sorts results from the paradigm the doctors employ. Instead, the reader is confronted with symptoms that are ‘without … findings’ or for which ‘no organic causes … can be found’, and with expensive patients who ‘receive many elaborate diagnostic examinations’ (omitting the doctors who are providing them). The narrative presents MUS as having to do with symptoms and their patients, but not with the medical profession and its knowledge base that play a constitutive role in making these cases into medical problems in the first place. Doxa thus creates a problem, while the doxic framing deletes any trace of its involvement.
Accordingly, MUS seems like a quality inherent in the symptoms rather than an ascribed attribute resulting from the mismatch between those symptoms and the biomedical paradigm. The examples above (
A minority of articles deviates from the doxic norm and instead employs what I have dubbed a heterodoxic framing. Most of these are by Peter Salmon, either alone (
Compared to the examples of doxic framing above (
Thus, although the doxic and heterodoxic framings both make MUS about the co-occurrence of present somatic symptoms and absent somatic signs, they disagree on the implications: the heterodoxic framing foregrounds biomedicine and its practitioners, thus making the doctors’ knowledge and practices figure as important factors. It does not, however, fully recognize the causal role of biomedicine in making MUS anomalous: What is highlighted is the ignorance and impotence of practitioners, but nothing is said about the causal role of their positive knowledge, for example, how the biomedical paradigm makes it problematic to have somatic symptoms but not somatic signs of disease. It is never pointed out how it is what is known (knowledge), as much as what is not (ignorance), that makes MUS ambiguous and problematic. Thus, the constitutive dynamic between symptom and epistemic order is made obscure by both framings.
Solid core, fuzzy boundaries
Apart from variations in framing, the sample is homogenous in its implicit agreement about the core criterion. But there are also important definitional variations, especially in the practices of establishing similarity between MUS and two other salient categories. The variations are interesting because they dramatically alter the scope and meaning of MUS, and thus about its constitution as a junk drawer in the epistemic order.
The first is ‘somatoform disorders’ (SD), referring to various forms of ‘somatization’, something a patient may be said to suffer from if (s)he is prone to ‘somatize’ (or ‘make somatic’), meaning that (s)he is likely to interpret and indeed experience mental illness as though it were bodily in kind. To somatize is to attribute pain to the body that is actually in the mind (e.g. Greco, 2012; Jutel, 2010). As stated above, SD were organized as a cluster of psychiatric diagnoses in the Diagnostic and Statistical Manual of Mental Disorders until its fifth revision in 2013 – but the practice of connecting SD with MUS has not stopped (e.g.
MUS connect with SD in one of two ways. Some present SD as a special and more serious type of MUS. For instance, in
The connection with SD is a frequent occurrence in the sample and in many cases the documents are as much about SD as they are about MUS. This is likely because most SD diagnoses have MUS as a core criterion. The explicit association with SD was stronger in articles in psychiatric than community medicine journals (~55% vs. ~15%): SD is a psychiatric category.
The second category with which MUS are frequently connected is ‘functional somatic syndromes’ (FSS). FSS refers to clusters of symptoms that are considered well-described and non-trivial complaints. FSS are typically exemplified by diagnoses such as chronic fatigue syndrome, fibromyalgia and irritable bowel syndrome, which, incidentally, are the most common exemplars of MUS in social science.
5
As with SD, FSS were articulated either as a more serious version of MUS, or as synonymous with them. For instance, consider the following examples (my emphasis):
Whereas
For our purposes, the connections with SD and FSS are interesting because they variously alter the scope and meaning of the MUS category, thus indicating differing practical applications. Moreover, they indicate differing thresholds for declaring something an anomaly. For instance, since FSS are relatively ordered and non-trivial conditions, articulating MUS as synonymous with FSS (as in
To sum up the analysis so far: The core criterion of MUS is the co-occurrence of present somatic symptoms and absent somatic signs. This criterion implicates the biomedical paradigm as a constituent factor. In the vast majority of cases, the category is framed in a way that conceals this from the reader. Thus, the core criterion comes across as capturing an important feature of a patient group, a group that can therefore meaningfully be classified as one. It is unclear, however, if the MUS category applies to all cases that fulfil this criterion or is limited to a subset. This implies an ambiguity of meaning. In the next part, we can see how this ambiguity extends to practical applications in research.
Managing the junk drawer
A junk drawer is for containing disorder, for anomalous cases. What characterizes medical scientists’ management of the junk drawer? That is, how is the MUS category operationalized in research? The answer is that operationalization varies tremendously, leading to the drawer being filled with the experiences and characteristics of very different groups of patients. Though one might have expected classification to vary according to disciplinary boundaries (between community medicine and psychiatry), my analysis reveals that, in the main, it does not. Here I present the most important ways in which operationalizing practices varied.
Operationalizing the core criterion
Among those that articulate an interpretation of the core criterion (which many do not, e.g.
Some researchers operationalize MUS inclusively as containing all symptoms not fully explained by ‘tissue abnormalities’ or other signs, including cases of doubt. If not MES, then MUS. For instance, in one study, symptoms were classified ‘as either “medically explained” or “(partly) medically unexplained”’ (
Others operationalize MUS restrictively as limited to cases that are fully unexplained, meaning that cases of doubt were excluded from the category. For instance, in one study, ‘where there was uncertainty, the case was reviewed by two other raters [other than the one who was uncertain] … and categorized as MUS only if agreement was unanimous’ ( Symptoms that could be attributed to a known medical condition (i.e., known somatic disease or pathophysiologic dysfunction) were regarded as ‘medically explained.’ In cases where no pathologic findings could be detected, symptoms were regarded as ‘medically unexplained.’ If the findings were ambiguous, symptoms were regarded as ‘mixed.’ (
Cases of doubt are categorized as ‘mixed’ and thus kept out of the MUS category. A similar strategy was devised in
Notably, a few studies are not interested in what the patients have per se but in what doctors (and sometimes patients themselves) believe they have (e.g.
Additional criteria
In addition to the core criterion, studies have often enlisted additional criteria. The four most common types are symptom count, impact and persistence and the frequency of attendance at the clinic (or some other measure of health care use). The first three characterize the complexity and severity of the complaint: Count specifies a minimum number of symptoms, persistence specifies a minimum timespan the symptom must have existed, and impact specifies the power of the symptom, typically to distance MUS from ‘trivia’. So for instance, in some cases, research includes patients with single, recently onset and merely bothersome symptoms, whereas in other cases it is limited to patients with multiple and seriously debilitating symptoms lasting six months or more. Frequency of attendance is included either because repeatedly seeking help is considered a sign that the patient has MUS, a form of behaviour revealing that the patient is ‘excessively’ worried (
Based on the various uses of these additional criteria, we can distinguish between more or less inclusive classifications and specify the types of conditions and patients that are variously omitted or included in the junk drawer.
First, we can note that some studies (e.g.
More often than not, however, one or more additional criteria are enlisted. For instance, in a study of predictors of psychiatric morbidity, impact was a criterion (though not a very specific one): ‘Mild symptoms that had not led to consultation with a health care professional … or to marked interference with normal activities were excluded’ ( ‘Criteria for ‘persistent medically unexplained physical symptoms’ a. The presentation of a physical symptom b. The symptom had existed for at least 3 months c. It had caused clinically significant distress or impairment d. It could not be explained by physical disease, that is; ‘physical symptoms for which no clear or consistent organic pathology can be demonstrated’ Other inclusion criteria (from electronic record search) Had consulted GPs (clinic, telephone or home consultations) 8 or more times in previous 12 months’ (
We can recognize the operationalized core criterion in item ‘d’ and we can see that frequency of attendance (‘8 or more times in previous 12 months’), persistence (‘at least three months’) and impact (‘clinically significant distress or impairment’) are listed. Symptom count, however, was not relevant to inclusion. Some studies used the same set of criteria but operationalized them differently. For instance, in a study testing the effectiveness of mindfulness-based cognitive therapy, (
To compare the examples reviewed so far, some studies make high and gender-specific demands on symptom count. For instance, a study testing the validity of a diagnostic instrument
7
operationalized MUS using the criteria for ‘abridged somatization’ – a diagnosis that requires ‘a history of six medically unexplained symptoms for women and four medically unexplained symptoms for men’ (
Other studies demanded multiple symptoms but typically set the bar at two or more without making gender specific demands (e.g.
Unwitting variations
As is apparent from the examples reviewed, the MUS category is used to study health problems that are potentially highly dissimilar in medically relevant ways. Thus, researchers cluster and store information about patients whose needs are potentially very different in the same category. These patterned variations help explain the extraordinarily confused prevalence estimates of MUS reported by medical scientists (3–50% of all primary care consultations, see introduction). Yet the variations take on extra significance because the medical scientists are strangely silent about them. During a close reading of the research literature, this absence is striking: there are almost no intertextual references or discussions in the sample to how others have classified MUS and how one’s own approach differs. Thus, medical scientists seem unaware of the tremendous variations in their management of the MUS category.
It is not uncommon to find researchers operating with differing criteria, but when methodological variations are accompanied by silence and widespread unawareness, it can be problematic. For clinicians who are expected more and more to keep up with the latest research, it can lead to confusion and exacerbation of ‘research-based uncertainty’ (Timmermans and Angell, 2001). It also seemingly causes confusion among medical scientists themselves, who uncritically draw on conclusions from studies that have operationalized MUS very differently from themselves (different criteria, data, procedures, etc.). For instance,
Discussion and concluding remarks
I have omitted some details concerning operationalization – notably the places (e.g. primary or secondary care, Manchester or Munich) and players (assistants, consulting physicians, patients, etc.) involved, and the varied uses of classification instruments and (more rarely) selected codes from WHO’s main diagnostic manuals used to operationalize MUS (see
The analysis has demonstrated how MUS is constituted as a ‘junk drawer category’, and how this category is managed in medical research. First, I have shown that the core criterion of MUS as a category is the co-occurrence of present somatic symptoms and absent somatic signs of disease, and that, fundamentally, this criterion is an expression that MUS violate expectations induced by the biomedical paradigm. Biomedicine as epistemic convention is therefore causally implicated in making symptoms anomalous and this ‘paradigm-induced’ anomalous character is what constitutes MUS as a category. In other words, the junk drawer is constituted as a contravention of the existing order. The majority of articles, however, hide the constitutive role of biomedicine, making the core criterion an ontological fact about the symptoms, rather than an epistemic fact about the beliefs and practices of the profession. Thus, the nature of the MUS category as a junk drawer is concealed.
Second, I have shown patterns of substantial variation in how the category is managed, focusing on the most important variations in what scientists think belongs in the MUS category. Thus, the analysis reveals a lack of consensus in the proper functioning of the junk drawer. I interpret this lack of consensus as a disagreement about the threshold where anomalous symptoms become important for science. On the one end are those who manage the category restrictively, thus ignoring a range of symptoms that are common yet, from the point of view of biomedicine, every bit as anomalous. On the other end are those who manage the category inclusively, including single, transient and relatively trivial symptoms. Importantly, however, the lack of consensus about the proper functioning of the junk drawer is silent, and also widely unrecognized (or ignored) by the scientists themselves. Although the category thus is a common interest and a ‘meeting ground’ for the scientists, it is not (yet) a site of interaction and exchange.
Though the claim that MUS are misfits in biomedical contexts is not new (Jutel, 2010: 230; Kirkengen et al., 2016: 496), the constitutive role of biomedical knowledge and research practice in medical science has, to my knowledge, not been explored and established empirically before.
Assumed psychogenic aetiology as monster-adjustment
Medical scientists are not discarding or ‘monster-barring’ (Bloor, 1978) MUS, not treating the symptoms like waste. Instead, they are including them in the system of medical knowledge, subjecting them to research, using a containment device I call a junk drawer to protect the system’s orderly state from contamination. The MUS category thus serves this containment function. There is a sense of optimism to it, in that a junk drawer saves puzzles for later, allowing for future scientific understanding.
Regarding puzzle solving, historians of science and others suggest that when anomalous phenomena are not simply ignored or discarded, scientists will typically try somehow to make them fit in by making slight adjustments or creating new categories to the established order, or by proposing rule-exceptions that dampen or remove the anomalous character. These strategies are called ‘monster-adjustment’ (Bloor, 1978).
There are strong indications of a move towards such strategies in the sample, in the form of assumptions that unexplained physical symptoms are really symptoms of mental distress (e.g. Jutel, 2010). Such assumptions are criticized in the sample (e.g.
This interpretation of MUS as caused by a misunderstanding on the patient’s part has been criticized by some social scientists as a form of blame-shifting (e.g. Horton-Salway, 2002; Jutel, 2010). Others have been more cautious. Greco (2012: 2365) warns against any knee-jerk criticism of psychogenic assumptions by social scientists. She argues that the medical profession might be right to treat MUS as psychogenic and that the question must be settled empirically. Inasmuch as ‘right’ indicates that it could work, I agree. However, from what evidence there is, it does not seem to do the trick: An important context where psychogenic assumptions are expressed is when researchers complain that patients reject psychiatric treatment (e.g.
Somatization in its varieties has yet to succeed as a monster-adjusting strategy. Moreover, due to recent changes whereby all SD diagnoses have been ejected from formal classifications (American Psychiatric Association, 2013), the strategy might have to change. But that is the beauty of a ‘junk drawer category’: They can try again later.
Standards and standardization
Members of the research community have lamented the lack of formalized and widely shared standards for classifying MUS. In the absence of standards, creative but highly varied classification practices characterize research. But what difference would shared standards make?
Formalizing a set of criteria, for instance relating to symptom count, impact and persistence, or the frequency of attendance, would probably enable researchers to study a more homogenous patient group than current practices allow for. However, standardized criteria do not necessarily make classification homogenous, as they must nevertheless be interpreted and applied in the course of situated practice (Bloor, 1997; Timmermans and Berg, 2003). This leaves room for substantial variation. In cases of MUS, standard criteria will not change the fact that counting or estimating the impact of symptoms is difficult work, with no definitive answers (Berg, 1992; Rosendal et al., 2013). Moreover, there are reasons to believe that what I call the core criterion is itself a major source of variation: studies indicate that even when criteria are formalized and shared, doctors disagree about where to draw the line between the explained and unexplained (e.g. Creed and Barsky, 2004: 404) – not least because they also disagree about the distinction between diseases and non-diseases (Smith, 2002; Tikkinen et al., 2012). This indicates a less than clear-cut line between the explained and the unexplained.
Standardizing the classification of MUS would therefore require a more thorough reflection over basic concepts such as disease, objective evidence and medical explanation. The potential advantage of doing so would be the ability to determine the value of MUS as a medical category – to test whether it is sensible and helpful to group patients based primarily on their lack of fit with the biomedical paradigm.
Footnotes
Appendix
Acknowledgements
I thank Steve Sturdy and Gethin Rees for invaluable motivation and critical yet constructive comments, and Vassilis Galanos and Sampsa Saikkonen for inspiring discussions. I also thank Dag Album, Berit Bringedal, Lars EF Johannessen, Mats Lillehagen, Marte Mangset, Tore Rafoss, and fellow sociologists in the ‘sociology of knowledge’ session at the Norwegian sociology association’s annual seminar, for comments on previous drafts. Additionally, I thank Annemarie Jutel for being so forthcoming when asked about details of her work. Finally, I thank the editor of SSS Sergio Sismondo and the anonymous reviewers for valuable input. For any remaining shortcomings, I am entirely to blame.