
Abstract
The integration of three-dimensional (3D) printing technology has profoundly transformed contemporary orthodontic practice by enabling highly customized, precise, and efficient digital workflows. This review aims to provide a comprehensive overview of the evolution, principles, clinical applications, and future prospects of 3D printing in orthodontics. The transition from conventional plaster models and laboratory-dependent procedures to digital intraoral scanning, computer-aided design and manufacturing (CAD–CAM), and additive manufacturing has enhanced diagnostic accuracy, treatment predictability, and patient comfort while reducing chairside time and laboratory turnaround. Various 3D printing technologies, including stereolithography, fused deposition modelling, digital light processing, selective laser sintering, and PolyJet printing, are discussed with respect to their orthodontic applications, advantages, and limitations. Current clinical uses encompass printed study models, aligners, customized brackets, archwires, functional and expansion appliances, surgical splints, fixation plates, and presurgical nasoalveolar molding devices. Recent advances such as compliance-monitoring appliances, integration of artificial intelligence, and emerging concepts of 4D printing further highlight the expanding scope of this technology. Despite challenges related to material properties, cost, regulatory approval, and long-term clinical validation, 3D printing represents a paradigm shift toward fully digital, patient-specific orthodontic care.
Keywords
Introduction
Modern orthodontics has undergone a significant transformation with the integration of digital technologies aimed at overcoming traditional communication barriers, optimizing treatment planning, enhancing patient care, and improving clinical efficiency. Today’s orthodontist has access to a wide range of digital documentation tools that support accurate diagnosis, effective treatment planning, and continuous treatment monitoring. Conventional imaging techniques have largely been replaced by digital radiography and photography, while cone beam computed tomography (CBCT) has become increasingly indispensable across multiple orthodontic applications. 1
Simultaneously, traditional plaster study models are rapidly being replaced by digital models due to their improved accuracy, quick data gathering, convenience of storage, smooth digital data transfer, easier orthodontic analysis, and capacity to create virtual treatment setups. Treatment options have greatly increased due to the quick development of technical advancements, especially in orthodontic materials, bracket design, and three-dimensional (3D) applications. These advancements have made it possible to manage borderline orthodontic cases to non-extraction by employing improved diagnostic methods, and advanced materials and techniques.2, 3
Among the most influential developments in contemporary orthodontics is the adoption of 3D modeling and printing technologies, which have shifted laboratory workflows from traditional manual processes to fully digital environments. Additionally, advances in intraoral scanning technology have eliminated the need for conventional impressions, enhancing patient comfort while improving appliance accuracy and reducing treatment duration. 4 The synergistic use of intraoral scanners and 3D printers represents a major paradigm shift in orthodontics, paving the way toward a more efficient, precise, and patient-centered digital practice. 5
History
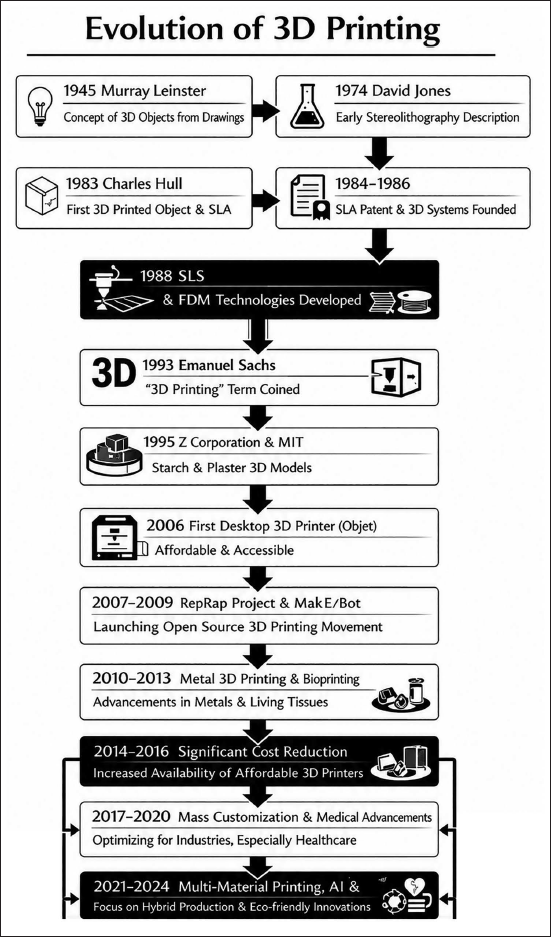
The origins of 3D printing can be traced to Murray Leinster’s 1945 short story Things Pass By, which envisioned a machine capable of converting drawings into 3D objects using melted plastic. In 1974, David Jones conceptually described stereolithography, laying the theoretical foundation for additive manufacturing. The first successful 3D-printed object was produced in 1983 by Charles Hull, who subsequently patented stereolithography in 1984 (approved in 1986) and founded 3D Systems. Fused deposition modeling (FDM) and selective laser sintering (SLS) emerged in the late 1980s. In 1993, Emanuel Sachs coined the term “3D printing,” and in 1995, ZCorp commercialized MIT’s binder-based printing technology. The early 21st century marked increased accessibility with the introduction of affordable desktop printers and open-source initiatives such as RepRap and MakerBot. Since 2010, advances in metal printing, bioprinting, and digital workflows have driven widespread clinical and industrial adoption. From 2021 onward, integration of artificial intelligence, multi-material printing, and biocompatible resins has further expanded the application of 3D printing in healthcare, particularly in orthodontics for customized appliance fabrication (Figure 1).
Evolution of Three-dimensional (3D) Printing.
Traditional Versus Digital Workflow
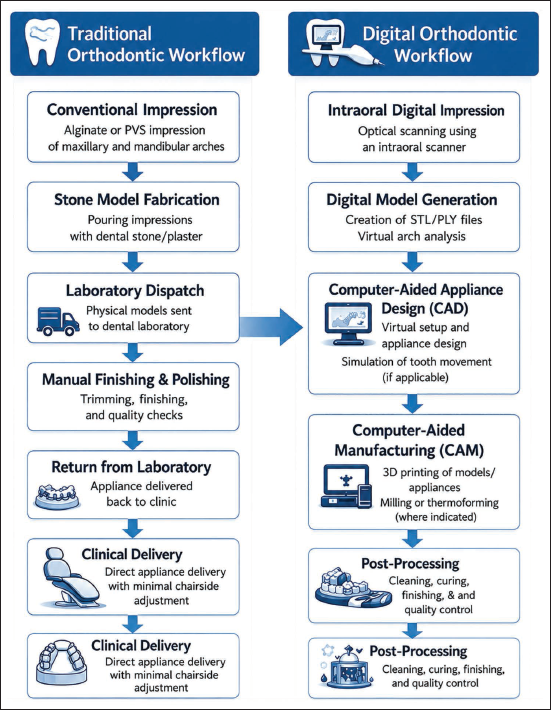
The comparative schematic of the traditional orthodontic workflow and the digital orthodontic workflow, highlighting the transition from conventional, laboratory-dependent procedures to a streamlined digital process. The traditional orthodontic workflow begins with a conventional impression using alginate or polyvinyl siloxane to record the maxillary and mandibular arches. The impression is used for stone model fabrication, followed by laboratory dispatch, where physical models are sent to the dental laboratory. After manual finishing and polishing, the appliance is returned to the clinic for clinical delivery, which includes try-in, adjustments, and placement. Any further modifications require returning the appliance to the laboratory, making the process time-consuming and technique-sensitive (Figure 2).
Whereas the digital orthodontic workflow starts with an intraoral digital impression obtained using an intraoral scanner. This data are used for digital model generation, allowing virtual arch analysis. Computer-aided design (CAD) is then performed for virtual appliance setup and simulation of tooth movement. The designed appliance is fabricated using CA manufacturing (CAM) techniques such as 3D printing, milling, or thermoforming. After post-processing, which includes cleaning, curing, and quality control, the appliance is delivered clinically with minimal chairside adjustments. Overall, the image emphasizes how digital workflows enhance accuracy, efficiency, customization, and predictability, while reducing laboratory turnaround time compared to traditional orthodontic methods—making digital orthodontics highly relevant in modern clinical practice. 7
Refined Comparison of Traditional and Digital Orthodontic Workflows in the Orthodontic Office.
Definition
3D fully programmed appliances are orthodontic devices that are digitally designed and fabricated based on the specific anatomy of each patient.
Three-dimensional Printing Procedures
In reality, either scanning an existing physical object or building a virtual model in a computer are the first steps in the 3D printing process. Slicing software instantly transforms the point cloud into a stereolithographic file, which is subsequently sent to an additive manufacturing machine to build the object. The following steps are included in the 3D printing process:
Digital scanning. Processing digital model. 3D model printing.
Digital Scanning
Digital cast models can be produced either by direct or indirect techniques. The direct method uses intraoral scanners, and the indirect method uses either laser scanning or computed tomography imaging of the impression or plaster models. The scans are then transformed into digital pictures and kept on the manufacturer’s server.8, 9 Gandedkar et al. highlight the role of advanced 3D diagnostic tools, including non-contact surface laser scanning, in comprehensive craniofacial care. The importance of accurate surface imaging for diagnosis, treatment planning, and multidisciplinary management of craniofacial anomalies using laser surface scanning. 9
Processing Digital Model
Standard tessellation language (STL), the worldwide format for 3D printing data, was first created by Chuck Hull and is utilized to build a digital model of the object using an intraoral scanner. The file is subsequently processed and made ready for printing using CAD/CAM software. 10 In the 3D printing process, the STL file is arguably the most crucial component. Due to its simplicity, it has certain limitations, such as simply specifying surface geometry, lacking color representation, and allowing only one color to be printed on the things. Furthermore, STL does not offer file security, copyright information, or surface mesh error detection. Another open file format is polygon file format (also known as the Stanford triangle format), which is useful when color and/or transparency information is needed. 3
Three-dimensional Model Printing
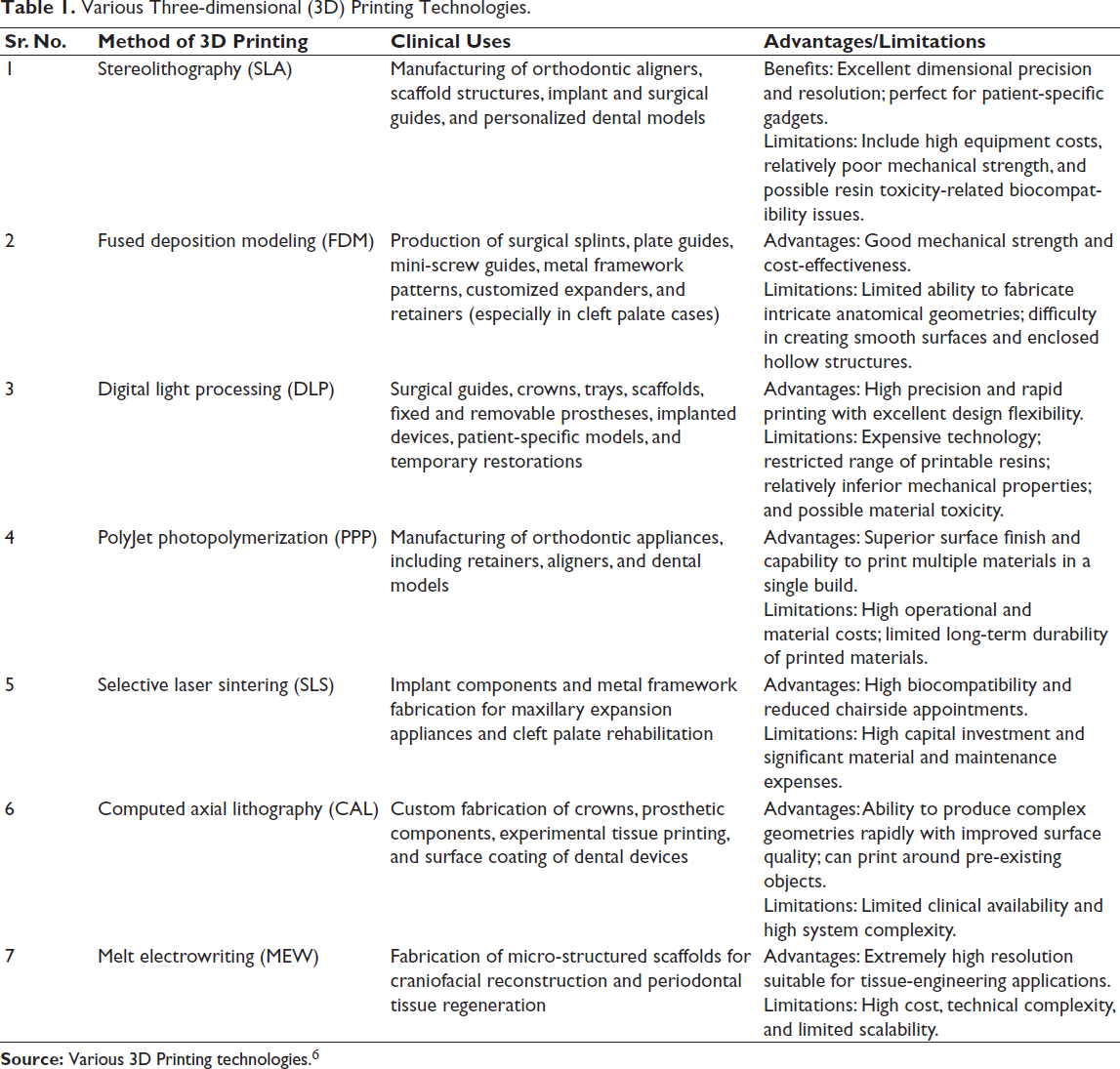
A wide variety of 3D printing technologies are currently used in orthodontics, and their respective uses, benefits, and drawbacks are summarized in Table 1.
Various Three-dimensional (3D) Printing Technologies.
Orthodontic Three-dimensional Printers
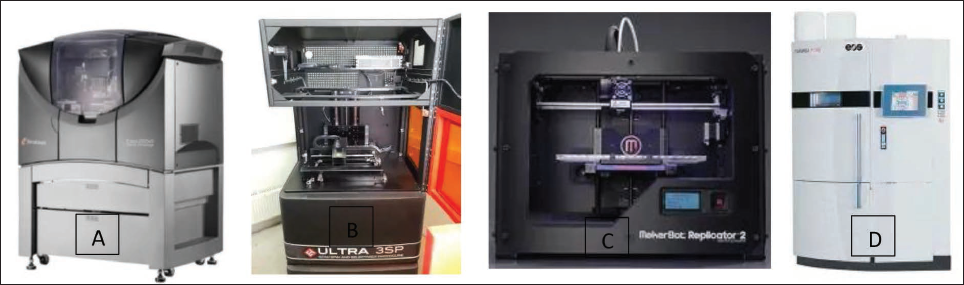
These days, the typical two-dimensional printer for printing on paper follows the x-axis from right to left and the y-axis from top to bottom. The up-and-down z-axis is added in 3D printing. The 3D printers used in orthodontics and dentistry that Stratasys has just purchased are called MakerBot and Objet (Figure 3). A wide variety of 3D printing technologies are currently used in orthodontics, and their respective uses, benefits, and drawbacks are summarized in Table 2.
Three-dimensional (3D) Printers Their Materials and Applications.
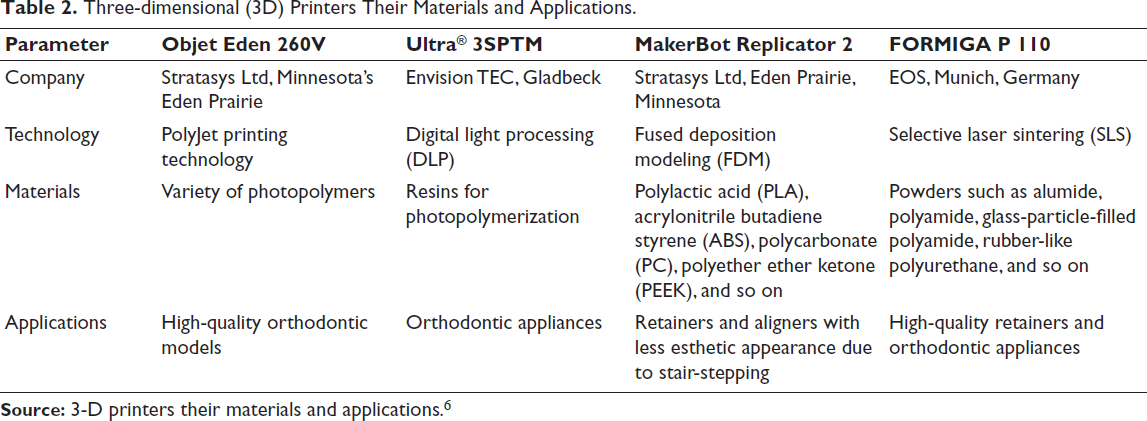
Three-dimensional (3D) Printer (A) Objet Eden. (B) Ultra® 3SP™. (C) MakerBot Replicator 2. (D) Formiga P 110.
Three-dimensional Printed Appliances Available for Orthodontic Practice
Three-dimensional Printed Archwire
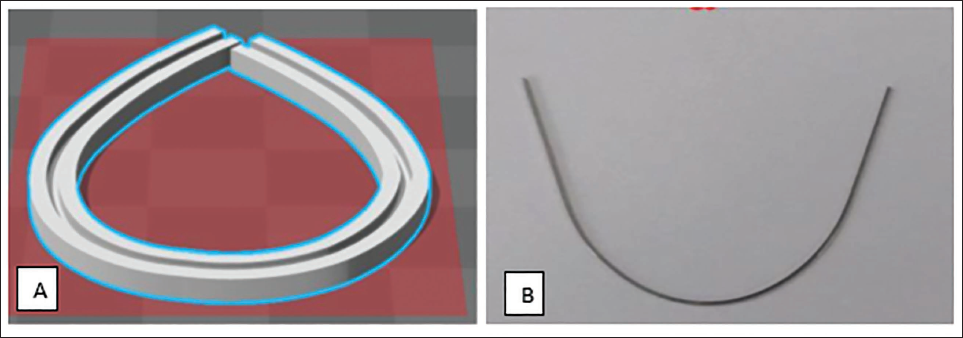
3D printed archwires represent an emerging advancement in digital orthodontics, enabling the fabrication of patient-specific orthodontic wires through additive manufacturing technologies. Based on intraoral digital impressions and CAD, these archwires are produced using metal 3D printing techniques, such as selective laser melting or direct metal laser sintering. Commonly fabricated from nickel–titanium (NiTi) or titanium-based alloys, 3D-printed archwires offer precise customization of arch form, force delivery, and tooth movement biomechanics. This approach reduces the need for manual wire bending, improves treatment predictability, and facilitates integration into fully digital orthodontic workflows. Despite these advantages, high production costs, limited clinical availability, and the need for long-term clinical validation currently restrict widespread adoption 11 (Figure 4). In designing a personalized archwire slot model, the mechanical properties of the wire material are crucial, particularly elasticity and springback after bending. Metallic orthodontic wires exhibit elastic recovery; therefore, the archwire groove geometry must be calculated to compensate for springback and achieve the desired final shape.
NiTi alloy was selected for the bending experiments due to its superior mechanical properties, including superelasticity, the shape memory effect, and a high elastic limit. Unlike conventional materials, NiTi does not strictly follow Hooke’s law over its deformation range, making it ideal for orthodontic applications. An experimental setup was developed to measure springback at different bending angles. The archwire was fixed on a base plate, and a vertical load was applied 2 mm from the reference point. The bending angle (θ) was defined as the angle between the tangent of the bending arc and the horizontal before bending, while the springback angle (α) was defined as the angular difference before and after elastic recovery.
(A) Three-dimensional (3D) Solid Model of Personalized Archwire Groove. (B) Archwire Bent with 3D Printed Model.
Experimental results showed that when the bending angle exceeded 10°, the springback angle increased approximately linearly with the bending angle. Using patient-specific dental arch data, discrete key points at 2 mm intervals were selected from the arch curve. The plastic deformation angle was calculated from adjacent points, and the required bending angle was determined by compensating for the measured springback. After coordinate transformation, these key points were used to generate the final personalized archwire groove and archwire geometry.
Functional Appliance
To lower the risk of upper incisor trauma, early treatment of some malocclusions, such as Class II Division 1, is advised; however, the use of traditional removable functional appliances is limited due to a lack of qualified technicians and limited resources. Automation presents a potential answer to these issues as digital orthodontics becomes more prevalent. This study investigates the viability of employing CAD-CAM technologies and 3D printing to facilitate the design and production of removable orthodontic appliances. 12
Although 3D printing presents promising advantages, its application in orthodontics is limited by challenges related to appliance redesign, material selection, and regulatory certification. Using appliances comparable in design and function to the functional regulator II and Sander II as examples, the article demonstrates the potential workflow for digitally designed and 3D-printed functional appliances, while acknowledging the need for modified nomenclature due to current limitations in replicating all analog features 13 (Figure 5).
Three-dimensional (3D) Fabricated Functional Appliance Incorporating Premade Screw.

Customized Orthodontic Brackets
A customized orthodontic bracket is a patient-specific bracket designed and manufactured using digital technologies to match the individual tooth anatomy and planned tooth movement. Based on intraoral digital impressions and virtual treatment planning, each bracket is tailored for a specific tooth with customized torque, tip, in–out values, and slot position.
These brackets are typically fabricated using CAD-CAM systems and are placed using indirect bonding techniques to ensure high placement accuracy. Customized orthodontic brackets improve treatment efficiency and predictability by reducing the need for wire bending and chairside adjustments, although they are associated with higher costs and reliance on digital infrastructure (Figure 6).
Customized Bracket.

Orthognathic Surgery Three-dimensional Planning
Orthodontists can more accurately plan surgical procedures, identify relevant anatomical structures, and simulate surgical movements in three dimensions by using CBCT and digital models for 3D planning. Surgical 3D-printed splints assist in directing screw placement, orthognathic correction, and surgical incisions to guarantee the precise execution of the treatment plan and improved patient outcomes.
The use of 3D printed models and patient-specific instructions has improved surgical planning and the transfer of surgical plans into the operating room for a better surgical outcome.
Surgical Splint Fabrication
With improved alternatives for surgical transfer, pre-operative planning, and procedure quality control, computer-assisted orthognathic surgery has become more common in recent years. 14 Pre-operative model surgery was the gold standard in classical orthognathic surgery, and numerous surgical splints were made to precisely align the fragments. This splint takes a long time to fabricate, and placement problems are a frequent issue. Computer-assisted technology has made it possible to create precise surgical splints, and 3D printing has been used to prepare surgical splints for orthognathic surgery prior to surgery 15 (Figure 7).

Although traditional surgical splints made with models and computer-assisted technologies have been shown to be comparable for routine clinical use, research indicates that computer-assisted surgical splints are useful in reducing the time and effort required for surgical planning. 16
Fixation Plates and Implants
Accurate 3D imaging is used to plan patient-specific fixation plates, which can secure the osteotomy segments in the proper place. Patient-specific titanium plates are made using the EOS Titanium Ti64 system (Electro Optical Systems) to repair and realign maxillary segments without the need for surgical splints. Numerous investigations have shown that these titanium implants offer accurate location, fixation, and sufficient stability for the maxillary Le Fort I osteotomy. 17
Three-dimensional Printed Surgical Model
For many patients undergoing orthognathic surgery, 3D models made from computer-generated images have greatly increased surgical success through precise pre-operative evaluation, surgical planning, intra-operative orientation, and pre-bending of microplates for fixation. This innovative method of model construction can eliminate many of the drawbacks of traditional surgery, such as improper condylar alignment or sag and inaccurate segment location. Three-dimensional printing (3DPTM), PolyJetTM.18, and SLS are common technologies used to create 3D printed models 18 (Figure 8).

Three-dimensional-printed Aligner
A 3D-printed aligner is an orthodontic appliance fabricated using digital workflows in which intraoral scans are used to design sequential tooth movements with CAD software, and aligners are produced using 3D printing technology. The digital model of each treatment stage is printed using biocompatible materials, followed by post-processing such as cleaning and curing. Compared to conventional thermoformed aligners, 3D-printed aligners offer improved customization, reduced material waste, and the potential for variable thickness and controlled force delivery. However, their widespread clinical use is still evolving due to material limitations, cost, and regulatory requirements (Figure 9).

Nasoalveolar Molding
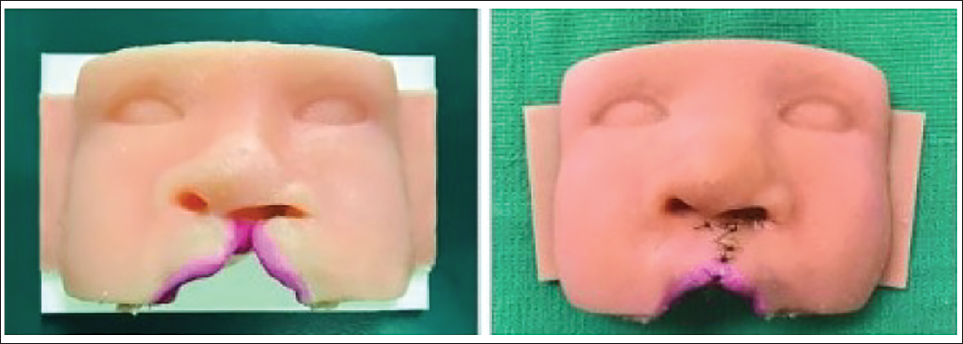
Maxillary alveolar abnormalities in neonates with cleft lip and palate have traditionally been treated with presurgical nasoalveolar shaping. Frequent visits, acrylic trimming as the section approaches, and the possibility of the device coming loose as it presses against the nasal tips using stents are the main disadvantages of the procedure. Virtual models of the ideal alveolar position can be created in order to avoid these issues, and 3D printing technology can be used to create a number of molding tools 19 (Figure 10).
Expansion Appliances
Rapid palatal expanders come in a variety of configurations, including single or linked bands, bands with arms, or, in the case of a facemask, arms with hooks that can extend anteriorly to attach elastics to the mask.
Hyrax-hayrake-blue-grass Combination
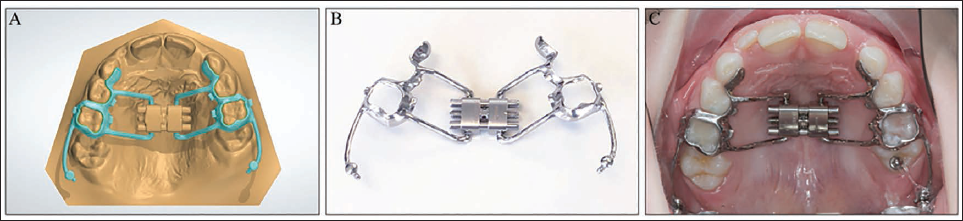
This apparatus incorporates three distinct devices: a hyrax, a split hayrake for habit breaking, and a blue-grass for tongue training. The blue-grass component’s movable metal bead was printed alongside the framework and joined by a sprue, a little rod that joins printed components. During electropolishing, the sprue was eliminated, releasing the bead 20 (Figure 11).
Hyrax-hayrake-blue-grass Combination. (A) Computer-aided Design and Manufacturing (CAD-CAM) Design. (B) Printed Appliance with Jackscrew Welded Afterwards. (C) Appliance Inserted with Movable Blue-grass Bead.

Hyrax-Halterman
This device uses a hyrax and a Halterman to distalize the ectopic molars and expand the maxilla simultaneously (Figure 3A-3C). On the deciduous second molars, 12 buccal cantilever arms protrude distally from the saddle bands. The first molars’ occlusal surfaces were fused together using buttons, and elastic chains were attached from the buttons to the arms (Figure 12).
Hyrax-Halterman. (A) Computer-aided Design and Manufacturing (CAD-CAM) Design. Saddle Bands on the Deciduous Second Molars are Ideal in the Presence of Ectopic First Molars. (B) Printed Appliance. (C) After Activation.
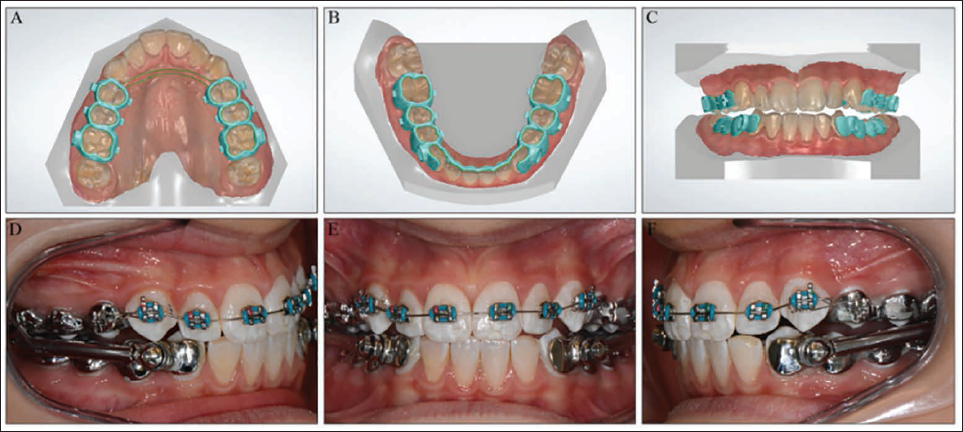
Herbst with Brackets
Instead of using traditional tubes, this gadget adds buccal brackets to the Herbst framework. This device incorporates buccal brackets into the Herbst framework in place of conventional tubes. The bracket groove enhances torque management, and the wings make it easier to install a steel ligature or an elastic chain. If a perfect slotwire contact is required, like in the lower arch where incisor torque control is crucial, the bracket slot should be printed somewhat smaller (Figure 13).
Hyrax-Halterman. (A) CAD-CAM Design. Saddle Bands on the Deciduous Second Molars are Ideal in the Presence of Ectopic First Molars. (B) Printed Appliance. (C) After Activation. (D–F) Intraoral Clinical Views.
Lingual Arch with Clasps
In order to prevent drift into the canine space, this device features clasps distal to the lateral incisors. An appliance that has been entirely printed will be stiff. Consequently, a traditional wire must be soldered onto the printed saddle bands if the orthodontist favors non-rigid adjustment loops (Figure 14).
Lingual Arch with Clasps. (A) Computer-aided Design and Manufacturing (CAD-CAM) Design. The Left Activation Loop was Unnecessary as the Printed Metal Framework Cannot be Adjusted. (B) Appliance Inserted. (C) Lower Canines Erupted.

Miniscrew Supported Hyrax Distalizer with Facemask Hooks
Miniscrew-supported Hyrax-distalizer with Facemask Hooks. (A) Pre-treatment Occlusal-view. (B) Computer-aided Manufacturing and Design (CAM-CAD). (C) Close-up View of the Saddle Band on the Ectopic Molar. (D) Appliance Inserted. (E) Following Expansion and Distalization. (F) Hyrax Removed and a Printed Transpalatal Arch (TPA) Inserted.
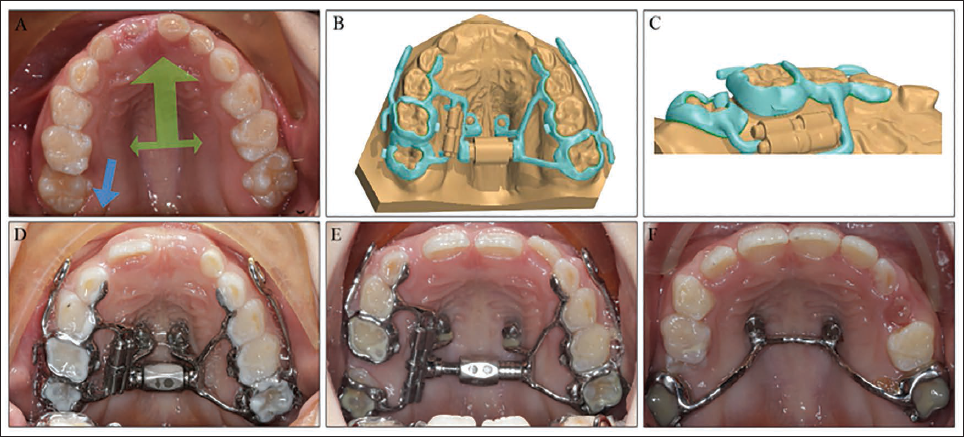
The benefits of 3D metal printing are best exemplified by this intricate device. One of the objectives was to design a miniscrew-supported hyrax with facemask hooks that also distalized an ectopic molar. The partially erupted tooth was best bonded with a saddle band. The two jackscrews, which differed in size and type, were soldered into the printed metal structure after being carefully measured visually 20 (Figure 15).
Recent Advances of Three-dimensional Printing in Orthodontics
A few years ago, the advantages of additive manufacturing were still theoretical, and it was debatable whether switching from conventional, high-volume techniques to additive ones was technologically or economically beneficial. The future of 3D printing is bright, as desktop manufacturing has found its footing and is now a prominent pillar in the manufacturing revolution. The following are the latest advancements.
Compliance Monitoring
Functional appliances, sleep disorder appliances, facemasks, active removable appliances, and long-term removable retainer wear are all advised in order to monitor compliance after orthodontic treatment. These gadgets have successfully included micro-electronic sensors. These cutting-edge 3D printed appliances can be used to assess wearable technology for continuous, covert, and objective monitoring of compliance, sleep problems, and jaw function and parafunction.
In order to track mandibular motion in realistic settings, wearable technology that is lightweight and inconspicuous is essential. It also works in tandem with microsensors to track compliance in obstructive sleep apnea subjects/participants. 21 It may take some time before 3D printed orthodontic brackets with light-emitting diode lights and batteries for better bone regeneration are used in clinical orthodontic practice after enough evidence-based studies and trials have been conducted, according to reports. Dentists can create more sophisticated and accurate gadgets with the aid of the software’s predictions and simulations. This is just the beginning of what can be 3D printed in the dental sector; it does not encompass the entire range of potential applications. Among the various options are surgical instruments, night guards, and other 3D-printed equipment. 22
Three-dimensional Printing: A Guide from the Present to the Future
Here are six predictions about the near future of additive manufacturing.
Larger, quicker, and significantly more affordable 3D printing will be possible. Future developments will be aided by additive manufacturing, which will develop into a robust component of the product supply chain. Collaboration will be crucial. Improved quality and cybersecurity assurance will be possible. The economy will benefit from 3D printing. Sustainability will be advanced and mastered by additive manufacturing.
Now that the concept and ideology of artificial intelligence are on the horizon, there are a number of opportunities that could improve the dental clinic’s operational model, lower labor costs, and boost industry efficiency. Effective device encapsulation (including supporting electronic interfaces and power supply) and the use of biocompatible materials to lower risks associated with salivary contact—specifically, the leaching of chemicals into surrounding areas—are necessary to protect the functionality of electronic devices. 23 3D printing has an even more promising, dynamic, and successful future than it does now. Orthodontics is one of the fields that has adapted to this technology in order to enhance its input and output. Commercially available (4D Facial Dynamics) offers a quantitative comprehension of facial expression, real anatomical motion, and soft tissue movement.
The human face is capable of producing distinct micro-expressions that last less than 0.04 seconds and have very little intensity. In order to obtain accuracy in interpreting the tracking motions, the dynamic systems continually track the movements of the facial surface frame by frame. Evaluation of facial animation may be crucial for craniofacial abnormalities, orthodontic diagnosis, virtual surgical planning, and treatment results. Using 3D printers, 4D printing produces 3D items in real time without the need for wires. It accomplishes this by employing intelligent materials, which may be programmed to alter their size, color, or shape in response to outside stimuli. This is true for active polymers, hydrogel resins, and even living tissues. For instance, an object may bend, fix, assemble, or even dissolve itself because of 4D printing. By responding to its surroundings, it naturally takes on a new form or purpose.
Conclusion
Digital technologies are reshaping orthodontics at a pace unmatched in the specialty’s history, extending their influence beyond clinical procedures to practice management, education, and professional identity. The transition from conventional workflows to fully digital, automated systems offers improved diagnostic accuracy, streamlined processes, enhanced customization, and reduced chairside time. While concerns regarding depersonalization and overreliance on technology remain, digital transformation has the potential to strengthen, rather than weaken, doctor–patient relationships by allowing clinicians to focus more on humane clinical care. As advances in artificial intelligence, machine learning, and digital manufacturing continue to accelerate, the proactive adoption, critical evaluation, and thoughtful integration of these technologies will be essential for orthodontists to remain relevant, efficient, and future-ready.
Footnotes
Authors Contribution
Dr. Suresh Kangane: Conceptualization, supervision, critical review, and final approval of the manuscript.
Dr. Sumit Honrao: Literature review, data collection, manuscript drafting, figure preparation, and coordination of manuscript submission.
Dr. Pravinkumar Maroore: Methodology development, technical validation, and critical revision of intellectual content.
Dr. Yatishkumar Joshi: Data interpretation, drafting of specific sections (clinical applications), and manuscript editing.
Dr. Shilpa Bikkad: Literature search, data organization, and assistance in manuscript writing.
Dr. Sujit Zadake: Review of 3D printing technologies, technical inputs, and manuscript proofreading.
Dr. Riya Gala: Data compilation, formatting, referencing, and assistance in final manuscript preparation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was not required for this study as it is a review article based on previously published literature and did not involve human participants or animals.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.