
Abstract
Pregnancy-related anxiety commonly occurs among first-time pregnant women, carrying an increased risk of harmful effects to both mother and the growing fetus or newborns. This study aims to assess the effectiveness of a Comprehensive Health-literacy And Relaxing Music (CHARM) intervention compared with two other stand-alone interventions (relaxing music–only intervention, comprehensive health literacy–only intervention) and a standard care group on pregnancy-related anxiety. We conducted an open-label, parallel four-arms, randomized controlled trial among 128 low-risk primigravid women, who were randomly allocated to one of the four groups (1:1:1:1). Women were assigned with a separate web-based link for the three interventions, which were provided for 4 weeks. The pregnancy-related anxiety was measured using the Pregnancy-Related Anxiety Questionnaire-Revised (PRAQ-R) assessed at baseline and post-intervention. After the 4-week intervention, a repeated-measures analysis of variance showed significant mean changes, and interaction effect between the groups on pregnancy-related anxiety levels (F(3,124) = 5.6, p = .001, ηp2 = .12); CHARM intervention significantly reduced pregnancy-related anxiety levels in comparison with other three groups including the standard care group. The CHARM intervention was thus found to be effective in reducing pregnancy-related anxiety levels, and may be recommended for pregnant women for promoting their perinatal mental well-being.
Pregnancy is a period where a woman experiences both physiological and psychological changes. Life stages such as pregnancy, birth, and early parenthood can be stressful for both women and their partners (World Health Organization [WHO], 2022). During the perinatal period, women are at risk of developing mental health issues due to changes in hormonal balance, poor quality of sleep and other contributing factors, which could lead them to feel vulnerable (Miller, 2020). The American College of Obstetricians and Gynecologists (ACOG) defined anxiety as the feeling of nervousness, worry, or concern felt by an individual and it can start at any time during or after pregnancy (American College of Obstetricians and Gynecologists [ACOG], 2021). According to the WHO, about 10% of pregnant women and 13% of women in the postnatal period experience a mental disorder, including depression (Hendrick et al., 1998; WHO, 2020). Anxiety affects women in all phases of their reproductive life and causes a greater risk of adverse effects on physical, emotional, and psychological well-being (ACOG, 2020). Perinatal general anxiety disorders significantly increase from 8.5% to 10.5% during pregnancy and from 4.4% to 10.8% during the postpartum period (Misri et al., 2015). Anxiety and depression during pregnancy are responsible for around 20% to 40% risk of developing obstetrical complications (Dhillon et al., 2017; Verbeek et al., 2015). Evidence suggests that pregnant women also experienced increased levels of anxiety (60%) and depression (30%) during the COVID-19 pandemic compared with the pre-pandemic period (Pallavi, 2022). Suicidal thoughts or acts of self-harm are associated with about 20% of pregnant women suffering from perinatal mental health conditions; hence ignoring mental health during pregnancy can significantly affect women’s health and well-being and, ultimately, children’s physical and emotional development (WHO, 2022). In South India, the prevalence of pregnancy-related anxiety has been reported to be 55.7% (Nath et al., 2019), with a higher rate of pregnancy-specific anxiety among the first-time pregnant women during their third trimesters of pregnancy (Madhavanprabhakaran et al., 2015). Several researchers have found that maternal anxiety or mental issues during pregnancy cause harmful effects on the mother and have a major impact on the developing fetus(es) and newborns (Nwebube et al., 2017; Pasha et al., 2022). Prenatal anxiety can also increase the risk of developing postnatal depression (Bright et al., 2018; Rwakarema et al., 2015). Pregnancy-related anxiety, which develops during the third trimester of pregnancy may also increase the risk of preterm births (Das, 2022). Maternal anxiety developed during the third trimester of pregnancy even increased the risk of shorter gestational age of the baby at birth (Dunkel Schetter et al., 2022).
With the development of advanced healthcare services, maternal mortality rates have been reduced (WHO, 2019). However, it should be noted that maternal mental health problems may affect pregnancy outcomes, affect the well-being of the child, and increase maternal morbidities (Herrman et al., 2009). Maternal mental health is an emerging public health priority and an area of interest in exploring or conducting an intervention for promoting maternal mental well-being and child health outcomes (Ramaswamy, 2017).
Improving health literacy regarding pregnancy care among the first-time pregnant women may help minimize anxiety levels pertaining to their health and pregnancy outcomes. According to WHO, “Health literacy is the ability to engage with health information and health care services” (WHO, 2014). A recent cohort study (Yee et al., 2021) found that inadequate maternal health literacy among nulliparous women is associated with increase in various health risk conditions in the mothers (higher risk of cesarean birth, perineal laceration) and also neonatal outcomes (low birth weight, low Apgar scores). However, higher maternal health literacy is associated with reduced levels of anxiety and depression among pregnant women (Haruyama et al., 2022). Glover (2014) conducted a study that found if a mother is depressed, anxious, or stressed during pregnancy, there may be a higher risk of their child being born with adverse emotional, neurodevelopmental, or behavioral outcomes. This implies that interventions for pregnant women should begin in the first or third trimester of pregnancy to reduce maternal depression, anxiety, and stress.
Two randomized controlled trials (RCTs) were conducted to assess the effect of health literacy education on adaptation to pregnancy, self-efficacy, fear of childbirth, depression, anxiety, mode of delivery, and health literacy. Studies found that pregnant women who received antenatal education to improve their health literacy had significantly improved pregnancy outcomes, increased self-efficacy, decreased fear of childbirth, reduced depression and anxiety and increased health literacy levels (Aslantekin Özçoban et al., 2022; Çankaya & Şimşek, 2021).
A RCT was conducted to assess the effect of a guided internet-based tool (MamaKits) for the treatment of depression and anxiety among 79 pregnant women (Heller et al., 2020). The study found that there was no significant reduction in anxiety levels, depression levels, and perinatal child outcomes among pregnant women. Zafman et al. (2023) conducted a RCT study to compare the effectiveness of an interactive online childbirth education with normal prenatal education (as intervention) and normal prenatal education alone (as control) on anxiety, emergency healthcare utilization, and delivery outcomes among 90 high-risk pregnant women. The findings revealed that pregnant women who received the intervention had significant reductions in pregnancy-related anxiety, increased emergency healthcare utilization and higher satisfaction with the intervention compared with the control group. Aksoy Derya et al. (2021) found that tele-education (interactive education and consultancy provided by phone calls, text message, and digital education booklet) for pregnancy and birth preparedness when provided among pregnant women during COVID-19, significantly reduced perinatal distress and pregnancy-related anxiety.
Complementary and alternative medicine (CAM) provides effective interventions in the management of pain, minor ailments of pregnancy-like symptoms of nausea, vomiting, back pain, and reduction of anxiety among pregnant women; also, use of CAM interventions is increasing among pregnant and postpartum women (Johnson et al., 2016). Music can also be considered as a CAM intervention (Halim, 2002). Music is used therapeutically in many forms, such as music therapy, music medicine, music-based intervention, and live music to promote psychological wellness. Music acts as a non-pharmacological intervention in the management of pain, anxiety, depression, and cognitive improvement. Available evidence indicates that listening to music during the antenatal period (while performing obstetrical procedures or at home) results in a reduction in anxiety levels among pregnant women, including high-risk women (Lin et al., 2019).
Research has shown that music-based interventions are effective in managing anxiety or stress, reducing anxiety related to obstetrical procedures, having lower pain intensity related to the childbirth process, improving quality of sleep, and having positive impact on the fetus or newborn, such as increasing birth weight, bonding, newborns behaviors (habituation, orientation, and so on), increased fetal heart rate and movement (Arya et al., 2012; Çatalgöl & Turfan, 2022; Chuang et al., 2019; García González et al., 2018; Liu et al., 2016, Santiváñez-Acosta et al., 2020).
Pregnant women listening to multi-music (self-selected music from different records) had significant reduction in perinatal anxiety compared with pregnant women listening to the lullaby music (Baltacı et al., 2024). Indian classical music is considered an ancient form of music that emerged around the 13th century AD, which has two sub-categories/genres, namely Hindustani classical music, which evolved in Northern India, and Carnatic classical music which emerged in Southern India. Hindustani classical music (also known as North Indian classical music) is the cultural synthesis of the Vedic chant traditions and the traditional Persian music, which can evoke emotions such as “calm, sad, happy, tensed, and longing” (Mathur et al., 2015). Indian classical music comprises of Ragas (derived from the Sanskrit phrase “Ranjayiti Iti Ragaha”), defined as “one which induces emotions in the mind”—a melodic framework for improvization and composition in Indian classical music (Nettl, 2022) and Taal (a rhythmic structure and cycle). The Ragas are also a basic framework, which provide the melodic basis for compositions and improvizations (Jairazbhoy, 1995). Each Raga has associated notes (Swar) and groups of notes combined to form a meaningful Raga. Ragas can evoke various emotions in the listener or in the person who performs the music, such as sadness, romance, peace, strength, anger, devotion, longing, and passion (Hegde, 2017). Very few available studies have been conducted using Indian Classical Music to assess emotions, states, anxiety, and pain levels in different populations (Padam et al., 2017; Sharma et al., 2021); however no studies have focused on listening to Hindustani classical music Ragas and their benefits among pregnant women in the perinatal period.
Comprehensive health literacy related to pregnancy care may provide pregnant women with the opportunity to clarify their doubts and increase their levels of understanding (Aksoy Derya et al., 2021). Also listening to music is assumed to provide soothing effects and may improve relaxation levels among pregnant women during the perinatal period (Corbijn van Willenswaard et al., 2017; Konsam et al., 2023; Lin et al., 2019; Sanfilippo et al., 2020; Shimada et al., 2021; Simavli et al., 2014). Hence, the combination of health literacy and listening to music as interventions may help promote perinatal mental wellness, thereby reducing levels of perinatal anxiety among primigravid women (Perković et al., 2021). A web-based intervention that combines Comprehensive Health literacy with Relaxing Music (instrumental Hindustani classical music Ragas)—termed ‘CHARM’—was thus developed to improve perinatal mental health among low-risk pregnant women by reducing their pregnancy-related anxiety, thereby promoting perinatal mental well-being in pregnant women, which is the first randomized trial in a low- and middle-income country like India. Providing comprehensive, necessary, customized health information to the low-risk primigravid women may help promote health outcomes. Also, listening to relaxing classical music can be implemented for pregnant women throughout their pregnancy to improve perinatal health outcomes and promote mental well-being. This study was thus conducted to determine the combined effects of listening to Hindustani classical music Ragas and providing access to comprehensive health literacy using the CHARM intervention for low-risk pregnant women on reducing their pregnancy-related anxiety compared with the effects of the stand-alone interventions (only relaxing music intervention, only comprehensive health-literacy intervention) and standard care. The hypothesis is that there will be significant differences in pregnancy-related anxiety between the intervention groups and the control group (tested at less than .05 level of significance).
Method
Study design
This was a single-center, open-label, parallel four-arms RCT carried out at the outpatient departments, the antenatal and postnatal in-patient wards of the Obstetrics and Gynecology department of a tertiary care center in Udupi district, Karnataka, South India. Details of the assessment are listed in Figure 1.
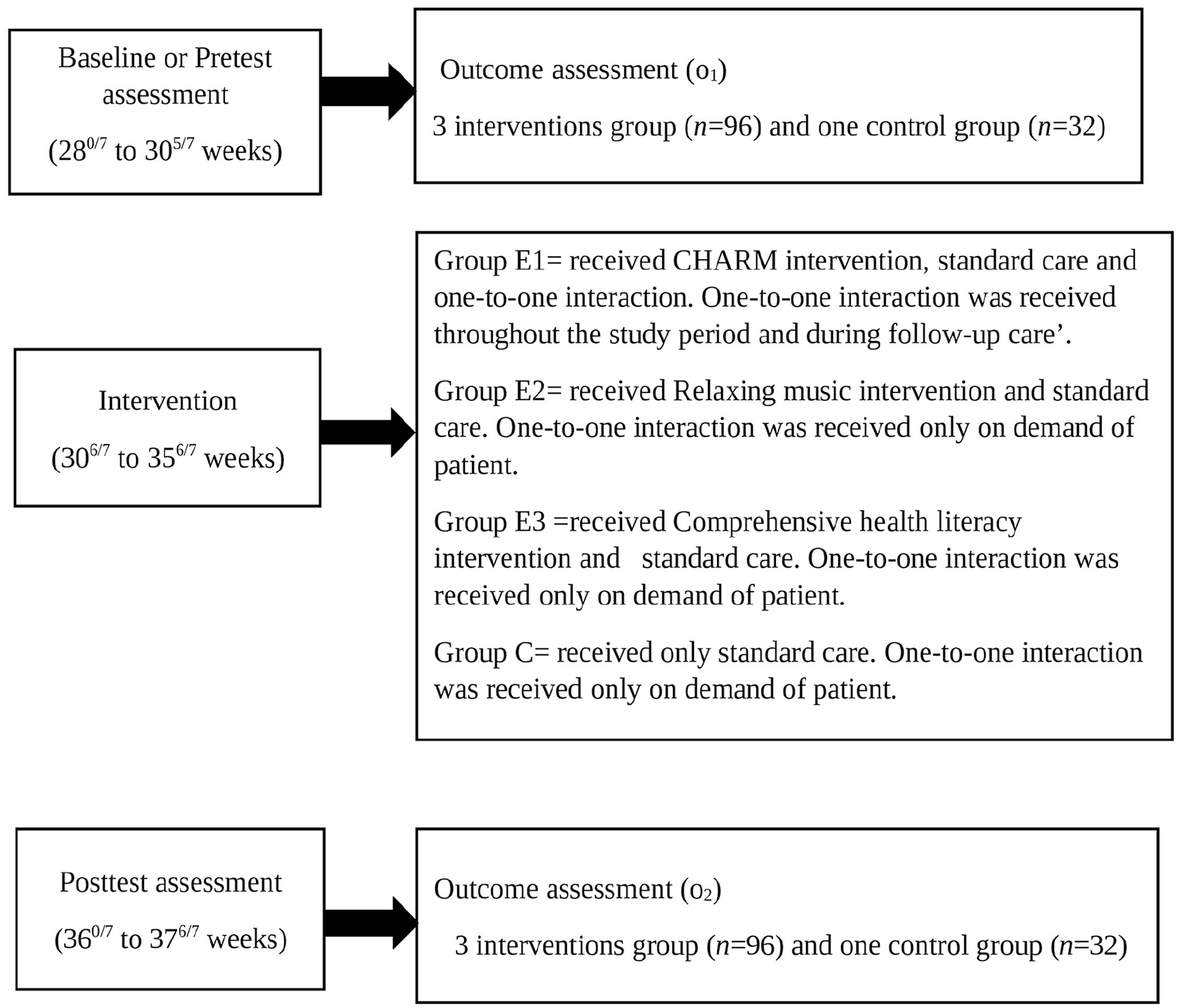
Description of Assessment Adopted in the Study.
Participants
A total of 128 eligible low-risk primigravid women aged 18 to 45 years, who could read and speak English or Kannada languages (the official language of the state of Karnataka, India), had normal hearing ability and possessed a smartphone, were recruited after 26 weeks of gestation. Those pregnant women who had pregnancy-related complications such as antepartum hemorrhage, pre-eclampsia, pregnancy-induced hypertension, gestational hypertension, cervical insufficiency, congenital fetal anomalies, and intra-uterine growth restriction diagnosed before 28 weeks of gestation or had multiple gestations; medical problems such as psychiatric disorders (known anxiety or depression, other illnesses), endocrine disorders (such as gestational diabetes mellitus, thyroid dysfunction), adrenal problems; had undergone assisted reproductive techniques (ART) such as in vitro fertilization, embryo transfer or who were at the risk of preterm birth, were excluded from the study. The Consolidated Standards of Reporting Trials (CONSORT) flow chart of participants is shown in Figure 2.
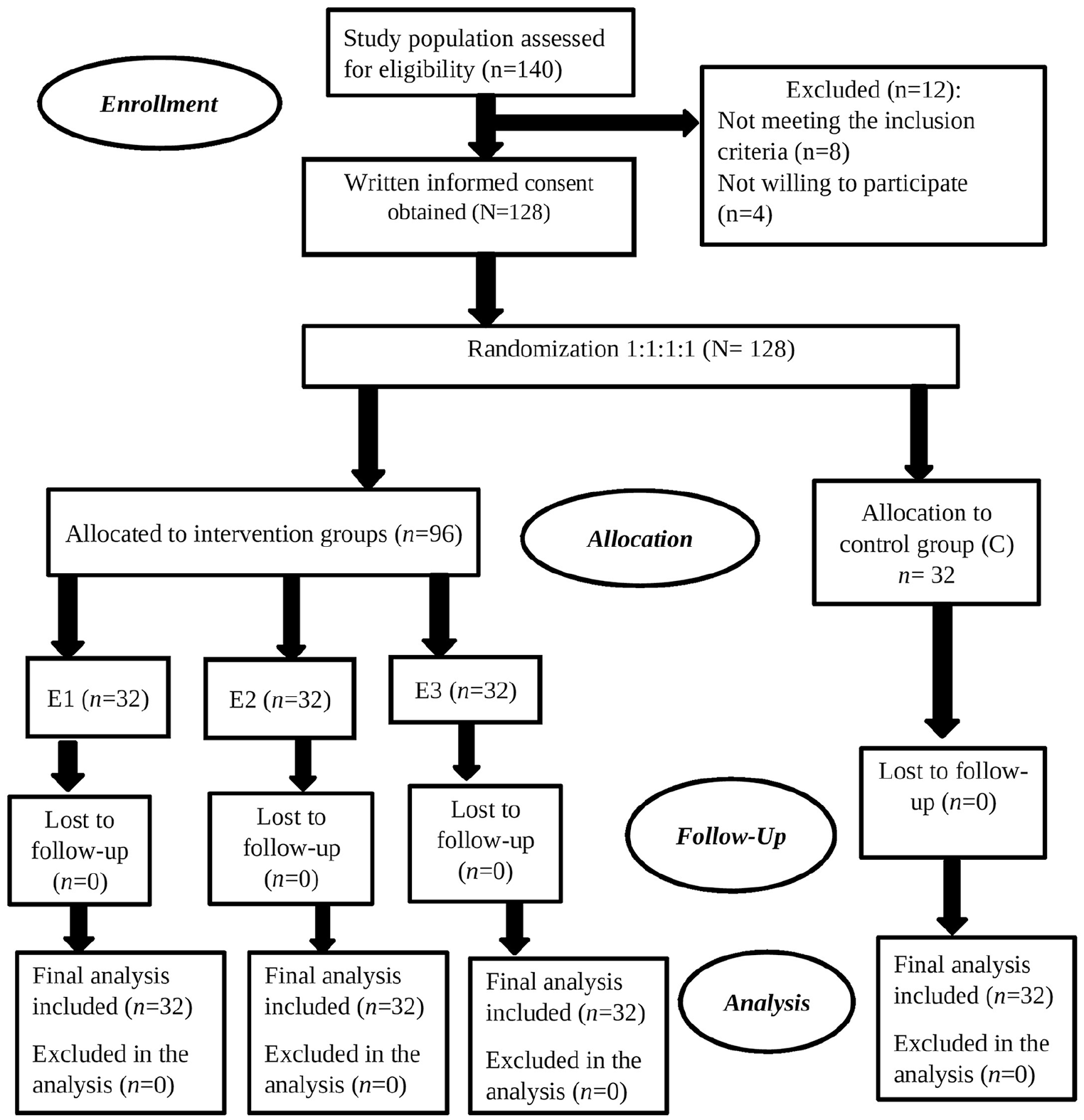
Consolidated Standards of Reporting Trials Diagram Showing the Recruitment of Participants for Four Groups.
Sample size calculation
The sample size was estimated using the formula of repeated-measures analysis of variance (RMANOVA), α = .05/3 adjusted for three comparisons (as three groups were compared with the control group), anticipated standard deviation of outcome variable = 1.15, 80% power, inter-class correlation = .4, calculated 27 participants for each of the four groups. Accounting for a drop-out rate of 15%, the sample size included was 128, which included 32 participants in each group.
Randomization
Participants were randomly assigned to each of the four groups of the study using the block randomization technique (1:1:1:1). For randomly assigning 128 participants, a total of 13 blocks of varying block sizes ranging from 8 to 12 were used. Computer-generated random numbers were generated using the Random Allocation Software (RAS) version 1.0.0 (Saghaei, 2004). Random numbers were generated by a researcher who was not involved in the recruitment or assessment of the outcome measures. Sequentially numbered, opaque sealed envelopes (SNOSEs) were used for allocation concealment. The researcher and the participants were blinded during allocation to intervention(s) or standard care. A nursing staff member working in the antenatal outpatient department who was not involved in the study allocated the participants following the SNOSE method. All participants received information about the study during the recruitment phase, with the option to withdraw from the study at any time without penalty. Voluntary participation was ensured to minimize the chance of loss to follow-up.
Materials
After the randomization procedure, the intervention groups were given a web link content with clear instructions regarding the interventions assigned to them. Group E1 received the CHARM intervention, group E2 received only relaxing music intervention, group E3 received only comprehensive health-literacy intervention, and group C received only standard care.
Relaxing music–only intervention
The relaxing music was chosen to be instrumental Indian classical music from the Hindustani genre. This mainly includes specific Hindustani classical music Ragas. The relaxing music was selected under the guidance and suggestions of Indian Classical (Hindustani) music experts—three Vidhwans /scholars trained in Hindustani Classical music (Vidya) who have the scholarship and experience in performing classical music concerts. Content and face validation was checked for the selected music tracks by the “Vidhwans” and found to be appropriate to be used for the study. The Ragas included were the morning Ragas (Bhairav, Bhatiyali, Lalit, Desh, Jaunpuri, and Todi), and the night Ragas (Rageshree, Jog, Jaijaivanti, Dharbari, Hansadhwani, and Shankara). The selected tracks of the specific Ragas were taken from Saregama India Limited (India’s oldest music label owned by the RP-Sanjiv Goenka Group, West Bengal, India), with the necessary permissions.
As India has diverse culture and norms that differ among different religions and communities, and also to minimize the chaos related to cultural and religious taboos among the listeners, this study included only Ragas, which were not devoted to any religious contexts and rendered using Hindustani Classical music instruments like the Santoor, Flute, and Tabla.
Comprehensive health literacy–only intervention
The health-literacy content was initially drafted by the researchers under the guidance of supervisors and subject experts (obstetricians and gynecologists, nurse-midwives, and researchers). Several discussions were conducted with selected primigravid women who attended the present setting to obtain information about their doubts and queries (especially information relevant to a first-time pregnant woman). The final draft of the complied health-literacy content was sent to the subject experts for content validation. Based on their suggestions, further modifications were made to the health-literacy content and validation of the content was carried out. The content was retranslated into the Kannada language (vernacular) and further back-translated to English to generate the final material for the study.
The comprehensive health-literacy intervention included information customized for low-risk primigravid women related to their antenatal care (antenatal diet, exercise, rest, sleep, maternal–fetal bonding, regular follow-up, daily fetal movement count, and management of minor discomforts during the third trimester of pregnancy), intranatal care (childbirth preparedness, pain management during childbirth process, childbirth care, early initiation of breastfeeding), and postnatal care (postnatal hygiene, breastfeeding, exercise, diet, minor discomforts, and their management, newborn care, mother and newborn bonding, birth spacing). The information was provided on a week-to-week basis to the antenatal women. The content was also embedded in a web-based application. The researcher instructed each participant included in group E3 (those women who received comprehensive health literacy along with standard care) to read the content during their free time and to ask questions via telephone calls, WhatsApp text chats, or text messages to the researcher. The comprehensive health-literacy content developed and validated for use in this study was registered for authorship in the Copyright Office, Government of India and has obtained a copyright (Registration no. L-117868/2022: Date of Registration: September 28, 2022).
The CHARM intervention
The CHARM intervention involved combining the two above-mentioned stand-alone interventions, that is comprehensive health literacy and provision of relaxing music, provided through a web-based application. Weekly regular reminders by means of text messages, WhatsApp chats, and phone calls were used to remind and ensure that the women regularly listened to music. The web-based application was developed by the researcher in a simple web interface, which allows the user to navigate through the content related to health literacy and also to choose the music track(s) that they would prefer to listen to. Also, the researcher ensured one-to-one interaction with the participants who received the CHARM intervention during their antenatal follow-up visits, discussed pregnancy care–related information, and clarified any doubts related to comprehensive health literacy shared through the web application as well as the music for approximately about 10 to 20 min during every subsequent follow-up visit until childbirth.
All the participants in the three intervention groups had received reminder texts, or WhatsApp chats or phone calls from the researcher; however, only the CHARM intervention group received an additional one-to-one interaction with the researcher during the follow-up visit. Nevertheless, the participants in the other three groups also received one-to-one interaction with the researcher but on demand, usually to clarify their doubts on pregnancy-related information and other aspects related to the intervention provided to them.
Standard care
Standard care referred to the regular antenatal care that included antenatal counseling and check-ups from the treating health care providers/consultants/obstetrician-gynecologist (OBGYN) consulting team. It also included routine antenatal visits, monitoring of fetal well-being, detecting pregnancies at risk, nutritional (prenatal vitamin, calcium, iron, and folic acid) supplementation during pregnancy, medications (if required), and antenatal counseling. All the low-risk primigravid women who participated in the study received standard care.
Demographic characteristics
Demographic characteristics included age of the women, educational qualification, religion, occupation, type of family structure, dietary pattern, and type of physical activity.
Procedure
The researcher (the lead author or the principal investigator) performed all the assessments included in the study by administering the self-reported structured questionnaire to each of the participant at baseline (or pretest) and after 4 weeks of the intervention (posttest). The data were collected between June 2021 and November 2022. Each Ragas track lasted for 10 to 15 min, and the researcher instructed the pregnant women to listen to the tracks for a minimum of 5 min or more regularly both in the morning as well as at night. The pregnant women were instructed to listen to the music sessions by selecting any track(s) of their choice available in the web-based application during the day (anytime in the morning between 6 a.m. and 12 p.m. Indian Standard Time (IST)) and at night (anytime between 6 p.m. and 10 p.m. IST), without using headphones, but by making sure that these sessions were listened to, while sitting or lying in a calm and quiet environment. The researcher had also sent daily reminders, either by text message or WhatsApp chat to each participant (in groups E1 and E2) to ensure that pregnant women regularly listened to the music.
Clinical proforma
This clinical proforma included the information collected from the health/clinical records of the women and fetus (es) during their third trimester of pregnancy (33 weeks +1 day to 37 weeks of gestation or till childbirth).
Pregnancy-Related Anxiety-Revised questionnaire
This standardized 10-item Pregnancy-Related Anxiety-Revised (PRAQ-R) questionnaire that assesses pregnancy-related anxiety was developed by Huizink et al. (2016) and is used to determine the pregnancy-related anxiety in primigravid pregnant women. There are three subscales of the PRAQ-R: fear of giving birth (three items), worried about bearing a physical or mentally disabled child (four items), and concern about own appearance (three items). The PRAQ-R is a revised version of PRAQ (Huizink et al., 2004). PRAQ has 34 items (Van Den Bergh, 1990) and was shortened to PRAQ-R with 10-items; PRAQ-R was applicable only for first-time pregnant women and hence it was used for this study. Currently, another version of PRAQ-R2 is used for multiparous women. The sum of the 10-item PRAQ-R total scale has a maximum score of 50, as each item is rated on a five-point scale from 1 (Absolutely not relevant) to 5 (Very relevant). The reliability of the translated tool (Kannada version) was tested among 20 low-risk primigravid women who visited the hospital. The reliability of the Kannada translated tool was .737 (calculated using Cronbach’s alpha); hence the tool was found to be reliable and appropriate for use in the study setting.
Ethical considerations
The project complied with standard ethical considerations, and ethical approval was obtained from the Ethical committee of Kasturba Medical College, Manipal and Kasturba Hospital Institutional Ethical Committee on November 11, 2019 (IEC 966/2019). Any protocol changes during the study period were updated as amendments and communicated to the ethical committee periodically. The participant information sheet containing a brief description of the study was given and explained to all participants a week before obtaining their written informed consent to allow voluntary participation. Written informed consent was obtained from all participants prior to conducting the study in the presence of a witness. The study was registered prospectively in the Clinical Trials Registry of India on 09/03/2020 (CTRI/2020/03/023848). No adverse events were reported by participants. Also, 2 weeks were allowed for participants to decide whether they wanted to take part, and there was no loss to follow-up.
Statistical analysis
The statistical analysis for the collected data was performed using Jamovi version 2.3.13.0 (The Jamovi project, 2022; R Core Team, 2021). Repeated-measures ANOVA was used to examine the main effects of time and the Time × Group interaction effect for PRAQ-R scores and subscale scores. Post hoc Tukey corrections were performed to identify the true value of significant difference among the groups and also to check whether significant groups or interventions differed in reducing scores of PRAQ-R. The effect sizes were reported as partial Eta square (ηp2). All p-values less than .05 (two-tailed) were considered significant.
Results
All participants in the four groups were included in the final analysis and there was no loss to follow-up or incomplete assessment.
Demographic characteristics
Out of the 128 pregnant women, 94 (73%) were aged between 26 and 33 years; group E1, 25 (78%); group E2, 24 (75%); group E3, 24 (75%); and group C, 21 (66%). Sixty-seven (52%) of the pregnant women included in the study had completed graduation, and 85 (66%) reported of living in a nuclear family. A total of 106 (83%) participants confirmed their pregnancy state by urine pregnancy test (UPT), and most of them performed physical activities in the form of regular walking 95%, jogging 4%, and yoga 1% (see Table 1).
Demographic Characteristics of Participants N = 128.
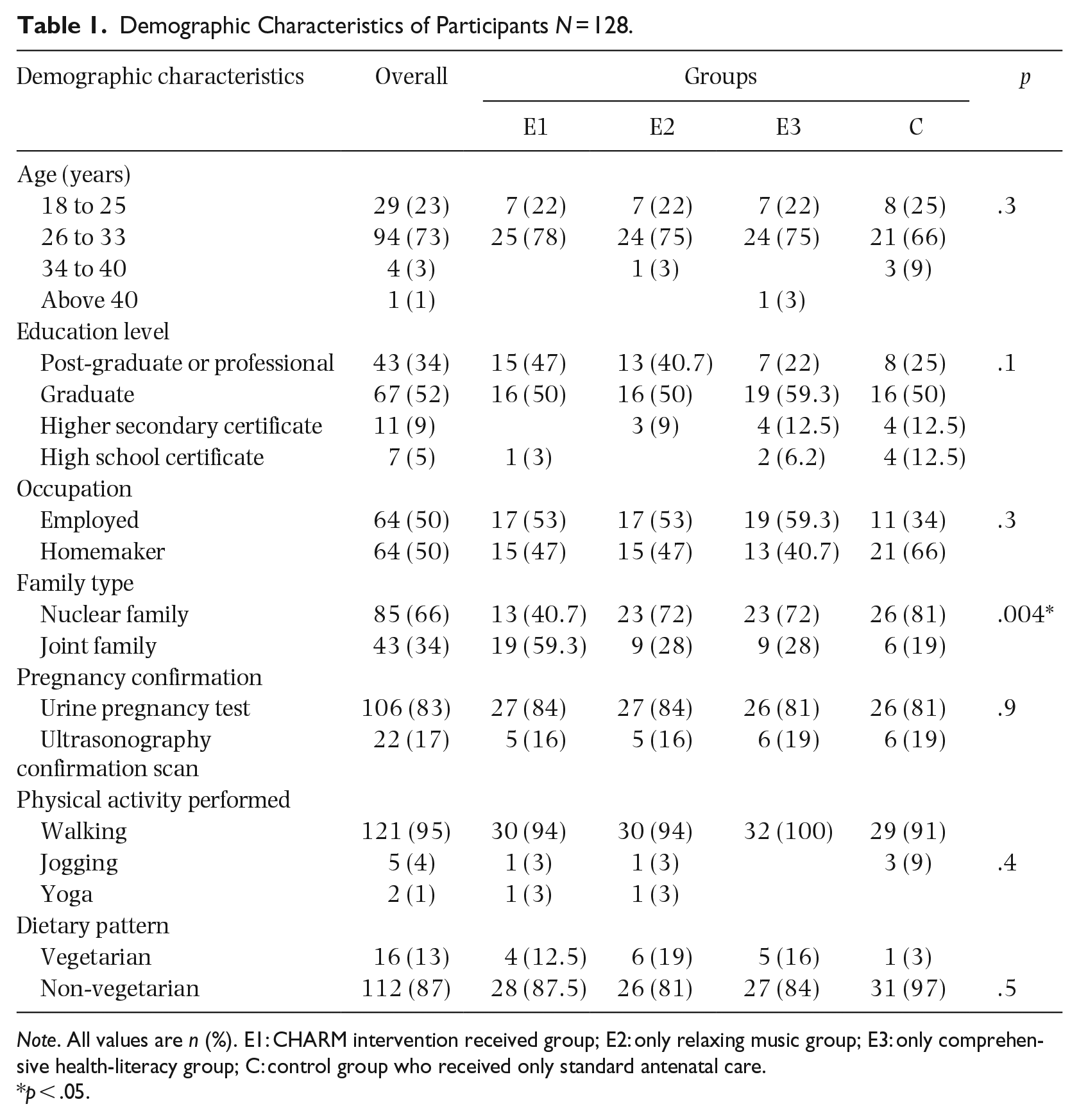
Note. All values are n (%). E1: CHARM intervention received group; E2: only relaxing music group; E3: only comprehensive health-literacy group; C: control group who received only standard antenatal care.
p < .05.
Clinical proforma
The clinical proforma includes the health/clinical records of the mother and their fetus(es) during 33+1 weeks to 37 weeks of gestation and above, out of 128 low-risk primigravid women; 31 (24.2%) women had a record of developing maternal complications such as 9 (7%) pregnant women had anemia, 3 women (2.3%) had pedal edema, 11 (8.5%) high blood pressure, 1 (0.7%) received oral tablet Labetolol for risk of pre-eclampsia, 6 (4.6%) had a low amniotic fluid index, and 1 (0.7%) was COVID-19 positive. There were no records of abnormalities or complications in the developing fetus among the women included.
Pregnancy-related anxiety scores
The mean, standard deviations, and 95% confidence intervals (CIs) were analyzed for the total scale scores of PRAQ-R; the pretest and posttest score varied across the four groups and its subscale scores as shown in Table 2.
Mean Difference and Repeated-Measures ANOVA Test of Pregnancy-Related Anxiety Questionnaire-Revised scale scores among four groups, N = 128.
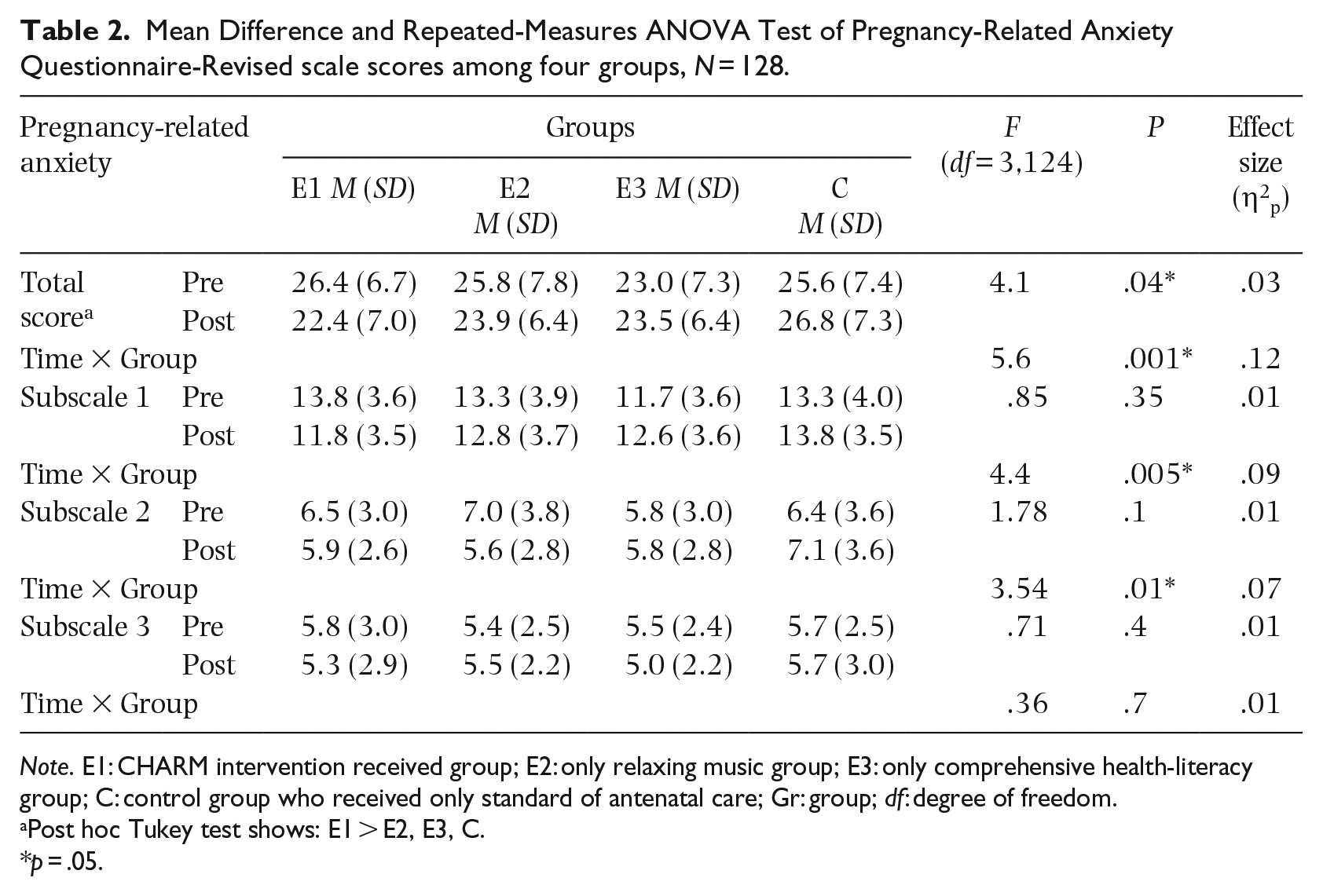
Note. E1: CHARM intervention received group; E2: only relaxing music group; E3: only comprehensive health-literacy group; C: control group who received only standard of antenatal care; Gr: group; df: degree of freedom.
Post hoc Tukey test shows: E1 > E2, E3, C.
p = .05.
To analyze the effect of the interventions on the mean scores of pregnancy-related anxiety among the pregnant women (four groups and two time points), repeated-measures ANOVAs were used, as shown in Table 2. The results showed significant difference in total mean scores of four groups (F(3,124) = 4.1, p = .04, ηp2 = .03) and interaction effect across groups (p = .001, ηp2 = .12), which reveals the large effect of the intervention. Furthermore, post hoc Tukey test showed that participants who received CHARM intervention (group E1) had significant reduction in the total mean scores of PRAQ-R after 4 weeks of the intervention (p = .04) and they significantly differed in their mean scores of PRAQ-R as compared with participants in the other two stand-alone interventions as well as the standard care group. Although the group E2 (relaxing music only intervention) also showed reduction in the mean score of PRAQ-R during post-test, there were no statistical significant differences within groups or between other groups using post hoc Tukey tests. Interestingly, pregnant women in both the groups E3 (only comprehensive health-literacy intervention) and standard care group were found to have increased mean post-test scores of PRAQ-R. Analysis of the PRAQ-R subscales reveals that repeated ANOVA test were significant for subscale 1, “fear of giving birth” (p = .005, ηp2 = .09), and subscale 2, “worried about bearing a physical or mentally disabled child” (p = .01, ηp2 = .07), but not for subscale 3, “concerned about own appearance” (p = .7).
Discussion
To our knowledge, this is the first study conducted in South Asia that assessed the combined effects of health literacy and relaxing music (instrumental Indian classical music) on pregnancy-related anxiety among low-risk pregnant women during their third trimester of pregnancy. CHARM is a web-based intervention, which helps participants to be highly motivated and be actively involved, as evident by feedback and responses from the participants throughout the study. The majority of the participants were employed and there was no loss to follow-up. The findings of this study showed that there was a significant reduction in pregnancy-related anxiety for women who received the CHARM intervention compared with those who received the relaxing music–only intervention, the comprehensive health literacy–only intervention, or standard care. Moreover, there were significant reductions in the PRAQ-R scores in the subscales “fear of giving birth” and “worries about bearing a physically or mentally handicapped child” among women in the CHARM intervention group compared with those in the relaxing music–only group, the comprehensive health-literacy group, or the standard antenatal care group. These findings are consistent with the findings of Shen et al. (2022), who assessed the effectiveness of needs-based education for prenatal anxiety and found that there was a significant reduction in the total scores of pregnancy-related anxiety levels and scores in the subscales “anxiety of child health” and “anxiety of giving birth,” but no significant difference in “anxiety of self” among women in prenatal education group compared with those who received standard care.
The recent pandemic has created changes in individuals’ states of mental health. An online survey (Haruyama et al., 2022) that assessed the impact of health literacy on anxiety and depression among 5,739 pregnant women found that women with higher rates of health literacy had reduced levels of anxiety and lower depressive symptoms. Another cross-sectional study (Luong et al., 2021) among 518 pregnant women that assessed the impact of health literacy and healthy eating behavior on fear of pandemic, anxiety and depression demonstrated that pregnant women who had higher levels of both had lower levels of anxiety. They also reported that higher gestational age, that is, second and third trimesters of pregnancy, were highly associated with developing anxiety among pregnant women. Estrella-Juarez et al. (2023) found that music therapy and virtual reality therapy had equal effects in reducing pregnant women’s anxiety levels. Tseng et al. (2010) reported that even listening to music during the postnatal period generated a significant reduction in anxiety levels among postpartum women. Also pregnant women listening to mixed music had significantly lower perinatal anxiety levels when compared with those listening to lullabies (Baltacı et al., 2024).
Another RCT that involved two groups by Perkovic et al. (2021) who combined two interventions for reducing childbirth pain experiences and psychological symptoms after childbirth such as interpersonal sensitivity, hostility, phobic anxiety, and paranoid ideations found that the intervention group had significant reduction in childbirth pain experience and reduced psychological symptoms after childbirth, as compared with the usual care group. This study supports existing findings that pregnant women who are in their third trimester and who receive the combined interventions of comprehensive health literacy along with relaxing music during antenatal period had a significant reduction in anxiety.
Almost half of the participants were employed and homemakers, and one-third had higher education. These findings differ from a study by Nath et al. (2019) study in Bangalore, South India, which reported out of 350 participants, majority were homemakers (92%), and around one-third had high school education.
Limitations
This study was conducted in a single health care center, which limits the generalization of the findings. As the assessments were carried out by the lead author, blinding could not be achieved. Although follow-up and reminders were provided for listening to the music, the researchers had no control over the duration of the music exposure because the intervention was performed at home, wherein some participants reported during the feedback that they were unable to listen to the morning “Ragas” due to their household chores during the specified morning timings, which may be a potential limitation. This research also did not follow-up the participants during the postnatal period, except for 3 days during the early postpartum period. This study analyzed only quantitative data; hence we do not have an in-depth understanding about what the participating women felt about the intervention(s) or the online delivery, though feedback from participants suggested that the web-based approach was convenient for them and they had an engaging experience. We also found that pregnant women who listened to relaxing music intervention showed a small reduction in post-test mean anxiety scores; however, there were no significant differences when compared with the other groups including the standard care group.
If further research is conducted in this area, significant maternal and child health outcomes (maternal and child bonding, newborn behaviors) could be followed up to validate the intervention. This study was conducted among primigravid pregnant women. The effectiveness of the combined intervention of music and health literacy could also be compared among multipara and primipara pregnant women.
Conclusion
The CHARM intervention was found to be effective in reducing pregnancy-related anxiety as compared with the other stand-alone interventions of relaxing music only and comprehensive health literacy only. Interventions that combine health literacy (related to basic knowledge of pregnancy care during the third trimester of pregnancy, childbirth, postnatal, and newborn care) and relaxing music (instrumental Indian classical music) not only enhance knowledge levels but create relaxation and help reduce pregnancy-related anxiety for first-time pregnant women, thus improving their perinatal mental wellbeing. The CHARM intervention can be provided as an additional non-pharmacological intervention or as an add-on to standard antenatal care. This web-based intervention can play a crucial role for pregnant women, especially following the recent pandemic, where information could be easily accessible and affordable to pregnant women. This study findings provide evidence about the acceptance of the intervention—music along with health information among pregnant women in the antenatal period, which may translate to promote their perinatal mental health. Future research should focus on interventions to facilitate individualized care, minimize knowledge gaps, increase awareness on benefits of using CAM therapies, rigor analysis of the classical music used for its benefit in health care settings, all with a focus on empowering pregnant women to experience healthy pregnancy outcomes, thereby contributing to their positive perinatal mental health. This study findings will provide evidence about the acceptance of music along with health information among pregnant women in their antenatal period, which may translate to promote their perinatal mental health.
Footnotes
Acknowledgements
We thank all pregnant women who have voluntarily agreed to participate in this study. We also thank the content validators for validating the content of the intervention and other validators of the Hindustani classical music “Ragas” used in the study.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors certify that they have participated sufficiently in the work to take public responsibility for the content including participation in the concept, design, analysis, writing, or revision of the article. Furthermore, each author certifies that this article has not been and will not be submitted to or published in any other journal. All authors have no known competing financial interests or personal relationships that could have influenced the work reported in this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.