
Abstract
Successful emotional processing is pivotal for the therapeutic change, and music can support emotional processing. However, we know little on how music-based emotional processing actually predicts clinical outcomes. This study investigated music therapeutic emotional processing (MEP) as a predictor of therapeutic outcome in treatment for depression. Data consisted of self-reports of 64 clients (age range 19–57, 74% female) from a clinical trial (12 sessions) of integrative improvisational music therapy (IIMT). A 19-item MEP questionnaire was developed for assessing clients’ experiences after sessions. Emergent MEP factors were correlated with clients’ perceptions of the therapeutic value of the sessions (Session Evaluation Questionnaire [SEQ]) and with recovery from depression (Montgomery–Åsberg Depression Rating Scale [MADRS]). MEP emerged as a constitution of three factors: expression, awareness, and pain. Expression and awareness increased across the process and correlated positively with session value and MADRS change. Pain demonstrated a more complex inverted u-shaped temporal curve and correlated with roughness of session experience. The presence of pain during the late part of the therapy predicted lower recovery. The findings support MEP factors as predictors of therapeutic outcome and provide conceptual insight into the mechanisms of change in art therapies. Knowledge on music-based emotional processing holds relevance also beyond therapy context for everyday music engagement.
Background and aim
Music in emotional processing
The capacity of music to activate and facilitate emotional processing has been widely noted in the field of music psychology research. Elements of musical expression—tempo, loudness, pitch, and timbre—hold resemblance to the early communication of emotion in infancy (Stern, 1999; Trevarthen & Aitken, 2001). Music can express and evoke a wide range of nuances in arousal and valence (Gabrielsson & Wik, 2003; Zentner et al., 2008) and it is often used to support self-therapeutic emotion-regulation of everyday life (Baltazar & Saarikallio, 2019; Saarikallio, 2011). As symbolic expression, music provides access to the difficult emotions like sadness in a detached, self-reflective, and sometimes even pleasurable way (Frijda & Sundararajan, 2007; Garrido & Schubert, 2011; Vuoskoski & Eerola, 2017). It has been argued that music can support emotional competence by allowing access to emotions, by increasing awareness of emotions, and by supporting emotional agency (Ruud, 1997; Saarikallio, 2019).
The role of music in music psychotherapy is to enrich and enhance the therapeutic process, by offering a non-verbal way of expressing emotions and experiences closely linked to emotions, providing absorbing experience anchored in the present, and allowing the emergence of unconscious material (Bruscia, 1998; MacDonald & Wilson, 2014). Music therapy clinical methods range from receptive (e.g., music-listening) to productive (e.g., musical improvisation), but the different methods share the common idea of using music as a facilitator of emotional experience. At our clinic for music therapy training and research, we have developed the clinical model of integrative improvisational music therapy (IIMT). This model (Erkkilä, 2004, 2013; Erkkilä et al., 2012) is associated with the integrative psychotherapy tradition, meaning that the working style can be adjusted in terms of depth and theoretical orientation according to the needs of a client and the premises (such as length) of the therapy. However, IIMT draws its inspiration particularly from psychodynamic music psychotherapy tradition (Bruscia, 1998) where various aspects of improvisational approach and relational principles have been defined in a universal way. Clinical improvisation typically triggers emotional memories, images, metaphors, and associations that can then be further processed in the verbal domain for meaning formation. In two randomized controlled trials, we have found this model to be an effective way to treat depression (Erkkilä et al., 2011, 2021).
Art-based psychotherapies generally offer a form of therapy that employs the nonverbal and symbolic expression as an addition to verbal expression. This type of processing can be considered to be particularly helpful with a range of client groups that face difficulties in verbal expression. Major depression, for instance, is known to relate to speech retardation and prolongation of quiet episodes (Flint et al., 1993; Hoffman et al., 1985). Increasing amount of reviews have recently found that music therapy (Aalbers et al., 2017; Maratos et al., 2008) and dance-movement therapy (Karkou et al., 2019) are beneficial forms of treatment with the depressed clients.
Relevance of emotional processing for the therapeutic outcome
Emotional processing has been observed to be of central importance for understanding the therapeutic change in psychotherapy (Auszra et al., 2013; Greenberg & Safran, 1989; Hayes et al., 2005; Hunt, 1998). Across the various psychotherapy traditions, emotions have been approached quite differently, but regardless of the approach, emotion processing emerges as a central feature that predicts therapeutic outcome (Dörig, 2014; Hayes, 2015; Watson & Bedard, 2006). For instance, Watson and Bedard (2006) studied depressed clients’ emotional processing in both cognitive-behavioral therapy and process-experiential therapy, comparing cases of good and bad outcomes. Emotional processing was measured by the experiencing scale (Klein et al., 1969), and it was related to good therapeutic outcomes across both therapy forms. Studies of Dörig (2014) and Hayes (2015) have also demonstrated that emotional processing during the exposure phase of exposure-based cognitive therapy is predictive of better treatment outcomes in depressed clients. Emotional processing also seems to have a specific temporal curve in a successful therapy process, with an early increase and later stabilization of the intensity of processing. Watson and Bedard (2006), for instance, observed that the clients’ level of emotional processing significantly increased from the beginning to the midpoint of therapy and then slightly decreased at late therapy for both cognitive-behavioral and process-experiential therapy types. Overall, the studies corroborate the central role of emotional processing as a mechanism of change in psychotherapy for depression.
The concept and measurement of emotional processing in therapy
To study emotional processing as part of a therapy process, it is critical to elaborate how to conceptualize and measure it. Greenberg and Safran (1989) proposed a set of general principles that can be applied for supporting emotional processing across different types of therapy interventions: directing attention to inner experience, refocusing on inner experience, encouraging present-centeredness, analyzing expression, intensifying experience, symbolizing experience, and establishing intents. Further drawn from this, Greenberg and Pascual-Leone (2006) proposed that the successful processing of emotions, in the context of any emotion-focused experiential therapy, consists of three core ingredients: (a) some emotions are activated (arousal); (b) the client is able to acknowledge, allow, and tolerate these emotions by finding a middle ground between avoidance and over-engagement (regulation); and (c) the emotional experience is explored and reflected upon, for example, through symbolization and meaning-making (meaning-making). Auszra et al. (2013) discussed the concept of client emotional productivity—the optimal client in-session emotional processing in experiential therapy. They consider this concept to be inclusive of seven emotion-processing features: attending, symbolization, congruence, acceptance, regulation, agency, and differentiation. The components included to the concept of emotional processing vary to an extent, but the common feature across the definitions is that emotional processing can be considered as actions to approach (e.g., express, accept, and transform) the unwanted thoughts and related negative emotions, instead of avoiding or suppressing them (Hayes et al., 2005; Hunt, 1998).
The components of emotional processing can also be differently measured. For instance, the experiencing scale (Klein et al., 1969) is a measure designed to describe and assess clients’ emotional processing during therapy sessions. The measure relies on the analysis of verbal expressions, with raters assessing each client statement in terms of clients’ awareness of, and exploration and reflection on their inner experience to achieve self-understanding and problem resolution (Klein et al., 1986). These types of measures can reach a relatively thorough understanding of the clients’ mental processing, but are time-consuming to administer. As an option, self-report instruments have been developed for both clients and therapists to assess their experiences immediately after the therapy sessions. One of these instruments, for instance, is the Session Evaluation Questionnaire (SEQ; Stiles, 1980), which assesses the client’s perception of the session in terms of its emotional character and impact through four dimensions: depth, smoothness, arousal, and valence. The SEC subscales depth and smoothness particularly focus on addressing the perceived personal and emotional impact of the session in terms of how powerful and valuable (depth) and how emotionally easy and relaxed (smoothness) the given session was.
These concepts and measures provide a solid starting point for assessing emotional processing also in the context of art-based psychotherapies. Nonetheless, all of these models have been developed in the context of verbal/general psychotherapy, and may overlook some of the key aspects of the nonverbal levels of emotional processing characteristic to art-based therapies. Concerning emotional skills, it has been critically argued that general emotional competence models do not include the embodied-experiential access to emotions as a competence, and therefore do not provide comprehensive grounds for defining music-based emotional competence (Saarikallio, 2019). Currently, the specific components of music (or art) therapeutic emotional processing have not been clearly conceptualized or operationalized into questions that could be used in studies for assessing the relevance of emotional processing in the context of art-based therapies. This relates to the larger challenge of evidencing the mechanisms of change when discussing the impacts of music. While an increasing number of studies have demonstrated that music therapy is effective in treating depression (Aalbers et al., 2017; Maratos et al., 2008) and there is growing global evidence on the beneficial effects of arts on wellbeing (Fancourt & Finn, 2019), this field is constantly, and justly, criticized for being ambiguous about the impact mechanisms (Clarke et al., 2015).
Aim and research questions: music therapeutic emotional processing
Emotional processing has been identified as a pivotal element for achieving therapeutic change in general psychotherapy and music has been identified as an effective facilitator of emotional processing, particularly at the nonverbal and symbolic levels. Yet, there is little empirical research on which particular aspects constitute emotional processing in the context of clinical music therapy and whether the different components of this processing predict clinical outcomes. The main aim of the current study was therefore to establish a definition and operationalization for the concept of music therapeutic emotional processing (MEP) as a mechanism of action for a therapeutic change. This main aim was divided into four research questions:
What are the key components of emotional processing in clients’ experiences of music therapy sessions? To develop a conceptualization of MEP that could be empirically tested we formulated a set of self-report items that would be applicable to the context of music therapy sessions. The items were developed based on the above-described prior theories of emotional processing and clinical experience. The internal composition of the items was explored through a factor analysis and reliability tests.
Do the emergent MEP factors correlate with emotional impact of the session? Validity of the emergent factors as relevant features for assessing the emotional impact of a therapy session was then tested through correlations with the depth and smoothness subscales of the SEQ (Stiles, 1980). Positive correlations with depth were interpreted to reflect favorable MEP, since depth reflects the client’s perception of the session as valuable and powerful. Exploring correlations with Smoothness provided insight on whether the presence of a given MEP component was related to the perceived easiness of the session.
Do the emergent MEP factors predict therapeutic outcome? As a third research question, we investigated which components of MEP would predict a desirable clinical outcome of the therapy process. Desirable therapeutic outcome in the current study was determined as a greater pre-post decrease in depression scores, as indexed by the primary clinical outcome measure of the trial, the Montgomery–Åsberg depression rating scale (MADRS; Montgomery & Åsberg, 1979). Positive correlation of a given MEP component with this outcome was considered to reflect desirable MEP.
What is the temporal evolution of the MEP factors across the music therapy process? Finally, we wanted to understand whether some aspects of MEP would be more salient at different phases of the therapy process and whether their temporal curve would play a role in predicting the therapeutic outcome. Since prior research has shown that general emotional processing typically shows an increase during the first part of a successful therapy process and thereafter stabilizes, we expected this type of temporal curve to be found for the favorable MEP factors.
Overall, drawn from the abovementioned steps, this study aimed to create grounds for better conceptualizing MEP as a predictor of therapeutic outcome in music therapy for depression. The results were expected to provide concrete grounds for both therapists and researchers to assess emotional processing as a mechanism of change in the particular context of a music (or art)-based therapy process.
Method
This study was conducted as part of a clinical trial designed for studying music therapy as a treatment for depression: the clinical outcomes of the trial are reported elsewhere (Erkkilä et al., 2021). In this study, we focused on the emotional processing among the clients of the trial.
Participants
Participants were recruited through announcements placed in local newspapers. A total of 102 people were initially invited for screening, out of whom 14 declined, 11 were no-shows, and 7 met an exclusion criterion. This left 70 eligible participants (74% female), with an age range of 19–57 years (M = 39).
Inclusion criteria were to be at least 18 years of age and to have a primary diagnosis of major depressive disorder (F32/F33, International Classification of Diseases, 10th Revision [ICD-10] criteria). The diagnosis was made using the MADRS, administered by a psychiatric nurse with an MA degree in nursing science and assessment qualification. Exclusion criteria were a known history of psychosis, bipolar disorder, personality disorder, other combined psychiatric disorders in which depression cannot be defined as primary disorder, acute and severe substance misuse, and depression severity impeding clinical measurements or verbal conversation. Musical skills were neither required nor constituted a reason for exclusion.
Fifty-six participants had responses for all 12 sessions. In addition, eight participants had responses for 11 sessions. Missing data for these participants were substituted with nearest-neighbor extrapolation for the first session (one participant) and linear interpolation for intermediate sessions (seven participants). Consequently, a total of 64 participants’ data were used in the subsequent analyses.
Study design and procedures for the intervention
The trial was conducted at the Music Therapy Clinic for Training and Research, Department of Music, Art and Culture Studies, University of Jyväskylä, Finland. All participants were offered 12 biweekly sessions of IIMT, 60 min each, over a period of 6 weeks.
The trial (Erkkilä et al., 2019) was designed to test the efficacy of two additional components that could be easily integrated to the general IIMT model: a breathing exercise at the beginning of each therapy session (resonance frequency breathing) and a homework task (listening to music therapy improvisations recorded in the sessions). Following a 2 × 2 factorial design, clients were randomly allocated to one of the four conditions via random integer generator. All clients in every condition received IIMT. The presence or absence of added components was not considered relevant for the purpose of understanding emotional processing as part of music therapy. Therefore, in this study, the clients in all four conditions were treated as one participant group.
The clinical setting was the same for every client. Digital pianos were used for melodic and harmonic improvisations, two pianos placed opposite to each other (one for the client, one for the therapist). Djembe drums were used for nonmelodic, rhythmic improvisations and placed next to the pianos. No other instruments or music therapy methods were used.
Eleven qualified and clinically experienced music therapists (five female, six male) were responsible for conducting the therapy sessions. To ensure treatment fidelity, the clinicians were offered intensive training in IIMT prior to the trial and regular clinical supervision was used for monitoring and maintaining the quality of the clinical work during the trial.
Data for the primary outcome measure of the trial (MADRS) were collected pre- and post-intervention. Data for MEP and the assessment of session impact (SEQ) were collected at the end of each session. Details of the measures are described.
Measures
The measurement of MEP required new item development, as no prior instrument for assessing MEP exists. A set of 19 items was formulated to reflect clients’ experiences of emotional processing as part of a music therapy session. Item development was based on the prior theory and knowledge on emotion processing and music therapy clinical practice as presented in the introduction. Thus, the items were designed to correspond to emotions being activated (experiencing emotions and related images, memories; e.g., Bruscia, 1998; Greenberg & Pascual-Leone, 2006), expressed (playing emotions through music, sharing emotions; e.g., Bruscia, 1998; Erkkilä, 2004, 2013; Erkkilä et al., 2012), regulated (ability to approach difficult emotions, not being stuck or overwhelmed by emotions, gaining relief; e.g., Auszra et al., 2013; Greenberg & Pascual-Leone, 2006) and properly reflected upon (gaining new insight and understanding; e.g., Erkkilä et al., 2012; Hayes et al., 2005; Hunt, 1998; Klein et al., 1986; Stiles, 1980). Most items were formulated to be generic, that is, not music-specific (e.g., “I understood why I feel a certain way”), but some were embedded in the musical activities of the sessions (e.g., “There were strong emotions in my playing”). Overall, the items were reflective of IIMT as a therapy model (Erkkilä, 2004, 2013; Erkkilä et al., 2012): (a) music serving as a trigger and a symbolic, nonverbal expression of emotionally charged experiences, and (b) these experiences further being verbally processed with the therapists for conscious meaning-making and insight. The list of the 19 items is presented in Appendix 1.
The perceived value of the music therapy session was assessed with the depth and smoothness subscales of the SEQ. SEQ is a self-report instrument designed to evaluate the client’s post-session mood and perceived therapeutic impact of the session (Stiles, 1980; Stiles & Snow, 1984). It consists of 21 seven-point bipolar adjective scales, regrouped into four independent dimensions: Positivity and arousal for the client’s affective state, and depth and smoothness for the perceived personal and emotional impact of the session. To keep the session-by-session reporting concise, only depth and smoothness, which provide insight on the emotional impact of the session, were used in this study. Depth is an expression of both the session’s potency (powerful-weak) and value (valuable-worthless), while smoothness expresses whether the session was experienced as relaxed and easy, as opposed to tense and difficult. A complete list of the adjective pairs is as follows: depth: valuable–worthless, shallow–deep, full–empty, weak–powerful, special–ordinary. Smoothness: difficult–easy, relaxed–tense, unpleasant–pleasant, rough–smooth, comfortable–uncomfortable.
The MADRS is a diagnostic questionnaire designed to assess the severity of depression (Montgomery & Åsberg, 1979). It consists of 10 items, assessing apparent sadness, reported sadness, inner tension, reduced sleep, reduced appetite, concentration difficulties, lassitude, inability to feel, pessimistic thoughts, and suicidal thoughts. The questionnaire is completed by a clinician during an interview with the patient. Each item is scored from 0 to 6. Consequently, the overall score can range between 0 and 60. A score above 7 indicates mild depression, above 20 indicates moderate depression, and above 34 indicates severe depression.
Analysis
To identify latent dimensions in the MEP questionnaire data, we applied maximum likelihood Factor Analysis with varimax rotation to all responses to the 19 MEP items. The thus obtained factors were correlated with the SEQ subscales by correlating the temporal means of the former with those of the latter. The degree to which the MEP factor scores could predict decrease in depression during the therapy process was assessed by correlating the temporal averages of the MEP factor scores with the MADRS changes scores obtained by subtracting the post-therapy MADRS score from the pre-therapy one. A positive MADRS change score thus indicates a decrease in depression level.
To model the time course of evolution of the MEP factor scores during the therapy process, we applied, for each factor separately, power regression using the model

where t denotes the session number and
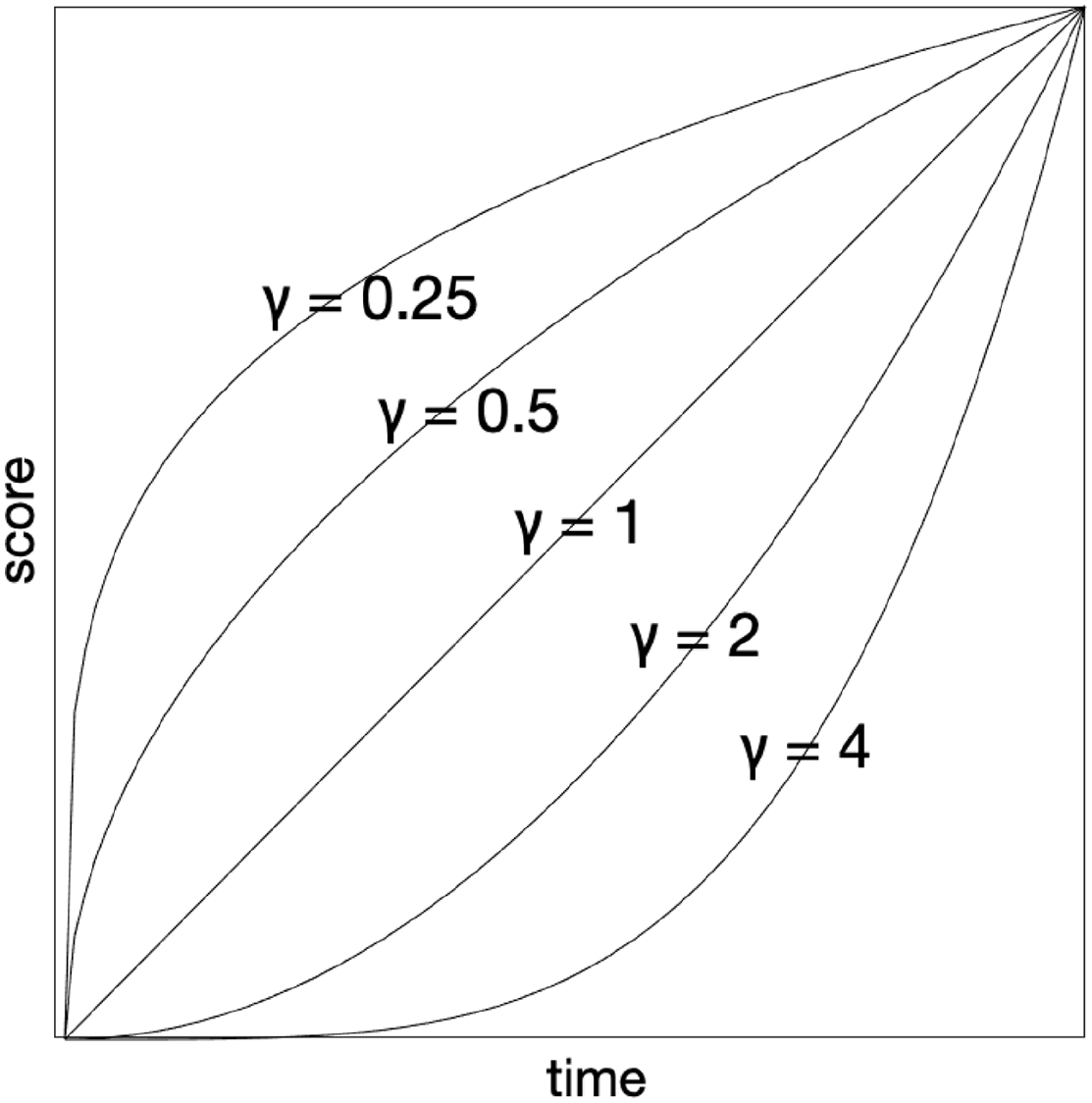
Power Regression Models of Equation (1) with a Positive
To obtain more detailed accounts of the temporal evolution, we computed regression models for three ranges of therapy sessions: all sessions (1–12), the first half of the sessions (1–6), and the second half of the sessions (7–12). These session ranges are subsequently referred to as “Whole,” “Start,” and “End.” We considered the power term as a fixed effect (common for all participants) and estimated it, separately for each factor, by maximizing the mean coefficient of determination across participants. Subsequently, using the optimal exponent obtained for each factor and modeling range, we investigated, for each factor, the beta coefficients to elucidate the time course of evolution of each factor.
Results
A descriptive overview of all MEP items is presented in Figure 2. The item numbers correspond to the items listed in Appendix 1. The mean scores of the 19 items, averaged across participants, are presented in a bar chart, in which the bar clusters represent ratings provided to the given item in each of the 12 therapy sessions. From visual inspection it can be seen that, for instance, the item number 11 I was able to share my emotions with the therapist receives high ratings overall and the ratings even appear to increase as the therapy progresses. Meanwhile, items such as 10. I felt emotionally numb, 13. I felt stuck with certain emotions, and 17. I was emotionally overwhelmed all receive relatively low ratings and the ratings seem to rather decrease than increase across the therapy process. After this initial inspection, we move forward to the analyses.
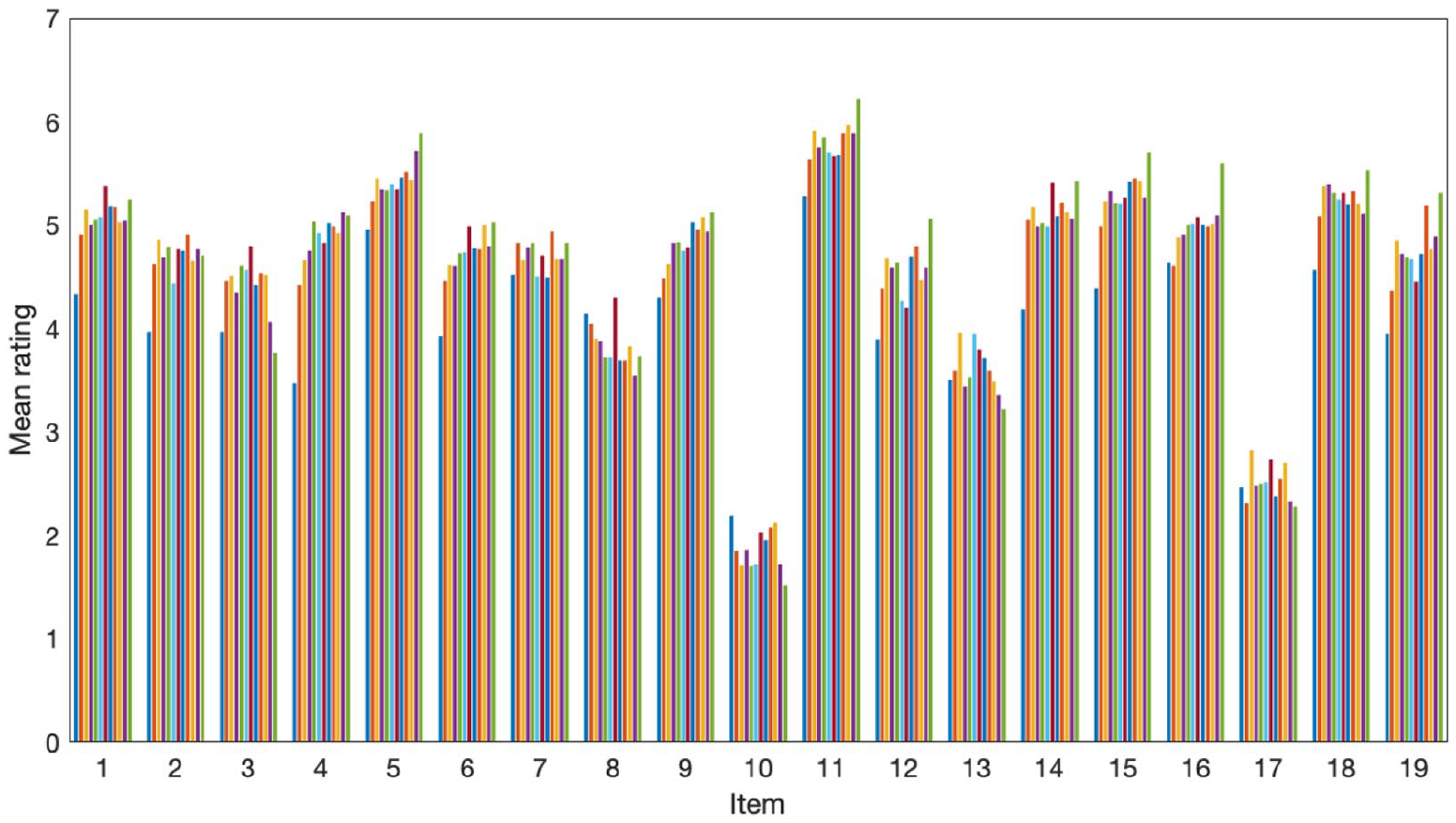
Mean Ratings of the 19 Original MEP Items in the 12 Therapy Sessions.
Factor analysis on MEP questionnaire scores
The first research question aimed at identifying the key components of MEP. To identify latent dimensions in the data, we applied factor analysis to all the responses to the 19 MEP items (64 participants × 12 sessions). First, to determine the number of factors, we applied Cattell’s (1966) scree test and Velicer’s minimum average partial test (Velicer et al., 2000). Cattell’s scree test is a graphical method based on determining the point at which the eigenvalues of successive principal components level off to the right of the plot. Velicer’s s minimum average partial test is a numerical method that aims to determine the number of components that consists primarily of common variance in the data. To this end, it finds the number of components m for which the partial correlation matrix (i.e., correlation matrix from which the first m components have been partialed out) has minimal norm. Cattell’s and Velicer’s tests were chosen because they have been found to be among the most accurate graphical and numerical methods, respectively (Peres-Neto et al., 2005; Velicer et al., 2000). Both tests suggested three factors, containing 61% of total variance (eigenvalues 18.00, 9.78, 2.95).
The loadings for the 19 MEP items are shown in Table 1. After investigation of the factor loadings, the factors (subsequently referred to as the MEP factors) were labeled awareness, expression, and pain. The labeling of the factors was data-driven, grounded in the high-loading items of each factor. The first factor was labeled awareness, because it received high loadings from items referring to an increased insight and understanding of one’s emotional behavior. The second factor was labeled expression, because it received high loadings from items reflecting the expression of strong personal emotions in one’s musical playing. Finally, the third factor was labeled pain, because it received high loadings from items reflective of difficult, unsettling, and overwhelming emotional sensations, becoming carried beyond one’s window of tolerance, and items designed as reversed ones for managing emotions. Awareness and expression were thus clearly reflective of theoretically favorable aspects of emotional processing, while pain was reflective of the favorable aspect of being able to face painful and difficult emotions, but also of the nonfavorable aspect of over-engagement/nonregulation. In Table 1, items with factor loadings greater than 0.7 for their respective factor have been indicated with boldface to highlight the most illustrative statements of each factor.
Factor Loadings for the Music Therapeutic Emotional Processing Items.
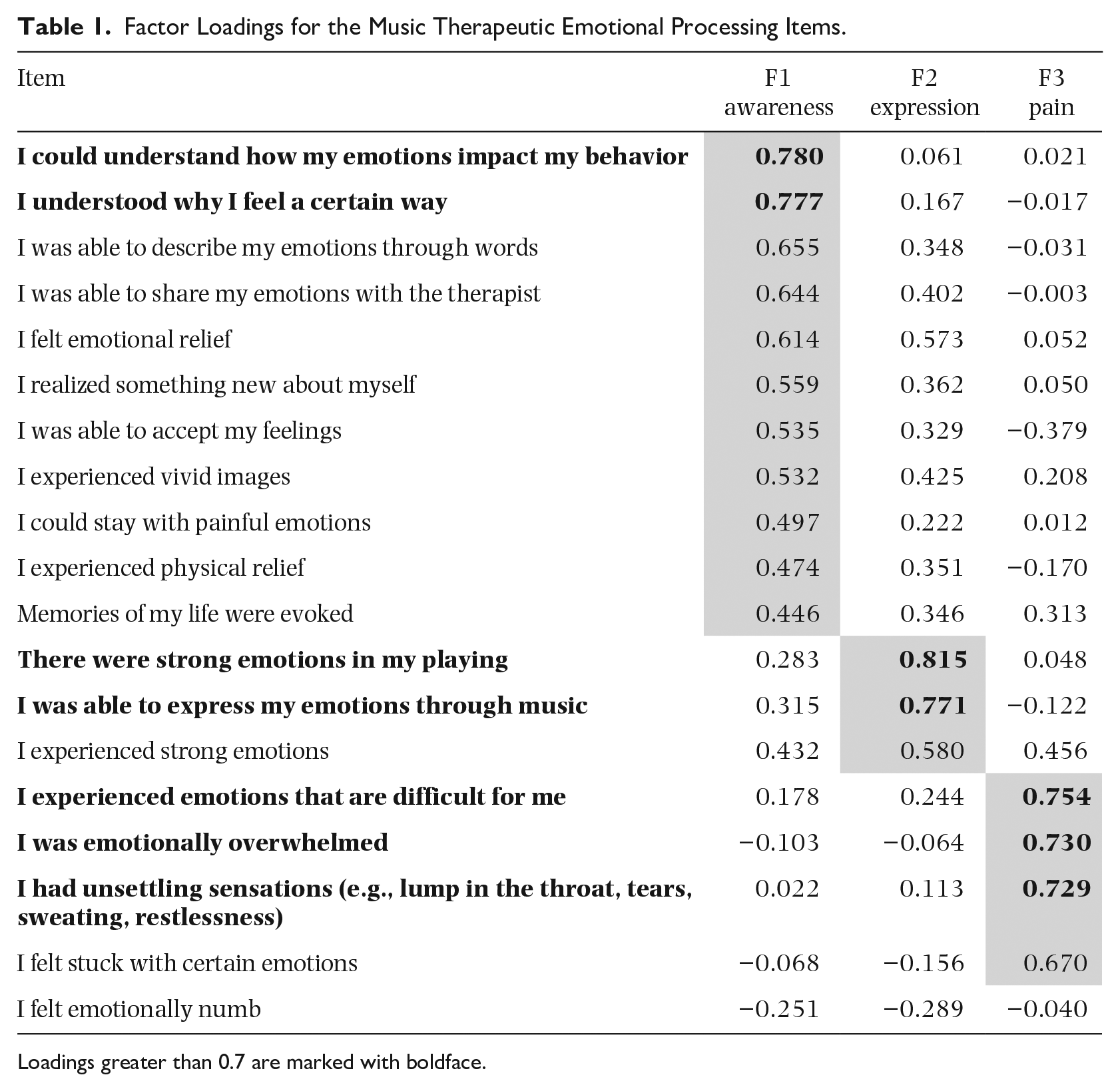
Loadings greater than 0.7 are marked with boldface.
The internal consistency reliability of the emergent factors was inspected with Cronbach’s alphas. When choosing items loading high (above 0.40) on their respective factor (indicated with a gray background in Table 1), the alpha coefficients were .903 for awareness, .840 for expression, and .812 for pain. When choosing only the most illustrative items of each factor (loadings greater than 0.70, cross-loadings lower than 0.40 with other factors, bolded in Table 1), the alpha coefficients still remained at acceptable levels with .796 for awareness, .837 for expression, and .783 for pain. The findings confirmed the structural clarity of the emergent three-factor solution, and the factor scores for each of the three factors were used in subsequent analyses.
MEP factor scores and SEQ subscales
The second research question focused on investigating whether and how the emergent MEP factors would relate to the general emotional impact of a therapy session. Awareness, expression, and pain were correlated with the depth and smoothness scores of the SEQ. To this end, we averaged, for each participant, all scores across the sessions.
The correlations between the temporal means are presented in Figure 3. Awareness, r = .759, p < .001, and expression, r = .805, p < .001, both showed strong, significant positive correlation with depth, thus providing support for these factors as being favorable aspects of MEP. In addition, Smoothness showed smaller but significant correlations with all MEP factors, correlating positively with awareness, r = .513, p < .001, and expression, r = .483, p < .001, and negatively with pain, r = –.523, p < .001. Significance estimations were based on a two-tailed test.
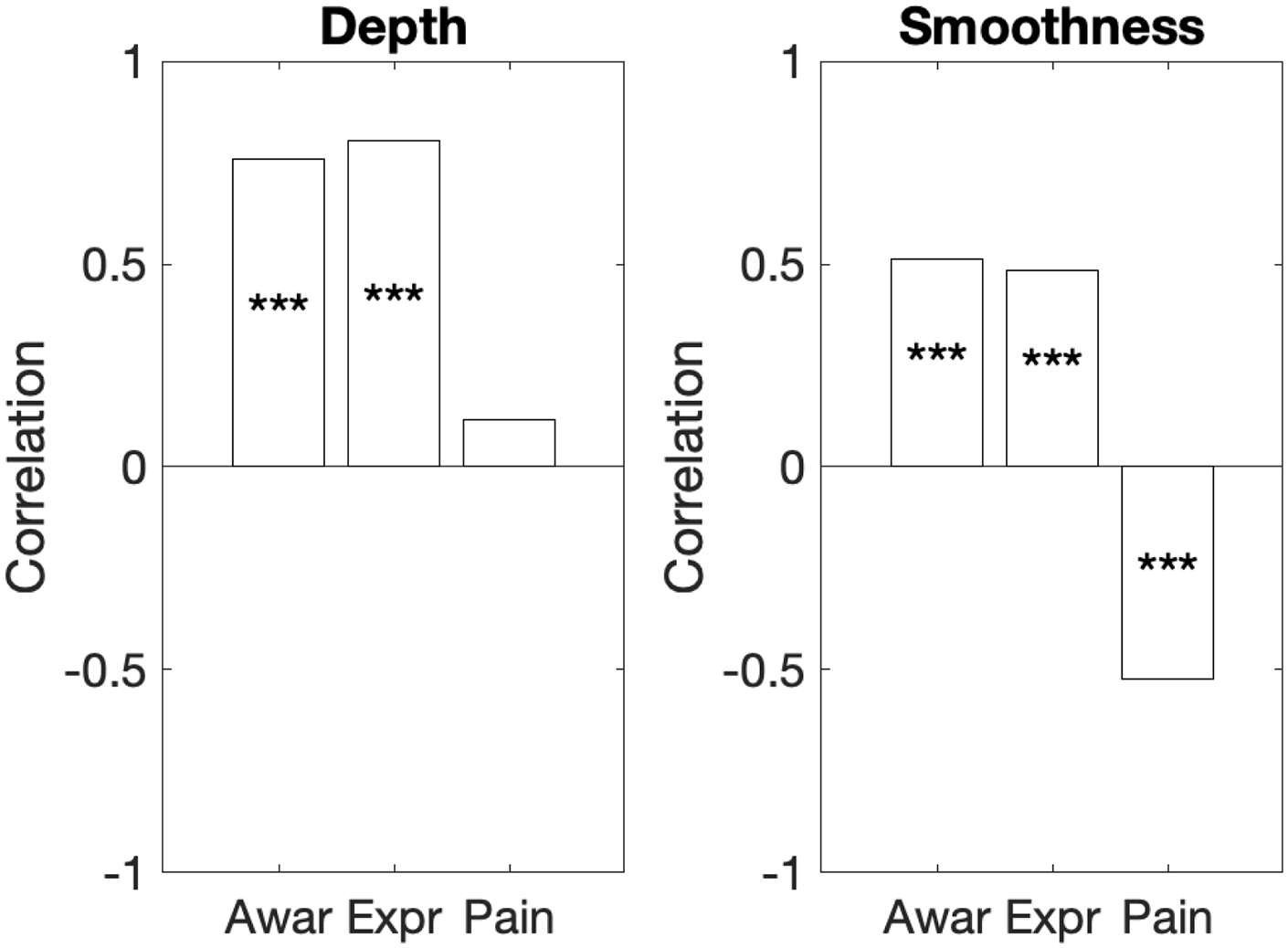
Correlations Between the Temporal Means of MEP Factors and the Temporal Means of the SEQ Subscales.
Mean MEP factor scores and MADRS change
The third research question addressed the connection of the MEP factors to the clinical outcome. To assess the extent to which the overall level of awareness, expression, and pain during the therapy process predicted decrease in depression level, each participant’s MEP factor scores were averaged across the 12 sessions and the thus obtained temporal averages were correlated with the MADRS change score. Awareness, expression, and pain were found to correlate .231, .264, and –.229, respectively, with MADRS change (all p values <.05, one-tailed). The results demonstrate awareness and expression as favorable aspects of MEP in terms of predicting the desired therapeutic outcome, while the presence of pain may even predict a negative outcome.
Temporal evolution of MEP factor scores
The final research question addressed the temporal evolution of the MEP factors across the therapy process. Figure 4 displays the mean scores across participants as a function of session number for awareness, expression, and pain. As can be seen, awareness and expression tend to follow similar kinds of trajectories, with a sharp increase in the beginning followed by a somewhat slower increase toward the end of the process. Pain, on the other hand, shows an entirely different trajectory which is characterized by more fluctuation between subsequent sessions and a roughly inverted U shape.
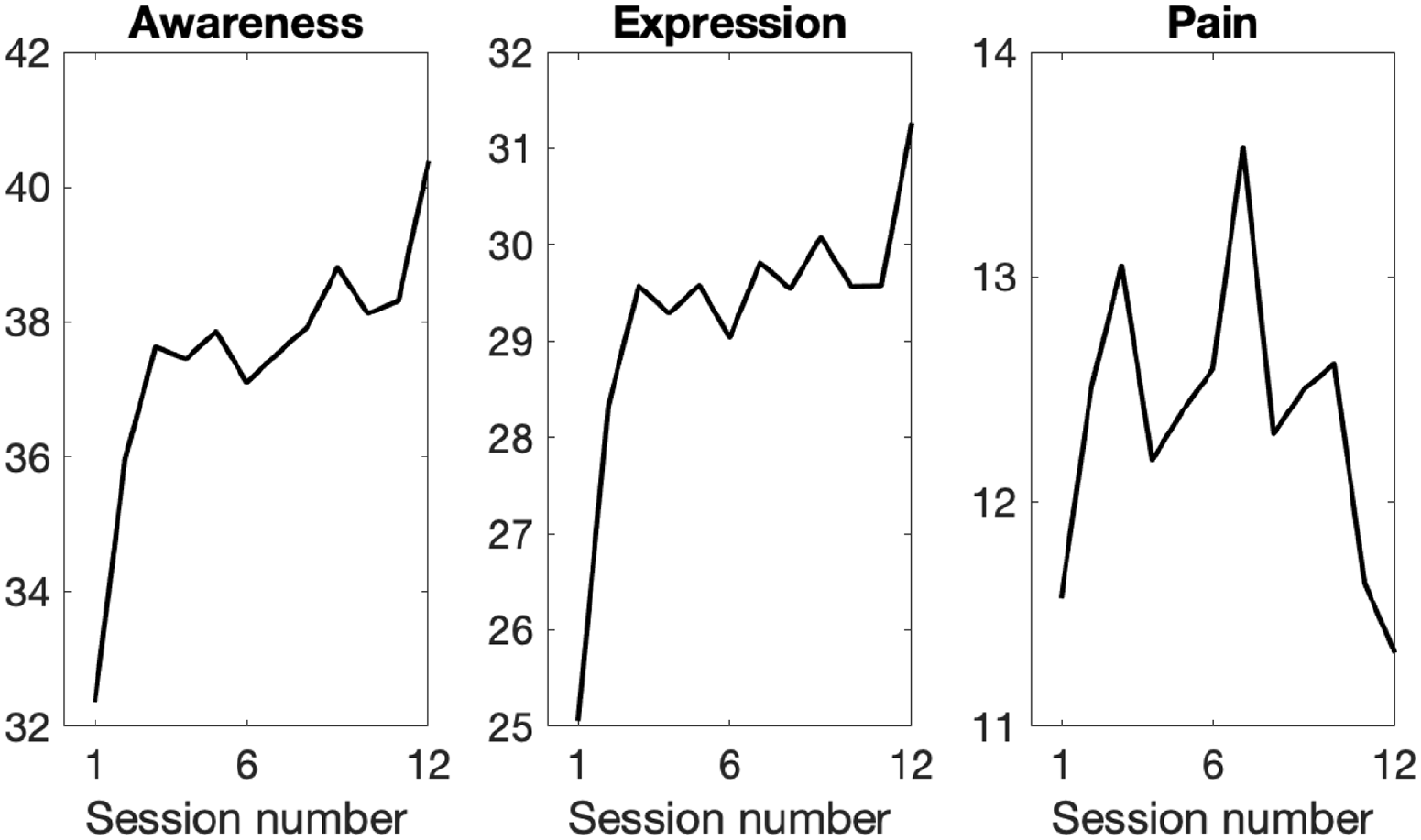
Mean Scores Across Participants for the MEP Factors.
Figure 5 shows the mean models, obtained by averaging, separately for each factor and modeling range, the model parameters across participants
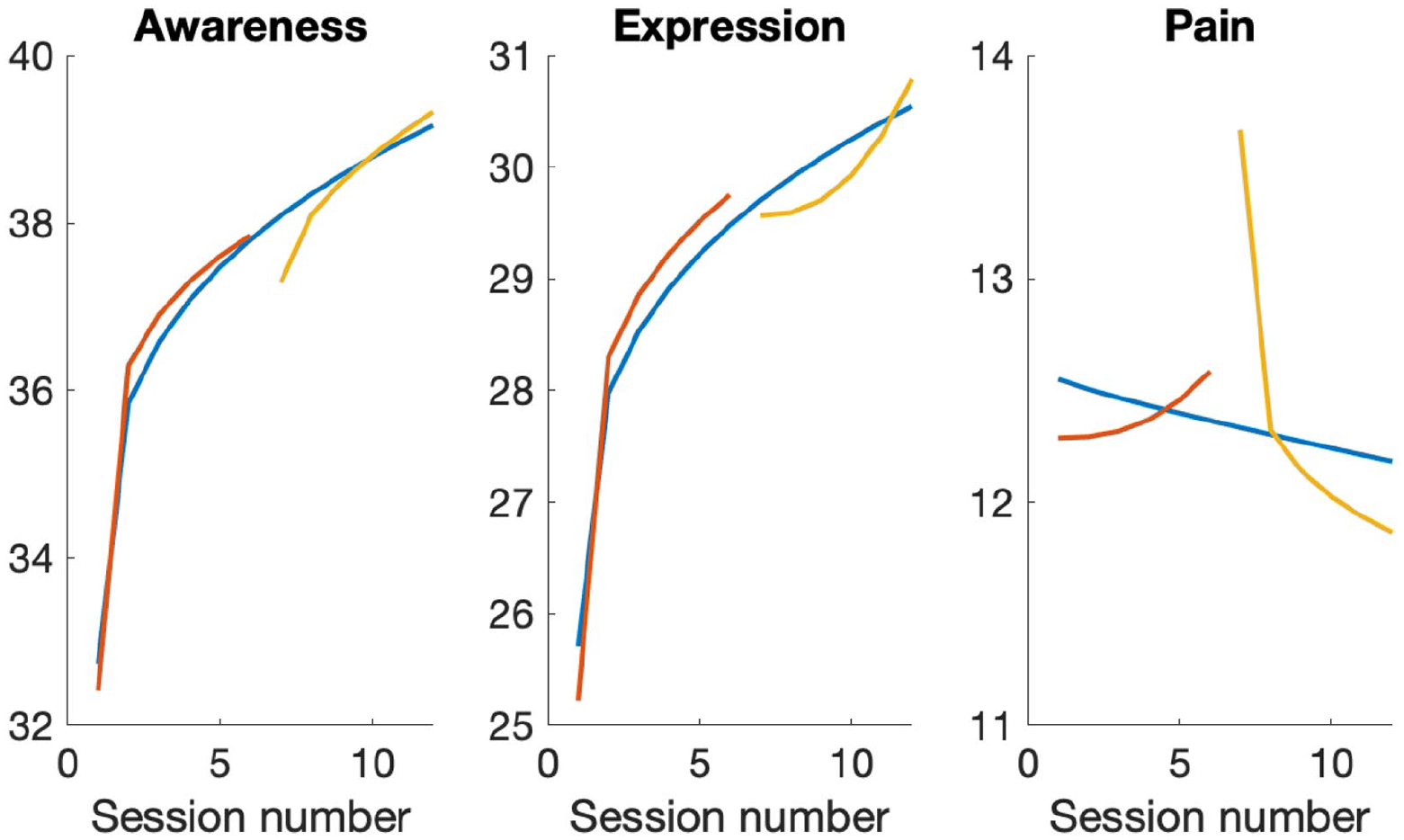
The Average Models for the Three Factors and Three Modeling Ranges.

where
Temporal evolution of MEP factor scores versus depression change
Finally, to investigate the association between the MEP scores during the different stages of the therapy process and the change in depression levels, we divided the process into three parts (sessions 1–4, 5–8, and 9–12), averaged the MEP factor scores within each part, and subsequently performed partial correlation analyses between the MADRS change score and the averaged factor scores of each of the three parts.
The results are displayed in Figure 6. Each MEP factor demonstrates a somewhat different temporal correlation profile with MADRS, although the effect sizes are small. For pain, low pain scores particularly at the end of the process significantly predict positive therapeutic outcome, while pain levels at the start and middle play no role. The importance of high scores in awareness and expression for predicting positive therapeutic outcome seems to gradually increase toward the end of the therapy process, particularly for awareness, but these remain as nonsignificant trends.
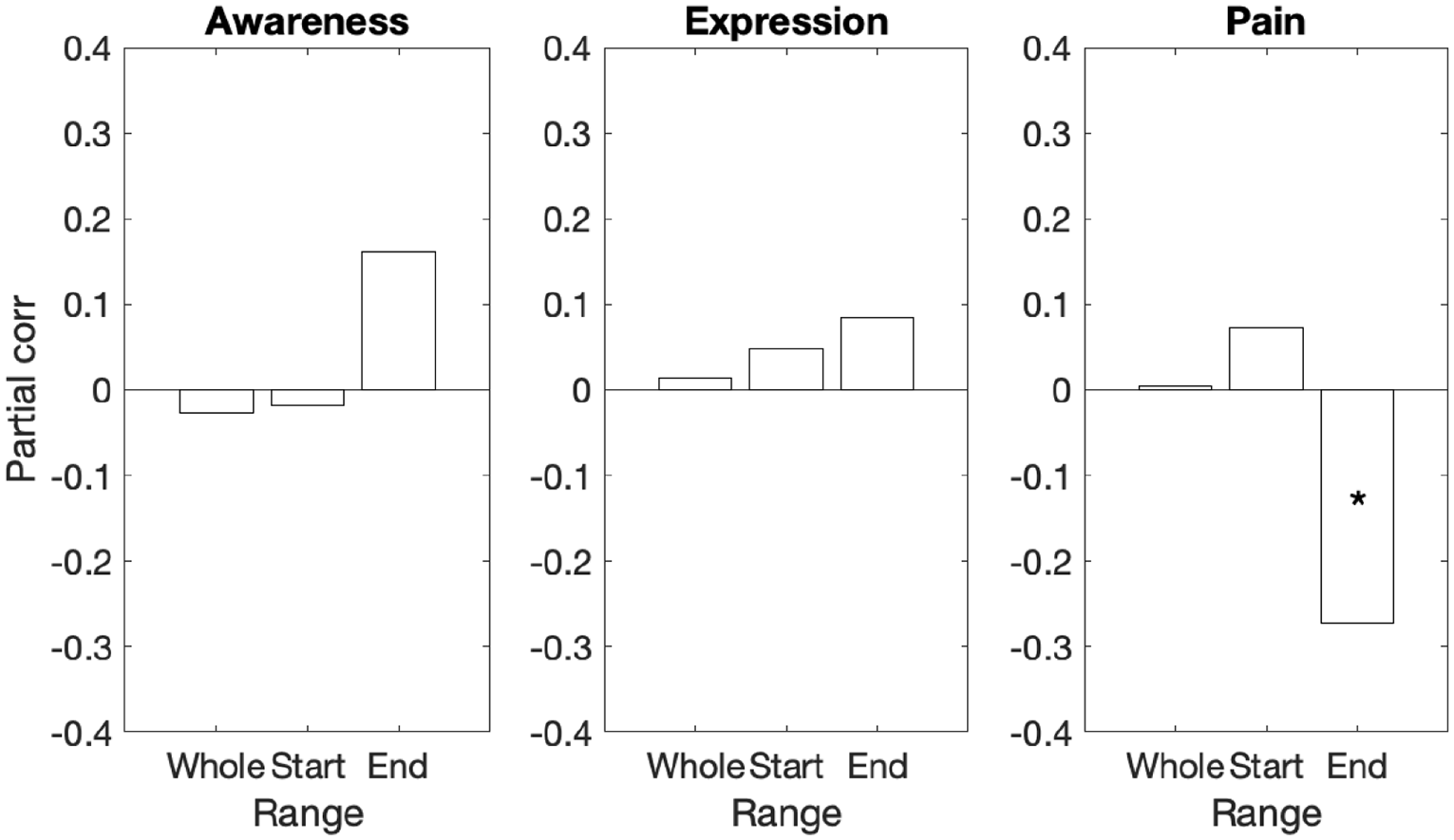
Partial Correlations Between MADRS Score Change and MEP Factor Scores for Start, Mid, and End Parts of the Therapy Process (*p < .05, Two-Tailed).
Discussion
Our study provides novel insight for the concept of MEP. The emergent MEP components, expression, awareness, and pain demonstrated distinctive profiles, in terms of their connection to the perceived impact and value of the session (depth and smoothness), their predictive potential concerning the therapeutic outcome (depression), and their temporal curves of how they evolved across the therapy process. The results establish musical expression of emotions (expression) and personal awareness of emotional experiences (awareness) as central aspects of favorable MEP.
The three-dimensional conceptualization of MEP is somewhat less fine-grained than some of the theoretically proposed models of general emotion processing, which may consist of up to seven components (Auszra et al., 2013; Greenberg & Pascual-Leone, 2006; Greenberg & Safran, 1989). However, MEP components do encompass most of the more fine-grained concepts of prior theoretical models of emotion processing. Expression includes aspects of attending, activating, intensifying, and even symbolizing emotions, while Awareness contains aspects that relate to analyzing, accepting, and meaning-making. Pain can be considered as a combination of arousal and intensification, yet also over-engagement (indicating nonregulation).
Expression and awareness emerged as the clearly favorable components of MEP. Both demonstrated positive correlations with depth and smoothness evaluations of the sessions and with greater recovery from depression as the therapeutic outcome. Both components also demonstrated an increase across the whole therapy process, with the sharpest increase occurring already during the early phase of the process. Such temporal curve of an early increase and later stabilization of the intensity of emotional processing has been linked to the success of a therapy process also in prior studies addressing both cognitive-behavioral and process-experiential therapy methods (Dörig, 2014; Hayes, 2015; Watson & Bedard, 2006). The two-dimensional definition of favorable emotional processing into components of expression and awareness is also perfectly in line with the theoretical grounding of the IIMT model, in which sessions are based on a dialogue of triggering emotional experiences through the musical expression that occurs during clinical improvisations (expression) and then further processing these experiences in the verbal domain for meaning formation (awareness; Erkkilä, 2004, 2013; Erkkilä et al., 2012). While this study was conducted in the context of IIMT-based therapy in particular, the findings hold wider relevance as this basic principle of how art functions as part of a therapy process is common to many other forms of experiential psychodynamic art therapies (Bruscia, 1998; MacDonald & Wilson, 2014).
The role of pain as an MEP component is more complex. Pain correlated negatively with the smoothness evaluation of the sessions and the temporal mean of pain was observed to correlate negatively with recovery from depression. However, pain did not show negative correlation with the depth of the sessions and when investigating how MEP components correlate with the therapeutic outcome it was found that, when dividing the therapy process into early, mid, and late phases of therapy, the correlations with the poorer therapeutic outcome were observed only for the presence of pain during the last (9–12) sessions. Overall, pain showed an inverted u-shaped curve across the therapy, typically being strongest at the middle phase of the process. It seems that while the presence of pain does not seem to be particularly beneficial for the therapy process, its presence during the early and middle phases of the therapy does not seem to be harmful either. Such observed nonharmfulness of painful experiencing in a music therapy process holds some resonance with prior accounts of music as a realm of accessing difficult emotions in a symbolic, self-detached, and bearable manner (Frijda & Sundararajan, 2007; Garrido & Schubert, 2011; Vuoskoski & Eerola, 2017). Only if pain continued to be present until the end of the therapy process, it predicted a poor therapeutic outcome. This finding potentially suggests that clients who began to experience pain toward the end of the therapy would have needed a longer clinical process. It must be noted that the current study was based on a short 6 week therapy trial, while IIMT therapies in real life often last somewhat longer. Inability to adjust the length of the therapy to the speed of how emotional processing evolves in each client can be seen as a limitation in terms of ecological validity of this type of trials.
Together, the findings of this study offer important new knowledge on the role of the different components of emotional processing—expression, awareness, and pain—within the frame of music therapy as clinical psychotherapy. Psychotherapy models range from psychoanalytic to humanistic and cognitive-behavioral ones and do have somewhat different grounds, for instance, in terms of how to consider the role of negative emotions and how deeply the traumatic experiences and psychohistory are to be addressed (Dryden, 2007). As an integrative model, IIMT regulates—according to the client’s situation, starting-points, and needs—its orientation between the analytical approach of going through, interpreting, and becoming aware of the meanings of emotional experiences and the short-term psychotherapy approach that does not emphasize the depth of processing but supportive, resource-orientated working style instead. IIMT represents a somewhat unique type of therapy, which enables and boosts deep emotional processing even within a short-term time frame if a client has capacity and willingness to it. We have noticed that in IIMT, music-based emotional processing sometimes tends to deepen the therapy quickly even without conscious aspiration to it both from the therapist’s or client’s side. Unlike many may assume, improvisational working often triggers painful emotions and according to our clinical observations, may do it sometimes in an unexpected way to which a client has not necessarily prepared herself/himself. According to analytical psychotherapy tradition, going through such painful experiences may be of therapeutic benefit and, thus, avoiding pain in psychotherapy is not self-evidently a goal. In the light of our findings, expressing and becoming aware of emotions seems to also include pain, which, however, goes away or diminishes toward the end of the therapy for those patients who benefit from therapy. A possible conclusion here is that pain has served therapeutic processing and perhaps acted as a mediator for improvement. With those clients, with whom the pain does not diminish toward the end of the therapy, a question remains whether the therapy process has been too short for them, or whether the therapeutic process has not been optimal in terms of pain regulation.
Our observations of both the music-based expression and the awareness of personal experiences emerging as central components of favorable MEP consolidate and refine current understanding of the integral working mechanisms of IIMT as a psychotherapy model. In terms of implementation, the MEP components identified in this study offer a clear conceptual frame for assessing music therapeutic emotional processing in both research and clinical practice. Such conceptual clarification is essential for the larger endeavor of understanding the impact mechanisms of art therapies. Our findings also offer preliminary grounds for further operationalization and measure development. The highest-loading item statements of each MEP component, bolded in Table 1, present a preliminary set of seven items that could be developed into a theoretically solid and easy-to-administer self-report instrument, through further testing and clinical validation. The items that, based on this study, can be recommended for such future work are listed in Appendix 2.
Finally, our findings provide theoretical grounding and new avenues also for the scientific inquiry into how music functions as an emotional resource in people’s everyday life. The role of music as a facilitator of emotional processing in terms of increased awareness and insight into one’s personal experiences has been observed by several researchers studying music as emotional self-regulation of daily life (Baltazar & Saarikallio, 2016; DeNora, 2001; Saarikallio & Erkkilä, 2007; Schäfer et al., 2013). Use of adaptive musical self-regulation strategies such as cognitive reappraisal have been proposed to explain the positive impact of music on everyday wellbeing (Chin & Rickard, 2013; Miranda et al., 2012), while, as a contrast, musical self-regulation that relies on inefficient regulation strategies is considered to be less effective or even maladaptive (Marik & Stegemann, 2016; Miranda & Claes, 2009; Saarikallio et al., 2015). In light of the current findings, it would be exciting to investigate what kind of relevance does the presence of expression, awareness, and pain hold for explaining the short- and long-term emotional impacts of music also in the context of daily life.
Footnotes
Appendix 1
Appendix 2
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was financially supported by the Academy of Finland (project numbers 298678, 346210, 332331).